
CLINICAL HANDBOOK OF Psychotropic Drugs - … Handbook of Psychotropic Drugs for Children and...
18
3 DEAN ELBE · KALYNA Z. BEZCHLIBNYK-BUTLER ADIL S. VIRANI · RIC M. PROCYSHYN (EDS.) Online version also available see http://chpd.hogrefe.com/ CLINICAL HANDBOOK OF Psychotropic Drugs for Children and Adolescents 3rd edition
Transcript of CLINICAL HANDBOOK OF Psychotropic Drugs - … Handbook of Psychotropic Drugs for Children and...
3DEAN ELBE · KALYNA Z. BEZCHLIBNYK-BUTLERADIL S. VIRANI · RIC M. PROCYSHYN (EDS.)
Online versi
on also availa
ble
see http://
chpd.hogrefe.com/
CLINICAL HANDBOOK OF
Psychotropic Drugsfor Children and Adolescents 3rd edition
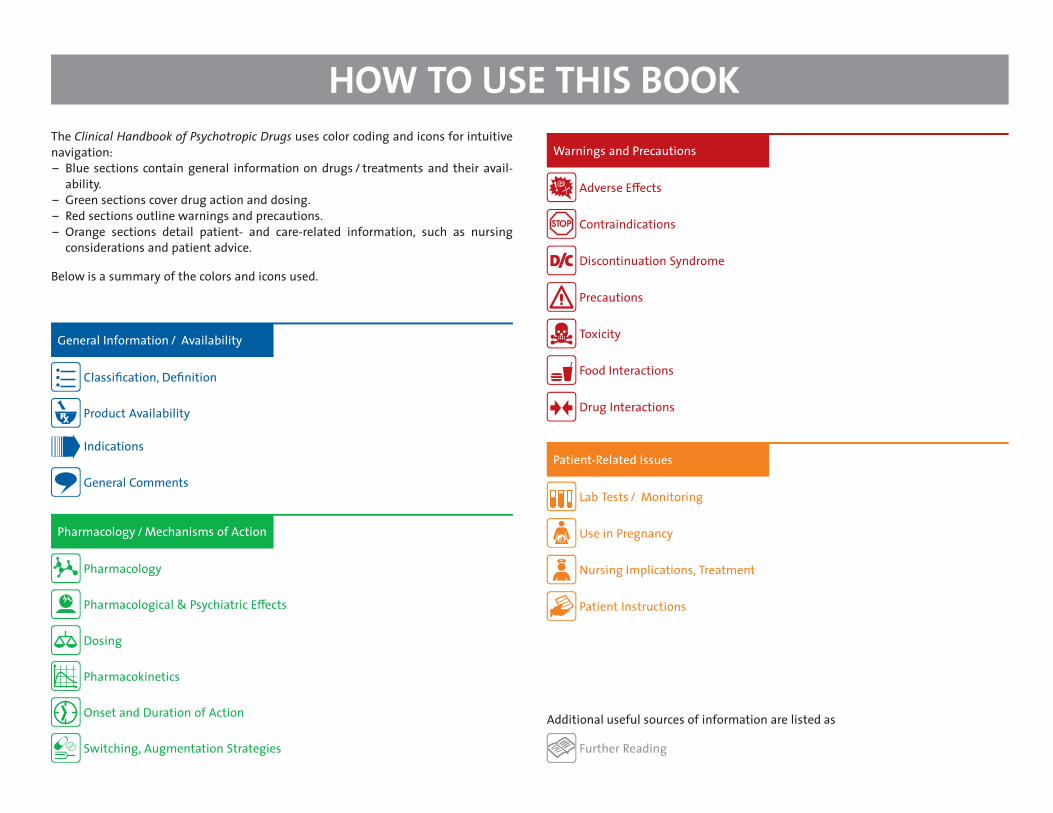
HOW TO USE THIS BOOKThe Clinical Handbook of Psychotropic Drugs uses color coding and icons for intuitivenavigation:– Blue sections contain general information on drugs / treatments and their avail-
ability.– Green sections cover drug action and dosing.– Red sections outline warnings and precautions.– Orange sections detail patient- and care-related information, such as nursing
considerations and patient advice.
Below is a summary of the colors and icons used.
General Information / Availability�
�
�
�
Classišcation, Dešnition�
�
�
�
Product Availability
Indications�
�
�
�
General Comments
Pharmacology / Mechanisms of Action�
�
�
�
Pharmacology�
�
�
�
Pharmacological & Psychiatric E−ects�
�
�
�
Dosing�
�
�
�
Pharmacokinetics�
�
�
�
Onset and Duration of Action�
�
�
�
Switching, Augmentation Strategies
Warnings and Precautions�
�
�
�
Adverse E−ects�
�
�
�
Contraindications�
�
�
�
Discontinuation Syndrome�
�
�
�
Precautions�
�
�
�
Toxicity�
�
�
�
Food Interactions�
�
�
�
Drug Interactions
Patient-Related Issues�
�
�
�
Lab Tests / Monitoring�
�
�
�
Use in Pregnancy�
�
�
�
Nursing Implications, Treatment�
�
�
�
Patient Instructions
Additional useful sources of information are listed as�
�
�
�
Further Reading
Clinical Handbook of Psychotropic Drugsfor Children and Adolescents
Dean Elbe, BSc (Pharm), PharmD, BCPP(A, B)
Kalyna Z. Bezchlibnyk-Butler, BScPhm, FCSHPAdil S. Virani, BSc (Pharm), PharmD, FCSHP(B)
Ric M. Procyshyn, BSc (Pharm), MSc, PharmD, PhD(C)
The Editors wish to acknowledge contributions from the following chapter co-editors:
Tyler R. Black, BSc, MD, FRCPC(D) (Psychiatric Disorders in Children and Adolescents)Carla Dillon, BSc (Pharm), ACPR, PharmD(E) (Antipsychotics)Lynda Eccott, BSc, MScPharm(F) (Natural Health Products)Barry A. Martin, MD, FRCPC(G) (Electroconvulsive Therapy)
Roger S. McIntyre, MD, FRCPC(H) (Mood Stabilizers)Leslie Phillips, BSc (Pharm), PharmD(E) (Antipsychotics)
(A) Department of Child and Adolescent Mental Health, Children’s & Women’s Health Centre of British Columbia, Vancouver, BC, Canada(B) Lower Mainland Pharmacy Services and Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC, Canada
(C) British Columbia Mental Health & Addictions Research Insitute, Vancouver, BC, Canada; Department of Psychiatry, University of British Columbia, Vancouver, BC, Canada(D) CAPE Unit, BC Children’s Hospital, and Department of Psychiatry, University of British Columbia, Vancouver, BC, Canada
(E) School of Pharmacy, Memorial University of Newfoundland, St. John’s, NL, Canada(F) Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC, Canada
(G) Centre for Addiction and Mental Health and Department of Psychiatry, University of Toronto, Toronto, ON, Canada(H) Toronto Western Hospital, University Health Network, and Department of Psychiatry, University of Toronto, Toronto, ON, Canada
Library of Congress Cataloging-in-Publication Data
is available via the Library of Congress Marc Database under theLC Control Number 2014933647
National Library of Canada Cataloguing-in-Publication Data
Main entry under title:
Clinical handbook of psychotropic drugs for children and adolescents/ [edited by] Dean Elbe, BSc (Pharm), PharmD, BCPP, Kalyna Z.Bezchlibnyk-Butler, BScPhm, FCSHP, Adil S. Virani, BSc (Pharm), PharmD,FCSHP, Ric M. Procyshyn, BSc (Pharm), MSc, PharmD, PhD. – Third revised edition.Text runs parallel to spine.Revision of: Clinical handbook of psychotropic drugs for children andadolescents / Kalyna Z. Bezchlibnyk-Butler, Adil S. Virani, [eds.]. –2nd rev. ed. – Toronto : Hogrefe & Huber, c2007.Includes bibliographical references and index.Issued in print and electronic formats.
ISBN 978-0-88937-456-0 (pbk.).–ISBN 978-1-61676-456-2 (pdf)
1. Psychotropic drugs–Handbooks, manuals, etc. 2. Pediatricpsychopharmacology–Handbooks, manuals, etc. I. Elbe, Dean, editorII. Bezchlibnyk-Butler, Kalyna Z., 1947–, editor. III. Virani, Adil S., editorIV. Procyshyn, Ric M. (Ric Michael), 1961-, editorRM315.C56 2014 615’.788083 C2014-901234-9
Copyright © 2015 by Hogrefe Publishing
PUBLISHING OFFICESUSA: Hogrefe Publishing, 38 Chauncy Street, Suite 1002, Boston, MA 02111
Phone (866) 823-4726, Fax (617) 354-6875;E-mail [email protected]
EUROPE: Hogrefe Publishing, Merkelstr. 3, 37085 Göttingen, GermanyPhone +49 551 99950-0, Fax +49 551 99950-425, E-mail [email protected]
SALES & DISTRIBUTIONUSA: Hogrefe Publishing, Customer Services Department, 30 Amberwood Parkway,
Ashland, OH 44805
Phone (800) 228-3749, Fax (419) 281-6883, E-mail [email protected]: Hogrefe Publishing c/o Marston Book Services Ltd, 160 Eastern Ave., Milton Park, Abingdon, OX14 4SB, UK
Phone +44 1235 465577, Fax +44 1235 465556, E-mail [email protected]: Hogrefe Publishing, Merkelstr. 3, 37085 Göttingen, Germany
Phone +49 551 99950-0, Fax +49 551 99950-425, E-mail [email protected]
No part of this publication may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying,microšlming, recording, or otherwise, without written permission from the publisher.The authors and publisher have made every e−ort to ensure that drug selections anddosages suggested in this text are in accord with current recommendations andpractice at the time of publication. However, due to changing government regulations,continuing research, and changing information concerning drug therapy and reactions,the reader is urged to check the package insert for each drug for any change inindications and dosage, or for added precautions. The authors and publisher disclaimany responsibility for any consequences which may follow from the use of informationpresented in this book.
www.hogrefe.com
3rd edition
ISBN 978-0-88937-456-0Hogrefe Publishing
INTRODUCTIONThe Clinical Handbook of Psychotropic Drugs for Children and Adolescents is intendedto be a user-friendly and practical resource guide on the use of psychotropic drugs inchildren and adolescents. Its content is derived from various forms of published literature(including randomized controlled trials, scientišc data such as pharmacokinetic trials,cohort trials, case series, and case reports) as well as from leading clinical experts. Weendeavor to continually update this handbook as the psychiatric literature evolves sowe can continue to provide evidence-based clinically relevant information that is easilyaccessed and utilized to aid with patient care decisions. New sections, periodically added,re¦ect changes in therapy and in current practice.
Many classes of psychotropic drugs are used to treat childhood and adolescent mentalillness on the basis of e³cacy in adults, despite not being currently approved for usein these populations. The lack of approval does not necessarily re¦ect lack of safety ore³cacy, but it does re¦ect a lack of controlled studies in these age groups. Many productmonographs include a statement stating their drug has not been adequately studied inchildren and the safety of the drug has not been established under a specišc age.
In the Product Availability section of each chapter, the Clinical Handbook includesmonograph statements regarding the recommendations for the use of each drug inchildren and adolescents. Approved indications for children and adolescents are stated,as are those for adults; also included are nonapproved indications for these drugs. Eachchapter includes data from open and double-blind studies, where available, regardingdoses, adverse e−ects, and other considerations in children and adolescents.
Because of a lack of comparative data in children and adolescents for most drug classes,Adverse Reaction tables and Drug Interaction charts re¦ect information that pertains toheterogeneous age groups (youth and adults).
Patient and Caregiver Information Sheets for most drug categories are provided asprintable pdf šles to facilitate education/counselling of patients receiving these medica-tions and their caregivers. For details, please see p. 354.
Most children and adolescents with a diagnosable psychiatric disorder require multi-modal interventions to address the symptoms of the disorder, the comorbid conditions,and the psychological, social, and developmental sequelae. Individual and family psy-choeducation are essential, and psychosocial interventions should be considered for mostpsychiatric disorders.
Until systematic double-blind studies of various psychotropic drugs have been con-ducted to determine the e³cacy, the pharmacokinetics, as well as the relative and
absolute risks of each drug in this population, physicians who choose to use specišcpsychotropic drugs in children and adolescents should review all available studies andmonitor their patients on a regular basis. Consideration should be given to obtaininginformed consent from the caregiver or youth (depending on the patient’s age) for usein unapproved indications.
Given that changes may occur in a medication’s indications, and di−erences are seenamong countries, specišc “indications” listed in this text as “approved” should be viewedin conjunction with product monographs approved in your jurisdiction of interest.
Dose comparisons and plasma levels are based on scientišc data. However, it isimportant to note that some patients will respond to doses outside the reported ranges.Age, sex, and the medical condition of the patient must always be taken into considerationwhen prescribing any psychotropic agent.
The purpose of this handbook is to provide quick access to relevant, practical, andimportant information clinicians should be aware of when considering pharmacologicaloptions available in the treatment of childhood and adolescent psychiatric disorders. Itprovides an overview of the plausible alternatives, dosing guidelines, as well as informa-tion on drug interactions and potential side e−ects. It is meant to be a resource to boththose in training and experienced clinicians.
For those who like the convenience of electronic resources, the Clinical Handbook ofPsychotropic Drugs for Children and Adolescents is also available as an online version thatprovides even quicker access to all the information in the handbook, with some addedextras: (1) An auto-completion powered search function, (2) browse features for genericnames, trade names, indications, and interacting agents, (3) column-selector enhance-ment of comparison charts (dosages, side e−ects, pharmacokinetics, interactions. . . ) thatallows you to choose which information is displayed, and (4) hundreds of additionalreferences. Further details on this can be found at http://www.hogrefe.com/chpd-online
Over the years, many readers have asked many interesting questions and provideduseful comments and suggestions regarding the content and format of the handbook.This input is critical to keeping this handbook current, accurate, and relevant to thereadership. We really appreciate the feedback. Please feel free to e-mail me at the addressbelow with your comments and questions.
Dean ElbeE-mail: [email protected]
The Clinical Handbook of Psychotropic Drugs for Children & Adolescents ONLINE is the full-text online version of the popular Clinical Handbook of Psychotropic Drugs for Children & Adolescents. It retains all the practical features for which the Clinical Handbook is re-nowned and makes the information even more easily accessible. As in the print edition, instantly recognizable icons and color coding allow you to find at a glance the informa-tion you seek. But the CHPD for Children & Adolescents ONLINE version offers much more. Unique features that allow even quicker access to the wealth of information include:
CLINICAL HANDBOOK OF PSYCHOTROPIC DRUGS FOR CHILDREN & ADOLESCENTS ONLINE
Also available:
Auto-completion powered search function
Browse features for
Generic Names Trade Names Indications Interacting Agents
Column-selector enhancement of comparison charts (dosages, side effects, pharmacokinet-ics, interactions, etc.) that allows you to choose which information is displayed.
Hundreds of additional references
Browse by generic names, trade names, indications, interacting agents
Column-selector enhancement of comparison charts
Auto-completion powered search function
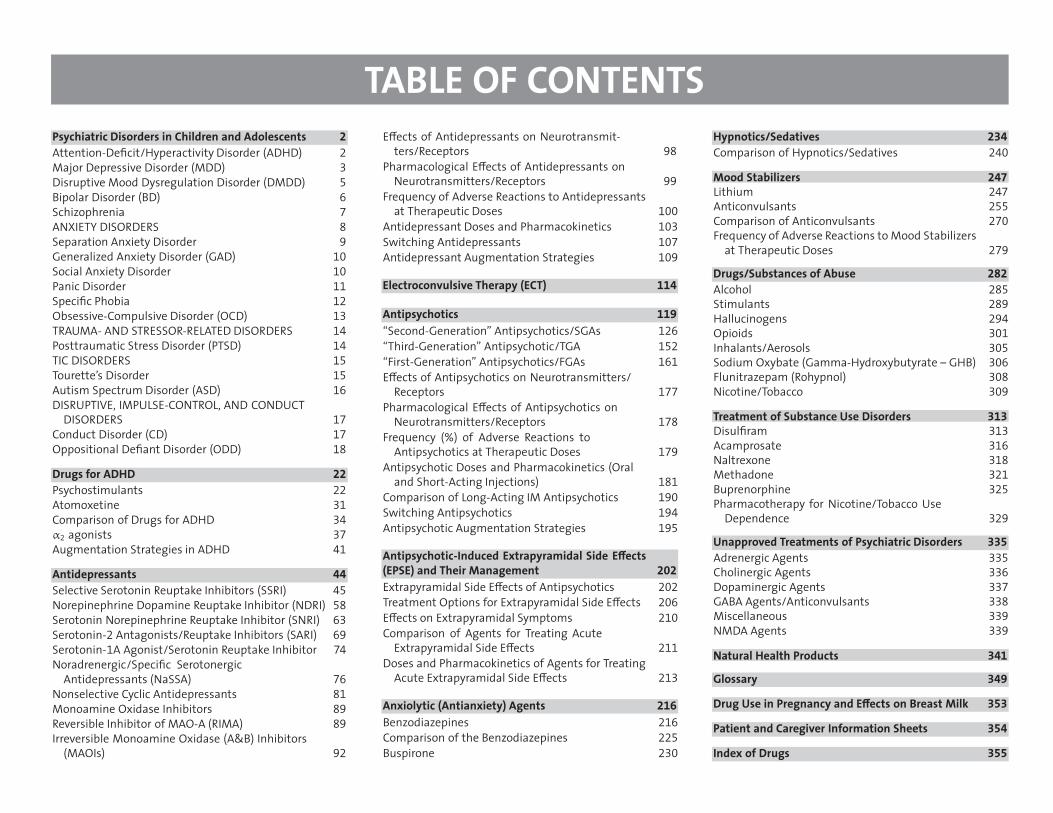
TABLE OF CONTENTSPsychiatric Disorders in Children and Adolescents 2
Attention-Dešcit/Hyperactivity Disorder (ADHD) 2
Major Depressive Disorder (MDD) 3
Disruptive Mood Dysregulation Disorder (DMDD) 5
Bipolar Disorder (BD) 6
Schizophrenia 7
ANXIETY DISORDERS 8
Separation Anxiety Disorder 9
Generalized Anxiety Disorder (GAD) 10
Social Anxiety Disorder 10
Panic Disorder 11
Specišc Phobia 12
Obsessive-Compulsive Disorder (OCD) 13
TRAUMA- AND STRESSOR-RELATED DISORDERS 14
Posttraumatic Stress Disorder (PTSD) 14
TIC DISORDERS 15
Tourette’s Disorder 15
Autism Spectrum Disorder (ASD) 16
DISRUPTIVE, IMPULSE-CONTROL, AND CONDUCTDISORDERS 17
Conduct Disorder (CD) 17
Oppositional Dešant Disorder (ODD) 18
Drugs for ADHD 22
Psychostimulants 22
Atomoxetine 31
Comparison of Drugs for ADHD 34
α2 agonists 37
Augmentation Strategies in ADHD 41
Antidepressants 44
Selective Serotonin Reuptake Inhibitors (SSRI) 45
Norepinephrine Dopamine Reuptake Inhibitor (NDRI) 58
Serotonin Norepinephrine Reuptake Inhibitor (SNRI) 63
Serotonin-2 Antagonists/Reuptake Inhibitors (SARI) 69
Serotonin-1A Agonist/Serotonin Reuptake Inhibitor 74
Noradrenergic/Specišc SerotonergicAntidepressants (NaSSA) 76
Nonselective Cyclic Antidepressants 81
Monoamine Oxidase Inhibitors 89
Reversible Inhibitor of MAO-A (RIMA) 89
Irreversible Monoamine Oxidase (A&B) Inhibitors(MAOIs) 92
E−ects of Antidepressants on Neurotransmit-ters/Receptors 98
Pharmacological E−ects of Antidepressants onNeurotransmitters/Receptors 99
Frequency of Adverse Reactions to Antidepressantsat Therapeutic Doses 100
Antidepressant Doses and Pharmacokinetics 103
Switching Antidepressants 107
Antidepressant Augmentation Strategies 109
Electroconvulsive Therapy (ECT) 114
Antipsychotics 119
“Second-Generation” Antipsychotics/SGAs 126
“Third-Generation” Antipsychotic/TGA 152
“First-Generation” Antipsychotics/FGAs 161
E−ects of Antipsychotics on Neurotransmitters/Receptors 177
Pharmacological E−ects of Antipsychotics onNeurotransmitters/Receptors 178
Frequency (%) of Adverse Reactions toAntipsychotics at Therapeutic Doses 179
Antipsychotic Doses and Pharmacokinetics (Oraland Short-Acting Injections) 181
Comparison of Long-Acting IM Antipsychotics 190
Switching Antipsychotics 194
Antipsychotic Augmentation Strategies 195
Antipsychotic-Induced Extrapyramidal Side E−ects(EPSE) and Their Management 202
Extrapyramidal Side E−ects of Antipsychotics 202
Treatment Options for Extrapyramidal Side E−ects 206
E−ects on Extrapyramidal Symptoms 210
Comparison of Agents for Treating AcuteExtrapyramidal Side E−ects 211
Doses and Pharmacokinetics of Agents for TreatingAcute Extrapyramidal Side E−ects 213
Anxiolytic (Antianxiety) Agents 216
Benzodiazepines 216
Comparison of the Benzodiazepines 225
Buspirone 230
Hypnotics/Sedatives 234
Comparison of Hypnotics/Sedatives 240
Mood Stabilizers 247
Lithium 247
Anticonvulsants 255
Comparison of Anticonvulsants 270
Frequency of Adverse Reactions to Mood Stabilizersat Therapeutic Doses 279
Drugs/Substances of Abuse 282
Alcohol 285
Stimulants 289
Hallucinogens 294
Opioids 301
Inhalants/Aerosols 305
Sodium Oxybate (Gamma-Hydroxybutyrate – GHB) 306
Flunitrazepam (Rohypnol) 308
Nicotine/Tobacco 309
Treatment of Substance Use Disorders 313
Disulšram 313
Acamprosate 316
Naltrexone 318
Methadone 321
Buprenorphine 325
Pharmacotherapy for Nicotine/Tobacco UseDependence 329
Unapproved Treatments of Psychiatric Disorders 335
Adrenergic Agents 335
Cholinergic Agents 336
Dopaminergic Agents 337
GABA Agents/Anticonvulsants 338
Miscellaneous 339
NMDA Agents 339
Natural Health Products 341
Glossary 349
Drug Use in Pregnancy and E−ects on Breast Milk 353
Patient and Caregiver Information Sheets 354
Index of Drugs 355
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing 2
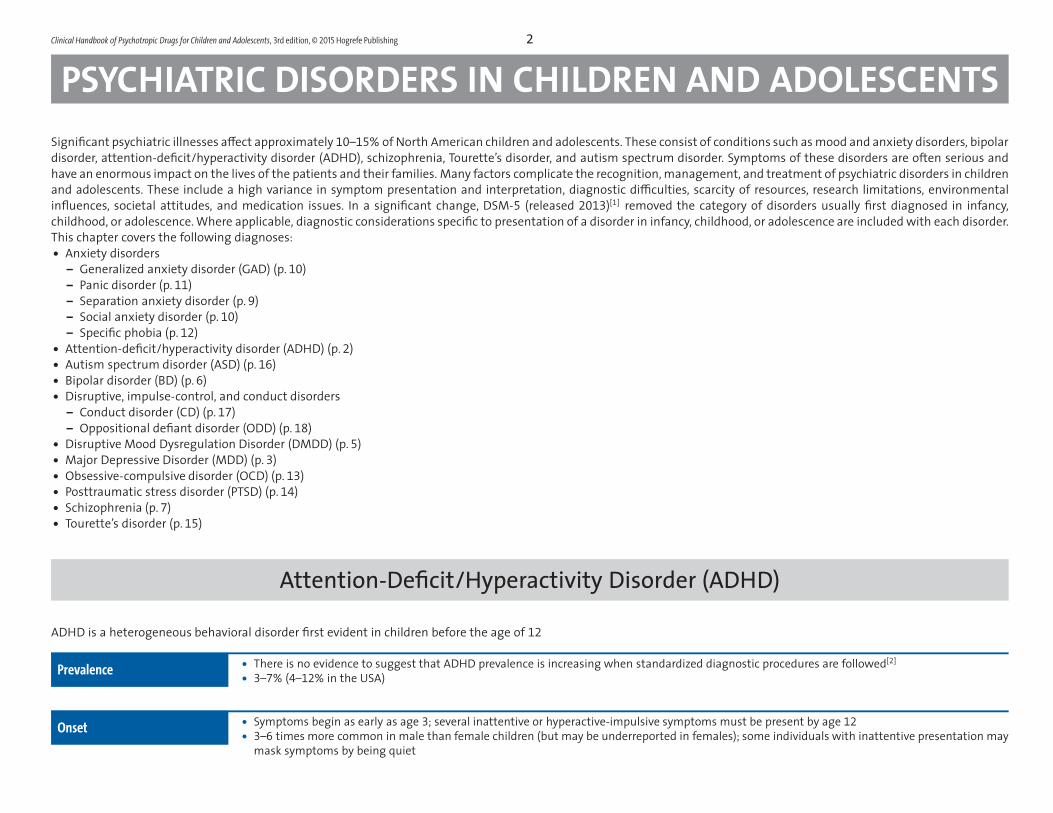
PSYCHIATRIC DISORDERS IN CHILDREN AND ADOLESCENTSSignišcant psychiatric illnesses a−ect approximately 10–15% of North American children and adolescents. These consist of conditions such as mood and anxiety disorders, bipolardisorder, attention-dešcit/hyperactivity disorder (ADHD), schizophrenia, Tourette’s disorder, and autism spectrum disorder. Symptoms of these disorders are often serious andhave an enormous impact on the lives of the patients and their families. Many factors complicate the recognition, management, and treatment of psychiatric disorders in childrenand adolescents. These include a high variance in symptom presentation and interpretation, diagnostic di³culties, scarcity of resources, research limitations, environmentalin¦uences, societal attitudes, and medication issues. In a signišcant change, DSM-5 (released 2013)[1] removed the category of disorders usually šrst diagnosed in infancy,childhood, or adolescence. Where applicable, diagnostic considerations specišc to presentation of a disorder in infancy, childhood, or adolescence are included with each disorder.This chapter covers the following diagnoses:• Anxiety disorders
– Generalized anxiety disorder (GAD) (p. 10)– Panic disorder (p. 11)– Separation anxiety disorder (p. 9)– Social anxiety disorder (p. 10)– Specišc phobia (p. 12)
• Attention-dešcit/hyperactivity disorder (ADHD) (p. 2)• Autism spectrum disorder (ASD) (p. 16)• Bipolar disorder (BD) (p. 6)• Disruptive, impulse-control, and conduct disorders
– Conduct disorder (CD) (p. 17)– Oppositional dešant disorder (ODD) (p. 18)
• Disruptive Mood Dysregulation Disorder (DMDD) (p. 5)• Major Depressive Disorder (MDD) (p. 3)• Obsessive-compulsive disorder (OCD) (p. 13)• Posttraumatic stress disorder (PTSD) (p. 14)• Schizophrenia (p. 7)• Tourette’s disorder (p. 15)
Attention-Dešcit/Hyperactivity Disorder (ADHD)
ADHD is a heterogeneous behavioral disorder šrst evident in children before the age of 12
Prevalence • There is no evidence to suggest that ADHD prevalence is increasing when standardized diagnostic procedures are followed[2]
• 3–7% (4–12% in the USA)
Onset • Symptoms begin as early as age 3; several inattentive or hyperactive-impulsive symptoms must be present by age 12
• 3–6 times more common in male than female children (but may be underreported in females); some individuals with inattentive presentation maymask symptoms by being quiet
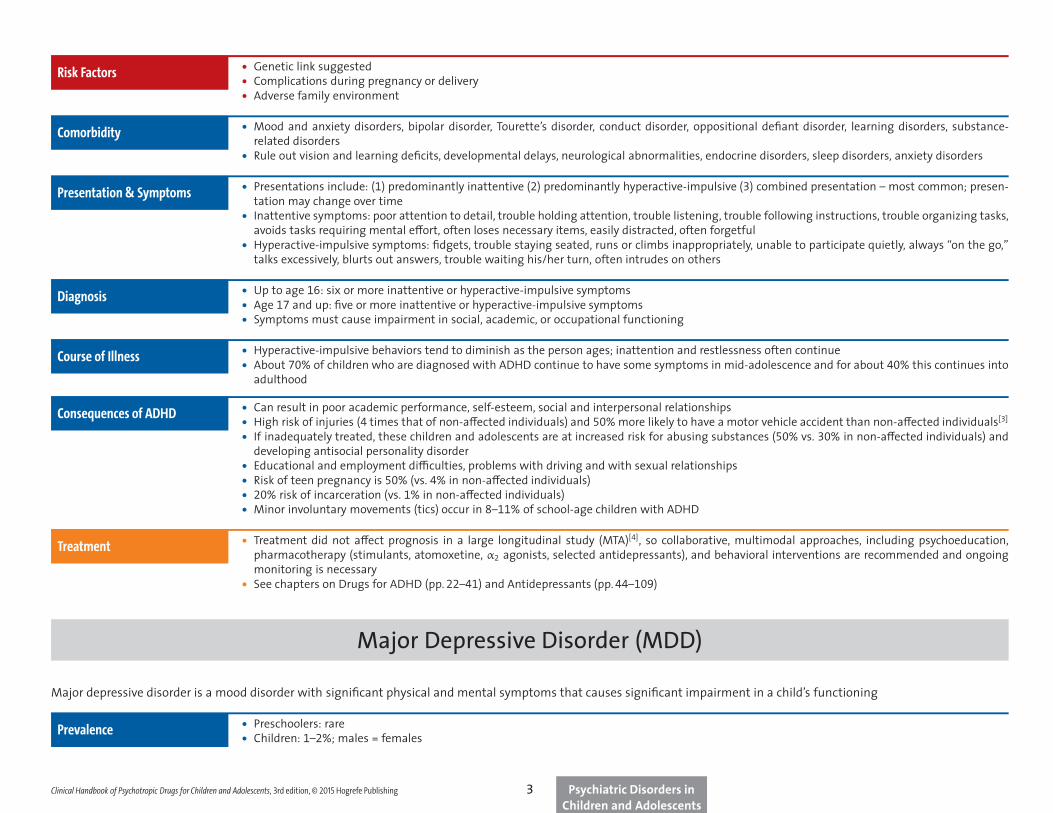
Risk Factors • Genetic link suggested• Complications during pregnancy or delivery• Adverse family environment
Comorbidity • Mood and anxiety disorders, bipolar disorder, Tourette’s disorder, conduct disorder, oppositional dešant disorder, learning disorders, substance-related disorders
• Rule out vision and learning dešcits, developmental delays, neurological abnormalities, endocrine disorders, sleep disorders, anxiety disorders
Presentation & Symptoms• Presentations include: (1) predominantly inattentive (2) predominantly hyperactive-impulsive (3) combined presentation – most common; presen-
tation may change over time• Inattentive symptoms: poor attention to detail, trouble holding attention, trouble listening, trouble following instructions, trouble organizing tasks,
avoids tasks requiring mental e−ort, often loses necessary items, easily distracted, often forgetful• Hyperactive-impulsive symptoms: šdgets, trouble staying seated, runs or climbs inappropriately, unable to participate quietly, always “on the go,”
talks excessively, blurts out answers, trouble waiting his/her turn, often intrudes on others
Diagnosis• Up to age 16: six or more inattentive or hyperactive-impulsive symptoms• Age 17 and up: šve or more inattentive or hyperactive-impulsive symptoms• Symptoms must cause impairment in social, academic, or occupational functioning
Course of Illness• Hyperactive-impulsive behaviors tend to diminish as the person ages; inattention and restlessness often continue• About 70% of children who are diagnosed with ADHD continue to have some symptoms in mid-adolescence and for about 40% this continues into
adulthood
Consequences of ADHD • Can result in poor academic performance, self-esteem, social and interpersonal relationships• High risk of injuries (4 times that of non-a−ected individuals) and 50% more likely to have a motor vehicle accident than non-a−ected individuals[3]
• If inadequately treated, these children and adolescents are at increased risk for abusing substances (50% vs. 30% in non-a−ected individuals) anddeveloping antisocial personality disorder
• Educational and employment di³culties, problems with driving and with sexual relationships• Risk of teen pregnancy is 50% (vs. 4% in non-a−ected individuals)• 20% risk of incarceration (vs. 1% in non-a−ected individuals)• Minor involuntary movements (tics) occur in 8–11% of school-age children with ADHD
Treatment • Treatment did not a−ect prognosis in a large longitudinal study (MTA)[4], so collaborative, multimodal approaches, including psychoeducation,pharmacotherapy (stimulants, atomoxetine, α2 agonists, selected antidepressants), and behavioral interventions are recommended and ongoingmonitoring is necessary
• See chapters on Drugs for ADHD (pp. 22–41) and Antidepressants (pp. 44–109)
Major Depressive Disorder (MDD)
Major depressive disorder is a mood disorder with signišcant physical and mental symptoms that causes signišcant impairment in a child’s functioning
Prevalence • Preschoolers: rare• Children: 1–2%; males = females
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing Psychiatric Disorders inChildren and Adolescents
3
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing 34
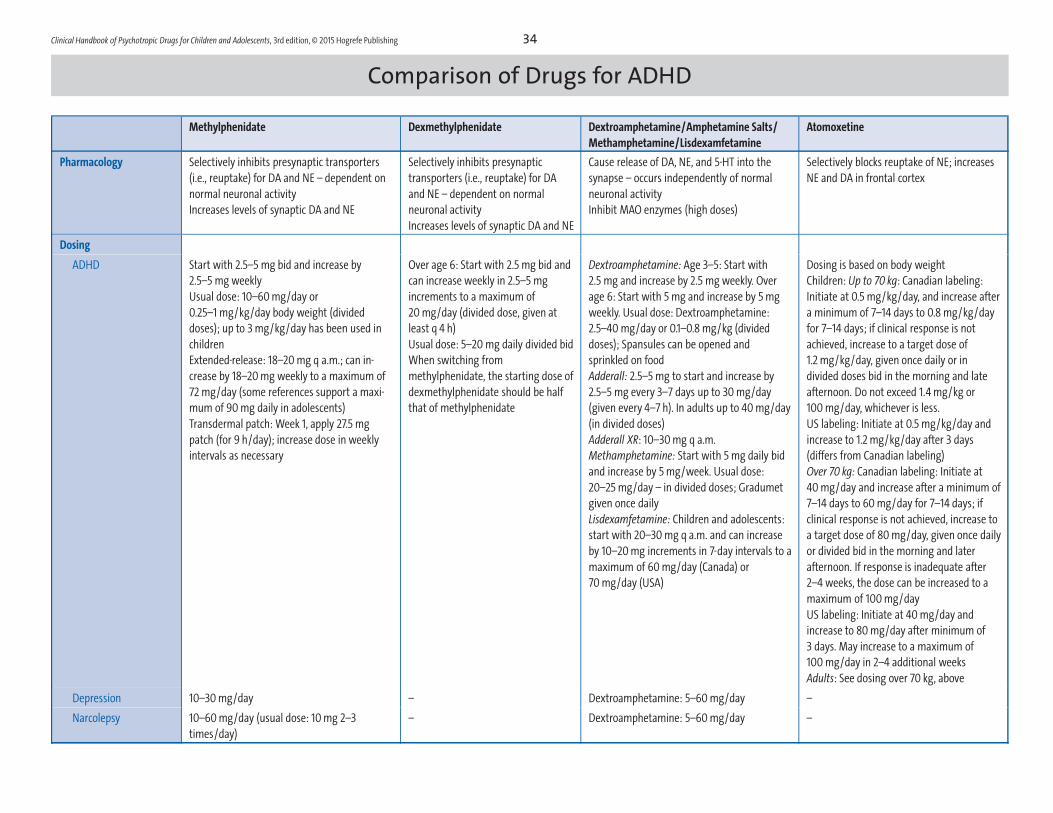
Comparison of Drugs for ADHD
Methylphenidate Dexmethylphenidate Dextroamphetamine/Amphetamine Salts/
Methamphetamine/Lisdexamfetamine
Atomoxetine
Pharmacology Selectively inhibits presynaptic transporters
(i.e., reuptake) for DA and NE – dependent on
normal neuronal activity
Increases levels of synaptic DA and NE
Selectively inhibits presynaptic
transporters (i.e., reuptake) for DA
and NE – dependent on normal
neuronal activity
Increases levels of synaptic DA and NE
Cause release of DA, NE, and 5-HT into the
synapse – occurs independently of normal
neuronal activity
Inhibit MAO enzymes (high doses)
Selectively blocks reuptake of NE; increases
NE and DA in frontal cortex
Dosing
ADHD Start with 2.5–5 mg bid and increase by
2.5–5 mg weekly
Usual dose: 10–60 mg/day or
0.25–1 mg/kg/day body weight (divided
doses); up to 3 mg/kg/day has been used in
children
Extended-release: 18–20 mg q a.m.; can in-
crease by 18–20 mg weekly to a maximum of
72 mg/day (some references support a maxi-
mum of 90 mg daily in adolescents)
Transdermal patch: Week 1, apply 27.5 mg
patch (for 9 h/day); increase dose in weekly
intervals as necessary
Over age 6: Start with 2.5 mg bid and
can increase weekly in 2.5–5 mg
increments to a maximum of
20 mg/day (divided dose, given at
least q 4 h)
Usual dose: 5–20 mg daily divided bid
When switching from
methylphenidate, the starting dose of
dexmethylphenidate should be half
that of methylphenidate
Dextroamphetamine: Age 3–5: Start with
2.5 mg and increase by 2.5 mg weekly. Over
age 6: Start with 5 mg and increase by 5 mg
weekly. Usual dose: Dextroamphetamine:
2.5–40 mg/day or 0.1–0.8 mg/kg (divided
doses); Spansules can be opened and
sprinkled on food
Adderall: 2.5–5 mg to start and increase by
2.5–5 mg every 3–7 days up to 30 mg/day
(given every 4–7 h). In adults up to 40 mg/day
(in divided doses)
Adderall XR: 10–30 mg q a.m.
Methamphetamine: Start with 5 mg daily bid
and increase by 5 mg/week. Usual dose:
20–25 mg/day – in divided doses; Gradumet
given once daily
Lisdexamfetamine: Children and adolescents:
start with 20–30 mg q a.m. and can increase
by 10–20 mg increments in 7-day intervals to a
maximum of 60 mg/day (Canada) or
70 mg/day (USA)
Dosing is based on body weight
Children: Up to 70 kg: Canadian labeling:
Initiate at 0.5 mg/kg/day, and increase after
a minimum of 7–14 days to 0.8 mg/kg/day
for 7–14 days; if clinical response is not
achieved, increase to a target dose of
1.2 mg/kg/day, given once daily or in
divided doses bid in the morning and late
afternoon. Do not exceed 1.4 mg/kg or
100 mg/day, whichever is less.
US labeling: Initiate at 0.5 mg/kg/day and
increase to 1.2 mg/kg/day after 3 days
(differs from Canadian labeling)
Over 70 kg: Canadian labeling: Initiate at
40 mg/day and increase after a minimum of
7–14 days to 60 mg/day for 7–14 days; if
clinical response is not achieved, increase to
a target dose of 80 mg/day, given once daily
or divided bid in the morning and later
afternoon. If response is inadequate after
2–4 weeks, the dose can be increased to a
maximum of 100 mg/day
US labeling: Initiate at 40 mg/day and
increase to 80 mg/day after minimum of
3 days. May increase to a maximum of
100 mg/day in 2–4 additional weeks
Adults: See dosing over 70 kg, above
Depression 10–30 mg/day – Dextroamphetamine: 5–60 mg/day –
Narcolepsy 10–60 mg/day (usual dose: 10 mg 2–3
times/day)
– Dextroamphetamine: 5–60 mg/day –
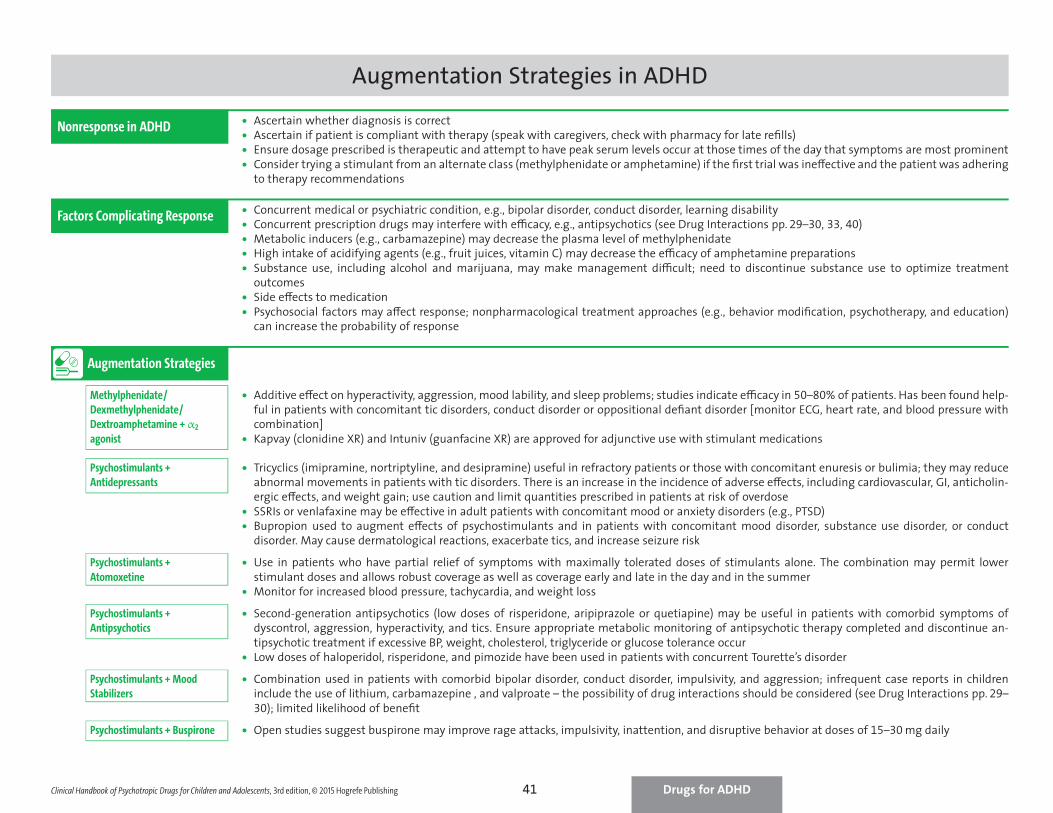
Augmentation Strategies in ADHD
Nonresponse in ADHD • Ascertain whether diagnosis is correct• Ascertain if patient is compliant with therapy (speak with caregivers, check with pharmacy for late rešlls)• Ensure dosage prescribed is therapeutic and attempt to have peak serum levels occur at those times of the day that symptoms are most prominent• Consider trying a stimulant from an alternate class (methylphenidate or amphetamine) if the šrst trial was ine−ective and the patient was adhering
to therapy recommendations
Factors Complicating Response • Concurrent medical or psychiatric condition, e.g., bipolar disorder, conduct disorder, learning disability• Concurrent prescription drugs may interfere with e³cacy, e.g., antipsychotics (see Drug Interactions pp. 29–30, 33, 40)• Metabolic inducers (e.g., carbamazepine) may decrease the plasma level of methylphenidate• High intake of acidifying agents (e.g., fruit juices, vitamin C) may decrease the e³cacy of amphetamine preparations• Substance use, including alcohol and marijuana, may make management di³cult; need to discontinue substance use to optimize treatment
outcomes• Side e−ects to medication• Psychosocial factors may a−ect response; nonpharmacological treatment approaches (e.g., behavior modišcation, psychotherapy, and education)
can increase the probability of response
Augmentation Strategies
Methylphenidate/
Dexmethylphenidate/
Dextroamphetamine + α2
agonist
• Additive e−ect on hyperactivity, aggression, mood lability, and sleep problems; studies indicate e³cacy in 50–80% of patients. Has been found help-ful in patients with concomitant tic disorders, conduct disorder or oppositional dešant disorder [monitor ECG, heart rate, and blood pressure withcombination]
• Kapvay (clonidine XR) and Intuniv (guanfacine XR) are approved for adjunctive use with stimulant medications
Psychostimulants +
Antidepressants
• Tricyclics (imipramine, nortriptyline, and desipramine) useful in refractory patients or those with concomitant enuresis or bulimia; they may reduceabnormal movements in patients with tic disorders. There is an increase in the incidence of adverse e−ects, including cardiovascular, GI, anticholin-ergic e−ects, and weight gain; use caution and limit quantities prescribed in patients at risk of overdose
• SSRIs or venlafaxine may be e−ective in adult patients with concomitant mood or anxiety disorders (e.g., PTSD)• Bupropion used to augment e−ects of psychostimulants and in patients with concomitant mood disorder, substance use disorder, or conduct
disorder. May cause dermatological reactions, exacerbate tics, and increase seizure risk
Psychostimulants +
Atomoxetine
• Use in patients who have partial relief of symptoms with maximally tolerated doses of stimulants alone. The combination may permit lowerstimulant doses and allows robust coverage as well as coverage early and late in the day and in the summer
• Monitor for increased blood pressure, tachycardia, and weight loss
Psychostimulants +
Antipsychotics
• Second-generation antipsychotics (low doses of risperidone, aripiprazole or quetiapine) may be useful in patients with comorbid symptoms ofdyscontrol, aggression, hyperactivity, and tics. Ensure appropriate metabolic monitoring of antipsychotic therapy completed and discontinue an-tipsychotic treatment if excessive BP, weight, cholesterol, triglyceride or glucose tolerance occur
• Low doses of haloperidol, risperidone, and pimozide have been used in patients with concurrent Tourette’s disorder
Psychostimulants + Mood
Stabilizers
• Combination used in patients with comorbid bipolar disorder, conduct disorder, impulsivity, and aggression; infrequent case reports in childreninclude the use of lithium, carbamazepine , and valproate – the possibility of drug interactions should be considered (see Drug Interactions pp. 29–30); limited likelihood of benešt
Psychostimulants + Buspirone • Open studies suggest buspirone may improve rage attacks, impulsivity, inattention, and disruptive behavior at doses of 15–30 mg daily
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing Drugs for ADHD41
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing 44
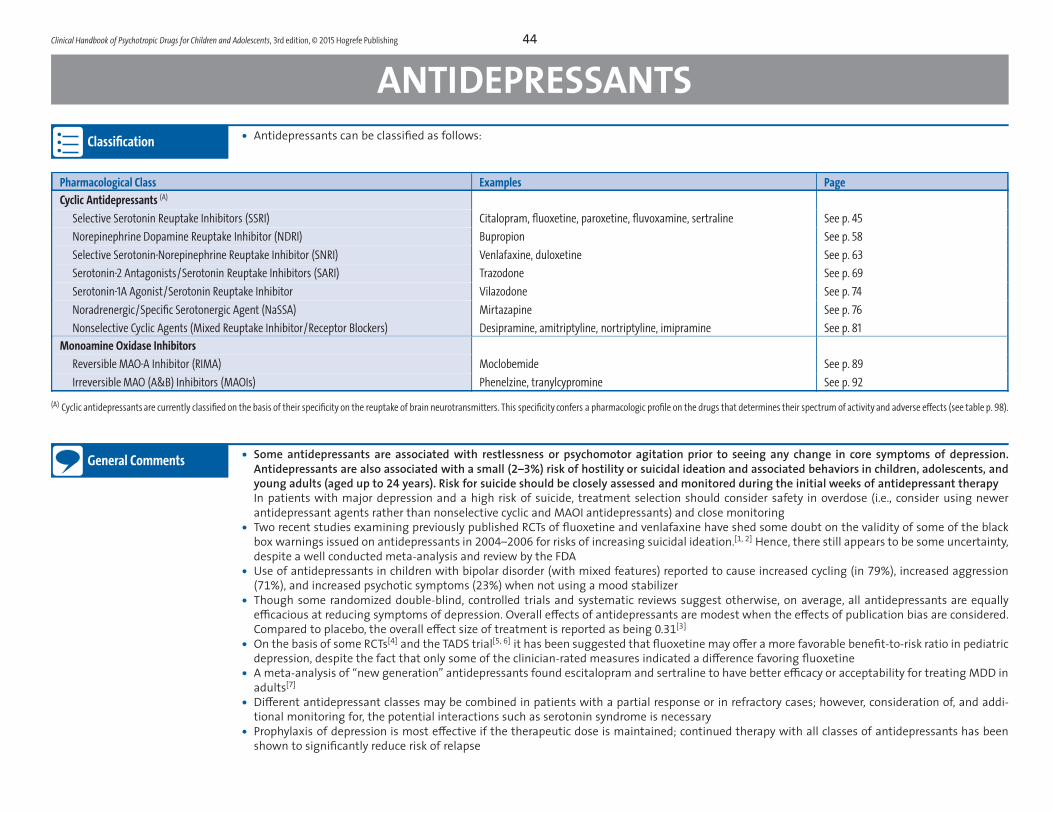
ANTIDEPRESSANTSClassification • Antidepressants can be classišed as follows:
Pharmacological Class Examples Page
Cyclic Antidepressants (A)
Selective Serotonin Reuptake Inhibitors (SSRI) Citalopram, fluoxetine, paroxetine, fluvoxamine, sertraline See p. 45
Norepinephrine Dopamine Reuptake Inhibitor (NDRI) Bupropion See p. 58
Selective Serotonin-Norepinephrine Reuptake Inhibitor (SNRI) Venlafaxine, duloxetine See p. 63
Serotonin-2 Antagonists/Serotonin Reuptake Inhibitors (SARI) Trazodone See p. 69
Serotonin-1A Agonist/Serotonin Reuptake Inhibitor Vilazodone See p. 74
Noradrenergic/Specific Serotonergic Agent (NaSSA) Mirtazapine See p. 76
Nonselective Cyclic Agents (Mixed Reuptake Inhibitor/Receptor Blockers) Desipramine, amitriptyline, nortriptyline, imipramine See p. 81
Monoamine Oxidase Inhibitors
Reversible MAO-A Inhibitor (RIMA) Moclobemide See p. 89
Irreversible MAO (A&B) Inhibitors (MAOIs) Phenelzine, tranylcypromine See p. 92
(A) Cyclic antidepressants are currently classified on the basis of their specificity on the reuptake of brain neurotransmitters. This specificity confers a pharmacologic profile on the drugs that determines their spectrum of activity and adverse effects (see table p. 98).
General Comments• Some antidepressants are associated with restlessness or psychomotor agitation prior to seeing any change in core symptoms of depression.
Antidepressants are also associated with a small (2–3%) risk of hostility or suicidal ideation and associated behaviors in children, adolescents, andyoung adults (aged up to 24 years). Risk for suicide should be closely assessed and monitored during the initial weeks of antidepressant therapyIn patients with major depression and a high risk of suicide, treatment selection should consider safety in overdose (i.e., consider using newerantidepressant agents rather than nonselective cyclic and MAOI antidepressants) and close monitoring
• Two recent studies examining previously published RCTs of ¦uoxetine and venlafaxine have shed some doubt on the validity of some of the blackbox warnings issued on antidepressants in 2004–2006 for risks of increasing suicidal ideation.[1, 2] Hence, there still appears to be some uncertainty,despite a well conducted meta-analysis and review by the FDA
• Use of antidepressants in children with bipolar disorder (with mixed features) reported to cause increased cycling (in 79%), increased aggression(71%), and increased psychotic symptoms (23%) when not using a mood stabilizer
• Though some randomized double-blind, controlled trials and systematic reviews suggest otherwise, on average, all antidepressants are equallye³cacious at reducing symptoms of depression. Overall e−ects of antidepressants are modest when the e−ects of publication bias are considered.Compared to placebo, the overall e−ect size of treatment is reported as being 0.31
[3]
• On the basis of some RCTs[4] and the TADS trial[5, 6] it has been suggested that ¦uoxetine may o−er a more favorable benešt-to-risk ratio in pediatricdepression, despite the fact that only some of the clinician-rated measures indicated a di−erence favoring ¦uoxetine
• A meta-analysis of “new generation” antidepressants found escitalopram and sertraline to have better e³cacy or acceptability for treating MDD inadults[7]
• Di−erent antidepressant classes may be combined in patients with a partial response or in refractory cases; however, consideration of, and addi-tional monitoring for, the potential interactions such as serotonin syndrome is necessary
• Prophylaxis of depression is most e−ective if the therapeutic dose is maintained; continued therapy with all classes of antidepressants has beenshown to signišcantly reduce risk of relapse
• Epidemiological studies of various designs have reported that antidepressant prescribing has declined following the 2004 increased suicidalitywarnings, however, other studies examining prescribing data from 1998 to 2007 suggest that prescription rates of antidepressants have notdecreased despite the warnings[8]
• The Treatment of Adolescent Suicide Attempters study, examined SSRI treatment, cognitive-behavioral therapy (CBT) plus suicide prevention, ora combination in 124 adolescents with moderate to severe depressive symptoms who had previously attempted suicide. After six months oftreatment, 22% taking an SSRI had a suicide-related event compared with 6.7% not on a SSRI[9]
• Tolerance (tachyphylaxis or “poop-out” syndrome) has been reported in 10–20% of patients on various antidepressants, despite adherence totherapy. Possible explanations include adaptations in the CNS, increase in disease severity or pathogenesis, loss of placebo e−ect, unrecognizedrapid-cycling, incorrect diagnosis, comorbid substance use, anxiety disorders, ADHD or eating disorders. [Check compliance with therapy; dosageadjustment may help; switching to an alternate antidepressant (p.107) or augmentation strategies (p. 109) have also been tried]
• A 2013 systematic review in depressed and anxious youths taking antidepressants demonstrated that the overall rate of activation-related orarousal adverse events of treated youths was 3–10 times higher than for those assigned to placebo.[10] Given the connection suggested betweenthe arousal adverse events and potential for suicidality, this šnding supports recommendations for close monitoring for arousal, agitation, and riskfor suicidality when youths are prescribed antidepressants
Therapeutic Effects • Elevation of mood, improved appetite and sleep patterns, increased physical activity, improved clarity of thinking, better memory; decreasedfeelings of guilt, worthlessness, helplessness, inadequacy, decrease in delusional preoccupation and ambivalence
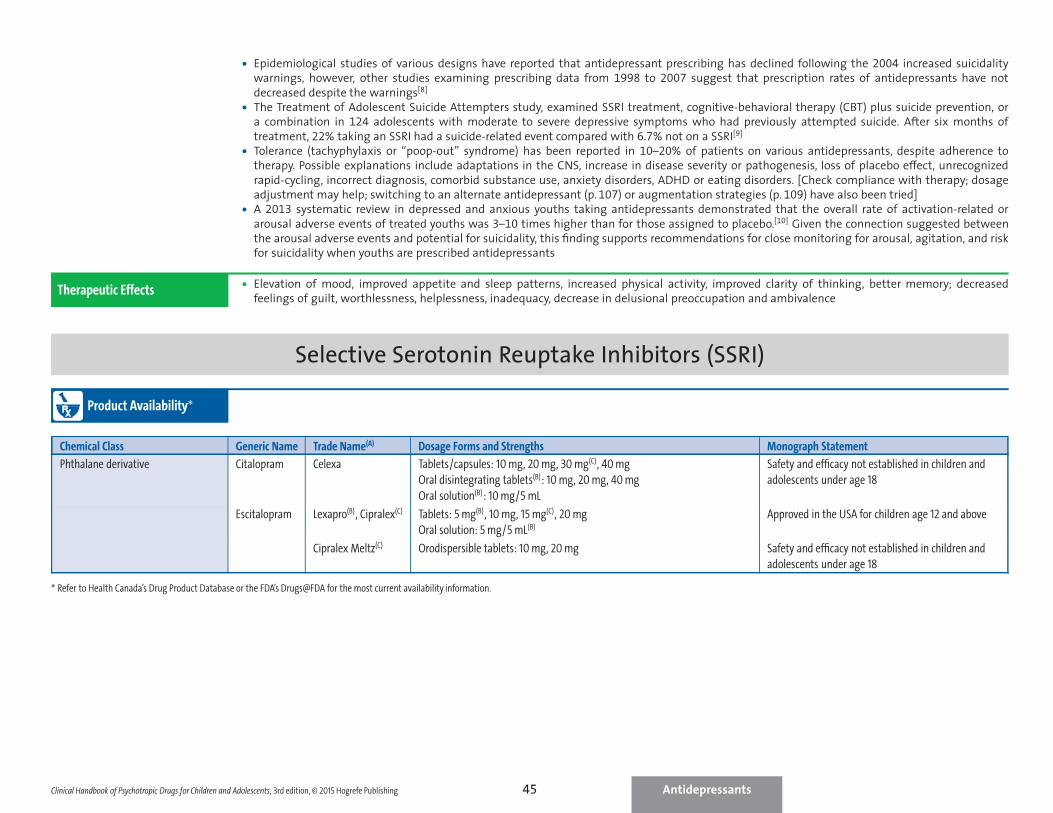
Selective Serotonin Reuptake Inhibitors (SSRI)
Product Availability∗
Chemical Class Generic Name Trade Name(A) Dosage Forms and Strengths Monograph Statement
Phthalane derivative Citalopram Celexa Tablets/capsules: 10 mg, 20 mg, 30 mg(C), 40 mg
Oral disintegrating tablets(B): 10 mg, 20 mg, 40 mg
Oral solution(B): 10 mg/5 mL
Safety and efficacy not established in children and
adolescents under age 18
Escitalopram Lexapro(B), Cipralex(C) Tablets: 5 mg(B), 10 mg, 15 mg(C), 20 mg
Oral solution: 5 mg/5 mL(B)
Approved in the USA for children age 12 and above
Cipralex Meltz(C) Orodispersible tablets: 10 mg, 20 mg Safety and efficacy not established in children and
adolescents under age 18
∗ Refer to Health Canada’s Drug Product Database or the FDA’s Drugs@FDA for the most current availability information.
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing Antidepressants45

Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing 46
Selective Serotonin Reuptake Inhibitors (SSRI) (cont.)Chemical Class Generic Name Trade Name(A) Dosage Forms and Strengths Monograph Statement
Bicyclic Fluoxetine Prozac, Sarafem(B) Capsules: 10 mg, 20 mg, 40 mg(B)
Tablets(B): 10 mg, 15 mg, 20 mg, 60 mg
Oral solution: 20 mg/5 mL
Approved in the USA for children age 7 and above
Prozac Weekly(B) Delayed-release pellets 90 mg Safety and efficacy not established in pediatric
patients under age 7 in obsessive-compulsive
disorder and under age 8 in major depressive disorder
Fluoxetine/olanzapine Symbyax(B) Capsules: Fluoxetine 25mg with 3 mg, 6 mg or 12 mg olanzapine;
fluoxetine 50 mg with 6 mg or 12 mg olanzapine
Approved in the USA for children age 10 and above
(safety and efficacy for acute treatment of depressive
episodes in bipolar I disorder established in patients
age 10–17 in a single 8-week randomized,
placebo-controlled clinical trial)
Monocyclic Fluvoxamine Luvox Tablets: 25 mg(B), 50 mg, 100 mg Approved in the USA for children age 8 and above
Luvox CR Extended-release capsules(B): 100mg, 150mg
Phenylpiperidine Paroxetine hydrochloride Paxil Tablets: 10 mg, 20 mg, 30 mg, 40 mg
Oral suspension(B): 10 mg/5 mL
Safety and efficacy not established in children and
adolescents under age 18
Paxil CR Controlled-release tablets: 12.5 mg, 25 mg, 37.5 mg(B)
Paroxetine mesylate(B) Pexeva Tablets(B): 10 mg, 20 mg, 30 mg, 40 mg
Tetrahydronaphthylmethylamine Sertraline Zoloft Capsules(C)/tablets(B): 25 mg, 50 mg, 100 mg, 150mg(B), 200mg(B)
Oral solution: 20 mg/mL(B)
Approved in the USA for children age 6 and above
(A) Generic preparations may be available, (B) Not marketed in Canada, (C) Not marketed in the USA
Indications‡
( approved)
In children and adolescents:Depression (age 8 and above: ¦uoxetine – USA; age 12 and above: escitalopram - USA)Bipolar depression (age 10 and above: ¦uoxetine/olanzapine combination - USA)Obsessive-compulsive disorder (OCD) (USA: sertraline – age 6 and above, ¦uoxetine – age 7 and above, ¦uvoxamine – age 8 and above) USA)
• No SSRIs are approved for use in children and adolescents in Canada• SSRIs have been used in the treatment of depression, dysthymia, social anxiety disorder, anxiety, panic disorder, bulimia, OCD, Tourette’s disorder,
and ADHD; preliminary data suggest e³cacy in some children with autism spectrum disorder and selective mutism
In adults:Major depressive disorder (MDD) (all – Canada; citalopram, escitalopram, ¦uoxetine, paroxetine, sertraline – USA)MDD, recurrent: ProphylaxisBulimia nervosa (¦uoxetine, sertraline)Obsessive-compulsive disorder (OCD) (¦uvoxamine, ¦uoxetine, paroxetine, escitalopram (Canada only), sertraline)Panic disorder with or without agoraphobia (paroxetine, sertraline, ¦uoxetine)Social anxiety disorder (paroxetine, sertraline)Posttraumatic stress disorder (PTSD) (paroxetine, sertraline)
‡ Indications listed here do not necessarily apply to all SSRIs or all countries. Please refer to a country’s regulatory database (e.g., US Food and Drug Administration, Health Canada Drug Product Database) for themost current availability information and indications
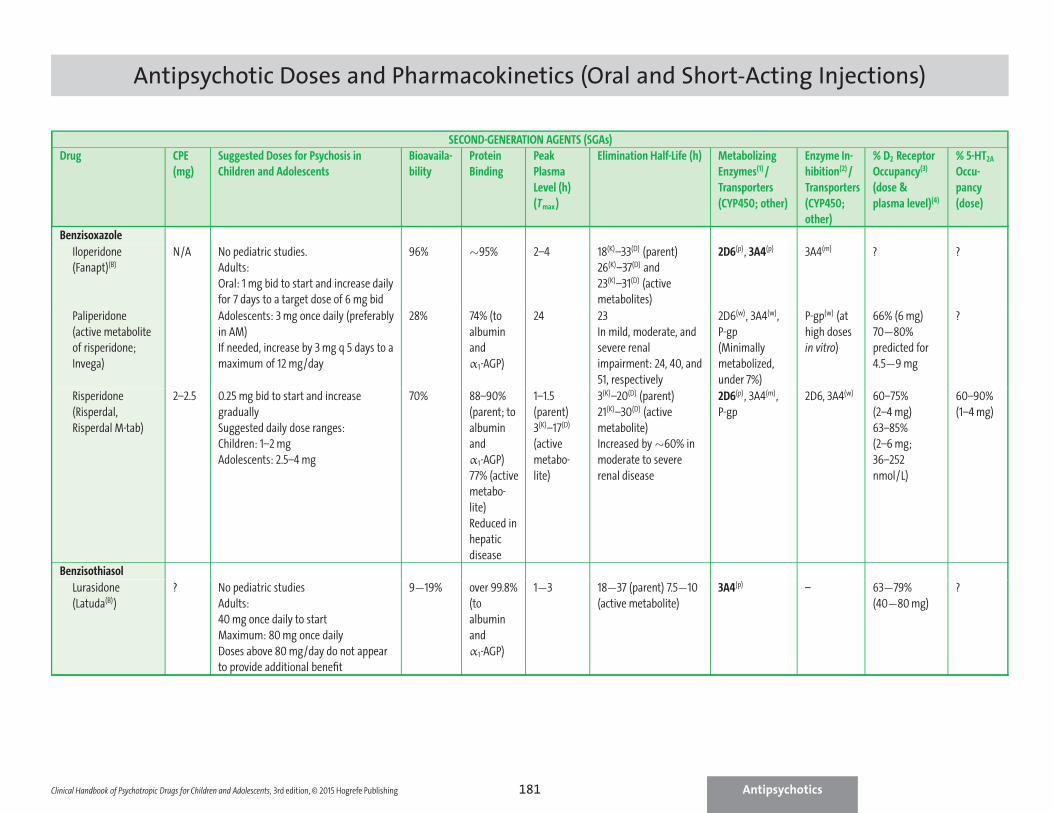
Antipsychotic Doses and Pharmacokinetics (Oral and Short-Acting Injections)
SECOND-GENERATION AGENTS (SGAs)
Drug CPE
(mg)
Suggested Doses for Psychosis in
Children and Adolescents
Bioavaila-
bility
Protein
Binding
Peak
Plasma
Level (h)
(Tmax)
Elimination Half-Life (h) Metabolizing
Enzymes(1)/
Transporters
(CYP450; other)
Enzyme In-
hibition(2)/
Transporters
(CYP450;
other)
% D2 Receptor
Occupancy(3)
(dose &
plasma level)(4)
% 5-HT2A
Occu-
pancy
(dose)
Benzisoxazole
Iloperidone
(Fanapt)(B)
N/A No pediatric studies.
Adults:
Oral: 1 mg bid to start and increase daily
for 7 days to a target dose of 6 mg bid
96% ∼95% 2–4 18(K)–33(D) (parent)
26(K)–37(D) and
23(K)–31(D) (active
metabolites)
2D6(p), 3A4(p) 3A4(m) ? ?
Paliperidone
(active metabolite
of risperidone;
Invega)
Adolescents: 3 mg once daily (preferably
in AM)
If needed, increase by 3 mg q 5 days to a
maximum of 12 mg/day
28% 74% (to
albumin
and
α1-AGP)
24 23
In mild, moderate, and
severe renal
impairment: 24, 40, and
51, respectively
2D6(w), 3A4(w),
P-gp
(Minimally
metabolized,
under 7%)
P-gp(w) (at
high doses
in vitro)
66% (6 mg)
70−80%
predicted for
4.5−9 mg
?
Risperidone
(Risperdal,
Risperdal M-tab)
2–2.5 0.25 mg bid to start and increase
gradually
Suggested daily dose ranges:
Children: 1–2 mg
Adolescents: 2.5–4 mg
70% 88–90%
(parent; to
albumin
and
α1-AGP)
77% (active
metabo-
lite)
Reduced in
hepatic
disease
1–1.5
(parent)
3(K)–17(D)
(active
metabo-
lite)
3(K)–20(D) (parent)
21(K)–30(D) (active
metabolite)
Increased by ∼60% in
moderate to severe
renal disease
2D6(p), 3A4(m),
P-gp
2D6, 3A4(w) 60–75%
(2–4 mg)
63–85%
(2–6 mg;
36–252
nmol/L)
60–90%
(1–4 mg)
Benzisothiasol
Lurasidone
(Latuda(B))
? No pediatric studies
Adults:
40 mg once daily to start
Maximum: 80 mg once daily
Doses above 80 mg/day do not appear
to provide additional benefit
9−19% over 99.8%
(to
albumin
and
α1-AGP)
1−3 18−37 (parent) 7.5−10
(active metabolite)
3A4(p) – 63−79%
(40−80 mg)
?
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing Antipsychotics181
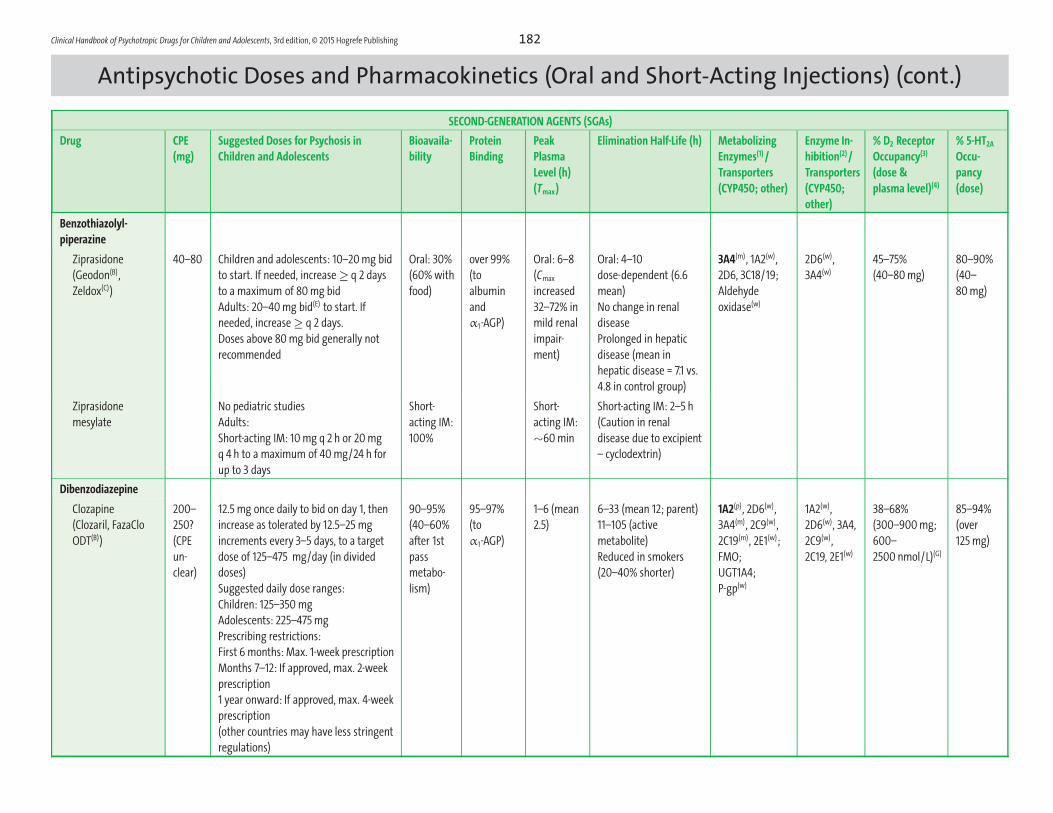
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing 182
Antipsychotic Doses and Pharmacokinetics (Oral and Short-Acting Injections) (cont.)SECOND-GENERATION AGENTS (SGAs)
Drug CPE
(mg)
Suggested Doses for Psychosis in
Children and Adolescents
Bioavaila-
bility
Protein
Binding
Peak
Plasma
Level (h)
(Tmax)
Elimination Half-Life (h) Metabolizing
Enzymes(1)/
Transporters
(CYP450; other)
Enzyme In-
hibition(2)/
Transporters
(CYP450;
other)
% D2 Receptor
Occupancy(3)
(dose &
plasma level)(4)
% 5-HT2A
Occu-
pancy
(dose)
Benzothiazolyl-
piperazine
Ziprasidone
(Geodon(B),
Zeldox(C))
40–80 Children and adolescents: 10–20 mg bid
to start. If needed, increase ≥ q 2 days
to a maximum of 80 mg bid
Adults: 20–40 mg bid(E) to start. If
needed, increase ≥ q 2 days.
Doses above 80 mg bid generally not
recommended
Oral: 30%
(60% with
food)
over 99%
(to
albumin
and
α1-AGP)
Oral: 6–8
(Cmax
increased
32–72% in
mild renal
impair-
ment)
Oral: 4–10
dose-dependent (6.6
mean)
No change in renal
disease
Prolonged in hepatic
disease (mean in
hepatic disease = 7.1 vs.
4.8 in control group)
3A4(m), 1A2(w),
2D6, 3C18/19;
Aldehyde
oxidase(w)
2D6(w),
3A4(w)
45–75%
(40–80 mg)
80–90%
(40–
80 mg)
Ziprasidone
mesylate
No pediatric studies
Adults:
Short-acting IM: 10 mg q 2 h or 20 mg
q 4 h to a maximum of 40 mg/24 h for
up to 3 days
Short-
acting IM:
100%
Short-
acting IM:
∼60 min
Short-acting IM: 2–5 h
(Caution in renal
disease due to excipient
– cyclodextrin)
Dibenzodiazepine
Clozapine
(Clozaril, FazaClo
ODT(B))
200–
250?
(CPE
un-
clear)
12.5 mg once daily to bid on day 1, then
increase as tolerated by 12.5–25 mg
increments every 3–5 days, to a target
dose of 125–475 mg/day (in divided
doses)
Suggested daily dose ranges:
Children: 125–350 mg
Adolescents: 225–475 mg
Prescribing restrictions:
First 6 months: Max. 1-week prescription
Months 7–12: If approved, max. 2-week
prescription
1 year onward: If approved, max. 4-week
prescription
(other countries may have less stringent
regulations)
90–95%
(40–60%
after 1st
pass
metabo-
lism)
95–97%
(to
α1-AGP)
1–6 (mean
2.5)
6–33 (mean 12; parent)
11–105 (active
metabolite)
Reduced in smokers
(20–40% shorter)
1A2(p), 2D6(w),
3A4(m), 2C9(w),
2C19(m), 2E1(w);
FMO;
UGT1A4;
P-gp(w)
1A2(w),
2D6(w), 3A4,
2C9(w),
2C19, 2E1(w)
38–68%
(300–900 mg;
600–
2500 nmol/L)(G)
85–94%
(over
125 mg)
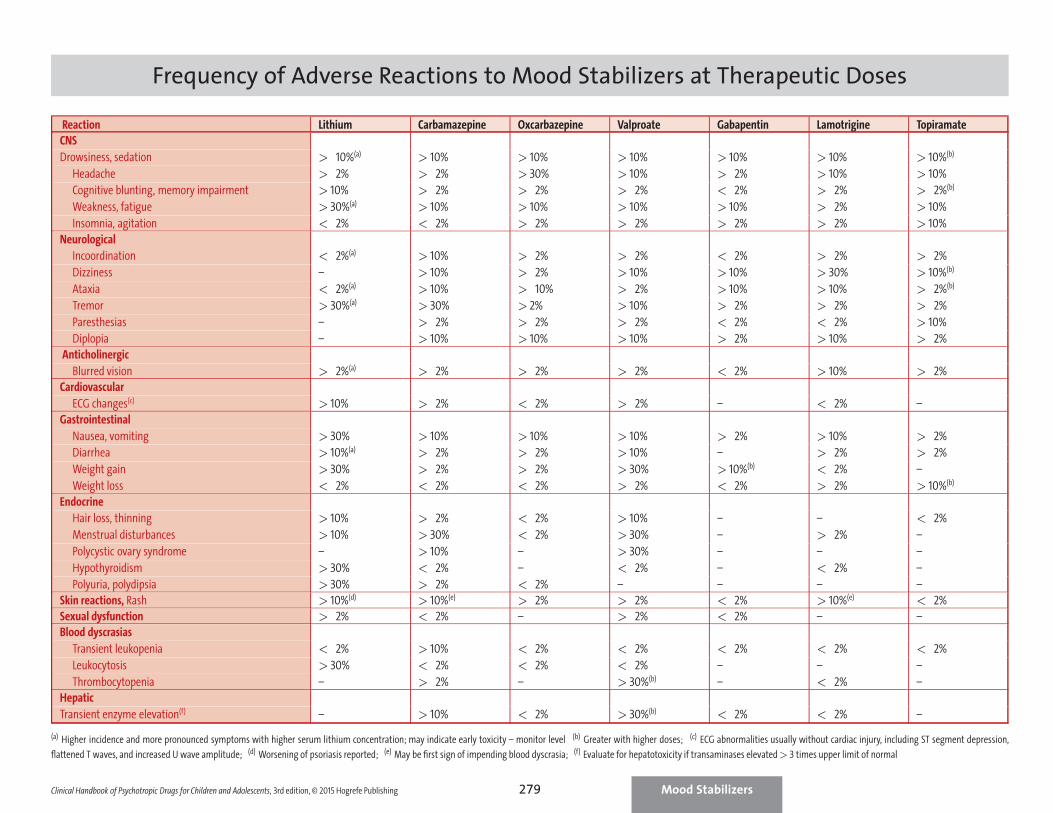
Frequency of Adverse Reactions to Mood Stabilizers at Therapeutic Doses
Reaction Lithium Carbamazepine Oxcarbazepine Valproate Gabapentin Lamotrigine Topiramate
CNS
Drowsiness, sedation > 10%(a) > 10% > 10% > 10% > 10% > 10% > 10%(b)
Headache > 2% > 2% > 30% > 10% > 2% > 10% > 10%
Cognitive blunting, memory impairment > 10% > 2% > 2% > 2% < 2% > 2% > 2%(b)
Weakness, fatigue > 30%(a) > 10% > 10% > 10% > 10% > 2% > 10%
Insomnia, agitation < 2% < 2% > 2% > 2% > 2% > 2% > 10%
Neurological
Incoordination < 2%(a) > 10% > 2% > 2% < 2% > 2% > 2%
Dizziness – > 10% > 2% > 10% > 10% > 30% > 10%(b)
Ataxia < 2%(a) > 10% > 10% > 2% > 10% > 10% > 2%(b)
Tremor > 30%(a) > 30% > 2% > 10% > 2% > 2% > 2%
Paresthesias – > 2% > 2% > 2% < 2% < 2% > 10%
Diplopia – > 10% > 10% > 10% > 2% > 10% > 2%
Anticholinergic
Blurred vision > 2%(a) > 2% > 2% > 2% < 2% > 10% > 2%
Cardiovascular
ECG changes(c) > 10% > 2% < 2% > 2% – < 2% –
Gastrointestinal
Nausea, vomiting > 30% > 10% > 10% > 10% > 2% > 10% > 2%
Diarrhea > 10%(a) > 2% > 2% > 10% – > 2% > 2%
Weight gain > 30% > 2% > 2% > 30% > 10%(b) < 2% –
Weight loss < 2% < 2% < 2% > 2% < 2% > 2% > 10%(b)
Endocrine
Hair loss, thinning > 10% > 2% < 2% > 10% – – < 2%
Menstrual disturbances > 10% > 30% < 2% > 30% – > 2% –
Polycystic ovary syndrome – > 10% – > 30% – – –
Hypothyroidism > 30% < 2% – < 2% – < 2% –
Polyuria, polydipsia > 30% > 2% < 2% – – – –
Skin reactions, Rash > 10%(d) > 10%(e) > 2% > 2% < 2% > 10%(e) < 2%
Sexual dysfunction > 2% < 2% – > 2% < 2% – –
Blood dyscrasias
Transient leukopenia < 2% > 10% < 2% < 2% < 2% < 2% < 2%
Leukocytosis > 30% < 2% < 2% < 2% – – –
Thrombocytopenia – > 2% – > 30%(b) – < 2% –
Hepatic
Transient enzyme elevation(f) – > 10% < 2% > 30%(b) < 2% < 2% –
(a) Higher incidence and more pronounced symptoms with higher serum lithium concentration; may indicate early toxicity – monitor level (b) Greater with higher doses; (c) ECG abnormalities usually without cardiac injury, including ST segment depression,
flattened T waves, and increased U wave amplitude; (d) Worsening of psoriasis reported; (e) May be first sign of impending blood dyscrasia; (f) Evaluate for hepatotoxicity if transaminases elevated > 3 times upper limit of normal
Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, © 2015 Hogrefe Publishing Mood Stabilizers279

3CLINICAL HANDBOOK OF
Psychotropic Drugs
This book is designed to fill a need for a com-prehensive but compact and easy-to-use reference for all mental health professio nals dealing with children and adolescents. This new edition of the widely praised Clinical Handbook summarizes the latest information from the published literature (monograph statements, scientific data, controlled clinical trials, case reports) and clinical experience in compact and easy-to-use charts and bulleted lists for each class of psychotropic drugs used in children and adolescents.
The Clinical Handbook includes for each class of drugs:
Monograph statements on use in children and adolescents
Approved indications in children and adolescents
Off-label indications Findings from open and double-blind studies
Product availability, dosing, pharmacokinetics, adverse effects, precautions, interactions, and other considerations relevant to these age groups.
This 3rd completely revised and expanded edition of the highly acclaimed psychotropic drug reference for all health care professionals dealing with children and adolescents is now more user friendly than ever:
Updated information on psychiatric disorders in children and adolescents (including DSM-V changes)
Packed with unique comparison charts (dosages, side effects, pharmacokinetics, interactions…) that allow you to see at a glance which medication is the most suitable for each patient
Now in full color throughout and with instantly recognizable icons that allow you to find at a glance all the information you seek:
– General information on medications, availability, and indications
– Drug action, dosing, pharmacokinetics, and related areas
– Warnings and precautions
– Patient-related information, such as lab monitoring recommendations, nursing implications, and patient advice
Patient and Caregiver Information Sheets provided as printable pdf files
“A ‘must-have’ for those prescribing psychotropic medications in children and adolescents. It remains by far the most user-friendly and comprehensive handbook available for prescribers, teachers, students, and others working or interested in the field of child and adolescent psychopharmacology.”
Pieter Joost van Wattum, MD, MA, in Journal of Clinical Psychiatry
“If you see children who are placed on psychotropic medications, this books clearly falls into your ‘must-have’ category.”
J.C. Courtney in Child Neuropsychology
“Provides the busy clinician with all the information that is essential for those prescribing a psychotropic drug to a child or adolescent....Very ‘user friendly’... Highly recommended to all clinicians that specialize in treating children and adolescents.”
B.E. Leonard in Human Psychopharmacology
“The main strength of this book is its ability to summarize a large amount of information and make it immediately available at one’s fingertips. The clinician needing facts and needing them fast will enjoy the handbook.”
S. C. Kowalik in Journal of Child and Adolescent Psychopharmacology
“Authoritatively and exhaustively compiles currently available infor-
mation in a user-friendly form. The aim of the Handbook is to be a source
of ‘fast facts’ for the busy clinician...an aim it achieves splendidly.”
M. Gittelman, Editor of International Journal of Mental Health
“Well-researched... An essential reference book [that] all professionals should have... Full of indispensable information and data in a sequenced and logical design.”
P. Shelley in International Journal of Psychiatric Nursing Research
“A useful guide for busy clinicians and one that puts pharmacotherapy
for child and adolescent psychiatry in context.”
Kelly Lai in Hong Kong Journal of Psychiatry
“Well organized... Excellent patient and caregiver information sheets...
Factual information is concisely displayed in tables that educators will
want to share.”
Leslie L. Citrome in Annals of Pharmacotherapy
From the reviews of the previous editions:
ISBN: 978-0-88937-456-0
9 780889 374560
90000
Now also available: The Clinical Handbook of Psychtropic Drugs for Children and Adolescents ONLINE. For details, see http://chpd.hogrefe.com/
for Children and Adolescents


















