
CliniCal Guide - Make it e.max · CliniCal Guide. 2. Contents 3 ... IPS e.max delivers...
44
all ceramic all you need CLINICAL GUIDE
Transcript of CliniCal Guide - Make it e.max · CliniCal Guide. 2. Contents 3 ... IPS e.max delivers...

all ceramic
all you need
CliniCal Guide

2
3Contents
IPS e.max® – all ceramics – all you need
•Onesystemforeveryindication •Indications Practical procedure for restorations with IPS e.max®
•Overview •Tooth–Shadedetermination •Preparation •Die–Shadedetermination •Impression •Cementation •Intraoraladjustments
Clinical cases
•Step-by-step – IPSe.maxlithiumdisilicateveneercementedwithVariolink®Veneer – IPSe.maxlithiumdisilicateinlaycementedwithMultilink®Automix – IPSe.maxlithiumdisilicateanteriorcrowncementedwithMultilink®Automix – IPSe.maxlithiumdisilicateposteriorcrowncementedwithMultilink®Automix – IPSe.maxlithiumdisilicateanteriorbridgecementedwithSpeedCEM® – IPSe.maxzirconiumoxidebridgecementedwithSpeedCEM®
– IPSe.maxlithiumdisilicatehybridabutmentandcrowncementedwithSpeedCEM®
– IPSe.maxlithiumdisilicatehybridabutmentcrown–screwed-in •Startingsituation–Finalresult
Aftercare
Results from more than 10 years of research
4
6
20
40
41
4
IPSe.max® isaninnovativeall-ceramicsystemwhichcoverstheentireall-ceramicindicationrange–fromthinveneerstolong-spanbridges.
IPSe.maxdelivershigh-strengthandhighlyestheticmaterialsforthePressandtheCAD/CAMtechnologies.Thesystemincludestheinnovativelithiumdisilicateglass-ceramicusedmainlyforsingle-toothrestorations,hybridabutmentsandsmallbridges,aswellasthehigh-strengthzirconiumoxideforlong-spanbridges.
All ceramic materials are based on an integrated material and shade concept for restorations as individual as your patients.
all ceramics – all you need
LS2Lithium disilicate glass-ceramic (LS2)
Lithiumdisilicate(LS2)glass-ceramicisideallysuitableforthefabricationofhybridabutments,aswellasmonolithicsingle-toothrestorationsandmayevenbeindicatedfor3-unitbridgesupto thepremolar region. Thepatentedglass-ceramichasbeen tried-and-tested inmillionsofcasessinceitsintroduction.Itisdistinguishedfromallpreviousceramicmaterialsmainlybyitsclearlyhigherstressresistanceanditsoutstandingestheticappearance.
ZrO2Zirconium oxide (ZrO2)
High-strengthzirconiumoxide(ZrO2)reallyprovesitsworthinlong-spanbridges. It isoneofthemostefficientall-ceramicmaterialsfordental-labapplications.Zirconiumoxideischaracter-izedbyitsexcellentbiocompatibilityandlowheatconductivityandcanbeindicatedforsingle-toothrestorationsandupto14-unitbridges.Zirconiumoxidecanbeveneeredwithnano-fluor-apatiteorlithiumdisilicateglass-ceramic.
FAPFluorapatite
Fluorapatite glass-ceramic (FAP)
IPSe.maxCeramisahighlyestheticlayeringceramicfortheIPSe.maxSystem.Thankstotheonecommonlayeringceramic,alltheveneeredIPSe.maxrestorationsexhibitthesamewearpropertiesandsurfacegloss.Zirconium frameworks pressed over with IPS e.max ZirPress, which are either stained orveneered,areanalternativetoconventionallyveneeredframeworks.
Afterall,IPSe.maxstandsforanall-ceramicsystemthatoffersanidealsolutionforallindications,whichnotonlyworksfromamaterialstandpoint,butisalsoconfirmedbyawealthofscientificdata.
Fromthebeginningofitsdevelopmentuntiltotoday,theIPSe.maxSystemhasbeenmonitoredbythescientificcommunityandmanyrenownedexpertshavecontributedtoanexcellentdatabasewiththeirstudies.
Theworldwidesuccessstory,theevergrowingdemand,aswellasmillionsoffabricatedrestorationsaretesta-menttothesuccessandthereliabilityoftheIPSe.maxall-ceramicsystem.
One system for every indication

5Indications
Indications
Cementation
adhesiveself-adhesive/ conventional
Thinveneers0.3mm
–
Variolink®Veneer,Variolink®II
–Veneers –
Occlusalveneers –
Inlays,onlays –
Multilink®Auto-mix,Variolink®II
–
Partialcrowns –
Anterior/posteriorcrowns 1)
SpeedCEM®,Vivaglass®CEM3-unitbridges 2) 1)
Multilink®Automix
4-andmulti-unit bridges
– 1)
Hybridabutments (cementedona Tibase)
–Multilink®Automix
3)
SpeedCEM® 3)4),Vivaglass®CEM3)
Hybridabutment crowns(cementedonaTibase)
– –5) –5)
1) IPS e.max ZirCAD (zirconium oxide) is veneered manually (fluorapatite) or digitally (lithium disilicate). 2) Up to the second premolar 3) For the cementation of the crown on the hybrid abutment 4) Only in conjunction with a suitable bonding agent 5) Hybrid abutment crowns are directly screwed on the implant.
Contraindications
–Verydeepsubgingivalpreparations–Patientswithseverelyreducedresidualdentition–Parafunctions,e.g.bruxism–Provisionalinsertion/trialwearperiod–Anyotherusesnotlistedintheindications
LS2 ZrO2
6
Practical procedure for restorations with
Working steps In the
dental officeIn the
laboratory Ivoclar Vivadent product
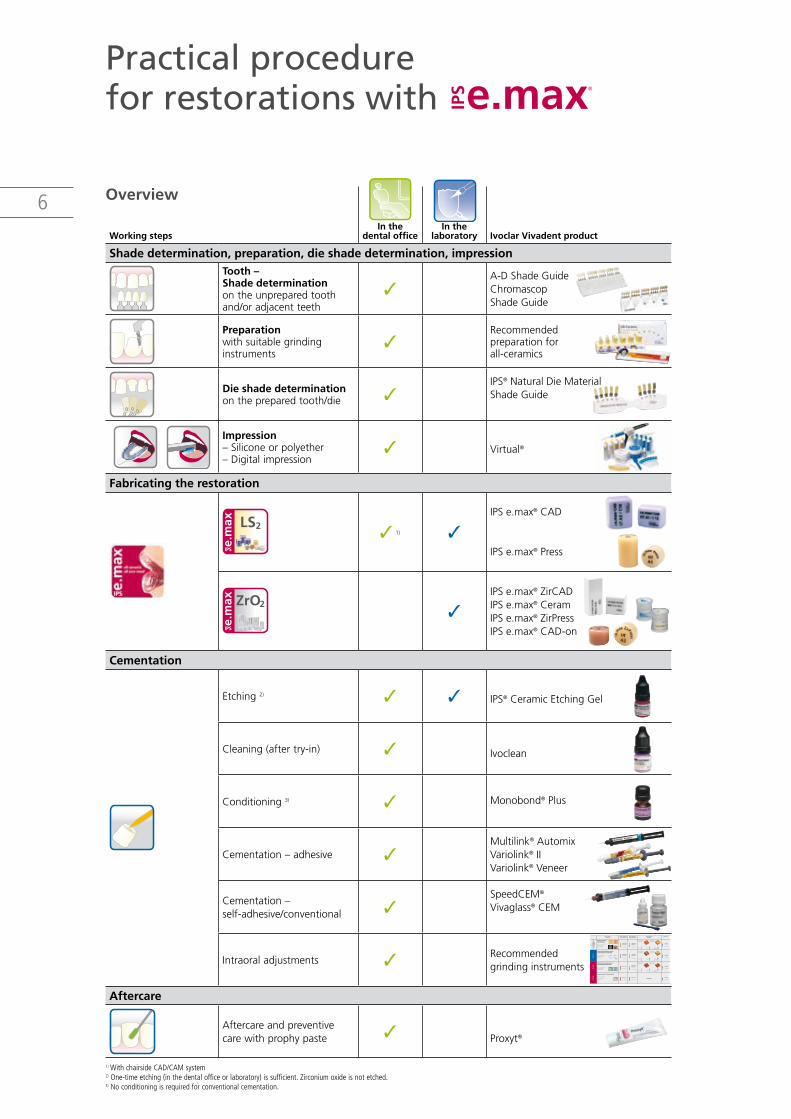
Shade determination, preparation, die shade determination, impression Tooth – Shade determination ontheunpreparedtoothand/oradjacentteeth
A-DShadeGuideChromascop ShadeGuide
Preparation withsuitablegrinding instruments
Recommended preparationfor all-ceramics
Die shade determination onthepreparedtooth/die
IPS®NaturalDieMaterialShadeGuide
LS2
ZrO2
FAPFluor-Apatit
Zirkoniumoxid
Lithiumdisilikat
LS2
ZrO2
FAPFluor-Apatit
Zirkoniumoxid
Lithiumdisilikat
Impression –Siliconeorpolyether–Digitalimpression
Virtual®
Fabricating the restoration
LS2 1)
IPSe.max®CAD
IPSe.max®Press
ZrO2IPSe.max®ZirCADIPSe.max®Ceram IPSe.max®ZirPressIPSe.max®CAD-on
Cementation
Etching2)IPS®CeramicEtchingGel
Cleaning(aftertry-in) Ivoclean
Conditioning3) Monobond®Plus
Cementation–adhesive Multilink®Automix Variolink®II Variolink®Veneer
Cementation– self-adhesive/conventional
SpeedCEM® Vivaglass®CEM
IntraoraladjustmentsRecommended grindinginstruments
Aftercare
Aftercareandpreventivecarewithprophypaste Proxyt®
1) With chairside CAD/CAM system2) One-time etching (in the dental office or laboratory) is sufficient. Zirconium oxide is not etched. 3) No conditioning is required for conventional cementation.
Overview
Layering ceramics /Schichtkeramik
Flexural strength / Biegefestigkeit 80–130 MPa
Type of ceramic /
Keramiktyp
Extensive corrections /
Grosse Korrekturen
Minor corrections /
Geringe Korrekturen
Endo AccessPolishing / Politur
(OptraFine)
extra fine /
extra fein
15–25 µm
extra fine /
extra fein
15–25 µm
medium
<_100 µm
extra fine /
extra fein
15–25 µm
extra fine /
extra fein
15–25 µm
medium
<_100 µm
fine / fein
40–50 µm
extra fine /
extra fein
15–25 µm
medium
<_100 µm
fine / fein
40–50 µm
fine / fein
40–50 µm
medium
<_100 µm
Leucite-reinforced glass-ceramic /Leuzitverstärkte Glasskeramik
Flexural strength / Biegefestigkeit 160 MPa
Lithium disilicate glass-ceramic /
Lithiumdisilikat-Glaskeramik
Flexural strength / Biegefestigkeit 360–400 MPa
Zirconium oxide / Zirkoniumoxid
Flexural strength / Biegefestigkeit 900 MPa
d.SIGN IPS ®
InLine PoM®
IPS
InLine ®IPS
Empress IPS ®
Esthetic Empress IP
S ®
CAD
before polishing / vor der Politur
Finisher F Polisher P High gloss
+ Polishing Paste
after polishing / nach der Politur
before polishing / vor der Politur
Finisher F Polisher P High gloss
+ Polishing Paste
after polishing / nach der Politur
before polishing / vor der Politur
Finisher F Polisher P High gloss
+ Polishing Paste
after polishing / nach der Politur
IPS
e.m
axIP
S In
Line
/IPS
InLi
ne P
oM
IPS
d.SI
GN
Recommended grinding instruments for ceramics – use in the dental practice
Schleifkörperempfehlung für Keramik – Anwendung in der zahnärztlichen Praxis

7
Practical procedure for restoration with IPS e.max | Tooth – Shade determination
Tooth – Shade determination
Optimum integration in theoral cavityof thepatient is theprerequisite fora true-to-natureall-ceramicrestoration.Toachievethis,thefollowingguidelinesandnotesmustbeobservedbyboththedentistandthelaboratory.
Theoverallestheticresultofanall-ceramicrestorationisinfluencedbythefollowingfactors:•Shade of the tooth stump(naturalstump,devitalizedstump,corebuild-up,abutment)• Shade of the cementation material•Shade of the restorative material(frameworkshade,translucency/opacity,brightness,veneer,
characterization)
Shade determination of the natural tooth
– Determinethetoothshadeofthenon-preparedtoothand/ortheadjacentteethaftertoothcleaning.
– Inaddition,determinethecervicalshadeifacrownpreparationisplanned,forexample.
– Determinetheshadeatdaylightandinfrontofaneutralbackground.– Avoidintensivelycolouredclothesand/orlipstickasthesemay
compromisetheresult.– UsetheA-DShadeGuideorChromascopShadeGuide.
8 Preparation
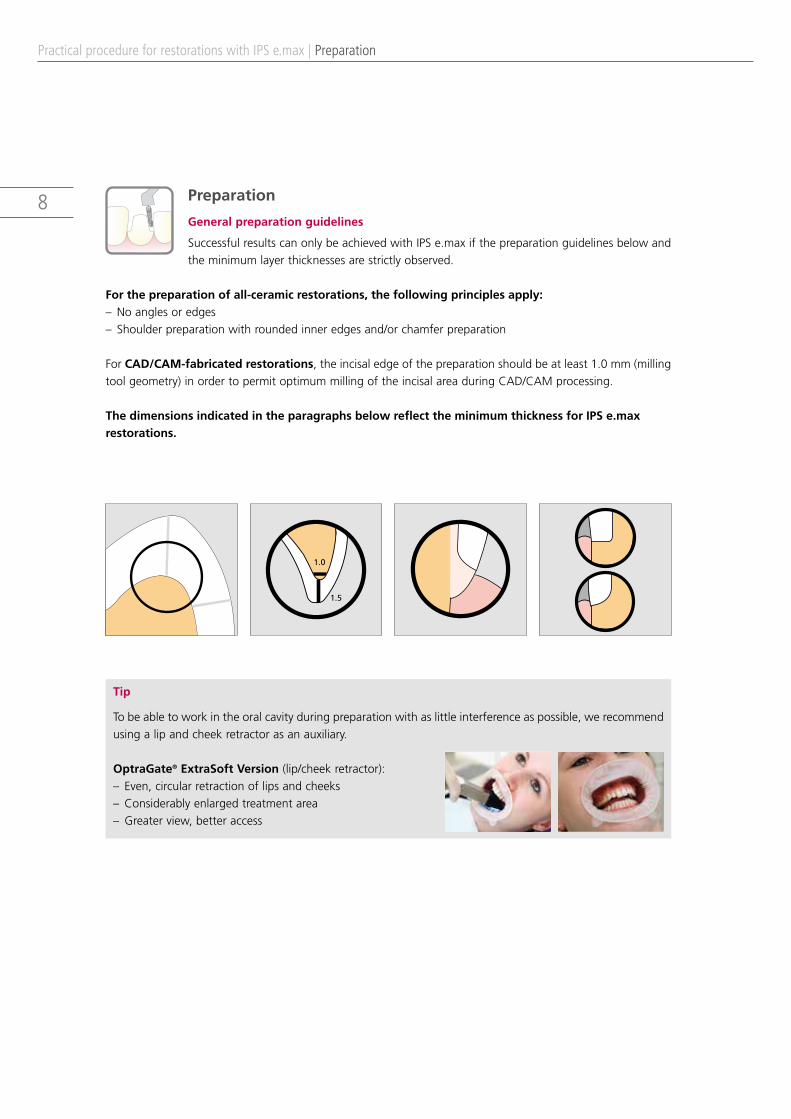
General preparation guidelines
SuccessfulresultscanonlybeachievedwithIPSe.maxifthepreparationguidelinesbelowandtheminimumlayerthicknessesarestrictlyobserved.
For the preparation of all-ceramic restorations, the following principles apply:– Noanglesoredges– Shoulderpreparationwithroundedinneredgesand/orchamferpreparation
ForCAD/CAM-fabricated restorations,theincisaledgeofthepreparationshouldbeatleast1.0mm(millingtoolgeometry)inordertopermitoptimummillingoftheincisalareaduringCAD/CAMprocessing.
The dimensions indicated in the paragraphs below reflect the minimum thickness for IPS e.max restorations.
1.0
1.5
Tip
Tobeabletoworkintheoralcavityduringpreparationwithaslittleinterferenceaspossible,werecommendusingalipandcheekretractorasanauxiliary.
OptraGate® ExtraSoft Version (lip/cheekretractor):–Even,circularretractionoflipsandcheeks– Considerablyenlargedtreatmentarea– Greaterview,betteraccess
Practical procedure for restorations with IPS e.max | Preparation
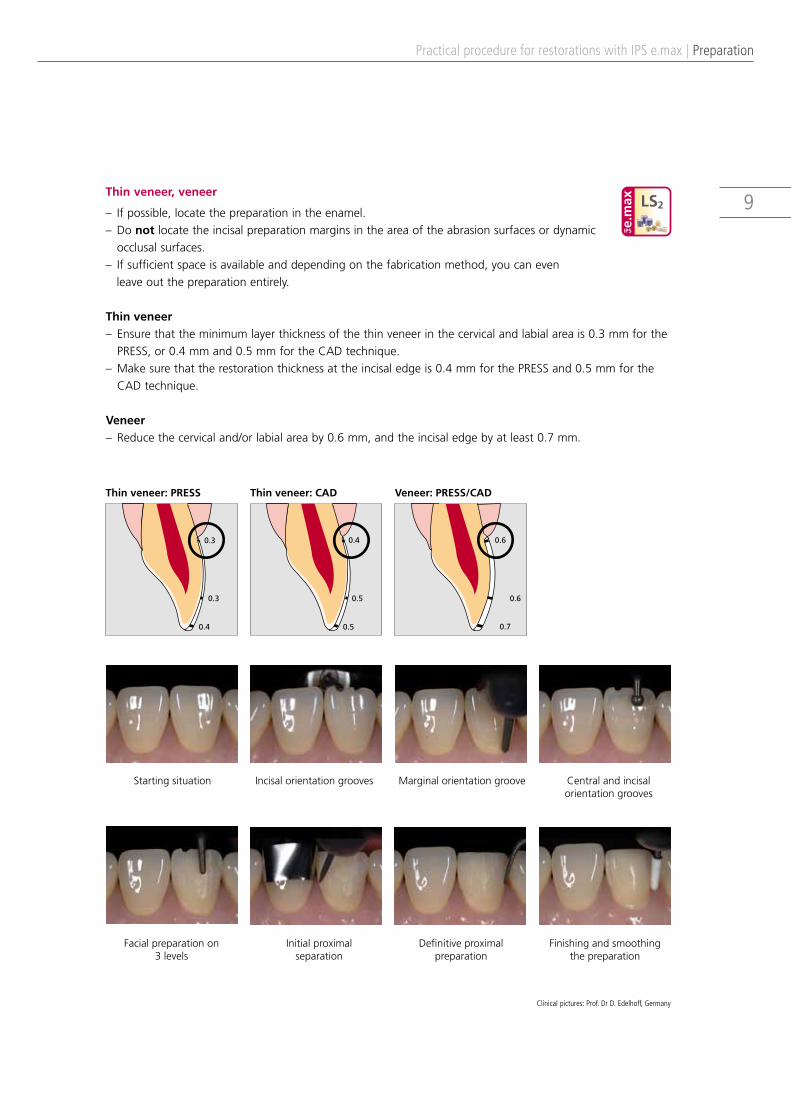
9Thin veneer, veneer
– Ifpossible,locatethepreparationintheenamel.– Donotlocatetheincisalpreparationmarginsintheareaoftheabrasionsurfacesordynamic
occlusalsurfaces.–Ifsufficientspaceisavailableanddependingonthefabricationmethod,youcanevenleaveoutthepreparationentirely.
Thin veneer–Ensurethattheminimumlayerthicknessofthethinveneerinthecervicalandlabialareais0.3mmforthe
PRESS,or0.4mmand0.5mmfortheCADtechnique.–Makesurethattherestorationthicknessattheincisaledgeis0.4mmforthePRESSand0.5mmforthe
CADtechnique.
Veneer–Reducethecervicaland/orlabialareaby0.6mm,andtheincisaledgebyatleast0.7mm.
Startingsituation Incisalorientationgrooves Marginalorientationgroove Centralandincisal orientationgrooves
Facialpreparationon 3levels
Initialproximal separation
Definitiveproximalpreparation
Finishingandsmoothing thepreparation
Practical procedure for restorations with IPS e.max | Preparation
LS2
Thin veneer: PRESS Thin veneer: CAD Veneer: PRESS/CAD
0.3
0.3
0.4 0.5
0.5
0.4 0.6
0.7
0.6
Clinical pictures: Prof. Dr D. Edelhoff, Germany

10
Practical procedure for restorations with IPS e.max | Preparation
Occlusal veneer
−Evenlyreducetheanatomicalshapewhileobservingthestipulatedminimumthicknesses.–Prepareacircularshoulderwithroundedinneredgesorachamferatanangleofapproximately
10to30degrees.–Ensurethatthewidthofthecircularshoulder/chamferisatleast1.0mm.–Reducetheocclusalpartbyatleast1.0mm.
Startingsituation Orientationgroove centralfissure
Orientationgrooves onthecusps
Shortening theocclusalsurface
Creatingthecircular preparationmargin
Proximalpreparation Finishingthepreparation Smoothingthepreparation
1.0 1.0
1.0
1.0
1.0
LS2
Clinical pictures: Prof. Dr D. Edelhoff, Germany
11
Practical procedure for restorations with IPS e.max | Preparation
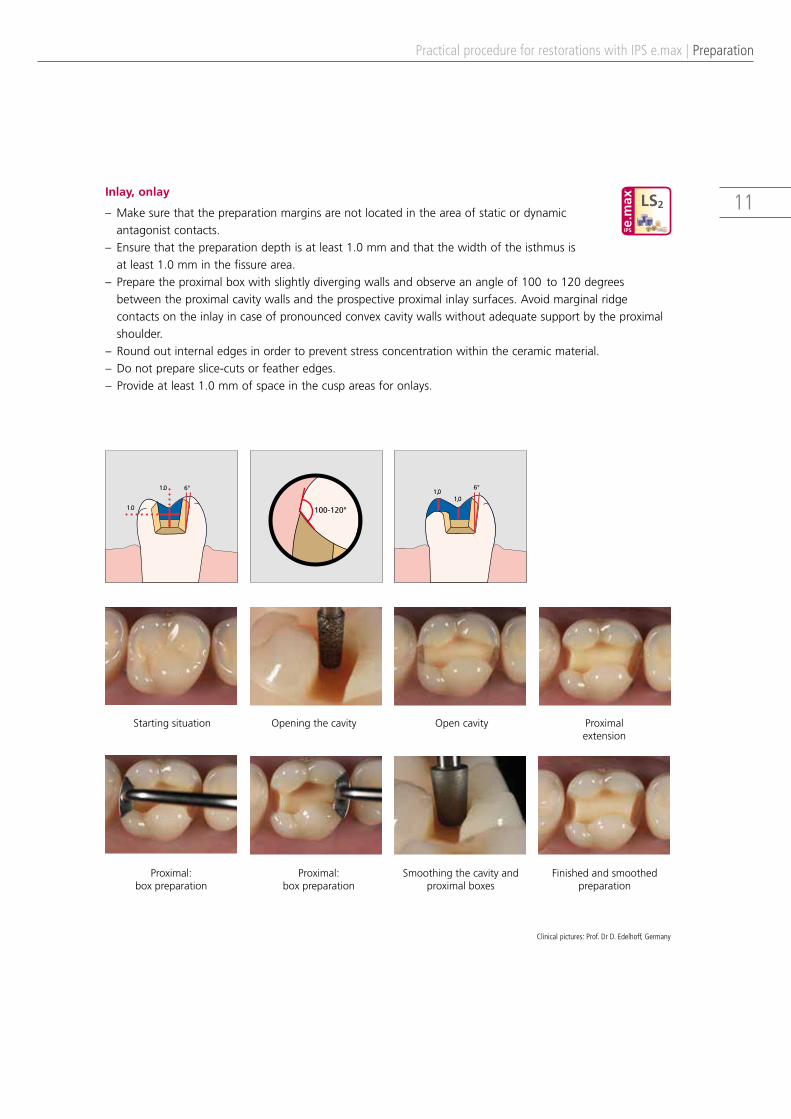
Inlay, onlay
–Makesurethatthepreparationmarginsarenotlocatedintheareaofstaticordynamic antagonistcontacts.
– Ensurethatthepreparationdepthisatleast1.0mmandthatthewidthoftheisthmusis atleast1.0mminthefissurearea.
–Preparetheproximalboxwithslightlydivergingwallsandobserveanangleof100to120degreesbetweentheproximalcavitywallsandtheprospectiveproximalinlaysurfaces.Avoidmarginalridgecontactsontheinlayincaseofpronouncedconvexcavitywallswithoutadequatesupportbytheproximalshoulder.
– Roundoutinternaledgesinordertopreventstressconcentrationwithintheceramicmaterial.– Donotprepareslice-cutsorfeatheredges.– Provideatleast1.0mmofspaceinthecuspareasforonlays.
Startingsituation Openingthecavity Opencavity Proximal extension
Proximal: boxpreparation
Proximal: boxpreparation
Smoothingthecavityandproximalboxes
Finishedandsmoothed preparation
1.0
1.0
6°
100-120°
6°
1,01,0
LS2
Clinical pictures: Prof. Dr D. Edelhoff, Germany

12Partial crown
–Makesurethatthepreparationmarginsarenotlocatedintheareaofstaticordynamic antagonistcontacts.
–Provideatleast1.5mmofspaceinthecuspareas.–Prepareacircularshoulderwithroundedinneredgesorachamferatanangleof
approximately20to30degrees.–Ensurethatthewidthoftheshoulder/chamferisatleast1.0mm.
Startingsituation Openingthecavity, occlusalorientationgrooves
Occlusalandoralreduction ofthecusp
Creatingthecircular preparationmargin
Smoothingthecusps Proximalpreparation Proximalpreparation Finishedandsmoothedpreparation
1.51.5
1.5
1.0
1.5
Practical procedure for restorations with IPS e.max | Preparation
LS2
Clinical pictures: Prof. Dr D. Edelhoff, Germany

13Anterior crown
−Evenlyreducetheanatomicalshapewhileobservingthestipulatedminimum thicknesses.
– Prepareacircularshoulderwithroundedinneredgesorachamferatanangle ofapproximately10to30degrees.Ensurethatthewidthofthecircular shoulder/chamferisatleast1.0mm.
– Reducetheincisalcrownthirdbyatleast1.5mm.–Reducethevestibularand/ororalareabyatleast1.2mm.–Forconventionaland/orself-adhesivecementation,makesurethatthepreparationdemonstratesretentive
surfacesandasufficientpreparationheightofatleast4.0mm.
Startingsituation Incisalorientationgrooves Facialandoral: marginalorientationgroove
Facial:centralandincisalorientationgrooves
Facialpreparationon 3levels:
oralconcavity
Proximalseparation Incisalshortening ofthetoothlength
Finishingandsmoothing thepreparation
1.0
1.0
1.5
1.2 1.2
Practical procedure for restorations with IPS e.max | Preparation
LS2
LS2
ZrO2
ZrO2
Clinical pictures: Prof. Dr D. Edelhoff, Germany

14
Startingsituation Openingthecentralfissure Occlusal orientationgrooves
Vestibularpreparation
Marginalpreparation Proximalpreparation Occlusalpreparation Finishingandsmoothing thepreparation
1.5
1.0 1.0
1.5
1.5
1.5
1.5
6°
1.0 1.0
1.5 1.5
6°
1.2
1.21.2
Practical procedure for restorations with IPS e.max | Preparation
LS2 ZrO2
Posterior crown
−Evenlyreducetheanatomicalshapewhileobservingthestipulatedminimum thicknesses.
–Prepareacircularshoulderwithroundedinneredgesorachamferatan angleofapproximately10to30degrees.Ensurethatthewidthofthecircular shoulder/chamferisatleast1.0mm.
– Reducetheocclusalcrownthirdbyatleast1.5mm.−Reducethebuccalorpalatal/lingualareabyatleast1.5mmforLS2andbyatleast1.2mmforZrO2.–Forconventionaland/orself-adhesivecementation,makesurethatthepreparationdemonstratesretentive
surfacesandasufficientpreparationheightofatleast4.0mm.
LS2 ZrO2
Clinical pictures: Prof. Dr D. Edelhoff, Germany

153-unit bridge
Thepreparationoftheabutmentteethisthesameasforanteriorandposteriorcrowns.
Note regarding lithium disilicate glass-ceramic (LS2) bridges: Giventhedifferentmasticatoryforces,themaximumacceptableponticwidthisdifferentintheanteriorandposteriorregion.
Theponticwidthisdeterminedontheunpreparedtooth.–Intheanteriorregion(uptothecanine),theponticwidthshouldnotexceed11.0mm.–Inthepremolarregion(canineuptothesecondpremolar),theponticwidthshouldnotexceed9.0mm.
Maximum pontic width
9 mmPremolar area
up to the canine
Maximum pontic width
11 mmAnterior region
Bridge (4–andmulti-unitbridges)
−Evenlyreducetheanatomicalshapewhileobservingthestipulatedminimumthicknesses.– Prepareacircularshoulderwithroundedinneredgesorachamferatanangleofapproximately
10to30degrees.−Ensurethatthewidthofthecircularshoulder/chamferisatleast1.0mm.−Reducetheincisalorocclusalcrownthirdbyatleast2.0mm.−Reducethevestibularand/ororalareabyatleast1.5mm.
Practical procedure for restorations with IPS e.max | Preparation
1.0
1.5
1.0
1.5
2.0
1.0
1.5
2.0
1.0 1.0
1.5
2.0
1.5
6°
ZrO2
LS2 ZrO2

16
Practical procedure for restoration with IPS e.max | Die – Shade determination
Die – Shade determination
TheIPSNaturalDieMaterialShadeGuideisusedtodeterminethedieshade.Determiningthedieshadeattheendofthepreparationisaveryimportantstepforthefabrica-tionofall-ceramicrestorations.Especiallywithseverelydiscolouredpreparationsthis isofut-mostimportance.Onlyifthedentistdeterminestheshadeofthepreparationandconsidersitintheselectionoftherestorativematerial,maythedesiredestheticsbeachievedinatargetedfashion.
Shade determination on the prepared tooth/die
– Carryouttheshadedeterminationatdaylight.– Carryouttheshadedeterminationonthepreparedtooth.– UsetheIPSNaturalDieShadeGuide.
Taketheimpressionasusual:– Silicone(e.g.Virtual®) – Polyether– Digitalimpression
Die shade Cementation material Restoration shade Desiredtooth shade
Die – Shade determination
Temporary restoration
Function,phoneticsandestheticsofthepermanentrestorationarepredefinedandmaystillbeadaptedanytime.Forthisessentialtreatmentstep,theTelio® productsystemprovidesamultitudeofapplicationoptions.
Important: The temporary restoration is cemented with a temporary, eugenol-free cement, such as the dual-curing Telio® CS Link.
LS2
ZrO2
FAPFluor-Apatit
Zirkoniumoxid
Lithiumdisilikat
LS2
ZrO2
FAPFluor-Apatit
Zirkoniumoxid
Lithiumdisilikat
Impression

17
Practical procedure for restorations with IPS e.max | Cementation
Cementation
Conditioning of the restoration
Material Lithium disilicate LS2 Zirconium oxide ZrO2
Indication
Thinveneers,veneers,occlusal
veneers,inlays,onlays,partialcrowns
Crownsand3-unitbridges uptothesecondpremolar Crownsandbridges
Cementation method adhesive adhesive self-adhesive/
conventional adhesive self-adhesive/conventional
Blasting – CleaningwithAl2O3atamaximumpressureof1bar
Etching 5%hydrofluoricacid(e.g.IPS®CeramicEtchingGel)20s –
Conditioning Monobond®Plus60s1)
Monobond®Plus60s1)
Cementation system
Variolink®Veneer, Variolink®II, Multilink® Automix
Multilink® Automix
SpeedCEM®
Vivaglass®CEMMultilink® Automix
SpeedCEM®
Vivaglass®CEM
1) With conventional cementation, conditioning is not necessary.
Please observe the corresponding Instructions for Use.
IPS® Ceramic Etching Gel–togenerateretentivebondingsurfacesonglass-ceramics– Itdecisivelyenhancesthebondingeffectbetweenthecementationmaterialandthe
ceramic.– IPSCeramicEtchingGelmustnotbeappliedintraorally!
Ivoclean–universalcleaningpastetoremoveproteins– Afterthetry-inofrestorationswithalreadyetchedsurfaces–Appliedbeforeconditioning
Monobond® Plus–universalsingle-componentbondingagent– Generatinganadhesivebond(e.g.oftheVariolinkandMultilinklineofproducts)– Forallindirectrestorativematerials(glass-andoxide-ceramics,metals,composites,fibre-
reinforcedcomposites)

18
Practical procedure for restorations with IPS e.max | Cementation
Tip
Toprovidethenecessaryandabsoluteisolationofthetreatmentareaduringincorporation,werecommendusingarubberdamasanauxiliary.
OptraDam® Plus (rubberdam):– Absoluteisolationofthetreatmentarea– Anatomicalshapeandflexible,three-dimensionaldesign– Comfortabletowear,evenduringlengthyprocedures
Cementation Navigation System – CNS
TheCNSwillsupportyouintheselectionofthesuitablecementationmaterialinvirtuallyeverysituationwherecementationonnaturaltoothstructureor implantabutments isrequired.Moreover,theCNSshowsyoutheoptionsprovidedbythecementationmaterialsfromIvoclarVivadent.Detailedanimationsguideyouthroughthecomprehensiveapplicationprotocol–fromtheremovalofthetemporaryrestorationtothefinalfluorideapplication.
Availableasonlineapplication,CD-ROM,andAppforiPhoneandAndroid
www.cementation-navigation.com
CnS
19
Practical procedure for restorations with IPS e.max | Cementation
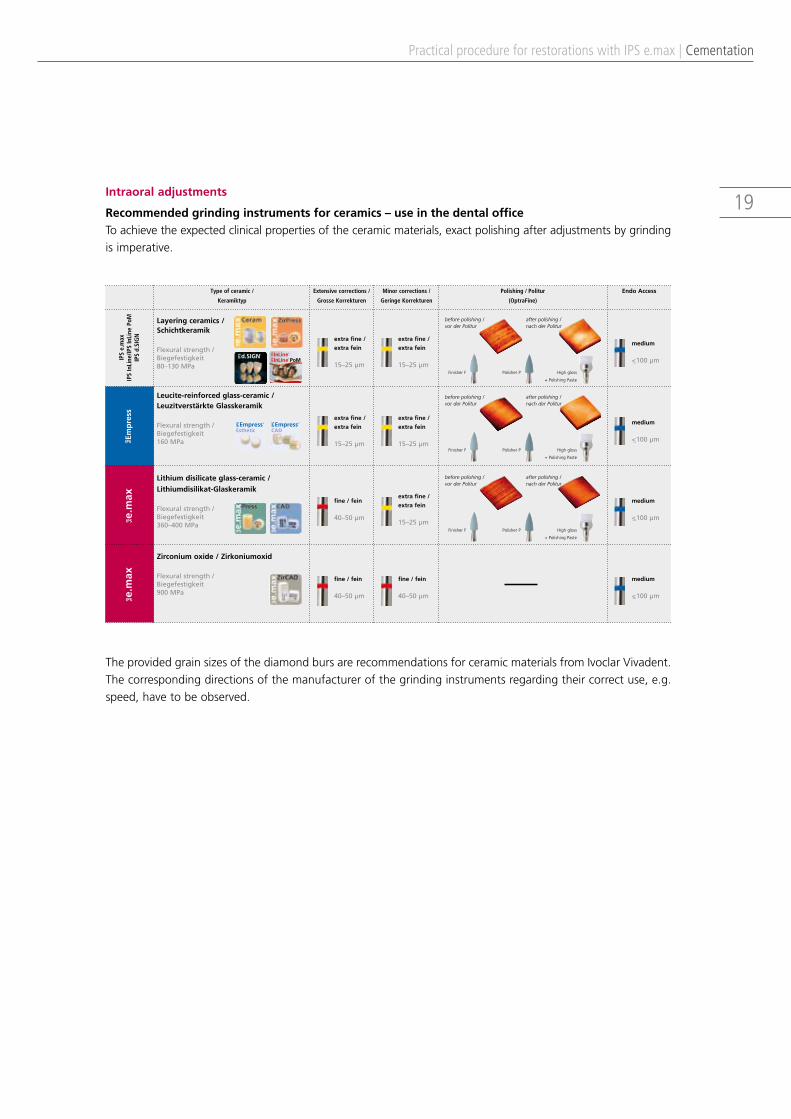
Intraoral adjustments
Recommended grinding instruments for ceramics – use in the dental officeToachievetheexpectedclinicalpropertiesoftheceramicmaterials,exactpolishingafteradjustmentsbygrindingisimperative.
Layering ceramics /Schichtkeramik
Flexural strength / Biegefestigkeit 80–130 MPa
Type of ceramic /
Keramiktyp
Extensive corrections /
Grosse Korrekturen
Minor corrections /
Geringe Korrekturen
Endo AccessPolishing / Politur
(OptraFine)
extra fine /
extra fein
15–25 µm
extra fine /
extra fein
15–25 µm
medium
<_100 µm
extra fine /
extra fein
15–25 µm
extra fine /
extra fein
15–25 µm
medium
<_100 µm
fine / fein
40–50 µm
extra fine /
extra fein
15–25 µm
medium
<_100 µm
fine / fein
40–50 µm
fine / fein
40–50 µm
medium
<_100 µm
Leucite-reinforced glass-ceramic /Leuzitverstärkte Glasskeramik
Flexural strength / Biegefestigkeit 160 MPa
Lithium disilicate glass-ceramic /
Lithiumdisilikat-Glaskeramik
Flexural strength / Biegefestigkeit 360–400 MPa
Zirconium oxide / Zirkoniumoxid
Flexural strength / Biegefestigkeit 900 MPa
d.SIGN IPS ®
InLine PoM®
IPS
InLine ®IPS
Empress IPS ®
Esthetic Empress IP
S ®
CAD
before polishing / vor der Politur
Finisher F Polisher P High gloss
+ Polishing Paste
after polishing / nach der Politur
before polishing / vor der Politur
Finisher F Polisher P High gloss
+ Polishing Paste
after polishing / nach der Politur
before polishing / vor der Politur
Finisher F Polisher P High gloss
+ Polishing Paste
after polishing / nach der Politur
IPS
e.m
axIP
S In
Line
/IPS
InLi
ne P
oM
IPS
d.SI
GN
Recommended grinding instruments for ceramics – use in the dental practice
Schleifkörperempfehlung für Keramik – Anwendung in der zahnärztlichen Praxis
TheprovidedgrainsizesofthediamondbursarerecommendationsforceramicmaterialsfromIvoclarVivadent.Thecorrespondingdirectionsofthemanufacturerofthegrindinginstrumentsregardingtheircorrectuse,e.g.speed,havetobeobserved.
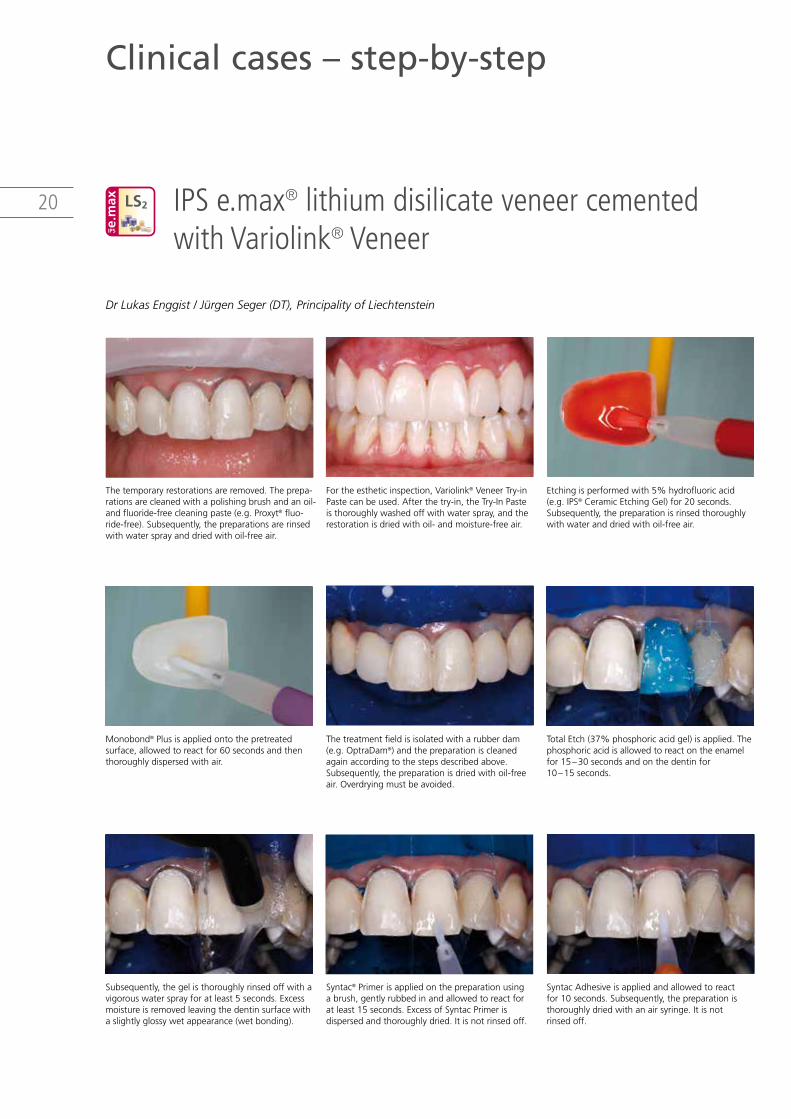
20 IPS e.max® lithium disilicate veneer cemented with Variolink® Veneer
Clinical cases – step-by-step
Thetemporaryrestorationsareremoved.Theprepa-rationsarecleanedwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxyt®fluo-ride-free).Subsequently,thepreparationsarerinsedwithwatersprayanddriedwithoil-freeair.
Subsequently,thegelisthoroughlyrinsedoffwithavigorouswatersprayforatleast5seconds.Excessmoistureisremovedleavingthedentinsurfacewithaslightlyglossywetappearance(wetbonding).
Monobond®Plusisappliedontothepretreated surface,allowedtoreactfor60secondsandthenthoroughlydispersedwithair.
Fortheestheticinspection,Variolink®VeneerTry-inPastecanbeused.Afterthetry-in,theTry-InPasteisthoroughlywashedoffwithwaterspray,andtherestorationisdriedwithoil-andmoisture-freeair.
Syntac®Primerisappliedonthepreparationusing abrush,gentlyrubbedinandallowedtoreactforatleast15seconds.ExcessofSyntacPrimerisdispersedandthoroughlydried.Itisnotrinsedoff.
Thetreatmentfieldisisolatedwitharubberdam(e.g.OptraDam®)andthepreparationiscleanedagainaccordingtothestepsdescribedabove.Subsequently,thepreparationisdriedwithoil-freeair.Overdryingmustbeavoided.
Etchingisperformedwith5%hydrofluoricacid(e.g.IPS®CeramicEtchingGel)for20seconds.Subsequently,thepreparationisrinsedthoroughlywithwateranddriedwithoil-freeair.
SyntacAdhesiveisappliedandallowedtoreact for10seconds.Subsequently,thepreparationisthoroughlydriedwithanairsyringe.Itisnot rinsedoff.
TotalEtch(37%phosphoricacidgel)isapplied.Thephosphoricacidisallowedtoreactontheenamelfor15–30secondsandonthedentinfor 10–15seconds.
LS2
Dr Lukas Enggist / Jürgen Seger (DT), Principality of Liechtenstein
21
Clinical cases – step-by-step | IPS e.max® lithium disilicate veneer cemented with Variolink® Veneer
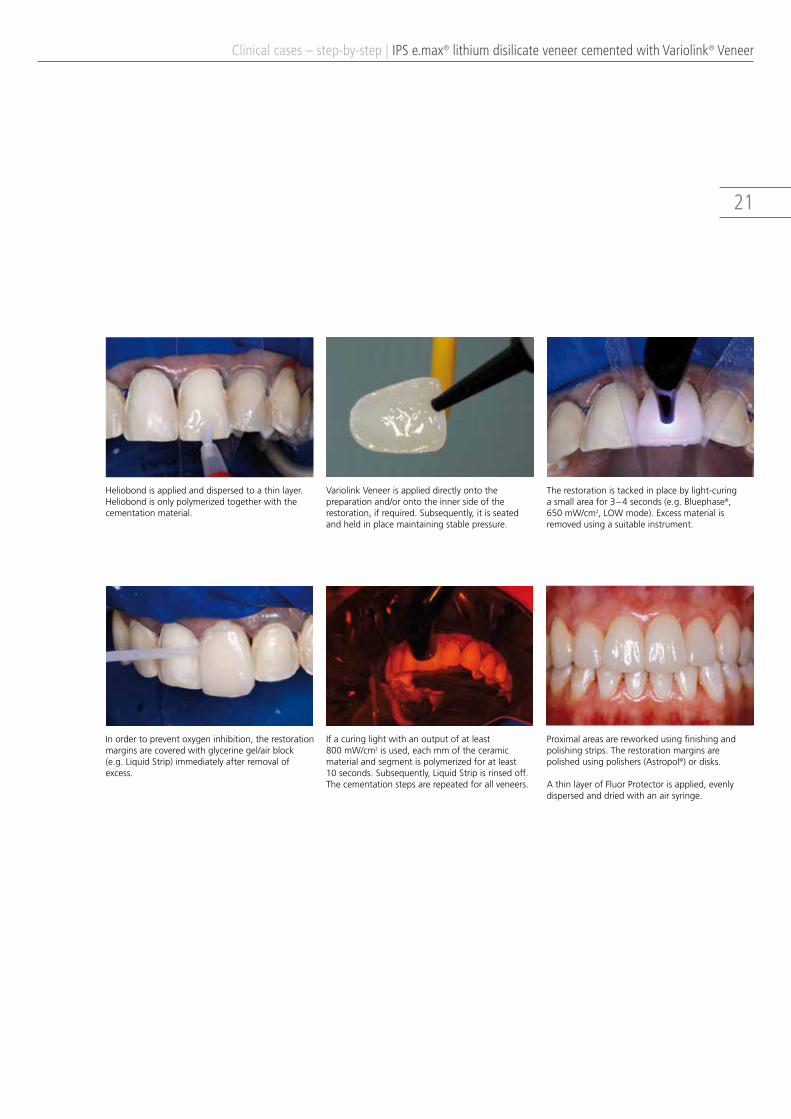
Heliobondisappliedanddispersedtoathinlayer. Heliobondisonlypolymerizedtogetherwiththecementationmaterial.
Inordertopreventoxygeninhibition,therestorationmarginsarecoveredwithglycerinegel/airblock (e.g.LiquidStrip)immediatelyafterremovalof excess.
VariolinkVeneerisapplieddirectlyontothepreparationand/orontotheinnersideoftherestoration,ifrequired.Subsequently,itisseatedandheldinplacemaintainingstablepressure.
Ifacuringlightwithanoutputofatleast 800mW/cm2isused,eachmmoftheceramic materialandsegmentispolymerizedforatleast 10seconds.Subsequently,LiquidStripisrinsedoff.Thecementationstepsarerepeatedforallveneers.
Proximalareasarereworkedusingfinishingand polishingstrips.Therestorationmarginsare polishedusingpolishers(Astropol®)ordisks.
AthinlayerofFluorProtectorisapplied,evenly dispersedanddriedwithanairsyringe.
Therestorationistackedinplacebylight-curing asmallareafor3–4seconds(e.g.Bluephase®, 650mW/cm2,LOWmode).Excessmaterialis removedusingasuitableinstrument.
22 IPS e.max® lithium disilicate inlay cemented with Multilink® Automix
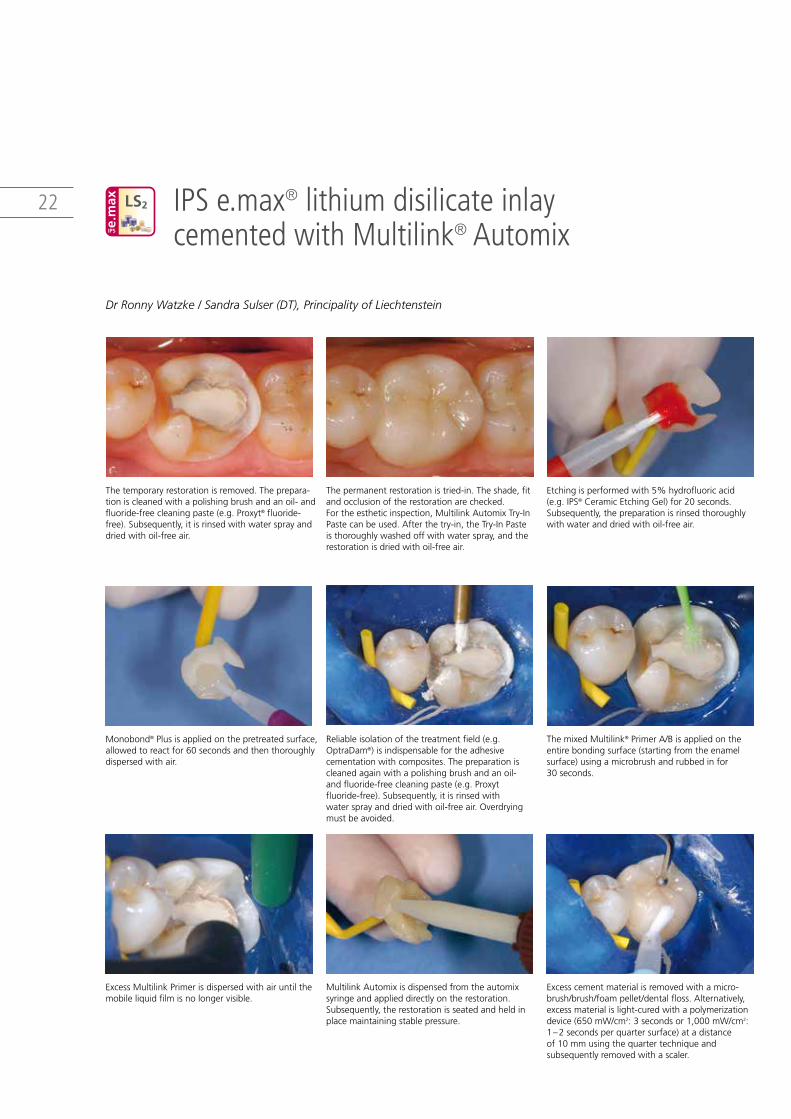
Thetemporaryrestorationisremoved.Theprepara-tioniscleanedwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxyt®fluoride-free).Subsequently,itisrinsedwithwatersprayanddriedwithoil-freeair.
ExcessMultilinkPrimerisdispersedwithairuntilthemobileliquidfilmisnolongervisible.
Monobond®Plusisappliedonthepretreatedsurface,allowedtoreactfor60secondsandthenthoroughlydispersedwithair.
Thepermanentrestorationistried-in.Theshade,fitandocclusionoftherestorationarechecked.Fortheestheticinspection,MultilinkAutomixTry-InPastecanbeused.Afterthetry-in,theTry-InPasteisthoroughlywashedoffwithwaterspray,andtherestorationisdriedwithoil-freeair.
MultilinkAutomixisdispensedfromtheautomix syringeandapplieddirectlyontherestoration.Subsequently,therestorationisseatedandheldinplacemaintainingstablepressure.
Reliableisolationofthetreatmentfield(e.g.OptraDam®)isindispensablefortheadhesivecementationwithcomposites.Thepreparationiscleanedagainwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxytfluoride-free).Subsequently,itisrinsedwith watersprayanddriedwithoil-freeair.Overdryingmustbeavoided.
Etchingisperformedwith5%hydrofluoricacid(e.g.IPS®CeramicEtchingGel)for20seconds.Subsequently,thepreparationisrinsedthoroughlywithwateranddriedwithoil-freeair.
Excesscementmaterialisremovedwithamicro-brush/brush/foampellet/dentalfloss.Alternatively,excessmaterialislight-curedwithapolymerizationdevice(650mW/cm2:3secondsor1,000mW/cm2:1–2secondsperquartersurface)atadistance of10mmusingthequartertechniqueand subsequentlyremovedwithascaler.
ThemixedMultilink®PrimerA/Bisappliedontheentirebondingsurface(startingfromtheenamelsurface)usingamicrobrushandrubbedinfor 30seconds.
LS2
Dr Ronny Watzke / Sandra Sulser (DT), Principality of Liechtenstein

23
Clinical cases – step-by-step | IPS e.max® lithium disilicate inlay cemented with Multilink® Automix
Inordertopreventoxygeninhibition,therestorationmarginsarecoveredwithglycerinegel/airblock(e.g.LiquidStrip)immediatelyaftertheremovalofexcess.
Proximalareasarereworkedusingfinishingandpolishingstrips.Theocclusionandfunctionarechecked.Restorationmarginsarepolishedusingpolishers(Astropol®)ordisks.
AthinlayerofFluorProtectorisapplied.Thevarnishisevenlyappliedanddriedwithanairsyringe.
Subsequently,allcementationjointsarelight-cured(approx.1,200mW/cm2)againfor20seconds.Ifnon-translucent,opaquerestorativematerialsareused,self-curingmustbecompleted.
Subsequently,LiquidStripisrinsedoffandtherubberdamisremoved.
24 IPS e.max® lithium disilicate anterior crown cemented with Multilink® Automix
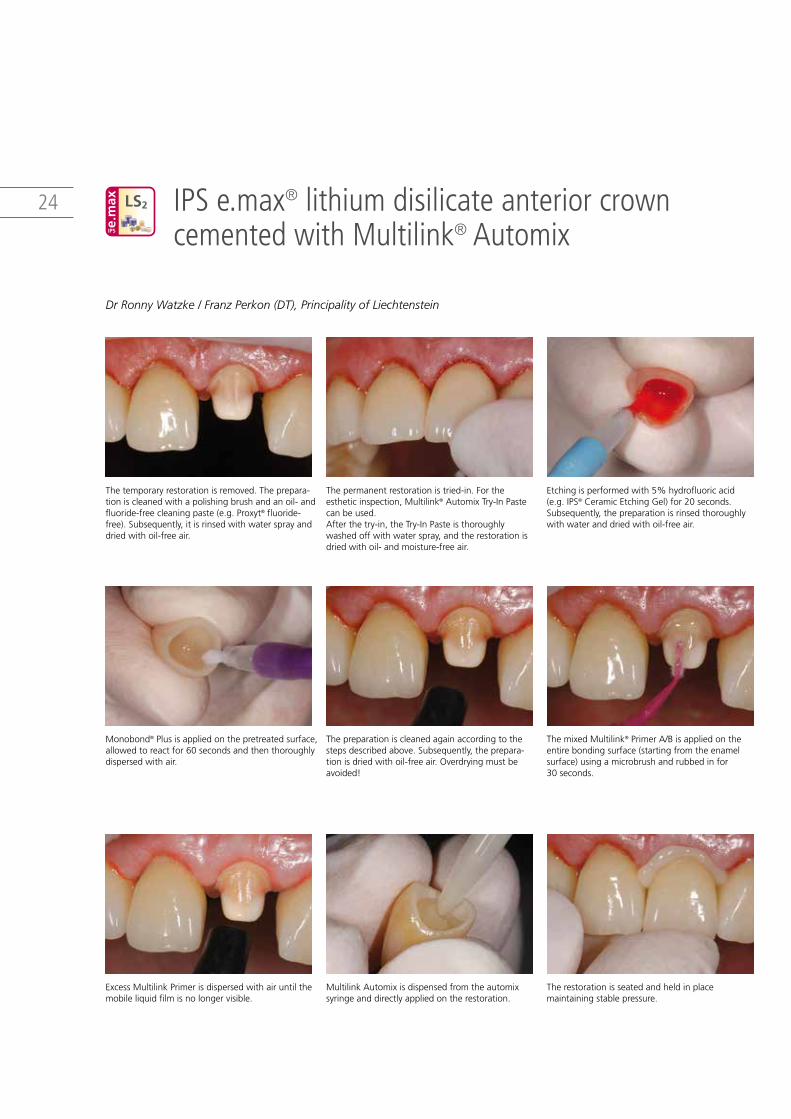
Thetemporaryrestorationisremoved.Theprepara-tioniscleanedwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxyt®fluoride-free).Subsequently,itisrinsedwithwatersprayanddriedwithoil-freeair.
ExcessMultilinkPrimerisdispersedwithairuntilthemobileliquidfilmisnolongervisible.
Monobond®Plusisappliedonthepretreatedsurface,allowedtoreactfor60secondsandthenthoroughlydispersedwithair.
Thepermanentrestorationistried-in.Forthe estheticinspection,Multilink®AutomixTry-InPastecanbeused.Afterthetry-in,theTry-InPasteisthoroughlywashedoffwithwaterspray,andtherestorationisdriedwithoil-andmoisture-freeair.
MultilinkAutomixisdispensedfromtheautomix syringeanddirectlyappliedontherestoration.
Thepreparationiscleanedagainaccordingtothestepsdescribedabove.Subsequently,theprepara-tionisdriedwithoil-freeair.Overdryingmustbeavoided!
Etchingisperformedwith5%hydrofluoricacid(e.g.IPS®CeramicEtchingGel)for20seconds.Subsequently,thepreparationisrinsedthoroughlywithwateranddriedwithoil-freeair.
Therestorationisseatedandheldinplacemaintainingstablepressure.
ThemixedMultilink®PrimerA/Bisappliedontheentirebondingsurface(startingfromtheenamelsurface)usingamicrobrushandrubbedinfor 30seconds.
LS2
Dr Ronny Watzke / Franz Perkon (DT), Principality of Liechtenstein

25
Clinical cases – step-by-step | IPS e.max® lithium disilicate anterior crown cemented with Multilink® Automix
Excesscementislight-curedwithapolymerizationdevice(650mW/cm2:3secondsor1,000mW/cm2:1–2secondsperquartersurface)atadistanceof 10mmusingthequartertechnique.
Subsequently,allcementationjointsarelight-cured(approx.1,200mW/cm2)againfor20seconds.Ifnon-translucent,opaquerestorativematerialsareused,self-curingmustbecompleted.Subsequently,LiquidStripisrinsedoff.
Proximalareasarereworkedusingfinishingandpolishingstrips.Theocclusionandfunctionarechecked.Restorationmarginsarepolishedusingpolishers(Astropol®)ordisks.
AthinlayerofFluorProtectorisapplied.The varnishisevenlydispersedanddriedwithanairsyringe.
Excessmaterialisnoweasilyremovedwithascaler. Inordertopreventoxygeninhibition,therestora-tionmarginsarecoveredwithglycerinegel/airblock(e.g.LiquidStrip)immediatelyaftertheremovalofexcess.
26 IPS e.max® lithium disilicate posterior crown cemented with Multilink® Automix
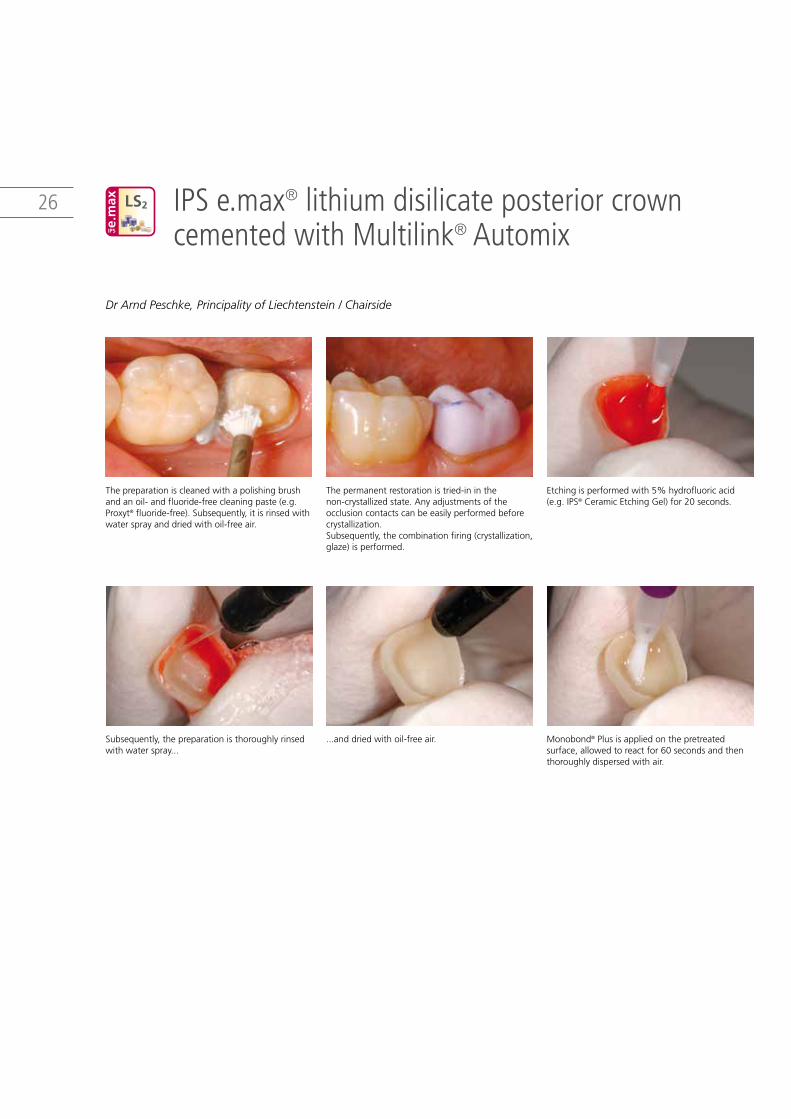
Thepreparationiscleanedwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxyt®fluoride-free).Subsequently,itisrinsedwithwatersprayanddriedwithoil-freeair.
Subsequently,thepreparationisthoroughlyrinsedwithwaterspray...
Thepermanentrestorationistried-ininthenon-crystallizedstate.Anyadjustmentsoftheocclusioncontactscanbeeasilyperformedbeforecrystallization.Subsequently,thecombinationfiring(crystallization,glaze)isperformed.
...anddriedwithoil-freeair.
Etchingisperformedwith5%hydrofluoricacid(e.g.IPS®CeramicEtchingGel)for20seconds.
Monobond®Plusisappliedonthepretreated surface,allowedtoreactfor60secondsandthenthoroughlydispersedwithair.
LS2
Dr Arnd Peschke, Principality of Liechtenstein / Chairside

27
Clinical cases – step-by-step | IPS e.max® lithium disilicate anterior crown cemented with Multilink® Automix
Excesscementmaterialislight-curedwithapoly-merizationdevice(650mW/cm2:3secondsor 1,000mW/cm2:1–2secondsperquartersurface) atadistanceof10mmusingthequartertechnique.
Excessmaterialisnoweasilyremovedwithascaler.
Inordertopreventoxygeninhibition,therestora-tionmarginsarecoveredwithglycerinegel/airblock(e.g.LiquidStrip)immediatelyaftertheremovalofexcess.Subsequently,allcementationjointsarelight-cured(approx.1,200mW/cm2)againfor20seconds.Ifnon-translucent,opaquerestorativematerialsareused,self-curingmustbecompleted.
Proximalareasarereworkedusingfinishingandpolishingstrips.Theocclusionandfunctionarechecked.Restorationmarginsarepolishedusingpolishers(Astropol)ordisks.
AthinlayerofFluorProtectorisapplied.Thevarnishisevenlydispersedanddriedwithanairsyringe.
ThemixedMultilink®PrimerA/Bisappliedontheentirebondingsurface(startingfromtheenamelsurface)usingamicrobrushandrubbedinfor 30seconds.ExcessMultilinkPrimerisdispersedwithairuntilthemobileliquidfilmisnolongervisible.
MultilinkAutomixisdispensedfromtheautomixsyringeanddirectlyappliedontherestoration.
Therestorationisseatedandheldinplace maintainingstablepressure.
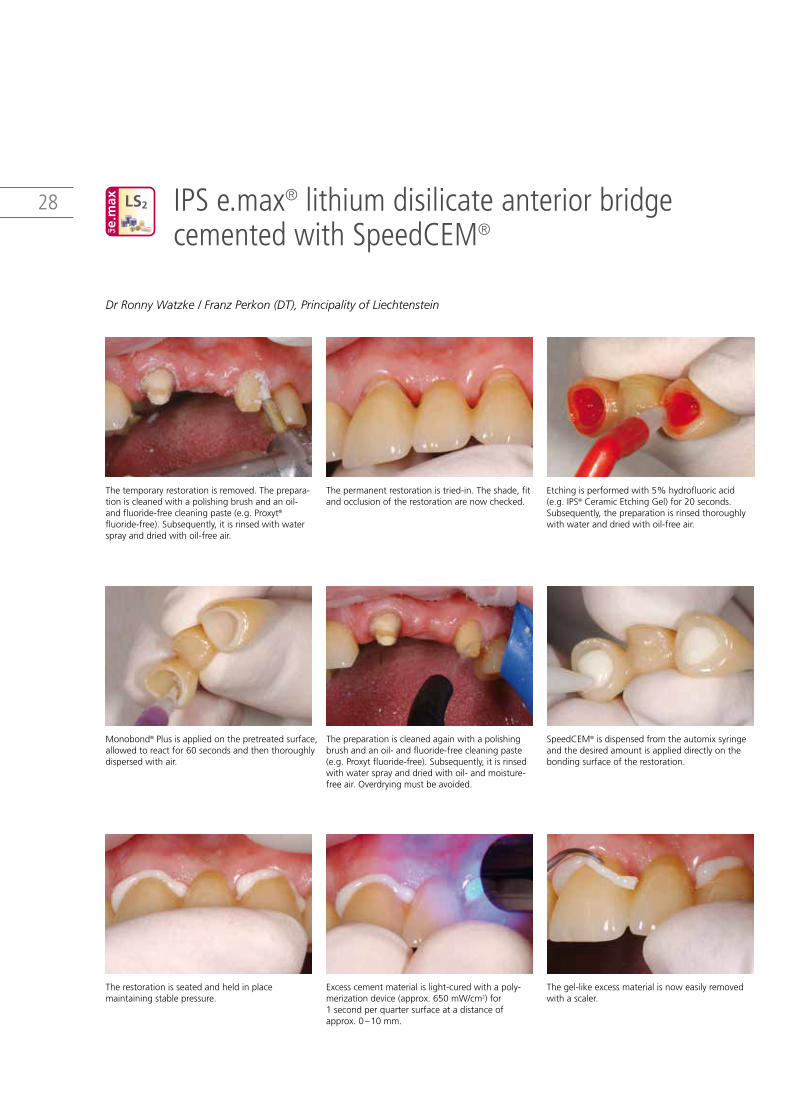
28 IPS e.max® lithium disilicate anterior bridge cemented with SpeedCEM®
Thetemporaryrestorationisremoved.Theprepara-tioniscleanedwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxyt® fluoride-free).Subsequently,itisrinsedwithwatersprayanddriedwithoil-freeair.
Therestorationisseatedandheldinplace maintainingstablepressure.
Monobond®Plusisappliedonthepretreatedsurface,allowedtoreactfor60secondsandthenthoroughlydispersedwithair.
Thepermanentrestorationistried-in.Theshade,fitandocclusionoftherestorationarenowchecked.
Excesscementmaterialislight-curedwithapoly-merizationdevice(approx.650mW/cm2)for 1secondperquartersurfaceatadistanceofapprox.0–10mm.
Thepreparationiscleanedagainwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxytfluoride-free).Subsequently,itisrinsedwithwatersprayanddriedwithoil-andmoisture-freeair.Overdryingmustbeavoided.
Etchingisperformedwith5%hydrofluoricacid(e.g.IPS®CeramicEtchingGel)for20seconds.Subsequently,thepreparationisrinsedthoroughlywithwateranddriedwithoil-freeair.
Thegel-likeexcessmaterialisnoweasilyremovedwithascaler.
SpeedCEM®isdispensedfromtheautomixsyringeandthedesiredamountisapplieddirectlyonthebondingsurfaceoftherestoration.
Dr Ronny Watzke / Franz Perkon (DT), Principality of Liechtenstein
LS2

29
Clinical cases – step-by-step | IPS e.max® lithium disilicate anterior bridge cemented with SpeedCEM®
Inordertopreventoxygeninhibition,therestorationmarginsarecoveredwithglycerinegel/airblock(e.g.LiquidStrip)immediatelyaftertheremovalofexcess.
Proximalareasarereworkedusingfinishingand polishingstrips.Theocclusionandfunctionarechecked.Restorationmarginsarepolishedusingpolishers(OptraPol®NextGeneration)ordisks.
AthinlayerofFluorProtectorisapplied.Thevarnishisevenlydispersedanddriedwithanairsyringe.
Subsequently,allcementationjointsarelight-cured(approx.1,200mW/cm2)againfor20seconds.Ifnon-translucent,opaquerestorativematerialsareused,self-curingmustbecompleted.
Subsequently,LiquidStripisrinsedoff.

30 IPS e.max® zirconium oxide anterior bridge cemented with SpeedCEM®
Thetemporaryrestorationisremoved.Theprepara-tioniscleanedwithapolishingbrushandanoil- andfluoride-freecleaningpaste(e.g.Proxyt® fluoride-free).Subsequently,itisrinsedwithwatersprayanddriedwithoil-freeair.
ThedesiredamountofSpeedCEM®isapplied directlyontothebondingsurfaceoftherestoration.
Thepermanentrestorationistried-in.Theshade, fitandocclusionoftherestorationarechecked. Theinnersurfaceoftherestorationiscleanedbyblastingit(e.g.IPSe.max®ZirCAD,1bar, Al2O3100μm).
Therestorationisseatedandheldinplace maintainingstablepressure.
Thepreparationiscleanedagainwithapolishingbrushandanoil-andfluoride-freecleaningpaste(e.g.Proxyt®fluoride-free).Subsequently,itisrinsedwithwatersprayanddriedwithoil-freeair.Over-dryingmustbeavoided.
Excesscementmaterialislight-curedwithapoly-merizationdevice(approx.650mW/cm2)for 1secondperquartersurfaceatadistanceof approx.0–10mm.
ZrO2
Dr Ronny Watzke / Pascal Scherrer (DT), Principality of Liechtenstein

31
Clinical cases – step-by-step | IPS e.max® zirconium oxide anterior bridge cemented with SpeedCEM®
Proximalareasarereworkedusingfinishingand polishingstrips.Theocclusionandfunctionarechecked.Restorationmarginsarepolishedusing polishers(OptraPol®NextGeneration)ordisks.
AthinlayerofFluorProtectorisapplied.Thevarnishisevenlydispersedanddriedwithanairsyringe.
Excessmaterialisnoweasilyremovedwithascaler. Inordertopreventoxygeninhibition,therestora-tionmarginsarecoveredwithglycerinegel/airblock(e.g.LiquidStrip)immediatelyaftertheremovalofexcess.
Subsequently,allcementationjointsarelight-cured(approx.1,200mW/cm2)againfor20seconds.Ifnon-translucent,opaquerestorativematerialsareused,self-curingmustbecompleted.Subsequently,LiquidStripisrinsedoff.
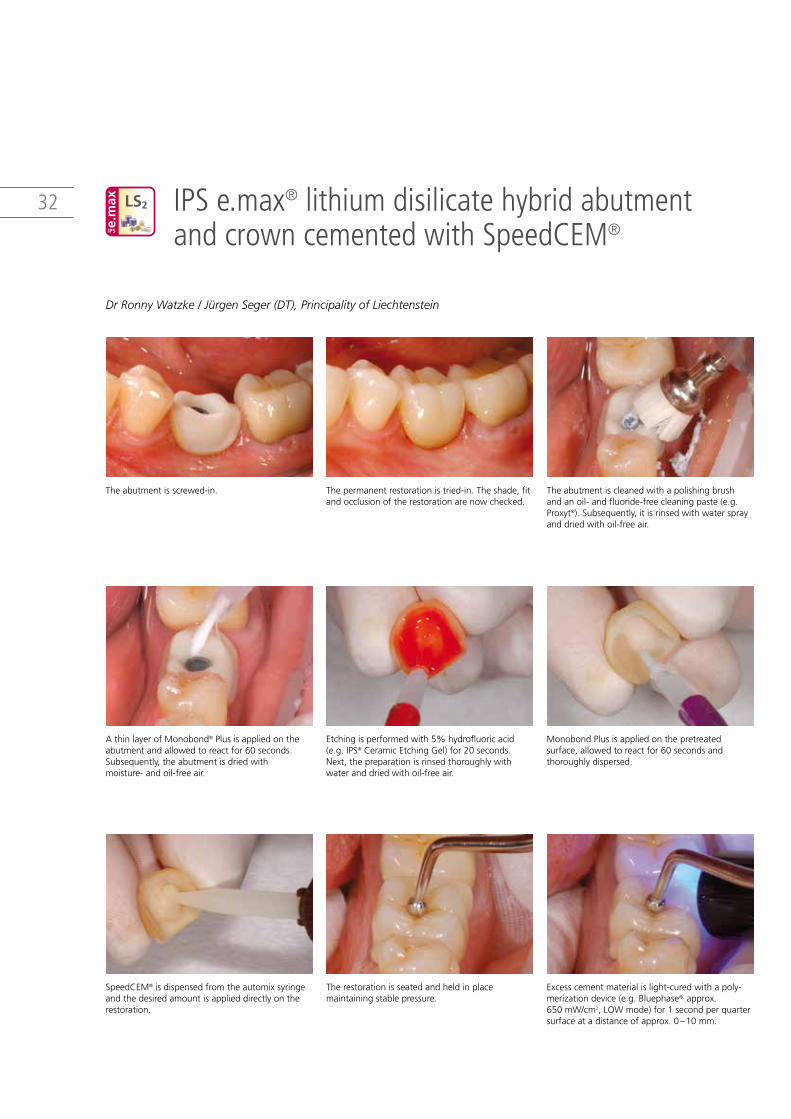
32 IPS e.max® lithium disilicate hybrid abutment and crown cemented with SpeedCEM®
Theabutmentisscrewed-in.
SpeedCEM®isdispensedfromtheautomixsyringeandthedesiredamountisapplieddirectlyontherestoration.
AthinlayerofMonobond®Plusisappliedontheabutmentandallowedtoreactfor60seconds.Subsequently,theabutmentisdriedwithmoisture-andoil-freeair.
Thepermanentrestorationistried-in.Theshade,fitandocclusionoftherestorationarenowchecked.
Therestorationisseatedandheldinplace maintainingstablepressure.
Etchingisperformedwith5%hydrofluoricacid(e.g.IPS®CeramicEtchingGel)for20seconds.Next,thepreparationisrinsedthoroughlywithwateranddriedwithoil-freeair.
Theabutmentiscleanedwithapolishingbrush andanoil-andfluoride-freecleaningpaste(e.g.Proxyt®).Subsequently,itisrinsedwithwatersprayanddriedwithoil-freeair.
Excesscementmaterialislight-curedwithapoly-merizationdevice(e.g.Bluephase®,approx. 650mW/cm2,LOWmode)for1secondperquartersurfaceatadistanceofapprox.0–10mm.
MonobondPlusisappliedonthepretreated surface,allowedtoreactfor60secondsand thoroughlydispersed.
LS2
Dr Ronny Watzke / Jürgen Seger (DT), Principality of Liechtenstein

33
Clinical cases – step-by-step | IPS e.max® lithium disilicate hybrid abutment and crown cemented with SpeedCEM®
Thegel-likeexcessmaterialisnoweasilyremovedwithascaler.
Proximalareasarereworkedusingfinishingandpolishingstrips.Theocclusionandfunctionarecheckedandadjusted,ifrequired.Restorationmarginsarepolishedusingpolishers(Astropol®)ordisks.
AthinlayerofCervitec®Plusisapplied.Thevarnishislefttodryordriedwithanairsyringe.
Inordertopreventoxygeninhibition,therestora-tionmarginsarecoveredwithglycerinegel/airblock(e.g.LiquidStrip)immediatelyaftertheremovalofexcess.Subsequently,allcementationjointsarelight-cured(approx.1,200mW/cm2)againfor 20seconds.Ifnon-translucent,opaquerestorativematerialsareused,self-curingmustbecompleted.
Subsequently,LiquidStripisrinsedoff.

34 IPS e.max® lithium disilicate hybrid abutment crown – screwed-in
Thetemporaryrestorationisremoved.
Thescrewchannelisetchedfromtheocclusalsidewith5%hydrofluoricacidgel(IPS®CeramicEtchingGel)for20seconds.
Thehybridabutmentcrownisscrewedinmanuallywiththededicatedscrewforthetry-inofthe permanentrestoration.Theshade,fitandocclusionoftherestorationarenowchecked.Subsequently,thehybridabutmentcrownis carefullyremovedagainforextraoralcleaning.
Next,thepreparationisrinsedthoroughlywithwateranddriedwithoil-freeair.
Thehybridabutmentcrowniscleaned,rinsedwithwatersprayandthendriedwithoil-freeair.
Thehybridabutmentcrownisinsertedintothe implantintraorally.Itisscrewedinmanuallywiththeappropriatescrew,whichistightenedwithatorquewrench(theinstructionsofthemanufacturermustbeobserved).
LS2
Dr Ronny Watzke / Franz Perkon (DT), Principality of Liechtenstein
35
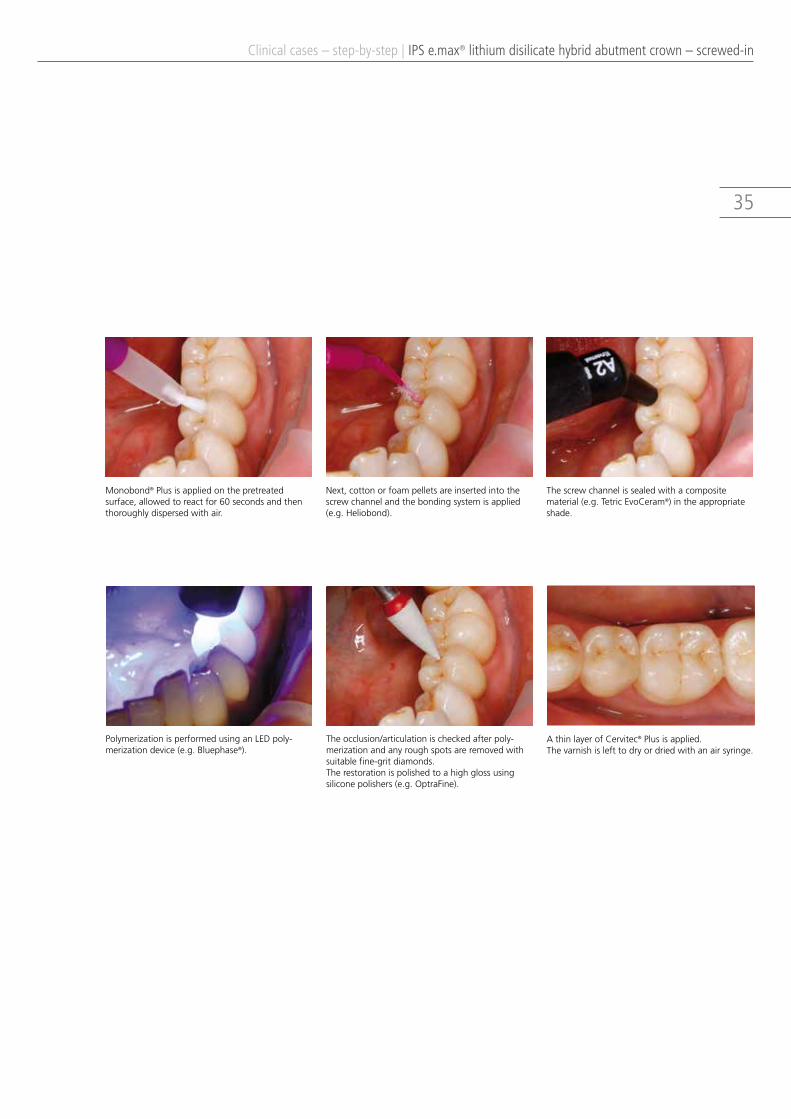
Clinical cases – step-by-step | IPS e.max® lithium disilicate hybrid abutment crown – screwed-in
PolymerizationisperformedusinganLEDpoly-merizationdevice(e.g.Bluephase®).
Monobond®Plusisappliedonthepretreated surface,allowedtoreactfor60secondsandthenthoroughlydispersedwithair.
Theocclusion/articulationischeckedafterpoly-merizationandanyroughspotsareremovedwithsuitablefine-gritdiamonds.Therestorationispolishedtoahighglossusingsiliconepolishers(e.g.OptraFine).
Next,cottonorfoampelletsareinsertedintothescrewchannelandthebondingsystemisapplied(e.g.Heliobond).
Thescrewchannelissealedwithacomposite material(e.g.TetricEvoCeram®)intheappropriateshade.
AthinlayerofCervitec®Plusisapplied.Thevarnishislefttodryordriedwithanairsyringe.

36 Starting situation – Final result
IPS e.max lithium disilicate veneer cemented with Variolink® VeneerDr Lukas Enggist / Jürgen Seger (DT), Principality of Liechtenstein
IPS e.max lithium disilicate inlay cemented with Multilink® AutomixDr Ronny Watzke / Sandra Sulser (DT), Principality of Liechtenstein

37
Clinical cases | Starting situation – Final result
IPS e.max lithium disilicate anterior crown cemented with Multilink® AutomixDr Ronny Watzke / Franz Perkon (DT), Principality of Liechtenstein
IPS e.max lithium disilicate posterior crown cemented with Multilink® AutomixDr Arnd Peschke, Principality of Liechtenstein / Chairside

38
Clinical cases | Starting situation – Final result
IPS e.max lithium disilicate anterior bridge cemented with SpeedCEM® Dr Ronny Watzke / Franz Perkon (DT), Principality of Liechtenstein
IPS e.max zirconium oxide anterior bridge cemented with SpeedCEM®
Dr Ronny Watzke / Pascal Scherrer (DT), Principality of Liechtenstein

39
IPS e.max lithium disilicate hybrid abutment and crown cemented with SpeedCEM®
Dr Ronny Watzke / Jürgen Seger (DT), Principality of Liechtenstein
IPS e.max lithium disilicate hybrid abutment crown – screwed-inDr Ronny Watzke / Franz Perkon (DT), Principality of Liechtenstein
Clinical cases | Starting situation – Final result
40
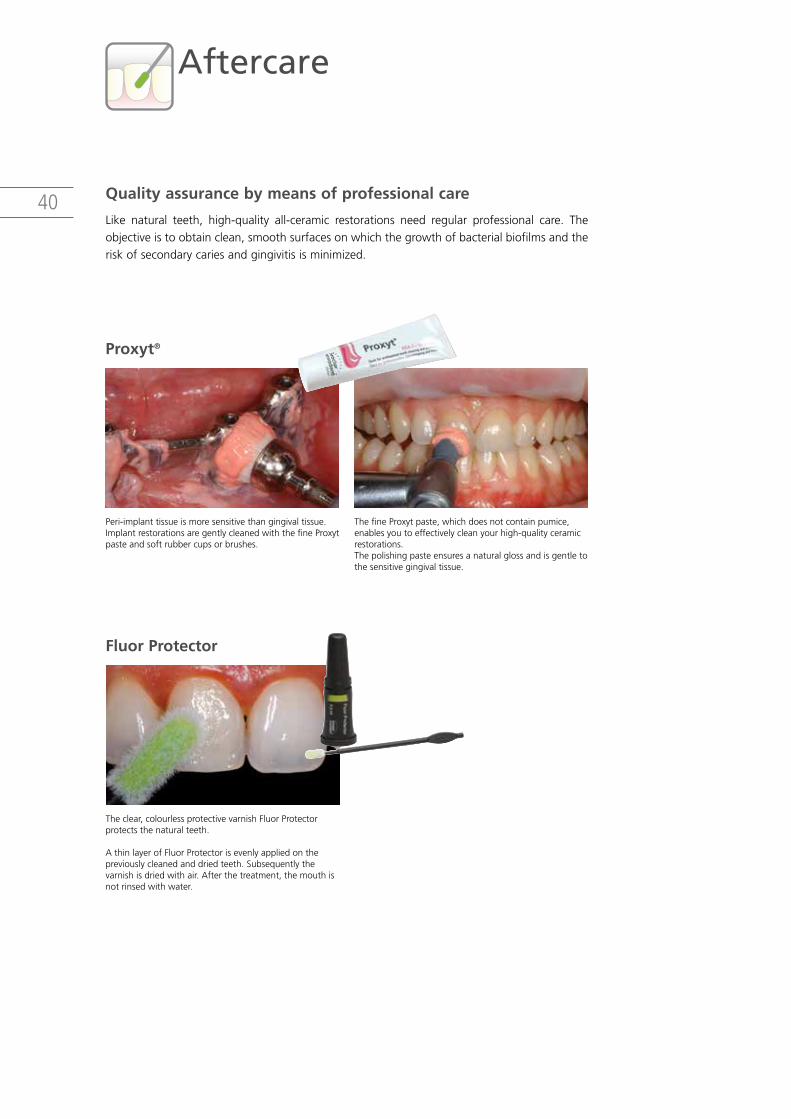
Aftercare
Quality assurance by means of professional care
Like natural teeth, high-quality all-ceramic restorations need regular professional care. Theobjectiveistoobtainclean,smoothsurfacesonwhichthegrowthofbacterialbiofilmsandtheriskofsecondarycariesandgingivitisisminimized.
Proxyt®
Fluor Protector
Peri-implanttissueismoresensitivethangingivaltissue.ImplantrestorationsaregentlycleanedwiththefineProxytpasteandsoftrubbercupsorbrushes.
Theclear,colourlessprotectivevarnishFluorProtectorprotectsthenaturalteeth.
AthinlayerofFluorProtectorisevenlyappliedonthe previouslycleanedanddriedteeth.Subsequentlythe varnishisdriedwithair.Afterthetreatment,themouthisnotrinsedwithwater.
ThefineProxytpaste,whichdoesnotcontainpumice, enablesyoutoeffectivelycleanyourhigh-qualityceramicrestorations.Thepolishingpasteensuresanaturalglossandisgentletothesensitivegingivaltissue.

41
Results from more than 10 years of research
The IPSe.maxSystem isan innovativeall-ceramic system,which includesmaterialsmadeoflithium disilicate (LS2) glass-ceramic and zirconium oxide (ZrO2) for the press technique andCAD/CAMtechnology.Inaddition,auniversallyapplicablenano-fluorapatiteglass-ceramicforveneeringallthedifferentcomponentsoftheIPSe.maxSystemisavailable.
Fromthebeginningofitsdevelopmentuntiltotoday,theIPSe.maxSystemhasbeenmonitoredbythescientificcommunityandmanyrenownedexpertshavecontributedtotheestablishmentofanexcellentdatabasewith their studies.Theworldwide success story, theevergrowingdemand,aswellasthemorethan40millionfabricatedrestorationsaretestamenttothesuccessandthereliabilityofthesystem.
More than 20 clinical in-vivo studies to date and evenmore in-vitro studies, aswell as thecontinuouslyrisingnumberofclinicalstudiesinvolvingthee.maxSystemthroughouttheworldshowthelong-termsuccessoftheproductintheoralcavitiesofpatients.
Summary of the IPS e.max System
DataontheclinicaluseoftheIPSe.maxSystemoveraperiodofupto5yearsforZrO2andupto10yearsforLS2isavailable.
The survival rates from clinical studies on IPS e.max Press (6 studies), IPSe.maxCAD(6studies)andIPSe.maxZirCAD(8studies)weresumma-rizedandtheoverallsurvivalrateofthesystemwascalculated.Atotalof1071 IPS restorations from20clinical studieswere included.The resultrevealedanoverallsurvivalrateof96.8%fortheIPSe.maxSystem.
all ceramic
all you need
SCIENTIFIC REPORTVol. 02 / 2001 – 2013Deutsch

42

43
665082/en/2013-09-30
ivoclar Vivadent aGBendererstrasse 29494 SchaanLiechtensteinTel. +423 235 35 35Fax +423 235 33 60www.ivoclarvivadent.com
ivoclar Vivadent Pty. ltd. 1 – 5 Overseas DriveP.O. Box 367Noble Park, Vic. 3174AustraliaTel. +61 3 9795 9599Fax +61 3 9795 9645www.ivoclarvivadent.com.au
ivoclar Vivadent ltda.Alameda Caiapós, 723Centro Empresarial TamboréCEP 06460-110 Barueri – SPBrazilTel. +55 11 2424 7400Fax +55 11 3466 0840www.ivoclarvivadent.com.br
ivoclar Vivadent inc.1-6600 Dixie RoadMississauga, OntarioL5T 2Y2CanadaTel. +1 905 670 8499Fax +1 905 670 3102www.ivoclarvivadent.us
ivoclar Vivadent Shanghai Trading Co., ltd.2/F Building 1, 881 Wuding Road, Jing An District 200040 Shanghai ChinaTel. +86 21 6032 1657Fax +86 21 6176 0968www.ivoclarvivadent.com
ivoclar Vivadent Marketing ltd.Calle 134 No. 7-B-83, Of. 520BogotáColombiaTel. +57 1 627 3399Fax +57 1 633 1663www.ivoclarvivadent.co
ivoclar Vivadent SaSB.P. 118F-74410 Saint-JoriozFranceTel. +33 4 50 88 64 00Fax +33 4 50 68 91 52www.ivoclarvivadent.fr
ivoclar Vivadent GmbH Dr. Adolf-Schneider-Str. 2D-73479 Ellwangen, JagstGermanyTel. +49 7961 889 0Fax +49 7961 6326www.ivoclarvivadent.de
Wieland dental + Technik GmbH & Co. KGSchwenninger Strasse 13D-75179 PforzheimGermanyTel. +49 7231 3705 0Fax +49 7231 3579 59www.wieland-dental.com
ivoclar Vivadent Marketing (india) Pvt. ltd. 503/504 Raheja Plaza 15 B Shah Industrial Estate Veera Desai Road, Andheri (West) Mumbai, 400 053 IndiaTel. +91 22 2673 0302 Fax +91 22 2673 0301www.ivoclarvivadent.in
ivoclar Vivadent s.r.l. Via Isonzo 67/6940033 Casalecchio di Reno (BO)ItalyTel. +39 051 6113555Fax +39 051 6113565www.ivoclarvivadent.it
ivoclar Vivadent K.K.1-28-24-4F HongoBunkyo-ku Tokyo 113-0033JapanTel. +81 3 6903 3535Fax +81 3 5844 3657www.ivoclarvivadent.jp
ivoclar Vivadent ltd.12F W-Tower, 1303-37Seocho-dong, Seocho-gu,Seoul 137-855Republic of KoreaTel. +82 2 536 0714Fax +82 2 596 0155www.ivoclarvivadent.co.kr
ivoclar Vivadent S.a. de C.V.Av. Insurgentes Sur No. 863,Piso 14, Col. Napoles03810 México, D.F.MéxicoTel. +52 55 5062 1000Fax +52 55 5062 1029www.ivoclarvivadent.com.mx
ivoclar Vivadent BVDe Fruittuinen 322132 NZ HoofddorpNetherlandsTel. +31 23 529 3791Fax +31 23 555 4504www.ivoclarvivadent.com
ivoclar Vivadent ltd.12 Omega St, RosedalePO Box 303011 North HarbourAuckland 0751New ZealandTel. +64 9 914 9999Fax +64 9 914 9990www.ivoclarvivadent.co.nz
ivoclar Vivadent Polska Sp. z o.o.Al. Jana Pawla II 7800-175 WarszawaPolandTel. +48 22 635 5496Fax +48 22 635 5469www.ivoclarvivadent.pl
ivoclar Vivadent Marketing ltd. Prospekt Andropova 18 korp. 6/ office 10-06 115432 Moscow Russia Tel. +7 499 418 0300 Fax +7 499 418 0310 www.ivoclarvivadent.ru
ivoclar Vivadent Marketing ltd.Qlaya Main St.Siricon Building No.14, 2nd FloorOffice No. 204P.O. Box 300146Riyadh 11372Saudi ArabiaTel. +966 1 293 8345Fax +966 1 293 8344www.ivoclarvivadent.com
ivoclar Vivadent Pte. ltd.171 Chin Swee Road#02-01 San CentreSingapore 169877 Tel. +65 6535 6775Fax +65 6535 4991www.ivoclarvivadent.com
ivoclar Vivadent S.l.u.C/ Ribera del Loira nº 46, 5ª planta28042 MadridSpainTel. + 34 913 757 820Fax + 34 913 757 838www.ivoclarvivadent.es
ivoclar Vivadent aBDalvägen 14S-169 56 SolnaSwedenTel. +46 8 514 939 30Fax +46 8 514 939 40www.ivoclarvivadent.se
ivoclar Vivadent liaison Office: Tesvikiye Mahallesi Sakayik SokakNisantas’ Plaza No:38/2Kat:5 Daire:24 34021 Sisli – Istanbul Turkey Tel. +90 212 343 0802 Fax +90 212 343 0842www.ivoclarvivadent.com
ivoclar Vivadent limitedGround Floor Compass BuildingFeldspar CloseWarrens Business ParkEnderbyLeicester LE19 4SEUnited KingdomTel. +44 116 284 7880Fax +44 116 284 7881www.ivoclarvivadent.co.uk
ivoclar Vivadent, inc. 175 Pineview DriveAmherst, N.Y. 14228USATel. +1 800 533 6825Fax +1 716 691 2285www.ivoclarvivadent.us
Ivoclar Vivadent – worldwide


















