Clinical Forum: Women in Forensic Mental Health Settings Martin Culshaw Lead Clinician for Women...
35
Clinical Forum: Women in Forensic Mental Health Settings Martin Culshaw Lead Clinician for Women Forensic Network [email protected]
-
Upload
ashley-foster -
Category
Documents
-
view
217 -
download
0
Transcript of Clinical Forum: Women in Forensic Mental Health Settings Martin Culshaw Lead Clinician for Women...
Clinical Forum: Women in Forensic Mental Health Settings
Martin CulshawLead Clinician for Women
Forensic Network

What is today all about?
• Focus on women in secure/forensic hospital settings
• A patient group whose needs are not always prioritised
• Overview of the female forensic estate
• Aspects of the various security levels
• Relational security
• Psychological treatment
What is today all about?
• Please participate!
• Input from all disciplines
• Future events

My experience
• Hospital
• Prison
• Network
• Challenges for services locally, regionally and nationally
• Borderline PD
‘Women’ as a category
• ‘Woman’ is not a diagnosis!
• Much fewer of them than men in forensic services
• At risk of being seen as a homogenous group with ‘similar enough’ needs
• Can be categorised by: diagnosis level of risk patient journey

Sub-categories in low/medium secure
• Acute admissions
• Step-down patients
• Patients who are likely to need hospital treatment for many years:• disturbed behaviour associated with PD, treatment-resistant psychosis,
institutionalisation. • may not have come into contact with local forensic services
• Women with learning disability

Female Forensic Estate: Where are we now?
• Different views about need to maintain distinction between low and medium security for women in Scotland.
• In the absence of readily accessible high security, the distinction between medium and low secure settings is even more important.
• S268 appeals…
Female Forensic Estate: Where are we now?
• Some women clearly need at least a medium secure setting
• Others are readily managed in low security en route to community • Lumping all such women together could be seen as inequitable, impractical
and outwith the ‘least restrictive alternative’ principle of the Act.
High Security
• Provision for women in TSH stopped in 2007/08
• Arrangements created for cross-border transfer to NHSHSW, Rampton Hospital
• 3 transfers since then
• Pros and cons

Medium Security
• 2 separate and currently different settings for women in Scotland:
Orchard Clinic
Rowanbank Clinic
• Some of these women could be managed in low security
• This has not necessarily disadvantaged them- can still be discharged to community without the additional “stepping stone” of a low secure ward
Orchard Clinic
• No specific number of female beds
• Up to 10 female patients at any one time
• Plans for a 6-bedded single sex female ward
• Specific female inpatient team
• Covers SE Scotland (+ NoS)
• Difficulty if primary diagnosis of PD/single sex environment required

Rowanbank Clinic
• 10 female beds: 4 beds for FLD (National Risk Share Scheme) 6 beds for FMI
• Split into 2 wards: 6 bedded ward for more acutely disturbed women 4 bedded rehab ward with a home style model of care
• LD women assigned to either ward depending on their needs • Has taken patients from NoS
• Occupancy has varied significantly

Low Security
• Limited low secure accommodation
• Some areas have open rehab wards for forensic women, including those with challenging behaviour, if low risk of absconsion.
• Difficult to quantify
• Definitions of ‘low secure care’ and ‘forensic patient’ are not clear and consistent for women
• HBs use IPCUs for forensic (female) patients differently depending on access to specific low secure beds

Low Security- West of Scotland
• GG&C No specific female low secure beds • A&A Use private sector with 4 beds in open forensic rehab ward,
Ailsa Hospital for step down stage.Unclear if any new low secure unit would cater for women.
• D&G 4 low secure/forensic rehab beds potentially suitable
(but no capacity)
• Lanarks. Beckford Lodge had 2 out of 15 beds designated as suitable for women
• Outwith step-down care, private beds used for women with long-term/
complex needs. • IPCU beds used for acute admissions in some areas.

Low Security- South-east Scotland
• Lothian Plans to develop a low secure/rehab unit for both male and female patients.
Section 52 transfers tend to go to the OC rather than IPCU.
• Fife Stratheden IPCU can take acute female patients. New low secure rehab unit- for women?
• Forth Valley Female beds in IPCU FVRH.
Use open rehab beds at Bellsdyke sometimes (under rehab consultant). Otherwise private.
• Outwith step-down care, private beds used for women with long-term/ complex needs.
• IPCU beds used for acute admissions in some areas.

Low Security- North of Scotland
• Generally very little low secure female accommodation
• Tayside Amulree Unit, Murray Royal: 6 beds locked rehab, mainly Ayr Clinic returns
• Grampian Blair Unit, Royal Cornhill: 2 beds within a mixed sex IPCU
• Highland Newcraigs Hospital: 1 potential female bed within its IPCU
• Other HBs use Newcraigs or private beds

Low Security- Private sector
• Significant use of the Ayr Clinic and Surehaven Clinic, Glasgow.
• Continue to admit women for acute, step-down and long-term care and function as national multi-purpose low secure units.
• Ayr Clinic 12 bedded female ward
• Surehaven 8-9 beds
• Possible expansion of private sector female beds
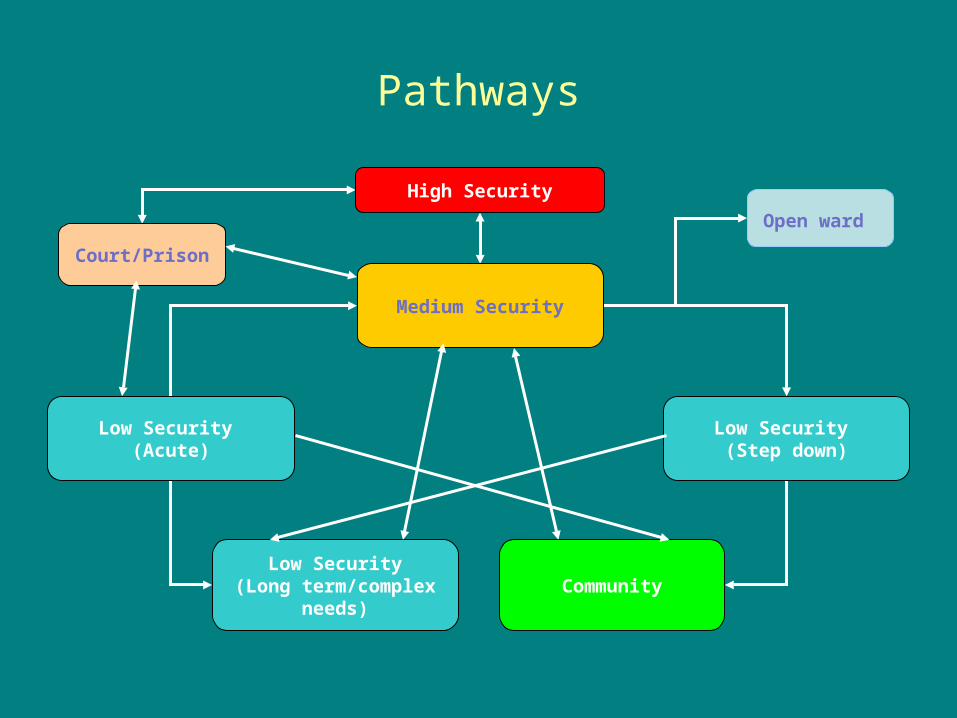
Pathways
High Security
Medium Security
Low Security (Acute)
Low Security (Step down)
Low Security(Long term/complex
needs)Community
Court/Prison
Open ward
Regional low security
• No regional units planned or constructed in any of the 3 regions since HDL (2006) 48 “Forensic Mental Health Services”.
• Whilst some local units currently have beds, it is unlikely that any are entirely suitable for all types of female forensic patient.
• Flexible accommodation designs at risk of accommodating only male patients due to pressures on beds.

Regional low security
• An alternative model could involve regional low secure units as previously recommended in HDL (2006) 48.
• i.e. 2 for the West, 1 for the East and 1 for the North • Advantages: single sex accommodation gender sensitive and gender specific approaches development of regional expertise
• May be more suitable for step-down patients. • Acute/S52 patients may be better off in local IPCU.

Long-term/complex needs patients
• Treatment-resistant illness/PD
• Single centralised national specialist unit could be considered • Less likely to return to their local community in the short-term • Opportunity to move patients back out of the private sector into an NHS
facility
• How many beds?

Long-term/complex needs patients
• Counter-arguments to having such a national service:
highly variable distribution of need across the country
would it be cheaper or better than current private sector services?
resulting disincentive for HBs to create what could be more appropriate patient-centred local solutions involving local rehabilitation/continuing care services.

High Security
NHSHSWRampton Hospital
Medium SecurityRowanbank Clinic
4 National LD beds6 WoS non-LD beds
Medium SecurityOrchard Clinic
6 East & North of Scotland beds
East of Scotland region:
Lothian, Borders, Fife, Forth Valley
West of Scotland region:
Greater Glasgow & Clyde, Ayrshire &
Arran, Lanarkshire, Dumfries & Galloway
Step down care
Local low secure/Local rehabilitation ward
Long term/complex needs
Local low secure/Local rehabilitation ward/
Continuing care ward/Private sector
(Ayr/Surehaven)
Acute Admissions/ Section 52s
Local IPCU/local low secure
Low Security
Regional Low Secure Units?
(as per HDL (2006) 48: 2 in West, 1 in East, 1 in
North)
National low secure unitOR
Better local rehab facilities?
North of Scotland region:
Highland, Grampian, Tayside,
Western Isles, Orkney, Shetland
National Learning Disability
(NSD)
Women with learning disability
• NRSS
• Lack of low secure options
• Mixed sex locked wards
• Use of NHS NTW Northgate/ private sector
• Bespoke arrangements
• Regional low secure?

Some stats…
Reports/papers
• Report of the Services for Women Working GroupForensic Network (2004)
• Likely demand for secure mental health services for women in Scotland: High and Other Levels of SecurityDr Lindsay Thomson (2008)
• Report on Low Secure Psychiatric Inpatient Services for Women in Scotland (2010)
• The Female Forensic Estate in Scotland (March 2013)• Survey of Scottish Female Patients in Secure Settings (July 2013)

2004 report
• Did not discriminate between low and medium secure services.
• Recommended: Dedicated MDTs across Scotland Core patient group should be adult women with complex mental health needs and should not
exclude women with PD Provision should be made within LD services for the small number of LD women with forensic
needs Secure beds provided in small, self contained units of no more than 10 beds Living accommodation should be separate from that for any male patients High secure provision should rarely be required and the service at TSH should close with the use
of high secure services in England in exceptional cases

2008 Needs Assessment (Dec 2007)
• No. women requiring female forensic services in Scotland = 43
(36 in Scottish units, 7 elsewhere in UK)
• No. women in medium security in Scotland = 15
No. women deemed to require it = 8
• No. women in private/OOA beds = 17 (40%)

HEALTH BOARD TOTAL NO. FEMALE PATIENTS
MSU NEEDED LSU NEEDED FORENSIC GAP
Shetland 0 0 0 0 0
Orkney 1 0 1 0 1
W. Isles 1 0 1 0 1
Highland 1 0 1 0 1
Grampian 2 0 2 1 1
Tayside 4 2 2 0 4
Fife 0 0 0 0 0
F. Valley 5 1 4 0 5
Loth/ Bord 7 2 5 5 2
GG&C 4 0 4 3 1
A & A 4 0 4 3 1
Lanarks. 6 1 5 4 2
D&G 1 0 1 1 0
TOTAL 36 6 30 17 19
Female forensic/secure care patients by Health Board of origin, level of security they require and their designation as Forensic or GAP
(Culshaw 2010)

HEALTH BOARD NUMBER IN PRIVATE SECURE SETTINGS
AYR CLINIC OTHER FORENSIC GAP
Shetland 0 0 0 0 0
Orkney 1 0 1 0 1
Western Isles 1 1 0 0 1
Highland 0 0 0 0 0
Grampian 0 0 0 0 0
Tayside 3 2 1 0 3
Fife 0 0 0 0 0
Forth Valley 1 0 1 0 1
Loth/Bord 1 0 1 0 1
GG&C 1 1 0 0 1
A&A 2 2 0 1 1
Lanarkshire 4 4 0 3 1
D&G 0 0 0 0 0
TOTAL 14 (39%) 10 4 4 10
Numbers of female patients in private secure settings by Health Board of origin (Culshaw 2010)

2013 Survey
• No. women requiring female forensic services in Scotland = 52
High 3
Medium 19
Low 30
• No. of women in private/OOA beds = 27 (52%)

2013 Survey
• Medium Security
• No. of women in medium security = 19
(16 (including 2 LD) in Scotland + 3 in England)
• No. of non-LD women deemed to require it = 12
• HDL (2006) 48:
“There will continue to be the need for medium secure female services but so low are the likely numbers only one national facility should be planned.”
2013 Survey
• Low Security
Difficult to quantify due to:
Level of returns Definitions/bed usage Cross-checking complexity

2013 Survey
• Low Security
• 24 women between 2 private units
• 6 women in NHS Tayside locked ward
• 8 in open rehab in NHS Forth Valley / A&A
• Overall some 30 women in low secure accommodation
(not including IPCUs).
• 80% in private sector beds

Summary
• Number of Scottish women in or requiring a secure setting can fluctuate significantly
• Probably around 40-55 at any one time in recent years
• May be rising
• Probably need 12 medium secure beds for non-LD women
• Local, regional and/or national units remain as options for an NHS estate that benefits women requiring low secure care
• In the meantime, increased use of private sector low secure beds may predict expansion in this area