Clinical Effectiveness Report Q1 2016/17 papers/Board papers 2016... · Clinical Effectiveness Team...
18
Page 1 of 18 APPENDIX 3 Clinical Effectiveness Report Q1 2016/17
Transcript of Clinical Effectiveness Report Q1 2016/17 papers/Board papers 2016... · Clinical Effectiveness Team...
Page 1 of 18
APPENDIX 3
Clinical Effectiveness Report
Q1 2016/17
Page 2 of 18
1.0 Introduction
This report outlines the key strategic aims identified in the Clinical Audit and Effectiveness Strategy
2016/19. Progress against these strategic aims is monitored by the Clinical Audit and Effectiveness
Committee with implementation being facilitated through the Clinical Care Groups Clinical
Networks. These networks report to the Quality and Patient Safety Committee which has
strengthened its focus during Q1 to provide leadership and support to the clinical networks to drive
the quality improvement agenda.
2.0 Clinical Audit & Effectiveness Strategy
There are four strategic aims set out in the Clinical Audit and Effectiveness Strategy which are
highlighted below together with the progress made during Q1.
Strategic Aim 1
2.1 Practice is based on the best available evidence
Strategic Statement: NICE quality standards set out the way care should be provided and these
standards will increasingly be used to hold our Trust to account for the care we provide. Our
strategy sets out to ensure that we review guidelines and consider variance in practice so that a
plan to fully implement guidelines can be actioned.
The Clinical Effectiveness Team reviews all newly published NICE Guidelines on a monthly basis.
Where a guideline is considered applicable they are cascaded to Associate Medical Directors,
Clinical Care Directors and relevant specialists for full review by the Clinical Care Networks.
The Care Group is asked to consider: Variance in practice between what is being delivered and
recommended in the guideline, consideration to the review or development of policy, procedure,
pathway or audit, potential gaps in commissioning.
The reviews of guidelines are received by the Clinical Audit and Effectiveness Committee and
going forward they will inform the work plan of this group.
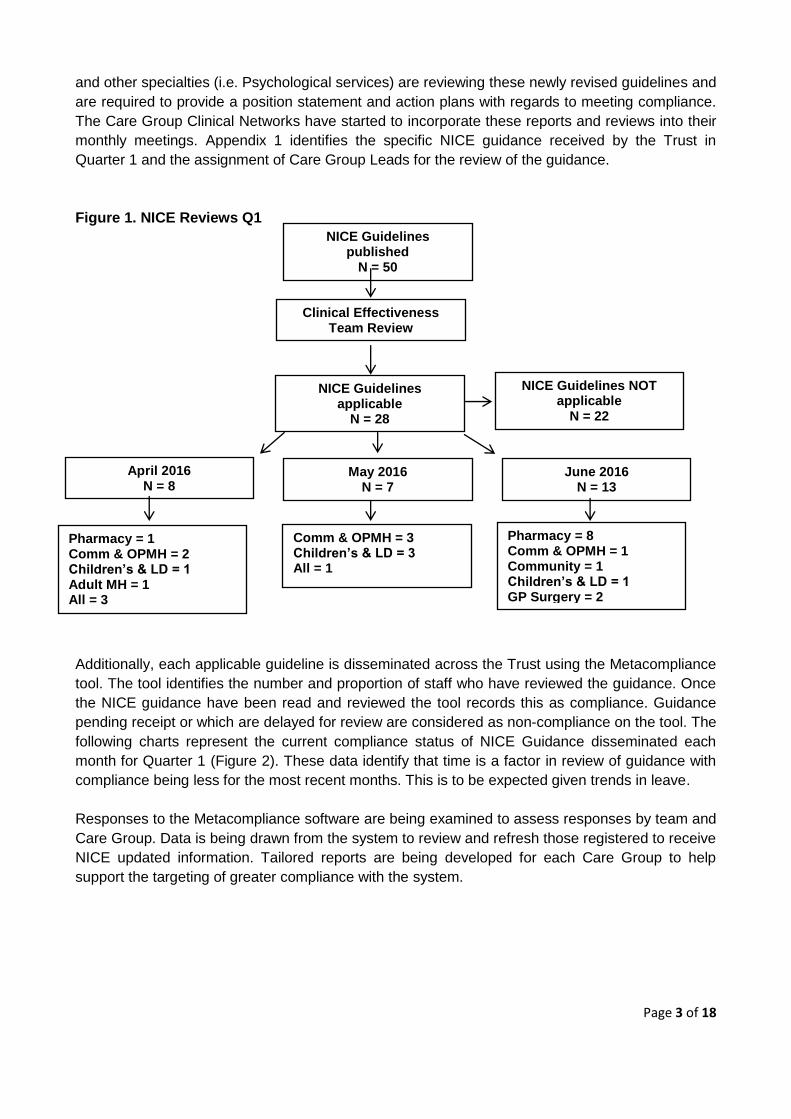
During Quarter 1 a total of 50 Guidelines were issued from NICE of which 28 were selected as
applicable to the Trust (Figure 1). A number of Clinical Guidelines were applicable to more than
one care group or service area, for example:
Antimicrobial stewardship (QS121)
Depression in adults: recognition and management (CG90)
Many of the new or updated guidelines set ambitious recommendations the Trust, for example the
Depression Guideline outlines, “For people with moderate or severe depression, provide a
combination of antidepressant medication and a high-intensity psychological intervention (CBT or
IPT)”. High-intensity psychological interventions (CBT) are defined as 16-20 sessions over 3-4
months. Full implementation of this new guideline may require up to 1,700 sessions of CBT being
available for these patient groups. Consequently, as with all applicable guidelines, the Care Group
Page 3 of 18
and other specialties (i.e. Psychological services) are reviewing these newly revised guidelines and
are required to provide a position statement and action plans with regards to meeting compliance.
The Care Group Clinical Networks have started to incorporate these reports and reviews into their
monthly meetings. Appendix 1 identifies the specific NICE guidance received by the Trust in
Quarter 1 and the assignment of Care Group Leads for the review of the guidance.
Figure 1. NICE Reviews Q1
Additionally, each applicable guideline is disseminated across the Trust using the Metacompliance
tool. The tool identifies the number and proportion of staff who have reviewed the guidance. Once
the NICE guidance have been read and reviewed the tool records this as compliance. Guidance
pending receipt or which are delayed for review are considered as non-compliance on the tool. The
following charts represent the current compliance status of NICE Guidance disseminated each
month for Quarter 1 (Figure 2). These data identify that time is a factor in review of guidance with
compliance being less for the most recent months. This is to be expected given trends in leave.
Responses to the Metacompliance software are being examined to assess responses by team and
Care Group. Data is being drawn from the system to review and refresh those registered to receive
NICE updated information. Tailored reports are being developed for each Care Group to help
support the targeting of greater compliance with the system.
NICE Guidelines applicable
N = 28
Pharmacy = 1 Comm & OPMH = 2 Children’s & LD = 1 Adult MH = 1 All = 3
Comm & OPMH = 3 Children’s & LD = 3 All = 1
Pharmacy = 8 Comm & OPMH = 1 Community = 1 Children’s & LD = 1 GP Surgery = 2
Clinical Effectiveness Team Review
NICE Guidelines NOT applicable
N = 22
NICE Guidelines published
N = 50
May 2016 N = 7
April 2016 N = 8
June 2016 N = 13

Page 4 of 18
Figure 2. NICE compliance as measured using Metacompliance Tool
Key:
I have read and understood the NICE Guidance
Delayed the review of the circulated Guidance (Snooze)
Pending receipt
Strategic Aim 2
2.2 Use the clinical audit programme to improve our services
Strategic Statement: Clinical audit identifies if the care we are providing is in line with recognised
standards. We aim to expand a programme of clinical audits across the services to include the use
of NICE quality standards and Care Quality Commission (CQC), Key Lines of Enquiries (2015). We
will use the themes emerging from serious incidents, adverse events and recorded complaints to
fully inform this programme of clinical audit.
Currently there are 31 clinical audits in progress that have been categorised under the
investigation of compliance with pathways (n=9), medication adherence and processes (n=11) or
clinical assessment procedures to support best practice (n=11) (figure 3). Within the reported
clinical audit activity there 6 National Audits:
Re-audit of Topic 9c Antipsychotic Prescribing in people with Learning Disabilities March
2016
POMH UK 7e Monitoring of Patients Prescribed Lithium
Sentinel Stroke National Audit Programme (SSNAP)
National Pulmonary Rehabilitation Audit (NICE Quality Standard 10)
National Audit of Dementia 2016
POMH UK 11c Prescribing Anti Psychotics for Dementia
A full list of clinical audits can be found in Appendix 2. Nine audits have been agreed and awaiting
to start data collection, one audit is overdue (Audit of HCR-20) with all other audits awaiting
completion and submission. All Audits are being monitored by the Care Groups with reports on
progress being received by Clinical Audit and Effectiveness Group. Outcomes from audits will be
reported from Q2 onwards in this report.

Page 5 of 18
Figure 3. Distribution of Clinical Audits investigating Clinical Pathways, Medication and
Clinical Assessment procedures
Six audits were completed in Q1:
Audit of Effective implementation of care plans to reduce the frequency of restraint and seclusion
Audit of Care Records – Defensible Documentation
Audit of Referrals to Autism Spectrum Disorder Diagnostic Service
Effective documentation of Smoking status and support for smoking cessation in Forensic in-patients
Audit of compliance with venous thromboembolism (VTE) assessment
Substance use disorders amongst inpatients in PICU in 2015 Audit of Effective implementation of care plans to reduce the frequency of restraint and seclusion (Specialist Services) This audit examined three criteria;
To ensure clinical teams have implemented individualised patient care plans to reduce the need for restraint and seclusion.
To determine if Ward Champions to promote this project have been identified from staff and patient cohorts.
To evaluate the frequency of restraint and / or seclusion for each ward across the forensic service.
The audit identified: Compliance with criteria 1 (all patients should have seclusion and restraint reduction plans) fell below the target of 90%. However, it was noted a number of plans were incorporated in other plans of care (eg. risk and relapse care plans). In the 6 month period covered by data collection across the forensic service (1st June 2014 to 30th November 2014) there were 25 recorded incidences of seclusion and 37 episodes of seclusion.

Page 6 of 18
The majority of incidences were attributable to 2 wards (Derwent 16% restraints and 43% seclusions) and Ullswater (76% restraints and 43% seclusions). It was reassuring that all wards have now identified staff and patient ward champions, with the exception of Greentrees and South West Lodge. The Seclusion and Restraint Reduction Group is taking forward key actions. All episodes of
seclusion are being reviewed by Modern Matrons to ensure appropriate plans are in place and
care is reviewed effectively.
Audit of Care Records – Defensible Documentation The Trust has been reviewing the content of care records for each team for a number of years.
Each service reviews n=5 cases per team each month using an online clinical audit tool formatted
through Survey Monkey. During quarter 1 there were n=479 case records reported onto the system
across the trust. The reported outcomes are detailed in table 1, which demonstrate high levels of
compliance with regarding to assessment, risk assessment, care planning and evidence of review,
There is considerable need to develop recorded practice of involving the patient in discharge
planning. Team/service reports are being developed on a monthly basis to target those areas that
require improvement and an Annual Audit Report for 2015/6 is being collated.
Table 1. The proportion of cases meeting Care Records Audit Standards for Quarter 1
(n=479)
Assessment domain %
Achieved
There is an up to date and fully completed assessment in place that identifies the needs of the
person using services.
100
There is an up to date and fully completed risk assessment in place (e.g. Mental Health Risk
Assessment or MUST and Walsall or Waterlow risk assessment in Community Services)
85
There is an up to date care/treatment/recovery plan in place that is based upon assessed
need/risk.
100
The care/treatment/recovery plan has been developed with the person and or their carer (if
applicable)
100
The care and or treatment being provided to the person is in line with the
care/treatment/recovery plan.
98
There is evidence of regular review/s taking place as directed by the care/treatment/recovery
plan.
98
There is clear evidence of discharge planning with the person and or their carer. 16

Page 7 of 18
Audit of Referrals to Autism Spectrum Disorder Diagnostic Service The aims were to assess the compliance of referral process with standards derived from NICE guidance. High levels of compliance was identified in key areas relating to personal history being described in the referral process, however levels of compliance with regards to requesting an opinion and describing the reason for referral were less developed. A template for the referral to the Autism Spectrum Disorder Diagnostic Service is presented to describe and adhere to best practice. Effective documentation of Smoking status and support for smoking cessation in Forensic in-patients The aim was to audit compliance with NICE recommendations on recording of smoking status and provision of information relating to smoking cessation. The audit found that out of 23 patients
16(69.56%) were Smokers
6 (26.08%) were non smokers
1(4.35%) smoking status not known as he was discharged from services. Nursing records were more compliant than medical records with NICE guidance on recording of smoking status on admission (92.86% compared to 35.71%). There was no documentation in the medical records of smoking cessation advice given to patients by doctors on admission.. It was evident on scrutinising the records that in some instances advice had not been given to patients about smoking cessation on admission due to concerns relating to their mental health ie. the patients were so unwell at the time that the information could not be presented in a meaningful way. This should however have been more clearly documented. Nine recommendations were identified with regards to increasing the detection and interventions for smoking including changes to policy and training Audit of compliance with venous thromboembolism (VTE) assessment To provide assurance that community ward and mental health inpatients are appropriately assessed for their risk of VTE and receive the appropriate management as per NICE guidance. Key findings presented in table 2.

Page 8 of 18
Table 2. The proportion of cases meeting VTE Standards
No. Criteria
Compliance in %
1 VTE Assessment completed on admission 82.40%
2 Mobility assessed on admission 89.76%
3 Thrombosis risk assessed on admission, where appropriate 92.91%
4 Bleeding risk assessed on admission, where appropriate 67.72%
5 VTE Assessment decision recorded 87.40%
6 VTE Assessment signed and dated 88.19%
7 24 hour reassessment completed 22.22%
8 Reasons for deviation from recommended pathway recorded 95.28%
9 MAR chart VTE summary section matches assessment decision
86.99%
10 MAR chart prescription section matches assessment decision 85.71%
11 When indicated, pharmacological prophylaxis is administered as soon as possible after assessment completion
96.85%
12 Baseline blood results available 97.64%
Key recommendations included:
Continue the ongoing prescriber induction training programme and ensure this includes community
services prescribers. Continue the ongoing pharmacy visits to inpatient units across the trust;
pharmacy team members to continue to reinforce messages about best practice and trust policy in
relation to the completion of VTE assessments. Continue the ongoing review of VTE policy and
procedures to ensure clear guidance is given to all staff.
Substance use disorders amongst inpatients in PICU in 2015 The aim of the audit was to utilise hospital data to assess the prevalence of patients with
Substance Use Disorders (SUD) admitted to a Psychiatric Intensive Care Unit (PICU), in order to
inform the development of appropriate recovery care pathways.
Key findings included:
Three quarters of admissions to PICU had a drug or alcohol disorder.
Males were more likely to have a diagnosis of SUD than females.
More patients were readmitted who had SUD than without, but the length of stay did was
generally within 56 days as compared to those who did not have a SUD.
The data showed higher prevalence of Substance Use Disorders than previous national
inpatient psychiatric unit studies, which may indicate a difference for the PICU population,
regional variation or increasing substance use, in particular the so called 'legal highs'.
As a consequence of the audit the Dual Diagnosis Project Group are developing a care pathway
for patients presenting with mental disorders and substance use disorders (Dual Diagnosis) in line
with NICE CG120. The project is identifying training for staff working on PICU/Inpatient units on

Page 9 of 18
assessing and managing patients with both substance use disorders and mental disorders (Dual
Diagnosis).
Strategic Aim 3
2.3 Use outcome measures to inform us, our patients, the public and commissioners on
our performance
Strategic Statement: Clinical outcomes play an important role in clinical decision-making. Routine
use of outcome tools allows services across the Trust to assess trends in groups of patients or
specific interventions/care pathways. NICE guidance for specific clinical conditions provides
information on the use of validated tools to support the measurement of clinical outcomes. If
appropriately embedded into practice outcome tools and methods will produce information that
enhances the quality of care.
The Care Pathway Development Group is considering the development of Clinical Care Pathways
regarding, Self-harm, Borderline Personality Disorder, Catheterisation and Pressure Ulcers. This
work has continued to be advanced.. Once care pathways have been drafted and reviewed by
Care Groups through the Clinical Networks these will be presented to the Quality and Patient
Safety Committee for approval and the identification of outcome metrics.
Strategic Aim 4
2.4 Innovate to improve outcomes in a safe and sustainable way
Strategic Statement: Innovation and the introduction of new interventions and technologies are
key drivers for quality improvements that will include the safe introduction of new devices,
procedures and protocols. To ensure our practice is current and developing in accordance with the
future needs of our patients there is a need to look elsewhere within the NHS to identify innovation
that will help transform care. There is emerging evidence that those Trusts involved in research
achieve improved outcomes for patients throughout the organisation through the adoption of a
learning and developing culture to innovative practice.
The Trust is actively involved in a number of clinical research programmes which are looking at
innovative practice such as the well-respected HealthApp project in Learning Disability services
and the ADAM Study that is developing a clinical procedure to support alcohol treatment through
community pharmacies. Additionally, through the R&D Committee research opportunities in
Dementia care, Falls Intervention, Alzheimer’s study, Medically Unexplained Symptoms and
Primary Care are being taken forward.. A full list of studies currently active in the Trust is reported
in the R&D report.
3.0 Care Group Clinical Networks
A new process and structure of reporting regarding clinical audit, effectiveness and quality
assurance has come into effect over the first quarter. Care Groups are currently developing quality
plans aligned to strategic priorities of the organisation, CQC requirements and care group needs.
Reporting against the plans will commence in Quarter 2 with progress updates being reported to
the Quality & Patient Safety Committee.

Page 10 of 18
4.0 Mortality Review & Review of Deaths Report
4.1 Mortality Review
The Trust has developed an approach to undertaking mortality reviews following the deaths of
people with learning disability and or people with mental health problems as part of a CQUIN in
2015/16. This work has enabled the Trust to develop systems and processes with regards to
undertaking reviews. The Trust has adopted the use of the structured case note methodology
promoted by the Improvement Academy and led by Professor Allen Hutchinson. Twenty-one staff
have been trained who work within Mental Health, Older People’s Mental Health and Learning
Disability services.
The process involves the practitioner reviewing the notes and making a judgement on the different
phases of care, the initial assessment and first 24 hours, the ongoing care and the discharge/end
of life and assessment of care overall. Each phase is given a score of between 1-5 with one being
poor care to 5 excellent care.
4.1.1 Summary and Conclusion
The use of this methodology has received very positive feedback from all reviewers, enabling a
comprehensive review of the notes, which is summarised in the structured judgement of the phase
of care.
Whilst the numbers reviewed in Quarter 1 are small (n=4 cases) common themes have been
detected. It is extremely positive that the reviews have found good and in some cases excellent
care in the majority of care being provided to people with learning disability and mental health
problems throughout the patient journey. Feedback of the excellent care has been fed back to
both the individual staff and the wider teams as identified and this has been very well received by
the individuals and staff teams. Areas for improvement in terms of care delivery have been
discussed with services to identify areas for learning.
The learning from the development of the mortality reviews has been integral to the development
of Trusts approach to the overall management of unexpected deaths.
5.0 Tissue Viability
The Tissue Viability team and the community/inpatient nursing teams workload is challenging and
demanding due to an ageing population with more complex co-morbidities, that put the patients at
an increased risk of skin break down due to the increasing risk factors.
Pressure ulcers have become a more focussed subject over the last year in an attempt to manage
the increasing risk. We have piloted the SKINN bundle which was found to be unsuitable for
community use in its current format as it was designed for more acute inpatient units. Additionally
the service has provided e- learning packages for Nursing homes and continued to provide
modular tissue viability courses running up to 6 times per year, with a significant focus on pressure
ulcer prevention and management.
New developments over the last quarter include:

Page 11 of 18
Pressure forum/group, consisting of the Head of Nursing, Safeguarding, Matrons and
Tissue Viability. This will review the overall findings and actions of the root cause analysis
and consider how the identified actions could be implemented across the patch to improve
outcomes.
The Root Cause Analysis [RCA] tool is continually being reviewed and revised to reflect the
ongoing investigations to ensure the right information is captured at the right time then
acted upon. Recent improvements have been the specific addition of the duty of candour
and the Safeguarding section. This is hoped to improve communication, documentation and
ultimately the patient’s safety and best interest.
The Datix are all reviewed by the Lead for Tissue Viability who makes recommendations for
any actions to be employed by the Matrons/Investigators whether an RCA is required or
not. This might be for example the need for a Doppler ABPI as part of the holistic
assessment if the pressure ulcer is below the knee.
The RCA as a process has now changed and the investigation is led by the Matron and a
local clinician. This ensures that the actions are owned by the team hoping to reduce the
risk and improve outcomes in a timely manner to meet the patient and organisation needs.
The Tissue Viability team has collaborated with another Trust and Industry to provide a
pressure ulcer prevention and management DVD. It is hoped this might be more accessible
to home care staff and easier for them to use as an aide memoire.
The pressure ulcer policy is to be reviewed and refreshed earlier than planned to reflect the
changing pressure ulcer landscape.
There are draft documents of pressure ulcer prevention and management pathways that
have been developed to reflect NICE guidance. They will be added to the policy once
approved.
There has been the development of a pressure ulcer tracker that allows us to see where in
the process the investigation is at and how it is developing.
We are also ready to go live with a virtual visit pilot to allow us to offer greater support to
the more rural areas within our geographical patch. This should have a significant outcome
as to how we manage and support the patients in the community.
The pressure ulcer quarterly report identifies that Grade 1 and Grade 2 pressure ulcers remain
static this quarter with reductions being observed in Grade 3 reported pressure ulcers. There is a
slight increase in the very small numbers of reported Grade 4 pressure ulcers.
Root Cause Analysis investigations are undertaken by the locality Matrons to identify areas of
learning for each pressure ulcer graded 3 and above. The RCA provides an outcome assessing
how avoidable the pressure ulcer was, which is used to inform learning and changes to practice.
score for each investigation
Each locality is developing quality improvement plans based on the findings of RCA investigations
which include pressure ulcer quality forums where the Matron presents findings from their
investigations.

Page 12 of 18
6.0 Overall Summary
The systems, processes and structures that underpin the promotion and monitoring of clinical audit
and application of evidence base practice continue to develop. There is an increasing knowledge
and use of NICE and best practice in the development of services and policies being undertaken.
Over the last quarter the Clinical Effectiveness Team has been enhanced by the inclusion of a
Clinical Effectiveness Nurse (Band 7) to support the Clinical Audit and Effectiveness work plan.
The refresh of a comprehensive Audit Plan that embraces NICE Clinical Guidance and Quality
Standards in the quarter identifies the commitment to analyse clinical performance against best
practice. The challenge for Care Groups will be the resourcing of these programmes of work.
The processes for acceptance and review of NICE guidance are currently under review with a
focus on the re-adoption of the HealthAssure NICE compliance tool. The continued review of
bespoke thematic reviews continues to inform quality improvements and service developments.
The Nursing & Quality Directorate and Care Groups are refining the plan and reporting processes
to ensure quality programmes fully enhance the development of practice.

Page 13 of 18
Appendix 1: NICE Guidance received by the Trust: Care Group Assigned for Review Table 1 - Applicable NICE Guidelines April 2016
Title Ref no Care Group
Controlled drugs: safe use and management
NG46 Pharmacy
Routine preoperative tests for elective surgery NG45 Community & OPMH
Updated Venous thromboembolism in adults: diagnosis and management
QS29 All
Updated : Antenatal care QS22 Children’s & Learning Disability
Updated : Stroke in adults QS2 Community & OPMH
In development Antimicrobial stewardship QSD All
Antimicrobial stewardship QS121 All
Updated : Depression in adults: recognition and management
CG90 Adult Mental Health / Community & OPMH
Total = 8
Table 2 - Applicable NICE Guidelines May 2016
Title Ref no Care Group
Canagliflozin, dapagliflozin and empagliflozin as monotherapies for treating type 2 diabetes
TA390 Community & OPMH
Updated Tuberculosis NG33 All
Updated Psychosis and schizophrenia in children and young people: recognition and management
CG155 Children’s & Learning Disability
Updated Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer's disease
TA217 Community & OPMH
Updated Jaundice in newborn babies under 28 days CG98 Children’s & Learning Disability
Updated Dementia: supporting people with dementia and their carers in health and social care
CG42 Community & OPMH
In development Neonatal jaundice diagnosis (SC update)
CG Children’s & Learning Disability
Total = 7
Table 3 - Applicable NICE Guidelines June 2016
Title Ref no Care Group
Complicated urinary tract infections: ceftolozane/tazobactam ESNM74 Pharmacy
Complicated intra-abdominal infections: ceftolozane/tazobactam
ESNM75 Pharmacy
S-Cath System for suprapubic catheterisation MIB68 Community Services
Bronchiolitis in children QS122 Child & LD

Page 14 of 18
Title Ref no Care Group
Home care for older people QS123 Community & OPMH
Suspected cancer QS124 GP surgery
Adalimumab for treating moderate to severe hidradenitis suppurativa
TA392 Technical Appraisal process
Alirocumab for treating primary hypercholesterolaemia and mixed dyslipidaemia
TA393 Technical Appraisal process
Evolocumab for treating primary hypercholesterolaemia and mixed dyslipidaemia
TA394 Technical Appraisal process
Ceritinib for previously treated anaplastic lymphoma kinase positive non-small-cell lung cancer
TA395 Technical Appraisal process
Trametinib in combination with dabrafenib for treating unresectable or metastatic melanoma
TA396 Technical Appraisal process
Belimumab for treating active autoantibody-positive systemic lupus erythematosus
TA397 Technical Appraisal process
Breast cancer QS12 GP surgery
Total = 13

Page 15 of 18
Appendix 2: Clinical Audits by Care Group - Quarter 1 2016-17
Status Key:
Tables 1 - 4 show further details of clinical audit status per care group for Quarter 1.
Table 1 - Children’s & Learning Disability
Red Audit overdue
Amber Awaiting actions to be completed
Green Data collection ongoing/All actions completed
Blue Audit agreed but not yet started
Care Group Audit ref Audit title National/Local audit Rating
Child & LD MHLD111 Audit of referrals to Autism Spectrum Disorder Diagnostic Service Local
Child & LD MHLD112 Audit on monitoring baseline physical health parameters in patients admitted to Townend Court and on antipsychotics
Local
Child & LD MHLD114 Re-audit of Topic 9c Antipsychotic Prescribing in people with Learning Disabilities March 2016
National
Child & LD MHCS116 Audit of off license prescribing done in CAMHS Local
Child & LD POMH-UK Topic 7e
POMH UK 7e Monitoring of Patients Prescribed Lithium National
Child & LD MHMS163 Audit of Care Records – Defensible Documentation Local

Page 16 of 18
Table 2 - Community & Older People’s Mental Health
Care Group Audit ref Audit title National/Local audit Rating
Community & OPMH
EYCT106 Sentinel Stroke National Audit Programme (SSNAP) National
Community & OPMH
EYCT107 Nutrition Mission Silver Award Audit (amended from EYCT105 which did not go ahead)
Local
Community & OPMH
MHAD278 National Pulmonary Rehabilitation Audit (NICE Quality Standard 10)
National
Community & OPMH
MHOP204 National Audit of Dementia 2016 National
Community & OPMH
MHOP205 Re-audit of MHAD254 : VTE assessment and prophylaxis in Mill View Lodge (Old age psychiatric ward)
Local
Community & OPMH
MHOP206 POMH UK 11c Prescribing Anti Psychotics for Dementia National
Community & OPMH
CT1 Clinical Outcomes Project - Podiatry Local
Community & OPMH
MHAD297 Audit of venous thromboembolism (VTE) assessment in community ward and MH inpatients
Local
Community & OPMH
SI-2015-23470 Audit of team record keeping audits within clinical network to identify individual and team level of adherence to standards
Local
Community & OPMH
POMH-UK Topic 7e
POMH UK 7e Monitoring of Patients Prescribed Lithium National
Community & OPMH
MHMS163 Audit of Care Records – Defensible Documentation Local

Page 17 of 18
Table 3 - Mental Health
Table 4 – Specialist Services
Care Group Audit ref Audit title National/Local audit Rating
Mental Health MHAD294 Compliance with monitoring of plasma lithium levels under shared care criteria
Local
Mental Health MHAD293 Re-audit of the Use of PRN Medications in Newbridges and Westlands
Local
Mental Health MHAD285 Re -audit of the Electroconvulsive Therapy (ECT ) Policy and Clinical Guidelines.
Local
Mental Health MHAD296 Audit of the quality of referrals into adult community mental health teams
Local
Mental Health MHAD298 Drug and alcohol use in patients admitted to Psychiatric Intensive Care Unit in 2015
Local
Mental Health POMH-UK Topic 7e POMH UK 7e Monitoring of Patients Prescribed Lithium National
Mental Health MHMS163 Audit of Care Records – Defensible Documentation Local
Care Group Audit ref Audit title National/Local audit Rating
Specialist MHFS110 Effective documentation of Smoking status and support for smoking cessation in Forensic in-patients
Local
Specialist MHFS109 Audit of Effective implementation of care plans to reduce the frequency of restraint and seclusion
Local
Specialist MHFS111 Re-audit of MHFS108: Compliance with T2 & T3 related to prescription charts
Local
Specialist MHSM110 Re-audit of MHSM107 the risk of QTc interval prolongation with methadone
Local
Specialist SI-2015-29198 Audit of HCR-20 completed prior to leave Local
Specialist POMH-UK Topic 7e POMH UK 7e Monitoring of Patients Prescribed Lithium National
Specialist MHMS163 Audit of Care Records – Defensible Documentation Local

Page 18 of 18