
CLINICAL CONFERENCE - Homepage | Circulationcirc.ahajournals.org/content/18/5/924.full.pdfCLINICAL...
12
CLINICAL CONFERENCE Editor: EDGAR V. ALLEN, M.D. Associate Editor: RxYMIONXD 1). PRIUITT, 2M.D. Syndrome of Carotid Artery Insufficiency Early Clinical Recognition and Therapy By LAMUAR E. CREVASSE, M.D., R. BRUCE T.OGUE, AI.D., AND J. WILLIS HURST, ,M.D. D R. IA)(iIE: Carotid artery insufficien- cv is a relatively common lut frequent- ly unirecoogitized syndrome. Fisher' in 432 consecutive autol)sies in which the brain and carotid arteries were studied found 28 cases of (ompl)lete occlusion of one or both carotid arteries. T Ii irteen cases showed very severe narrowineg of the arterial lumina, making a total of 9.5 per cent with advanced carotidl disease. The classic concept of carotid ar- tery thronhol)(sis, Iiamely monocular blindness and contralateral hemiplegia, is the exception rather than the rule, since visual (listurbances occur in on0ly\ 15 per cent. Furthermorc, about 15 per cent of l)atients with carotid artery thronibosis miay have no synliptoms.' Like atherosclerotic occiusiotis in other ves- sels, occlusion of the internal carotid artery is more common ini the male over 40, although the age gronl) varies from 13 to 85 years. Occlusions ini the younger age group are not infrequent. Am my disease process producing occlusive vascular disease may be implicated. By far the most frequent offender is athero- sclerosis with a normal bloo1( pressure. Hy- pertensive persoits for some unknown reason are less frequently affected by this syndrome. Angiitis of any cause, trauma, embolus, coml- pression of the internal carotid by the lateral process of the atlas,2 and rarely syphilis have been implicated. FroIm the Department of Medicine, Emory Unii- versity School of _Medicine and the AMedical Services of Emory University and Grady _Memorial Hospitals, Atlanta, Ga. The arterial blood supply to the head is illustrated in figure 1. The internal carotid artery bifurcates froni the common carotid artery distal to the carotid bulb amtd courses through the retrophar.yngeal space into the cranium, givingfr off as its first branch tbe oph- tihalmic arterv. The central retinial artery branches froimi the ophthalmic coursing through the optic nerve furnishing the blood supply to the retina. It is an end artery with no collateral circulation. Other branches of the ophthalmmmic, however, have rich collateral circulation, with 1)oth the ipsilateral external carotid and cotitralateral internal and exter- nal carotids. Tue internal carotid artery subsequently bra iches into the posterior com- mullicatin g-r, anterior choroidal, anterior an(l middle cerebral, thus providing the blood su)- ply for the homnolateral retina, frontal, tent- poral, parietal lobes and posterior limb of tlhe internal capsule. The cliiiical patterin of the syndrome and specific symptoms are deter- mined by the adequacy of the collateral cir- culation. Approximately 15- per cent of the patients with complete carotid occlusion may have no neurologie symptoms because of ade- quate collateral circulation. In the past, the finding of thrombosis of the internal carotid artery has commonly beeti attributed to retrograde extension from the middle cerebral artery, rather than originat- ing front the cervical portion of the carotid artery. Routinie atutopsyexav exnmiiatiolts of the cervical portioit of the itterital carotid is seldom done. It is well to note that in Fish- Circulation, Volume XVIII, November 1958 924 by guest on June 17, 2018 http://circ.ahajournals.org/ Downloaded from
-
Upload
phungxuyen -
Category
Documents
-
view
217 -
download
2
Transcript of CLINICAL CONFERENCE - Homepage | Circulationcirc.ahajournals.org/content/18/5/924.full.pdfCLINICAL...

CLINICAL CONFERENCEEditor: EDGAR V. ALLEN, M.D.
Associate Editor: RxYMIONXD 1). PRIUITT, 2M.D.
Syndrome of Carotid Artery InsufficiencyEarly Clinical Recognition and Therapy
By LAMUAR E. CREVASSE, M.D., R. BRUCE T.OGUE, AI.D., AND J. WILLIS HURST,,M.D.
D R. IA)(iIE: Carotid artery insufficien-cv is a relatively common lut frequent-
ly unirecoogitized syndrome. Fisher' in 432consecutive autol)sies in which the brain andcarotid arteries were studied found 28 casesof (ompl)lete occlusion of one or both carotidarteries. TIi irteen cases showed very severenarrowineg of the arterial lumina, making atotal of 9.5 per cent with advanced carotidldisease. The classic concept of carotid ar-tery thronhol)(sis, Iiamely monocular blindnessand contralateral hemiplegia, is the exceptionrather than the rule, since visual (listurbancesoccur in on0ly\ 15 per cent. Furthermorc,about 15 per cent of l)atients with carotidartery thronibosis miay have no synliptoms.'Like atherosclerotic occiusiotis in other ves-sels, occlusion of the internal carotid arteryis more common ini the male over 40, althoughthe age gronl) varies from 13 to 85 years.Occlusions ini the younger age group are notinfrequent. Am my disease process producingocclusive vascular disease may be implicated.By far the most frequent offender is athero-sclerosis with a normal bloo1( pressure. Hy-pertensive persoits for some unknown reasonare less frequently affected by this syndrome.Angiitis of any cause, trauma, embolus, coml-pression of the internal carotid by the lateralprocess of the atlas,2 and rarely syphilis havebeen implicated.
FroIm the Department of Medicine, Emory Unii-versity School of _Medicine and the AMedical Servicesof Emory University and Grady _Memorial Hospitals,Atlanta, Ga.
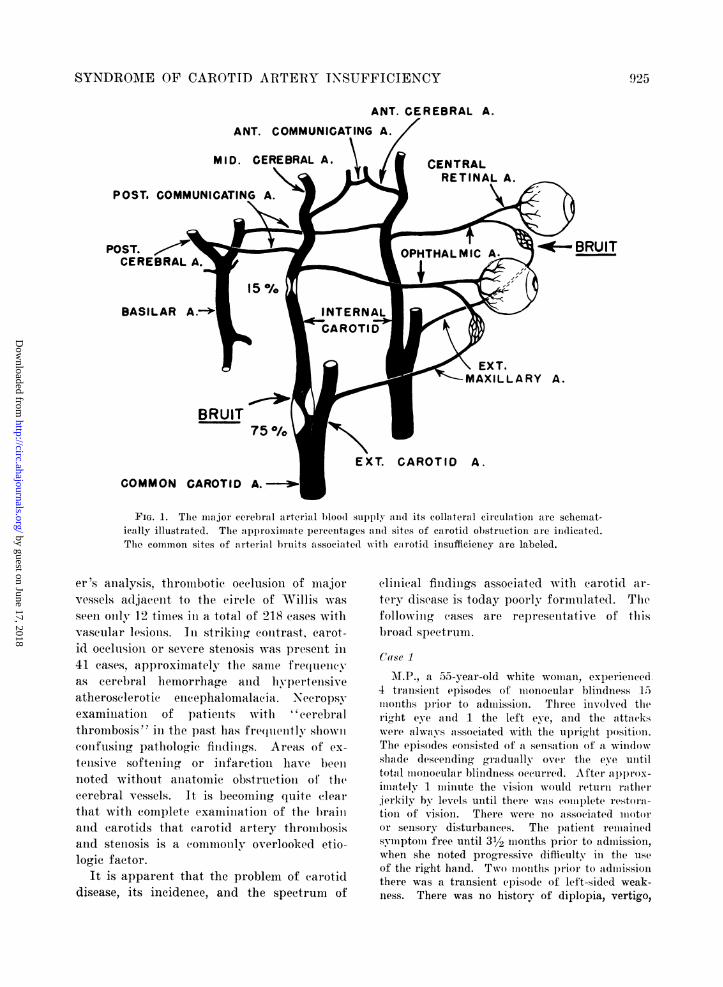
The arterial blood supply to the head isillustrated in figure 1. The internal carotidartery bifurcates froni the common carotidartery distal to the carotid bulb amtd coursesthrough the retrophar.yngeal space into thecranium, givingfr off as its first branch tbe oph-tihalmic arterv. The central retinial arterybranches froimi the ophthalmic coursingthrough the optic nerve furnishing the bloodsupply to the retina. It is an end artery withno collateral circulation. Other branches ofthe ophthalmmmic, however, have rich collateralcirculation, with 1)oth the ipsilateral externalcarotid and cotitralateral internal and exter-nal carotids. Tue internal carotid arterysubsequently braiches into the posterior com-mullicatin g-r, anterior choroidal, anterior an(lmiddle cerebral, thus providing the blood su)-ply for the homnolateral retina, frontal, tent-poral, parietal lobes and posterior limb of tlheinternal capsule. The cliiiical patterin of thesyndrome and specific symptoms are deter-mined by the adequacy of the collateral cir-culation. Approximately 15- per cent of thepatients with complete carotid occlusion mayhave no neurologie symptoms because of ade-quate collateral circulation.
In the past, the finding of thrombosis of theinternal carotid artery has commonly beetiattributed to retrograde extension from themiddle cerebral artery, rather than originat-ing front the cervical portion of the carotidartery. Routinie atutopsyexavexnmiiatiolts of thecervical portioit of the itterital carotid isseldom done. It is well to note that in Fish-
Circulation, Volume XVIII, November 1958924
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from
SYNDROME OF CAROTID ARTERY INSUFFICIENCY
ANT. CEREBRAL A.
ANT. COMMUNICATING A.
MItD. CEREBRAL A. CENTRALRETINAL A.
\ EXT.-MAXILLARY A.
BRUIT
CAROTID A.
COMMON CAROTID A.
FIG. 1. The major cerlel)i.rl arterial b)loo00 supply and its collateral circulation are schemnat-ically illustrated. The approximate percentages aIl(l sites of carotid obstructioIl are indicated.The common sites of arterial bruits associated wvith ecarotid insufficiency are labeled.
er 's analysis, thrombotie occlusion of majorvessels adjacent to the circle of Willis wasseen only, 12 times ini a total of 218 eases withvascular lesions. Iin striking contrast, carot-id occlusion or severe stenosis was present in41 cases, approximately the same frequencyas cerebral hemorrhage and hypertensiveatherosclerotic enceephalomalacia. Necropsyexamination of patients with ''cerebralthrombosis" in the past has fre(luently slhownicotifusing pathologic findin.gs. Areas of ex-tensive softeninog or infarction have beeiinoted without aniatomic obstruction of thecerebral vessels. It is becoming quite clearthat with complete examination of the l)railland earotids that carotid artery thrombosisand stenosis is a commonly overlooked etio-logic factor.
It is apparent that the problem of carotiddisease, its incidence, and the spectrum of
clinical findings associated with carotid ar-tery disease is today poorly formulated. Thcfollowinlg cases are represelltative of thisbroad spectrum.
Case 1
a 55-year-old white woman, experienced4 transient episodes of monocular blindness 15months plrior to admission. Three involved theright eye and 1 the left eye, and the attafckswere always associated with the upright position.The episodes consisted of a sensation of a windowshalde deseending graldually over the eye untiltotal Monocular blindness occurre(l. Aofter. appllOx-imatelv 1 minute the vision would return rathjerkily by levels until there was eomplete restoml-tioIi of vision. There were no ,assoeiateld motoror sensory disturbanees. The patient remainedsymptom free until 31/2 months prior to admission,when she noted progressive difficulty in the useof the right hand. Two months p1ri' to a(ldllissiolithere was a transient episode of left-sided weak-ness. There was no history of diplopia, vertigo,
POST.
POST.CEF
BASILAR
925
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from

(REVASSE, L( )( I TE, IT1TI'
CONTINUOUS MURMUR RIGHT SU PRA CLAVI CULAR FOSSAr. . ~~~~~~~~~~~~~~~~~~~~~~~~:~~~~~
MARKED ACCENTUATION OF CONTINUOUS MURMUR
WITH CONTRA LATERAL CAROTID COMPRESSIONL. * I -!,,, ;?!:; I 1, . .............:'I'-t 11 .-
t~~~~~~~~~~h-~~~~~~~~~.......... . !,I: ::
._ ...............~~~~~~~~~~~~~~~... ........... -;;
.... .. .. ... .__.__........ ... _...__.... .,....
ALL STETHOGRAMS SEN - 6 PAPER SPEED 25mm./ Sec.
IF G.. ' \\ lo0n1i i/l colit ilil(ilis 1111,1 liii at t el(i1,, oof the neck ini the righlt s~ l l ;ieilafOSSXl ill thel aorttia a1(1rel 11( llie. A f;iiit s\-stoli(' Iiiiui'riii is t insull iitted opl) the right carotidonly. Thses marked la (('clint-uatio Ot tle('li iliiiiliii 1' ll' 011 (Contrl' hiternil (e'1 'otid co( mplrii essionis relatedl to an inereaise in s*stolie 11d (liaistol i(' pr'('ssure gradI eats aIl(oss the rtialy
obstructed right ii111111iii;ite bY torill tilelr re lletion il col l . bl11oodl flo\.
01 dysllpasia. Iler father (lied(l of a1 eele)1'a
vascular accident at age 7:3 11d(1 sister (lied of'
coronary thromlbosis at age 43. The blood pIles-sure was 140/90 minl. 1Ig in the left aria all(d110/90 m1n. 1ig ill the ri-ht. The rigiht r(Iial
pulse was diminished. The a(.1iloti(l vessels pul-sated vigorously to the angle of the jaw. Auscul-tationi over the right carotid 'eeale(l al barshgrade III systolic murmur. There was a palpablethrill over thre left carotid bulb, <(11( a grade III
continuous murinur was presellt. Changes ilposition, jugular coim1pression, .cand the Valsallvamianeuver l)Produced 11o app eciable chanoes inthe mIurmaurs. There w's 10o evidence of venious
collaterals. Carotid compression just proximal tothe bulb obliterated thie umlurnur Onl the ipsilateralside and a ccentunte(l the cointralateral Illurillur.
O01 comupression of tlie left carotid artery thepIreviouxsly noted svstoli( ie1mlll'uIUr ovelr the ri-lltcarotid bull) becaime conitillUOus. There was bi-
lateral diminiutioni of the plharyvl-eal carotioll)ulsations and(] tllis .1s more evident oln the le ft.
Th'lei visual fields were normnal. The fundi revealedII changes. The heart was not enlarged
allld there was a grade 1 to 11 nortic svstoli-Illurlllur. Tlhe mneurolog'ic exauminuationr was nrel'a-
tive excelt for miiotor weakness of the right afruia.
The cranial nerves were i'itact, save for sliglt
flattenuing of tlhe' left nasolabial fold. The re-
mnainder oif the neurolog)ic examuninationr was nornila1.The electrocardiogramii was norummal. X-r.ays ofthe skull and neck revealed calcium plaques in thecaroti(l arteries. The serumr cholesterol was 299ag,. per cent. The e1letroenic(phaloglsrami was
normal1. Following complll)ression of alternatecarotids for 10 seconds frontal dsrliytlhini(cc'lianIges occurred oll the side of carotid compression.
The lpatient exp)eriellced onle( episode of' left-
sidle(l W'eakness concomitant with a drop ill )lomd
I)1essure from 141) 90 to l'0 8(), probably induced1)v oversedation. Function ralpi(llv returned witlilestoratioll of blood pressure to the previouls levels.The patienut's conudition has remmiained stable on
shloirt-teri a nticoagulanat the apy.
926
* A .1.
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from
SYNI)H( )i\E' ( )JI' (AP12()TII) A1lTErY IN'SV1'F1(IEN\92
STETHO- LOCALIZED CONTINUOUS MURMUR OVER LEFT CAROTID BULB.
;.~~~ ~ ~ ~ ~~~o -AIA":t4'51t 'h -jl0r 0 F- i hi _
_ * ~~L-. 7....14__*_; ;:. ~-
STETHO- 5 CMS BELOW CAROTID BULB ON IPSELATERAL COMMON CAROTID
BOTH STETHOGRAMS RECORDED - SEN-6 - PAPER SPEED 75 MM / SEC.
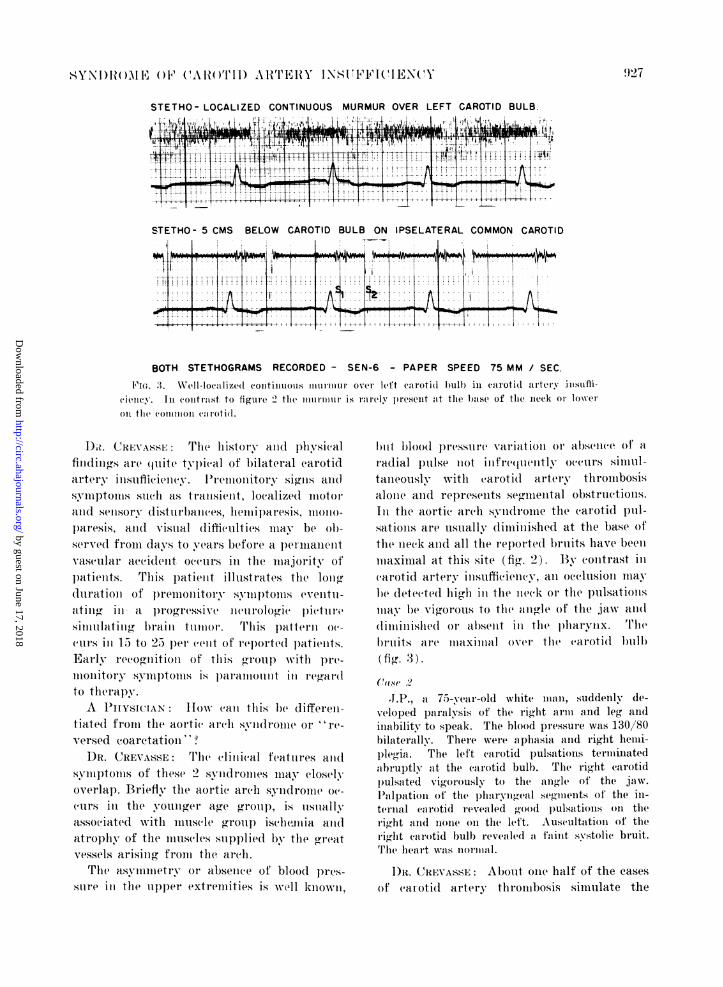
F.Ia. .3. W\ell-lIo(lized CoiitiiilXot 1111111M11MM Ov. Ift C.roti l in carotidl artery insuffi(i^lell. 1it contrast to figure 2' the murninr is iaiely present at the biase of the ineek or lowero1i the (0o11111oll (calotid.
D1). CREVASSE: The history and physical
finidings are quite typical of bilateral carotidartery iPisufiieiiev. l'remnonitory signsl aiud
symptoms such as transient, localized imotor.and senisory disturbanices, hem iil)aresis11,m1ono-
paresis, a11(l visual (difficulties mnay be Ob-served from davs to years before a I)ernilalelntvascular accident occurs in the majority of
patients. This patient illustrates the lonogduration of premoinitory smmptoms cventu-aIting. ini a )rogressive leurologic pictuire
silattinig brain tuimor. 'T'his l)attern oc-
('illrs in 15) to 25 p)er' ((cit of rle)orted Ilatielits.Early irecog(niitioin of this gr&oulp with pre-
nIonitory sympi)tomsl is llaramoiunilt inl regi(l
to therapy.A PHYSICIAN low ca(i this be differein-
tiate(1 from the aorti(' archl svyndro(me or "re-versed coaretation''?
DR. CREVASSE: Thie cliiical features and(symlll)toflls of these 2 syndromes imlay closelyoverlap. Briefly the aortic arch syndroie oc-
(ul.rs iii the younger age group, is usuallyassociated with muscle group) ische..mia and
atrophy of the muscles supplied by the grecatvessels arisintg from the arch.
The asvNiuniiietr- or absenice of bloocl l)les-
suire ini the upper extremities is wel1 known,
) ii b)10( p)r(sLue variationi or alm;ence of a
radial pulse not iuire neatly occurs simuli-tanieously with earoti(l artery thrombosisalone anid represents segmental obstruetions;.Ini the aortie areh svid(lroiiie the carotid pill-sations are usually dimujiuished at the l)ase ofthe ineek amnd all the reporte( bruits have beenmaximal at this site (fig. 2). Bly contrast in('arotid artery imsuftici(ency, all occlusioilmaybe detected(l hihl in the nmeck or the pulsationsmay b)e vigorous to tlhe angfle of the jaw all(ddliminishie(l or albsellt iin teIme)llatrynx. 'T'hbIrits are maximal o(er the (caroti(l bulb
(fi(r. 3).Ca1Se .2
,I.P.a71-year-old white mian, suddenlyv de-veloped paralysis of the right aria and leg andinability to speak. The blood pressure was 130/80hilaterally. There were aphasia anid right heini-ple'gia. The left carotid pulsatiotis terminatedabruptly at the carotid bulb. The right carotidl)ulsiated vigorously to the angle, of the jaw.Palpation of the sharyngeal setientof the in-ternal carotid revealed good l)ulsatiolis on1 ther'i(g.ht and none on the lett. Auseultation of theii-lit carotid bulbl reveale(l a faint systolic bruit.Tlhe heart was norlmIal.
D)R. CREVASSE: About oie half of the casesof caarotid artery thrombosis simulate the
9}27
0
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from
CREVASSE, OUGUE, HURST
A HORIZONTAL B 700 MINI-7 l-7--------/ -2-8 8
8-6-
73 7-341/g4-8 4-8
BP 144/78 BP 100/605-6-
M.S.
4 50 UV S
SEC
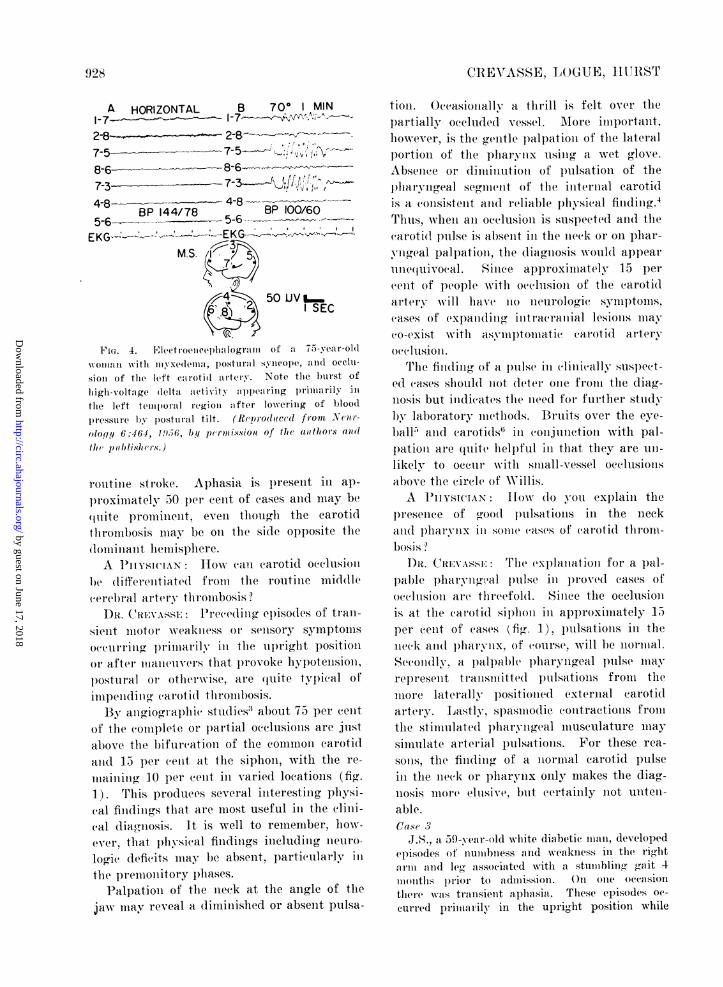
F ir. 4. Eletro e phalogram of a 75- ear-ol01woman with ityl xedemna.t, postural synicoieo , and occlti-sion of tlme left earotid artery. Note time burst of
luigl- voltage (lelta acetivity lappearing primarily iII
time left temporal legion :after lowering of blood
pressure b)y postural tilt. (R(prod(lce(d(1 front Nc o-
olofl/y 6:464, 19W.,6, by pernission of tie authors and
thl)(liosh8r.)
routine stroke. Aphasia is present in ap-
proximately 50 per cent of cases and may be(luite lprominent, even though the carotidtlhrombosis mnay be oml the side opposite the
1loiuiaiit hemisphere.
A 1PiYS1CIAN: Ilow (ca1in carotid o(clusionibe (liflerelitiated frolln the routine middle
cerebral artery throinbosis
DR. CREVASSE: Precediiing episodes of tran-
sient motor weakitess 0r se sory symptomls
o(eurriiig l)rimiiiaiily- ill the up right positioi
or after mtanetIvers that l)rovoke hylpotensiomi,p~ostulral or otleisi, are quite typical of
iiospetlirl (r carotir tisroe osis.By angioi(ral)lpi( stu(lies' about 75 per cent
of the coml)leie or l)artial occlusions are justabove the bifurcation of the common carotidamid 1 5 per cent at the siphon, with the re-
mainiiig 10 per cent ill varied locations (fig.
1). This produces several interesting pliysi-(al findings that are most useful in the clini-cal (liag.,iiosis. It is well to remember, how-ever, that p)lysieal findings including iieuro-
logic (leficits may be absent, particularly iil
the premoititory phases.
Palpatioii of the neck at the angle of the
jaw may reveal a diminished or absent pulsa-
tiOl. OccasionalvN' a thrill is felt over thepartially ochluded 'vessel. Mtore important,however, is the genitle l)alI)atiomi of the lateral
portion of the pharyox using a wet glove.Absence or dimitiution of pulsation of the
hpharyiLgeal segment of the iiiteriial caroti(lis a (onisistelit and reliable physical findinig.4Thus, when ani oeclusioii is susj)ected and the('aroti(l pulse is absent in the nieck or on phar-yngreal palIpatioln, the diagnosis would appearime(uivocal. Since approximately 15 percent of people with ocecltisioni of the carotidartery will have no neurologie sylnl)tOlis,('ases of cxj)andcillg initracrlaniial lesion.s llmayco-exist waith asympll)tomiiati( carotid arteryocclusioi .
Trhe finiding of a )nulsc ini (cliniically. suspect-ed cases should uot deter one from the diag-nosis but inidicates the liee(d for further studyby laboratory methods. Bruits over the eye-
ball5 and carotidZs inl conjunction with pal-
p)atiom are quite helpful iii that they are uli-likely to occur' w-ith small-vessel occlusionsabove the eircle of Willis.A IMi1YSlCIAN lIow (1o vou exilaiti the
presence of good p)ullsations in the neckAtrid p)harvhxiix sonc cases, of earoti(l thirom-bosis ?
l)D. CREVAS'SI: The cxlplaiiatioii for a l)al-pable pharyngeal pulse iii l)roved eases of
'cclusion are threefold. Sincee the ocelusionis at the caroti(l sip)holi in approximately 15per cent of cases (fig. 1), I)lulsations ini theneck and pharyiix, of (ours(e, will be nonnal.Se.ondlNly, a l)allalule p)haryngeal p)ulse mayrepresent transmitted pulsations from themore laterally positioned external carotidartery. Lastly, spasmiodic contractions frontthe stimulated phary igreal musculature maysimulate arterial pulsations. For these rea-sons, the finidingt. of a normnal carotid pulsein the neck or plharynx oiily makes the diag-nosis more elusive, but certainly not unten-able.Case 3
J.S., a 59-year-old white diabetic man, developedepisodes of nuiiibness and weakness iii the rightaria and le, associated with a stumbling' gait 4illonitis prior to admission. On one occasiontliere was transient aphasia. These episodes oc-curied priimarily in the upright position while
928
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from
SYNDROME OF CAROTID ARTERY INSUFFICIENCY
working, lasted 4 to 5 minutes, and promptlycleared with rest. After being given a Rauwolfiapreparation because of mild hypertension, thepatient noted a marked increase in number ofthese episodes. He discontinued his medicationand there was an abrupt decline from 10 to 15to approximately 1 such episode each day. Theblood pressure was 190/90. The fundi showedgrade II changes. The right posterior tibialpulse was absent. The left carotid pulsationswere absent below the angle of the jaw. Theright carotid pulsated vigorously. The pharyngealsegments were not palpable. There were no bruitsover the head or carotids. The neurologic exam-ination was normal. The electrocardiogram re-vealed left ventricular hypertrophy. The serumcholesterol was 360 mg. per cent. Anticoagulanttherapy was instituted and there was no recurrenceof symptoms during a short follow-up period.
DR. CREVASSE: This case demonstrates aphenomenon that may occur in patients withcerebral vascular disease treated with hypo-tensive agents. The pathophysiology of thesesymptoms now seems clearer. In general, 55to 60 mm. Ilg is the critical systolic bloodpressure to maintain adequate cerebral cir-culation, but with a compromised cerebralvascular circulation the critical blood pres-sure is considerably higher, and seeminglyinsignificant falls in blood pressure may causesignificant symptoms. Shanbrom and Levy7observed the appearance of hemiplegia in acase of carotid thrombosis when the bloodpressure fell below 160 mm. Hg followingcarotid arteriography. When the blood pres-sure was maintained above this level by vaso-pressor agents, the hemiplegia would resolve,only to reappear when the pressure fell againbelow this level. We have recently observeda patient with basilar artery insufficiencywith tetraplegia precipitated by a fall inblood pressure from 200/110 to 130/110 in-cident to myocardial infarction. Restorationof function on 1 side with clearing of the sen-sorium rapidly occurred when the blood pres-sure was again maintained with vasopressoragents at 200 mm. systolic.Meyer et al.8 studied a group of 36 pa-
tients with recurrent signs and symptoms ofmajor arterial insufficiency to the head in thelight of the electroencephalogram, electrocar-diogram, and clinical manifestations as the
S.F.AHORIZONTAL BEFORE TILT
A2 BP 120/80
9G 50LVA d- 4-..t - ISEC.
7B? FOR 3 MIN. C HORIZONTAL MIN AFTER TILT
BP 90/60 - 04/70 2 BP 118/803
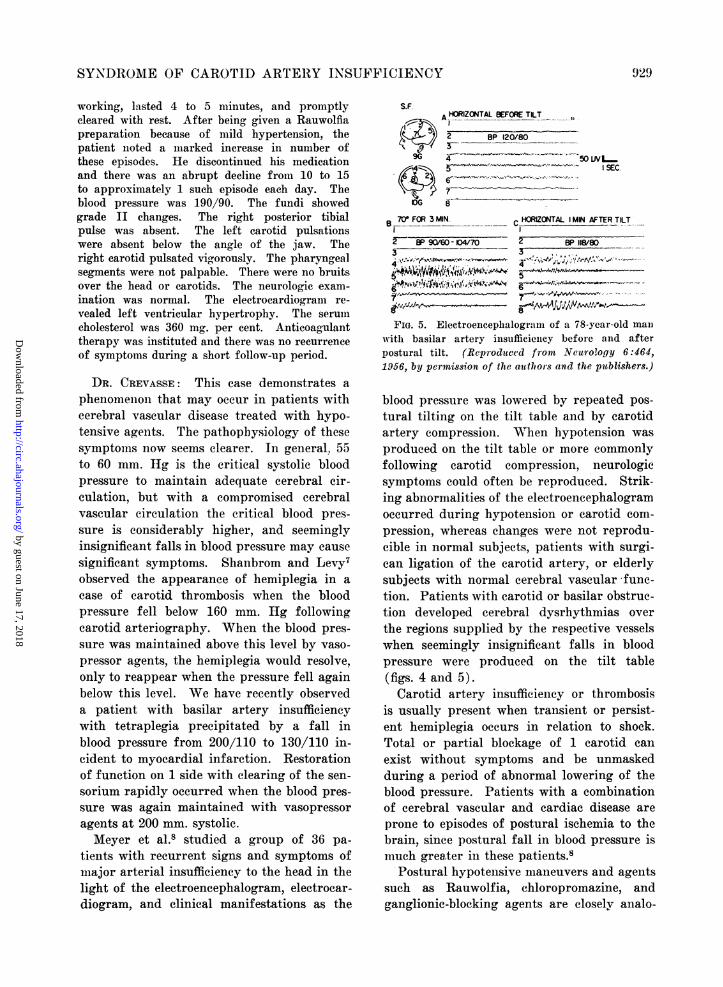
FIG. 5. Electroencephalogrami of a 78-year-old manwith basilar artery insufficiencey before and afterpostural tilt. (Reproduced from Neurology 6:464,1956, by permission of the authors and the publishers.)
blood pressure was lowered by repeated pos-tural tilting on the tilt table and by carotidartery compression. When hypotension wasproduced on the tilt table or more commonlyfollowing carotid compression, neurologicsymptoms could often be reproduced. Strik-ing abnormalities of the electroencephalogramoccurred during hypotension or carotid com-pression, whereas changes were not reprodu-cible in normal subjects, patients with surgi-can ligation of the carotid artery, or elderlysubjects with normal cerebral vascular func-tion. Patients with carotid or basilar obstruc-tion developed cerebral dysrhythmias overthe regions supplied by the respective vesselswhen seemingly insignificant falls in bloodpressure were produced on the tilt table(figs. 4 and 5).Carotid artery insufficiency or thrombosis
is usually present when transient or persist-ent hemiplegia occurs in relation to shock.Total or partial blockage of 1 carotid canexist without symptoms and be unmaskedduring a period of abnormal lowering of theblood pressure. Patients with a combinationof cerebral vascular and cardiac disease areprone to episodes of postural ischemia to thebrain, since postural fall in blood pressure ismuch greater in these patients.8
Postural hypotensive maneuvers and agentssuch as Rauwolfia, chloropromazine, andganglionic-blocking agents are closely analo-
92
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from

(CREVASSE, LOGUE, HURST
gous to the tilt-table observationsx and shouldbe avoided in all lpatieiits with cerebral vas-cular itisuffi(ieiiev. Furthermore, one shouldcorrect Plrolptly in these patients hbypoteni-sion incideint to cardiac arrhythmi1ia, myocar-dial infarction, I)lood loss, acute left ventricui-lar failure, aniestlhesia, or other less common
etiologies.A PHYSICIAN: Whlat iS the rIo Of Cerl),ral
allniospasmll ill the production of symptomsDR. CREVASSE From clinical observatiolns
i11 man anid laboratory evidence in1 animalswhere the cerebral vessels cail I)( viewedthrough a skull Win(ow, alterations ill bloodflow related to changes in systemic arterialpressure rather tlhani cerebral angiospasmseein to be the major factor. It is difficult,however, to explain the transieint neurologic(leficits accoinpainyilig migraill eada(.1h1(esand, of course, art(eriosl)aslni has been ob-
served l)y ileuorgeons op)elatinrg on thecircle of Willis.A PHYSItcAN Canl carotid artery tlhromn-
bosis be established without resortintg to ar te-riography ?
DR. CREVASSE: Carotid artery insufficien-cy andcl thronhllosiiis is rapidly be(com(linlg a (liin-ical diagnosis. Ophthalmodyniainiomietrvr is avaluable adljunet in the diagnosis and cons'istsof insertion of a (rage with a s)ring-loadedplunger between the lid aiidl selerac for themeasurement of intra-ocular pressure. Theretinal arteries are observed wvith the oph-thalmoscope as l)iresslre is gently increased.When the retinal arteries begin to pulsatethis represents the diastolic pressure and canbe iiiter)reted from the gage. The intra-ocular pressure is further increased until pul-sationis cease, and this reflects systolic pres-sure. This is repeated in the opposite eye.There is a striking pressure differential be-tween the involved and the opposite eve, areflection of carotid arterial ol)struction. Theaverage retinal artery pressure has beenfound to be 30 to 45 mnm. Jig diastolic and65 to 75 mmn. systolic, that is, approximatelyhalf the systemic bloo)( pressure.' It seemsthat a reduction of 2.5 to 30 per (edit in bothsystolic and diastolic l)'ess5u es is diagnosticof iml)aired carotid circulation,1 0
Cause 4.J.A., n 47-year-old white man, (levelope(l epi-
sodes of sudden blindness in the right eye, (bhar-aicterized by a fog' rolling in froma the temporalside until vision was coimpletely oh(scured. Tlweblindness lasted 4 to 5) iminutes aii(l vision returnedgraduallly froim the l to the temtpoirall side.I)nuring the past year lhe has ha(l rel)eated pisodeso)f weakness a(l nulmbnless of the left a11rmo anldleg-, not a ycoimi pained by visual syimp)tomns. i'Therlehave been persistent anii(l severe tal headachesfor the l)ast 8 months. Menital ac(uity has progeres-sivelv diminished.
The bloo(d}p}essure was 16()/ 90(. Therle wasslight alphaia with iiioderate weakness of the leftairsa and leg. There was a systolic blruit over thmeleft eve ball. Thme fuiidi werec miorlijal. The rig~htp)haryingeal pulse was absent. The reflexes werehyperactive on the left. The righit (crotid l)n1lsa-tioii ended abruptly ait the bulb, and the leftlulsated vigorously. A guide 11 systolic murmmurwas present over the left caroti(l bulb.A rig~ht carotid arteriograim deimonstrated(l occl
sion below the right (caotid lulb. A thromboemn-(l.i.terecotoiiiv( was pert 'oried by D)r. GalrlandPerdue but (lesIpite reimoval of the thromumbius andilpassage of a1 catheter into the carotid siphon nohack flow fr.omm the distal carotid oc(urre~d. Theimmiiediate postoperative (ourlse was characterizedby recurrent episodes of inioiio(oula r blindness atwhich time his blood l)iessuIe wats 10 to 20 mom.JIg lower than when he was asyptomnatic.
DR. CREVAISSE Mo0n11ular blindnes andcottralateral nieuirologi( deficits are the hall-mark of carotid artery thrombosis'. As inthis case, tllhe uslually (1o iiot occur simul-tanieously-. Trliis )atienmt has severe headache,w-hich is plreseit iii about half of all relortedcases. The combination of headache, clhangresiii mental aculity, iieurologi( deficits, andseizures frequently occurs in carotid arterythrombosis alid is invrariablys confused withbrain tumor.The systolic bruits over the eyeball and
(arotid bulbl) opposite the ocecluded carotidare valuable signs in (liagnosis and probablyrepresent a compensatory increase in bloodflow through the o0))osite larti ally involved(arotid artery.A PHYSI(IAN: What is tle sitgnfificance and
mechanism of monocular blindiniess?DR. CREVASSE: Monocular blindness is
usuallyl transient lasting fromt 2 to 3 iuimitesand is subjectively described as a fog rolling
930(
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYNI)RO)M1l E OF CAR( )T II) ARTERY INSITFFIC IENCY
ill, a veil (comillg over the eye, or a curtaingradually obscuring vision. This type ofblindness is typical of retinal ischemia. Sincethe central retinal artery is all end artery(fig. 1) with no collateral circulation, alter-ationis ini 1)lood flow through this vessel onl theside of a I)artially or completely occludedcarotid is markedly affected by spontaneousfalls il blood pressure or cardiac output. Wehlave made observations; on1 the preceding pa-tient, and illdee(I when monocular blindnessoccurre(1 his svstolic blood pressure was 10to 20 nun. hIg loNel thani when he was asymp-tomatic. With falls ill blood pressure, thefundus became pale, with a decrease ill cali-ber of the branllches of the central retinalarterv, an(l retinal isebemia aind blindnessfollowed. When the factors that have re-duced blood flow were (colupensated or (cor-reeted, visioni returned.
Para(loxi(ally, ill somlle cases whell l)'ellioll-itorv visual disturlances have been lreselltanl(1 (caroti(d thrombosis finally occurs, withcontralateral hemiplegia, the vision may re-main unimpaired, as adequate time haselapsed for collateral circulation to maintainblood flow to the retinae.A PHYSICIAN: What about the results of
surgery and anticoagulant therapy?DR. CREVASSE: As ill this case ill gen(eral,
the surgical results have been disappoinitincg.When symptoms are present with carotidthrombosis, the collateral circulation througfhthe 1)asilar and opposite carotid is impaired.This concept is substantiated by the highincidence of asyml)tomnat ic carotid thrombosisand the tilt-table experimentllts oln otherwisenormal persons with carotid artery ligationswithout syllptoms.Rob and Wheeler"' have reported the
largest successful series of operated cases.They have en1ployed direct arterial surgerywith and without hypothermia to restore bloodflow through a partially or completely ob-structed carotid ill a total of 27 patiemlts.Eleveni of this series had l)artial occlusionwith tr at sient nenirologic symptoms. 'rhexwere alble to re-establish ood blood flow inall of tlhese. Four. latinllts l)ecamc asv iii)to-.mati(, 2 improved, antld 4 showed no chancre.
There was one death. Of the 16 patientswith complete occlusion, good blood flowcould be re-established in only 4 patients.After complete occlusion, as in the precedingcase, blood flow couldl be re-established onlyduring a short interval before the clot e-
tende(1 higher into the cranial cavity. In thegroup of complete occlusion only 1 patient'lecamne asymln)tomatic and the remaining), 13showed 11O change. There were 2 deaths. Itseems that the patients most likely to blenefitfrom surgery are those with incom plete occlu-sioiis who consult their physician because oftransiemit symptomss of cerebrovascular inisuffi-(ielncy. This is the group in whom the neuro-logic examination will most likely be negativeand the only physical finiding may be a systolicor (continuous murmur over the partially ob-structe(d carotid, usually contralateral toneu'rologic syptoms. Restoration of flow insthese I)atiellts will l)e rewarding not only infrequetntl- relieving symptoms of cerebralvascular inisufficieiie y but may in turni preventthe later development of complete thrombosisand irreversible iieurologic deficits.Though long-termn follow-up and double-
blind studies are umot (complete, promisingresults are seeni with anticoagulants,12 whichappear to be the medical treatment of choiceat the moment. In our experience, symp-tomns of cerebral vascular inisufficiency diim-ish, and the neurologic status appears tostabilize after aniticoagyulatioin.
The rational and beneficial effects are notentirely clear. Anticoagulation may furtherdelay occlusion of a partially obstructed(arotid or prevent extension of the thrombusinto the cranial cavity. Autopsy material'has revealed forumation of thrombi in thecarotid bull) and eml)olization of the ipsilat-eral cerebral blernlispheres. AnticoagulationWollld appear motre specific in this situation.A PInSImCIAN: What is the I)rogllosis of
this syn1idrome ?DR. CREVASSE: Againi, lonr-term follow-up
studies in large series of )atiemits are imnade-quate, auid the relative p)rognlosis is unknown.Ilowever, in a revie(vof 107 cases of ('omnl leteo('clnsion of the (.'roti(d artery,, Johlnsoln anllWalker" rep)orted 1 . per cent niortality with-
931
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from
CREVASSE, LOGUE, HURST
in several months, 15 per cent revealed noessential change, and 25 per cent showedimprovement over varying periods of time.There was no follow-up study of the remain-ing patients. The follow-up of patientstreated by anticoagulants and surgical recon-struction is again limited and inadequate. Itappears, however, that their prognosis willbe, somewhat improved by these methods.
Case 5E.S., a 56-year-old white woman, gave a history
of benign hypertension for several years. Fourweeks ago the patient developed typical anginapeetoris precipitated by exertion and relievedpromptly by nitroglycerin. There was no historyof neurologic symptoms or visual disturbancesalthough there had been slight impairment ofmemory in the past few months.Her father died at age 45 of high blood pres-
sure and cerebral vascular accident. Her motherdied at age 59 of coronary artery disease.The blood pressure was 160/90. The carotids
pulsated vigorously to the angle of the jaw. Overthe right carotid bulb a loud continuous murmurwas present. This murmur was hemodynamicallyidentical with the continuous murmur in case 1and figure 3. There was no bruit over the heador the left carotid artery. Pharyngeal palpationof the internal carotids revealed diminished pulsa-tions bilaterally, with no obvious asymmetry. Theheart revealed a grade II aortic and mitral systolicmurmur. The neurologic examination was com-pletely negative.
DR. CREVASSE: Approximately 3 per centof Fisher 's unselected autopsy series hadsevere stenosis of the carotids and 11 of Rob's27 operated cases had partial occlusion withneurologic symptoms. The pathophysiologiccounterpart of these findings may be a sys-tolic or continuous murmur over the carotidbulb, the most common site of involvement.We have recently correlated the frequency
and significance of localized carotid murmursin 100 consecutive general hospital patients.Well localized systolic murmurs were heardover the carotid in 7 and continuous murmurswere present in 2. These murmurs occurredboth in asymptomatic patients and patientswith overt carotid artery insufficiency as incases 1, 2, 4, and 5. In a 4-month period wehave observed a well-localized continuousmurmur over the carotid bulb in 8 patients.
Five of these patients had neurologic symp-toms or deficits, usually on the side oppositethe carotid murmur.The final clinical spectrum of carotid ar-
tery insufficiency and thrombosis has yet tobe defined. The initial evidence of carotidobstruction may be localized murmurs overthe carotid bulb and these may be noted priorto the development of symptoms. The pa-tients may complain of "swishing sounds"or roaring in the head. When completethrombosis ensues, the head noises and bruitscease and neurologic symptoms may appear,depending on alterations in blood flow andadequacy of collateral circulation.A PHYSICIAN: What are the mechanisms
responsible for the bruits heard in thesepatients ?
DR. HURST: One can divide the bruitsheard in these patients into those heard inthe head and those in the neck. The examinershould establish the habit of listening overthe cranium and especially over the eyeballs,in patients suspected of carotid insufficiency.It is a good plan to have the patient closehis eyelids and place the bell of the stethos-cope over 1 eye and have the patient "open"his eyes. This allows one to listen througha relaxed eyelid, thereby eliminating thesounds of muscle tremor.The high-pitched bruit heard over the eye-
ball on the side opposite the carotid throm-bosis (fig. 1) can be due to 1 of 2 mechanisms:1. The retrobulbar arterial collateral circu-lation may be so abundant that a bruit isproduced. 2. It is likely that a bruit pro-duced by a partially occluded. artery withinthe skull will be heard better over the nearesteyeball. In this case, the bony orbit acts asa megaphone. Intercranial arteriovenousfistulae and severe anemia can produce suchmurmurs but are not as common as vascularocclusive disease of the head and neck.
It is convenient to divide the murmurs inthe neck into systolic and continuous mur-murs.Everyone is aware of the systolic arterial
bruit heard in the neck vessels in patientswith anemia, fever, thyrotoxicosis, and theother causes of high cardiac output. In the
932
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYNDROME OF CAROTID ARTERY INSUFFICIENCY
absence of these conditions a systolic bruitin the carotid artery should force one to con-sider the murmur of aortic stenosis, which isfrequently transmitted into the neck orcarotid arterial obstruction. Aortic stenosisis usually heard best maximally over the pri-mary aortic area, may be heard at the apex,and is transmitted up both earotids, diminish-ing in intensity as one approaches the angleof the jaw. When atheroselerosis of the ca-rotids occurs without significant obstruction,the systolic bruit is seldom loud and occurswith equal intensity through both carotids.When one encounters a loud and localizedsystolic murmur in a carotid artery, thisshould be considered as an important diag-nostic clue of partial occlusion of this vessel.The systolic bruit is heard over the site ofthe arterial narrowing and can, therefore,disappear if the occlusion becomes complete.Occasionally, in complete occlusion of onecarotid artery, collateral blood flow is in-creased through the opposite carotid and ifit is partially occluded, a systolic or contin-uous murmur may be detected over the oppo-site carotid. Occasionally a faint systolicmurmur is present over the site of carotidocclusion. It can be obliterated by manualcompression of the branches of the externalcarotid and is related to an increase in collat-eral flow through this vessel (fig. 1).
There are several causes of a continuousmurmur in the neck. The most common causeis the normal venous hum that is usuallyheard in children and rarely heard in adults.This type of murmur can be eliminated oraltered significantly by light pressure on thejugular veins and is seldom a diagnosticproblem.
Graves' disease or an arteriovenous fistulabetween the carotid artery and jugular veinmay cause a continuous murmur. One isusually able to identify systolic pulsations ofthe neighboring vein, and an increase in skintemperature and venous return in the latter.A continuous murmur may be heard over
an area of partial carotid occlusion when thecollateral vessels are inadequate. Edholmet al.13 have shown that localized or segmen-tal obstruction in arteries has no effect on
diastolic pressure distal to an obstruction pro-ducing only a systolic pressure gradient.Flow to the segment distal to the obstructionis provided by adequate collateral circulationand equal diastolic pressures are maintainedboth proximal and distal to the obstruction.The turbulence of flow in systole producedby the narrowed carotid and systolic pressuregradient accounts for the systolic bruit heard.Myers and co-workers'4 have made observa-tions on continuous murmurs over partiallyoccluded vessels, with particular reference tothe aortic arch syndrome. The production ofa similar hemodynamic situation in animalsclearly substantiated their hypothesis thatthe continuous murmur was due simply topartial occlusion of a major artery under cir-cumstances where collateral circulation wassimultaneously diseased or inadequate tomaintain diastolic pressure distal to the in-volved area. In this situation, a considerablepressure gradient exists both in systole anddiastole, producing a continuous murmur overa partially occluded vessel. In carotid arteryinsufficiency when collateral circulationthrough the opposite carotid and the basilarsystem is inadequate, a continuous murmur isproduced usually over the carotid bulb, themost common site of involvement (fig. 3).This is often confused with an arteriovenousfistula in the neck.
In summary, there are several points worthremembering. 1. Carotid artery thrombosisand stenosis is a common disease occurring in9.5 per cent of one unselected autopsy seriesbut is infrequently recognized clinically.2. Physicians interested in cardiovasculardisease are being confronted with this syn-drome because of its relationship to changesin blood pressure and cardiac output. 3. Thecarotid arteries are neglected by the patholo-gist and are a no man 's land between theinternist and neurologist. Careful examina-tion and auscultation of the head and neckare rewarding in "routine strokes" and mayclarify bizarre neurologic symptoms in pa-tients with cardiovascular disease. 4. A con-tinuous machinery murmur may be presentover a partially occluded carotid and is avaluable adjunct in the early recognition of
933
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from

4CREVASSE, LOG(1 TE? HURST1
carotid artery insufficiency. 5. Carotid arteryinsufficiency is a treatable disease. Its earlyrecognition and appropriate therapy beforecomipl ete thrombosis occurs will directly inI-fluence the therapeutic results.
REFER XNCES
1. FisERn, M.: Occlusion of the carotid arteries.IArchi. Neurol. & Plsvchiat. 72: 187, 1954.
2. BALDREY, E., MAASS, L., AND MILLER, E.: Therole of atlantoid compression in etiology ofinternal carotid thrombosis. J. Neurosurg.13: 127, 1956.
3. JOIINSON, H. C., AND WALKER, A. E.: Thea1ng1iographic (liagn()sis of spontaneousthrombosis of the internal and common ca-r(otid arteries. J. N\eurosurg. 8: 631, 1951.
4. I)DUNNINc, H. S.: l)etection of occlusion ofthe internal carotid artery by pharyngealpalpation. J.A.MA. 152: 321, 1953.
5. COHEN, J., AND MILLER, S.: Eyeball bruits.NTew Ehngland J. AMed. 255: 459, 1956.
6. FISH ER, C. AI.: Cranial bruit associated withocclusion of the internal carotid artery.Neurology 7: 299, 1957.
7. SHANBROM` E.. AND LEVY, L.: The role ofsystemimic blood pressure in cerebral circu-
lation in carotid and basilar artery throma-boses. Am, . J. Med. 23: 197, 1957.
8. AMEYER, J. S., LEIDERMAN, H., ANI) DENNY-BROWN, D.: Electroencephalographic studyof insufficiencv of the batsilalr and caroti(larteries in mIlan. Neurology 6: 455, 1956.
9. KocH, F. L. P.: Ophthalmmmodynamnalommmetry.Arch. Ophthahlol. 34: 234, 194.5.
10. HEYMAN, A., KARP, H., AND Bioo..), B.: De-terMinations of retinal artery pressure india-nosis of carotid artery occlusion. Neu-rology 7: 97, 1957.
11. RoB, C., AND WHEELER, E. B.: Throambosis ofinternal carotid artery treated by arterialsurgery. Brit. MW. J. 2: 264, 19,57.
1 2. MILLIKAN, C. H., SIEKERT, R. G., AND SHICK,R. M.: Studies in cerebral vascular diseaseV. The use of anticoagulants in the treat-ment of intermittent insufficiency of theinternal carotid arterial system. Proc. StaffMeet., Mayo Clin. 30: 578, 1955.
13. EDHOLM, 0. G., HOWARTH, S., AND SHARPEY-SCHAFER, E. P.: Resting blood flow andblood pressure in limbs with arterial ob-struction. Clin. Sc. 10: 361, 19151.
14. M1YERS, J. D., MURDAUGH, H. V., MCINTOSH,H. D, AND BLAISDELL, R. K.: Observationson continuous murmurs over partially ob-structed arteries. Arch. Int. AMed. 97: 726,1956.
Rob, C., and Wheeler, E. B.: Thrombosis of Internal Carotid Artery Treated byArterial Surgery. Brit. M. J. 2: 264 (Aug. 3), 1957.1n 27 patients with synmptomnatic ocelusiouis of the internal carotid artery dilrcet
arterial surgery was performed in an attempt to restore adequate blood flow. iA goodblood flow was obtained in all 11 patients with partial oeclusion, and in only 4 of the16 with complete occlusions. In complete ocelusions blood flow could only be reestab-lished during the short period before the clot extended into the cranial cavity, but eventhen irreversible cortical damnage might have occurred. The risk of surgery is not toorleat in these patients since only 2 of th- 27 patients so treated had any postopera.tive
exacerbation of their neurologic symptoms. The authors believe that the patients mmostlikely to benifit from such surgery are those with incomplete ocelusions who lh.avtesymml)ptonis of evrebrovaseular insufficiency. In these patients restoration of adequateblood flow not only frequently relieves the symptoums but also mmav prevent the laterdeveloplment of comnplete throabosis a iid irreversible bra indaimimae.
SAG.ALLT
!) 1,34
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from
LAMAR E. CREVASSE, R. BRUCE LOGUE and J. WILLIS HURSTTherapy
Syndrome of Carotid Artery Insufficiency: Early Clinical Recognition and
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1958 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.18.5.924
1958;18:924-934Circulation.
http://circ.ahajournals.org/content/18/5/924.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Rights Question and Answer
Permissions andpage under Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the WebCenter, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the Copyright ClearanceCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 17, 2018http://circ.ahajournals.org/
Dow
nloaded from


















