Clinical Cases Meeting
24
Society for Endocrinology Clinical Cases Meeting In association with the RSM Section of Endocrinology and Diabetes Tuesday 26 February 2008 The Royal Society of Medicine, 1 Wimpole Street, London W1G 0AE Programme and Abstracts Supported by Society for Endocrinology Corporate Members: Almirall, Ardana Bioscience Ltd, AstraZeneca plc, Bayer Schering Pharma, BioScientifica Ltd, Eli Lilly and Co Ltd, Ferring Pharmaceuticals Ltd, Genzyme Therapeutics, Ipsen Ltd, Merck Serono, Novartis Pharmaceuticals UK Ltd, Novo Nordisk Ltd, Nycomed UK Ltd, Organon Laboratories Ltd, Pfizer Ltd, ProStrakan and Sandoz Ltd Also supported by Clinical Endocrinology Exhibitors: Bayer Schering Pharma Merck Serono Novartis Pharmaceuticals UK Ltd Novo Nordisk Ltd Sandoz Ltd CPD approved TEXT PAGES 1UP.indd 1 4/1/08 08:58:19
-
Upload
roger961 -
Category
Health & Medicine
-
view
1.087 -
download
2
Transcript of Clinical Cases Meeting

Society for Endocrinology
Clinical Cases Meeting In association with the RSM Section of Endocrinology and Diabetes
Tuesday 26 February 2008 The Royal Society of Medicine, 1 Wimpole Street, London W1G 0AE
ProgrammeandAbstracts
Supported by Society for Endocrinology Corporate Members:
Almirall, Ardana Bioscience Ltd, AstraZeneca plc, Bayer Schering Pharma, BioScientifica Ltd, Eli Lilly and Co Ltd, Ferring Pharmaceuticals Ltd, Genzyme Therapeutics, Ipsen Ltd, Merck Serono, Novartis Pharmaceuticals UK Ltd, Novo Nordisk Ltd, Nycomed UK Ltd, Organon Laboratories Ltd, Pfizer Ltd, ProStrakan and Sandoz Ltd
Also supported by Clinical Endocrinology
Exhibitors: Bayer Schering Pharma Merck Serono Novartis Pharmaceuticals UK Ltd Novo Nordisk Ltd Sandoz Ltd
CPD approved
TEXT PAGES 1UP.indd 1 4/1/08 08:58:19

Forthcoming Society events:
2008
Society for Endocrinology BES 2008 7 – 10 April 2008 HIC, Harrogate, UK
Endocrine Nurses Training Course 8 – 10 September 2008 University of Exeter, UK
Clinical Update 2008 October 2008 TBC
Any comments on Clinical Cases Meetings would be welcome by Dr Steven Ball (Programme Advisor to the SFE Clinical Committee), School of Clinical Medical Sciences, The Medical School, 4th Floor William Leech Building, Newcastle upon Tyne, NE2 4HH. Tel: 0191 232 5131, Fax: 0191 222 0723, Email: [email protected]
This meeting is accredited for 4 CPD credits
TEXT PAGES 1UP.indd 2 4/1/08 08:58:19

Society for EndocrinologyClinical Cases Meeting In association with the RSM Section of Endocrinology and Diabetes
RegistrationPlease register before the start of the meeting online at: http://www.endocrinology.org/meetings/2008/cc2008/registration/
Case discussions Lecture Theatre Chairman: Dr Steven Ball (Newcastle upon Tyne)
13.30-14.00 Coffee and registration
14.00-14.30 POSTER VIEWING (Atrium)
14.30-14.45 A step towards unravelling the genetics of polycystic ovarian syndrome S Chakrabarti1, V Crowley1, C Johnston1, S O’Rahilly2
Department of Diabetes and Endocrinology, Hemel Hempstead Hospital1, University of Cambridge, Cambridge2
14.45-15.00 Hyperinsulinaemic Hypoglycaemia Post gastric bypass due to massive elevation of GLP1: Response to somatostatin analogue KS Myint, S Farooqi, N Finer Department of Endocrinology, Addenbrooke’s Hospital, Cambridge
15.00-15.15 A Case of Carney’s Triad VJ Moyes1, K Thomson1, RH Reznek3, DM Berney4, F Hughes2, JP Monson1, SA Akker1
1Department of Endocrinology and 3Dept of Radiology, St. Bartholomew’s Hospital, West Smithfield, London, 2Dept of Surgery and 4Dept of Histopathology, Royal London Hospital, London
15.15-15.30 Multiple endocrine manifestations of the MTTL1 A3243G mutation B Khoo12, F Medici1
1Dept of Metabolic Medicine, Homerton University Hospital, Homerton Row, London, 2Dept of Endocrinology, Royal Free Hospital, London
15.30-15.45 A case of Neurofibromatosis type 1 with Phaeochromocytoma and Gastrointestinal Stromal Tumour (GIST) H Kahal, E. Cooper, D Coppini Poole Hospital NHS Foundation Trust, Poole
15.45-16.00 An unusual cause of panhypopituitarism LF Clark1, D Culligan2, D Currie3, JS Bevan4
Department of Endocrinology, Raigmore Hospital, Inverness1
Departments of Haematology2, Neurosurgery3 and Endocrinology4,Aberdeen Royal Infirmary, Aberdeen
TEXT PAGES 1UP.indd 3 4/1/08 08:58:19

16.00-16.30 POSTER VIEWING and afternoon tea (Atrium)
16.30-16.45 Apparent Familial Isolated Hyperparathyroidism due to MEN-1 11q13 Mis-sense Mutation Successfully Treated with Cinacalcet KL Bavidge1, TJ Archer1, GC Wishart2 and C Parkinson1
The Ipswich Hospital, Heath Road, Ipswich1, Addenbrooke’s Hospital, Hills Road, Cambridge2
16.45-17.00 Severe postmenopausal hyperandrogenism due to insulin resistance state: A case report Ebaa Al-Ozairi 1, Andrew Advani 1, Kim Johnson 1, Enid Michael 2,Richard Quinton 1Departments of Endocrinology1 and Womens’ Health2, Royal Victoria Infirmary & University of Newcastle-upon-Tyne, Newcastle
17.00-17.15 Does IGF-1 deficiency have a role in the development of syringomyelia?
A Smyth, SC Wong, SF Ahmed Bone and Endocrinology Research Group, Royal Hospital for Sick Children, Yorkhill, Glasgow
17.15-17.30 Management of phaeochromocytoma in the presence of critical coronary artery disease IS Mackenzie1, N Cartwright4, C Mitchell2, M Gurnell2, MJ Brown1,VK Chatterjee2, NV Jamieson3 K Valchanov5, SAM Nashef4, HLSimpson2
Clinical Pharmacology Unit1, Institute of Metabolic Science2,Department of Surgery3, Addenbrooke’s Hospital and University of Cambridge, Department of Cardiothoracic Surgery4, and Anaesthetics5, Papworth Hospital, Cambridge
17.30 Wine Reception (Atrium) There will be a short reception following the meeting at which two oral communication prizes of £250 and £150 and two poster presentation prizes of £100 each will be awarded for the best presentations by authors below the grade of consultant.
TEXT PAGES 1UP.indd 4 4/1/08 08:58:20

A step towards unravelling the genetics of polycystic ovarian syndrome
S Chakrabarti1, V Crowley1, C Johnston1, S O’Rahilly2
Department of Diabetes and Endocrinology, Hemel Hempstead Hospital1, University of Cambridge, Cambridge2
A 19-year-old lady presented to endocrine outpatients in 1990 with a one year history of hirsutism, oligomenorrhea and ultrasound evidence of polycystic ovaries. She had a raised random glucose of 10.2. Her BMI at this time was 27 and a diagnosis of impaired glucose tolerance linked to polycystic ovarian syndrome was made. She was advised on diet and exercise and asked to lose weight. Over the course of the following two years, she managed to lose 5kg. Her hirsutism and oligomenorrhea continued and she was therefore started on hormonal treatment in the form of Dianette with initial good results. However due to adverse effects on her lipid profile and blood glucose readings this was subsequently stopped. Spironolactone was substituted but this too had to be stopped due to postural hypotension. Over the course of the next few years, it became apparent that our patient had a progressive metabolic syndrome with increasingly abnormal lipid profile (total cholesterol 6mMol/L triglycerides 5mMol/L in 1997) and deterioration into frank diabetes (fasting plasma glucose 9.7mMol/L and HbA1C 7.9% by 1997). She was treated with metformin and this initially controlled her HbA1C and a fibrate to control her raised triglycerides. Both her blood sugar and lipid profile continued to deteriorate such that by 2003 her HbA1C was 8.4% on 1.5g metformin (maximum tolerated) and her cholesterol was now 7.1mMol/L with triglycerides of 4.97mMol/L on 200mg bezafibrate.
Due to her young age of onset and progressive symptoms she was referred for gene analysis, which revealed the presence of PPAR (peroxisome proliferator-activated receptor) gamma co-activator 1 (PGC-1) heterozygosity. PGC-1 is a co-activator of a number of nuclear hormone receptors including the PPARs and was demonstrated to coordinately activate a programme of adaptive thermogenesis in adipocytes and muscle. Subsequent work also showed it is involved in the regulation of Glut 4 expression and insulin stimulated glucose uptake in skeletal muscle and in the coordinate regulation of hepatic gluconeogenesis. There are associations with the development of type 2 diabetes, dyslipidemia, hypertension, polycystic ovaries and possibly an increased risk of breast cancer and decreased aerobic exercise capacity with abnormalities of the gene.
The optimum treatment for patients with this condition is as yet unknown and we expect prognosis is linked to cardiovascular risk. Our patient has been encouraged to maintain lifestyle measures such as adherence to a low-fat diabetic diet and regular exercise schedule as these are thought to be beneficial. A thiazolidinedione and statin were added to her metformin and fibrate in 2003 but a similar pattern has repeated itself with initial benefit and subsequent deterioration and the direction further treatment should take is still somewhat uncertain. Our case demonstrates that progressive metabolic syndromes can be due to novel gene mutations, which may lead to new targets for treatment in future.
TEXT PAGES 1UP.indd 5 4/1/08 08:58:20

Hyperinsulinaemic hypoglycaemia post gastric bypass due to massive elevation of GLP1: Response to somatostatin analogue
KS Myint, S Farooqi, N Finer Department of Endocrinology, Addenbrooke’s Hospital, Cambridge
Introduction: Bariatric surgery is an effective treatment for severe obesity, ‘curing’ type 2 diabetes, and reducing cardiovascular events and mortality. Recent case reports have described hypoglycaemia developing after gastric bypass surgery (GBS); various mechanisms have been suggested as the cause of such spontaneous persistent hyperinsulinaemic hypoglycaemia (PHH). History : A 43 year old lady with the history of severe obesity since a teenager developed type 2 diabetes at age 36 and treated with metformin. In 2000 (age 37), weighing 165 kg, BMI 71kg/m2, she underwent gastric bypass surgery (GBS). Following surgery anti-diabetic medication was withdrawn and she remained ‘diet controlled’ thereafter. Steady weight loss over the first 2 years was followed by maintenance of a 53% weight loss at BMI 32.3kg/m2.In 2006 she reported symptoms suggestive of hypoglycaemia occurring while fasting and after meals. Hypoglycaemia was supported by a HbA1c of 4.9%.
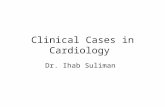
Investigations and results: After 66 hrs fasting, she developed symptomatic hypoglycaemia with plasma glucose of 1.8mmol/l and inappropriate levels of insulin (15pmol/l), proinsulin (2.9pmol/l), and C peptide (185pmol/l). The 32-33 split proinsulin level was undetectable (<2pmol/l). These results suggest spontaneous hyperinsulinaemic hypoglycaemia. An MRI pancreas showed no lesion in the pancreas. In order to investigate the cause of her hypoglycaemia and the possible role of the incretin GLP1, plasma GLP1, insulin and glucose were measured for 5 hours after three interventions on different days: a. 75g oral glucose (OGTT), b. Standard Meal, c. OGTT 30min after subcutaneous injection of the somatostatin analogue octreotide 100µg. While fasting, GLP1 was elevated compared to obese matched control. (22 Vs 10pmol/l). Following OGTT, a markedly exaggerated rise in GLP1 was seen, peaking at 30min and returning to basal levels after 240min. Plasma glucose levels showed a rapid peak at 30min (7mmol/l) and returned to baseline by 90min. Insulin levels peaked at 15min (643pmol/l). The GLP1 response to a standard meal was similar but greater. Octreotide injection prior to OGTT attenuated both GLP1 and Insulin responses and not only reversed the low levels of glucose but elevated them into a diabetic range (2 hr glucose 11.2mmol/l). (Fig) Management and conclusion: Treatment with octreotide (escalating to 200mcg bd), combined with low glycaemic index diet and corn starch improved symptoms and HbA1c We demonstrate that following GBS altered GLP1 levels both basally and in response to meal or glucose challenges can result in both fasting and post prandial hypoglycaemia. Suppression with octretide has proved to be an initially successful therapeutic approach that could avoid pancreatectomy (the treatment employed in previous cases of post GBP hypoglycaemia).
0
5
10
15
(a)G
luco
se (
mm
ol/l)
1
10
100
1000
(b) I
nsul
in (p
mol
/l)
0 60 120 180 240 3001
10
100
1000
Control (OGTT), n=8 JM(OGTT) JM(Octreotide + OGTT)
Time (minutes)
(c)G
LP (p
mol
/l)
Fig . (a) Glucose, (b) Insulin and (c) GLP1 response to OGTT (75g glucose load) without or withprior Octreotide 100µg s/c injection. The error bars for control group indicate mean±SD.
TEXT PAGES 1UP.indd 6 4/1/08 08:58:20

A case of Carney’s triad
VJ Moyes1, K Thomson1, RH Reznek3, DM Berney4, F Hughes2, JP Monson1, SA Akker1
1Department of Endocrinology and 3Dept of Radiology, St. Bartholomew’s Hospital, West Smithfield, London, 2Dept of Surgery and 4Dept of Histopathology, Royal London Hospital, London
A 34yr old Nigerian lady was investigated for hypertension at the age of 26. A right sided phaeochromocytoma was identified during renal angiogram and a right adrenalectomy was performed with post-operative normotension. Persistent iron deficiency anaemia requiring blood transfusions, was noted pre- and post-operatively. Investigation for primary infertility in Nigeria was delayed following the detection of recurrent hypertension with raised urinary metanephrines. Simultaneously, the patient had an episode of haematemesis and her care was transferred to the UK for further investigation and management.
Gastroscopy identified multiple tumours within the stomach wall, the largest measuring 5cm. Biopsy revealed a sub-mucosal spindle tumour with expression of CD117 and CD34, consistent with a gastro-intestinal stromal tumour (GIST). CT scan confirmed a large lobulated mass within the stomach, and other abnormalities were noted; a large enhancing mediastinal mass consistent with a paraganglioma, enlargement of the left adrenal gland suggestive of a phaeochromocytoma and an 8mm left apical lung nodule. Additionally there was an unexplained, unusual appearance of the kidneys with an irregular cortical outline. MIBG scan revealed uptake within the mediastinal mass and on the left side of the abdomen, presumed to be in the left adrenal bed. A total gastrectomy and left adrenalectomy were performed under phenoxybenzamine, propranolol and hydrocortisone cover, with good post-operative recovery. Histology of the stomach confirmed multiple GISTs within the stomach, with an additional GIST in the jejunum and involvement of 7 out of 13 lymph nodes. Histology of the left adrenal gland revealed adrenocortical hyperplasia with no evidence of phaeochromocytoma.
Post-operative MIBG scan confirmed the presence of multiple paragangliomata; in the mediastinum, at the liver hilum and in the right para-aortic region. Bilateral, small carotid body tumours have been detected on ultrasound; these are non-MIBG avid. Restaging CT scan demonstrated these multiple paragangliomata, no recurrence of GIST and no enlargement of the left apical nodule, compatible with a pulmonary chondroma. Current management includes MIBG therapy, long term alpha and beta blockade and regular reassessment.
The presence of GIST, functioning extra-adrenal paraganglioma and pulmonary chondroma are consistent with a diagnosis of Carney’s triad; which was originally described in 1977. Other diagnoses associated with Carney’s triad include adrenal adenoma (13%) and oesophageal leiomyoma. Young women are typically affected, with no familial cases reported and no responsible genetic mutation has yet been identified. Complete triad cases are rare; this is the 22nd reported case and the first in a patient of African origin. The widespread and atypical distribution of paragangliomata in our patient is characteristic of Carney’s triad, with involvement of the middle mediastinum, right adrenal gland, bilateral carotid body tumours and liver hilum. Associated GISTs have a predilection for the stomach; however our case also demonstrates the unusual occurrence of GIST within the jejunum. Carney’s triad related tumours and sporadic tumours vary considerably with regards to age at presentation, treatment and prognosis, thus highlighting the importance of a correct diagnosis.
TEXT PAGES 1UP.indd 7 4/1/08 08:58:20

Multiple endocrine manifestations of the MTTL1 A3243G mutation
B Khoo12, F Medici1
1Dept of Metabolic Medicine, Homerton University Hospital, Homerton Row, London, 2Deptof Endocrinology, Royal Free Hospital, London
A 23-year-old Indian lady was referred to our service for evaluation of her low body weight and hypothyroidism. She had been diagnosed with hypothyroidism at age 12 and had been treated with levothyroxine since then, but had discontinued it for the 6 months preceding our assessment. Clinical examination revealed an under-nourished woman with normal sexual development, patches of vitiligo on the hands, a weight of 28.4 kg, height 1.42 m and a BMI of 14.08. Thyroid function tests were consistent with primary hypothyroidism with undetectable free T4 of <3.9 pmol/l and a TSH of 375 mU/l. Thyroid peroxidase antibodies were within normal limits at 12 (NR <50 IU/ml).
Although levothyroxine was re-started and titrated to achieve euthyroid levels, she continued to suffer from chronic frontal headaches, loss of weight, poor appetite, nausea and vomiting. A short Synacthen test showed evidence of a subnormal cortisol response (baseline cortisol 292 nmol/l, peak cortisol 485 nmol/l); interestingly her ACTH at 0900h was within normal limits at 11 ng/l (NR <50). Anti-adrenal and tissue transglutaminase antibodies were both negative. A 75g oral glucose tolerance test showed a fasting glucose: 4.2 mmol/l, 2-hour glucose 8.7 mmol/l.
She was commenced on hydrocortisone replacement. During follow-up over the next year she continued to lose weight to a nadir of 24 kg and developed seizures with tongue biting, limb shaking, moaning and other incomprehensible verbalisations. She required admission to intensive care with status epilepticus. Her recovery from this was complicated by pneumonia and Clostridium difficile infection. An EEG at this juncture showed no diagnostic changes.
A few months later she was re-admitted with myoclonic seizures, cortical blindness and deterioration in consciousness. An MRI scan revealed evidence of bilateral T2 hyperintensity of the cortex and subcortex in the right temporo-parietal and the left temporo-occipital lobes. Her lactate levels were elevated at 6.70 (local NR 0.6-2.4 mmol/l). A muscle biopsy revealed evidence of mitochondrial abnormalities and significant amounts of ragged red fibres, as well as inflammation. Analysis of her mitochondrial DNA showed the presence of the MTTL1 A3243G mutation in blood (heteroplasmy 43%). She was commenced on coenzyme Q10 and nutritional supplementation via a percutaneous gastrostomy. She has since been fit-free and has gained 13 kg in weight.
Although the A3243G mutation is well known as a cause of maternally-inherited diabetes mellitus and sensorineural deafness, this mutation is associated with other endocrinological disorders. In our patient’s case, these were primary hypothyroidism, secondary hypoadrenalism and glucose intolerance in association with anorexia, low body weight and vitiligo. The case presentation will review the other known endocrinological associations with the A3243G mutation.
TEXT PAGES 1UP.indd 8 4/1/08 08:58:21

A case of Neurofibromatosis type 1 with Phaeochromocytoma and Gastrointestinal Stromal Tumour (GIST)
H Kahal, E. Cooper, D Coppini Poole Hospital NHS Foundation Trust, Poole
A 69 year old female with newly diagnosed phaeochromocytoma was seen in clinic. Her past medical history included hypertension which was well controlled on Atenolol.
She first presented with abdominal discomfort to the general surgeons in 1990, when an abdominal computed tomography (CT) scan revealed a large incidental right suprarenal mass. Biopsies were deemed difficult due to adherent bowels to the mass and follow-up CT scans suggested a benign stable adenoma. Urinary catecholamines or metanephrines had never been checked.
In June 2006 she re-presented with peritonitis and a laparotomy revealed a thickened wall cyst at the duodeno-jejunal junction. An elective excision of the cyst was performed in April 2007 and during the procedure it was very difficult to achieve haemodynamic stability because of variations in systolic blood pressure of between 50 – 200 mmHg. An unplanned resection of the mass was concomitantly performed.
Histology of the cyst showed a (23 X 20 X 20 mm) malignant Gastrointestinal Stromal Tumour (GIST) and histology of the suprarenal mass confirmed phaeochromocytoma (67 X 50 X 25 mm; weighing 80 grams).
She had numerous truncal and upper limb neurofibromata, café-au-lait macules, axillary freckling and relative macrocephaly. Her mother and the eldest of her two daughters had a similar phenotype. One daughter had learning difficulties.
Although unlikely in this age group we considered the possibility of MEN IIB, but genetic screening for RET proto-oncogene was negative. She was normocalcaemic although serum PTH was 5.2 pmol/L (0.5 - 4.4). Thyroid ultrasound showed a multinodular goitre with no dominant nodule.
Although the patient had neurofibromatosis type 1, her phaeochromocytoma only came to light 17 years later, during surgical intervention for an abdominal cyst. The coincidence of both gastrointestinal stromal tumours (GIST) and phaeochromcytoma in neurofibromatosis type1 is very rare [1].Clinical studies indicate that GISTs are identified in 5 - 25% of patients with type 1 neurofibromatosis [2-5]. Gastrointestinal symptoms are not uncommon in patients with phaeochromocytoma. We recommend that such symptoms in patients with NF-1 may need further investigations to rule out the possible co-existence of GISTs.
References 1. Kramer K, Hasel C, Aschoff AJ, Henne-Bruns D, Wuerl P. Multiple gastrointestinal stromal tumors and bilateral pheochromocytoma in neurofibromatosis. World J Gastroenterol. 2007 Jun 28; 13(24):3384-7. 2. Rhonda K Yantiss, Andrew E Rosenberg, Lisa Sarran, Peter Besmer and Cristina R Antonescu. Multiple gastrointestinal stromal tumors in type I neurofibromatosis: a pathologic and molecular study. Modern Pathology (2005) 18, 475–484.
TEXT PAGES 1UP.indd 9 4/1/08 08:58:21

3. Fuller CE, Williams GT. Gastrointestinal manifestations of type 1 neurofibromatosis (von Recklinghausen’s disease). Histopathology 1991;19:1–11. 4. Giuly JA, Picand R, Giuly D, et al. Von Recklinghausen disease and gastrointestinal stromal tumors. Am J Surg 2003;185:86–87.5. Ghrist TD. Gastrointestinal involvement in neurofibromatosis. Arch Intern Med 1963;112:357–362.
TEXT PAGES 1UP.indd 10 4/1/08 08:58:21

An unusual cause of panhypopituitarism
LF Clark1, D Culligan2, D Currie3, JS Bevan4
Department of Endocrinology, Raigmore Hospital, Inverness1
Departments of Haematology2, Neurosurgery3 and Endocrinology4, Aberdeen Royal Infirmary, Aberdeen
Initial presentation A 59 year old man presented with polyuria, polydipsia, confusion, leg pain, oedema and pyrexia. He had a past history of splenectomy for marginal zone lymphoma in 2003 and a history of alcohol excess. His only medication was omeprazole. On examination he was tachycardic and tachypnoeic. Blood pressure 132/88 and temperature 38.8oC. He was confabulating and gait was unsteady. Other neurological findings and examination were normal.
Initial investigations and management He was hypernatraemic (Na+ 153mmol/l, K+ 4.0mmol/l), creatinine 129µmol/l. Liver function tests: ALT 43U/l, AP 116U/l, GGT 173U/l. Fasting glucose 6.4mmol/l. TSH 1.44mU/l (0.3 – 3). Chest x-ray showed nil abnormal. He was initially treated empirically with antibiotics and IV fluids. CT scan showed a 2x2cm suprasellar mass. A diagnosis of cranial diabetes insipidus was made.
Further investigations and management He was referred to Endocrinology and further investigations were suggested. TSH 0.97mU/l (0.3-3), fT3 3.2pmol/l (3-7), fT4 8pmol/l (10-25), ACTH <5ng/l, Cortisol <20nmol/l, LH <0.1U/l, FSH <0.1U/l, Testosterone <0.1nmol/l, Prolactin 206mU/l (40-520). Serum and urine osmolalities were checked after commencement of glucocorticoid replacement, serum osmolality 363mosmol/kg, urine osmolality 513mosmol/kg. Blood glucose was 25mmol/l after glucocorticoid replacement was started and he was commenced on an insulin sliding scale. When glucocorticoid doses were reduced blood glucose levels did not require treatment. He was treated with replacement hydrocortisone, levothyroxine and desmopressin and prepared for surgery. He underwent craniotomy and tumour extending out of posterior aspect of chiasm and extending into hypothalamus was found. A frozen section showed lymphoma that was later defined as diffuse large B-cell lymphoma that was thought to have transformed from the original marginal zone lymphoma. Post operative recovery was slow. He was treated with methotrexate chemotherapy and developed acute renal failure as a result. He underwent haemodialysis and died 10 weeks after admission to hospital.
DiscussionThis is an unusual case in that it is rare for marginal zone lymphoma, which is considered to be an indolent lymphoma, to transform and there are few reports of pituitary failure due to lymphoma (1,2). In a series of 12 cases of marginal zone lymphoma that transformed into large B-cell lymphoma, none involved the CNS (1).In keeping with this case, most marginal zone lymphoma related deaths are associated with transformation to diffuse large cell lymphoma and are associated with p53 and other mutations (3).
TEXT PAGES 1UP.indd 11 4/1/08 08:58:21

References 1. Camacho, F.I., Mollejo, M., Mateo, M-S et al. Progression to Large B-Cell Lymphoma in Splenic Marginal Zone Lymphoma. Am J Surg Pathol 2001 25(10):1268-12762. Samuels, M.A. and De La Monte, S. A 49 Year Old Man with Hypopituitarism, Multifocal Neurological Defects and an Intracranial Mass. N Engl J Med 1994 331:1093-11043. Oscier, D., Owen, R. and Johnson, S. Splenic Marginal Zone Lymphoma. BloodReviews 2005 19: 39-51
TEXT PAGES 1UP.indd 12 4/1/08 08:58:21

Apparent Familial Isolated Hyperparathyroidism due to MEN-1 11q13 Mis-sense Mutation Successfully Treated with Cinacalcet
KL Bavidge1, TJ Archer1, GC Wishart2 and C Parkinson1
The Ipswich Hospital, Heath Road, Ipswich1, Addenbrooke’s Hospital, Hills Road, Cambridge2
Parathyroidectomy remains the treatment of choice for problematic hyperparathyroidism. Calcimimetics may have a role where surgery is contraindicated, refused or unsuccessful. In a placebo controlled study, Cinacalcet achieved normocalcaemia in 73% of primary hyperparathyroid subjects with mean baseline serum calcium (Ca2+) and parathyroid hormone (PTH) levels of 2.67±0.12 mmol/l and 11.0±3.78 pmol/l respectively1. There are, however, no published reports of Cinacalet use in patients with parathyroid hyperplasia.
A 36 year old female was screened after elevated Ca2+ was observed in her brother and paternal uncle. Ca2+ of 3.00 mmol/l was found, with 8 family members from 3 generations thereafter observed to have hypercalcaemia or manifestations thereof. Subsequently a mis-sense 11q13 MEN-1 mutation was identified in 7 family members, including this patient, and a diagnosis of familial isolated primary hyperparathyroidism established2. SestaMIBI demonstrated dominant uptake in the left lower position. At operation (1995), three hyperplastic parathyroid glands were removed (right lower gland left in situ as macroscopically normal) and calcium stabilised.
Four years later, routine surveillance revealed a rising serum Ca2+ but normal PTH. Repeat SestaMIBI demonstrated uptake at the inferior aspect of the right thyroid lobe. Given that Ca2+ levels were 2.62-2.66 mmol/l, further surgery was not deemed appropriate at this stage.
In 2002, serum Ca2+ rose to 2.93 mmol/l and repeat SestaMIBI demonstrated continued activity in the right lower position. A further neck exploration took place in 2004 and histology once again confirmed parathyroid hyperplasia. Post operatively, she remained hypercalcaemic with PTH inappropriately normal.
Given ectopic (mediastinal) parathyroid tissue in other family members and persistent hypercalcaemia, repeat SestaMIBI with wide fields was performed. Once again this identified activity at the right side of the neck with possible increased uptake at the right nipple (thought to represent a submammary lymph node) and myocardium. A further neck exploration at a tertiary centre removed more tissue from the right lower pole and resulted in a laryngeal nerve palsy, but histology revealed no obvious parathyroid tissue.
Despite the above, she remained hypercalcaemic and symptomatic and thus Cinacalcet was considered. At baseline serum Ca2+ was 2.75 mmol/l and PTH was 11 pmol/l. After two weeks of Cinacalcet 30mg b.d., this had dropped to 2.53 mmol/l and has remained within normal limits to date.
Cinacalcet is an oral calcimimetic which increases sensitivity of PTH-sensing receptors to extracellular calcium, reducing PTH secretion. There is no previous
TEXT PAGES 1UP.indd 13 4/1/08 08:58:21

literature on the use of Cinacalcet in patients with familial hyperparathyroidism/parathyroid hyperplasia with recurrent hyperparathyroidism after failed surgery. This case suggests that Cinacalcet may be of use in patients with familial hyperparathyroidism who remain hypercalcaemic despite intervention.
Subsequently, elevated gut peptides have been described in her brother with further investigations in to the possibility of true MEN-1 currently underway.
References 1Peacock M et al. Cinacalcet hydrochloride maintains long-term normocalcaemia in patients with primary hyperparathyroidism. J Clin Endocrinol Metab 2005; 90(1):135-1412Teh BT et al. A family with isolated hyperparathyroidism segregating a missense MEN1 mutation and showing loss of the wild-type alleles in the parathyroid tumors. Am J Hum Genet 1998; 63:1554-1549
TEXT PAGES 1UP.indd 14 4/1/08 08:58:22

Severe postmenopausal hyperandrogenism due to insulin resistance state: A case report
Ebaa Al-Ozairi 1, Andrew Advani 1, Kim Johnson 1, Enid Michael 2, Richard Quinton1
Departments of Endocrinology1 and Womens’ Health2, Royal Victoria Infirmary & University of Newcastle-upon-Tyne, Newcastle
Background: Hyperandrogenism in postmenopausal women is poorly characterized and often leads to fruitless investigation for adrenal/ovarian tumor if the association of insulin resistance is not recognized. We present a case of an obese insulin resistant postmenopausal woman with high testosterone level, failing to suppress with endocrine testing and responsive to weight loss and orlistat treatment.
Case summary: A 56-year-old woman (gravida 6 para 2) complained of localized facial hirsutism. Menses had been regular, but her weight had progressively increased with more rapid gain after menopause age 50yrs. She developed Type 2 diabetes, hypertension and dyslipidaemia by 53yrs. Examination revealed morbid central obesity (Body Mass Index 46.2 kg.m-2; waist circumference 120 cm), acanthosis nigricans and multiple skin tags indicative of insulin-resistance (IR), Ferriman-Gallwey score 10/36, but no virilization.
Investigations confirmed marked biochemical hyperandrogenism with hyperinsulinaemia and serum gonadotrophin levels appropriate for postmenopause. Serum cortisol level suppressed physiologically with dexamethasone suppression testing, whereas serum testosterone (T) failed to suppress. Ultrasonographic and computed tomographic imaging showed normal ovaries and adrenals, with a thin endometrial stripe.
Given her obesity and co-morbidities, the risks of bilateral salpingo-oophrectomy were felt to outweigh any clinical benefits given the low pre-test probability of ovarian neoplasia. She therefore underwent an 8-week period of intensive diet and lifestyle modification. She was commenced on simple home resistance exercise and 120 mg of orlistat thrice-daily with full dietetic support (600 kCal deficits). By the end of this period she had lost nearly 10% of initial body weight which was maintained at 6 months. Serum T normalized, with a proportional fall in fasting insulin and repeat ultrasonography showed a thin, linear endometrium.
Conclusion: The above case illustrates the centrality of hyperinsulinaemia in postmenopausal hyperandrogenism. In this patient’s case, hyperandrogenism was not attributable to a tumour aetiology, but was instead directly linked to somatic insulin resistance caused by morbid obesity. Such cases are likely to become increasingly frequent with the exponential rise in the prevalence of obesity worldwide.
TEXT PAGES 1UP.indd 15 4/1/08 08:58:22

Does IGF-1 deficiency have a role in the development of syringomyelia?
A Smyth, SC Wong, SF Ahmed Bone and Endocrinology Research Group, Royal Hospital for Sick Children, Yorkhill, Glasgow
Laron Syndrome (LS) is the commonest cause of primary growth hormone insensitivity (GHI), and is characterised by extreme short stature, characteristic facial features, high serum GH levels and very low serum IGF-1 levels. It is an autosomal recessive condition with abnormalities of the growth hormone receptor gene. Syringomyelia is a cystic cavity within the spinal cord which develops due to inadequate circulation of CSF secondary to an obstruction. It has been previously described in cases of short stature and growth hormone deficiency and has been reported in an adult with GHI and Type I Chiari malformation (TICM). There are no previous reports of its association with GHI in children.
A young prepubertal girl of Pakistani origin presented at the age of 7.1yrs with proportionate short stature and a height of 88.3cm (Ht SDS, -6.4). She was born at term by ventouse vaginal delivery weighing 2.72kg. Shortly after birth she was admitted with breathing abnormalities secondary to right upper lobe collapse of unclear aetiology. Her mother (Ht SDS, -2.7) and father (Ht SDS, -3.7) were first cousins and had 3 other children of average height. In addition, the index girl’s bone age was delayed by 3.5 years, she had a weak, immature voice, bilateral clinodactyly, frontal bossing and mid-facial hypoplasia, facial features that were characteristic of LS. Arginine GH stimulation showed a series of GH levels ranging between 21.5mu/l and 101mu/L; serum IGF-1 level was undetectable, TFTs were normal and LH/FSH showed a prepubertal response. Fasting blood glucose measurements ranged between 4.5-5.8mmol/l and serum cholesterol and LDL were raised at 7.7mmol/l (2.8-5.7mmol/L) and 6.1mmol/l (<4.5mmol/l), respectively. An MRI of the pituitary glanddid not show any pituitary abnormality but showed a cervical syrinx at C5 as a coincidental finding. She had no neurological findings and further MRI scans over a period of 2 years did not show any change in the original findings, no evidence of obstruction and no TICM.
In children with growth hormone deficiency and syringomyelia, treatment with growth hormone therapy and a consequent increase in height velocity may be associated with a worsening of neurological symptoms. However, rapid growth has also been associated with resolution of syringomyelia. After careful discussion with the family, at the age of 10.7 yrs, the patient commenced therapy with recombinant IGF-I, which became available for children with primary forms of GHI in August 2007. Given the relatively short period of therapy, a clinical response has not yet been detected. There have been no neurological symptoms or signs over this period.
The identification of a cervical syrinx in a child with GHI broadens the phenotype spectrum of this condition. It is uncertain whether the pathogenesis of a cervical syrinx is related to short stature, associated craniofacial anomalies or IGF-1 deficiency per se. Screening for such conditions may be necessary in children with profound congenital GH or IGF-1 deficiency.
TEXT PAGES 1UP.indd 16 4/1/08 08:58:22

Management of phaeochromocytoma in the presence of critical coronary artery disease
IS Mackenzie1, N Cartwright4, C Mitchell2, M Gurnell2, MJ Brown1, VK Chatterjee2,NV Jamieson3 K Valchanov5, SAM Nashef4, HL Simpson2
Clinical Pharmacology Unit1, Institute of Metabolic Science2, Department of Surgery3, Addenbrooke’s Hospital and University of Cambridge, Department of Cardiothoracic Surgery4, and Anaesthetics5, Papworth Hospital, Cambridge
A 60-year-old man was admitted to hospital complaining of breathlessness. He had a history of hypertension and recently diagnosed type 2 diabetes mellitus. He was found to be in pulmonary oedema and had episodes of non-sustained ventricular tachycardia. ECGs showed anteroseptal Q waves, persistent ST elevation and lateral T wave inversion, but serum troponin was normal. Coronary angiography showed severe disease with 70% stenosis of left main, occlusion of the left anterior descending, multiple tight stenoses in the circumflex and right coronary arteries and antero-apical aneurysm with severely impaired left ventricular function (ejection fraction 10%). He was scheduled for coronary artery bypass graft and aneurysm surgery. Following induction of anaesthesia and skin incision, the operation was abandoned due to uncontrolled hypertension and tachycardia. Post-operatively, urinary noradrenaline (4862 nmol/24hrs), adrenaline (2611 nmol/24hrs) and vanillylmandelic acid (118 µmol/24hrs) levels were found to be significantly elevated and a CT scan showed a 4.6cm right adrenal mass consistent with a phaeochromocytoma. This was confirmed on 123I-MIBG scanning. He was treated with oral phenoxybenzamine and carvedilol, achieving good blood pressure control. A decision to undertake cardiac and adrenal surgery as a joint procedure was made. Phenoxybenzamine was stopped seven days before surgery. A pulmonary artery flotation catheter was inserted and he was treated with the reversible alpha-antagonist phentolamine intravenously, titrated to maintain normal systemic vascular resistance. At operation, an intra-aortic balloon was inserted first and counterpulsation used to prevent coronary ischaemia, before proceeding to a sternolaparotomy. The adrenal mass was removed, intravenous phentolamine was stopped and ADH started. Cardiopulmonary bypass was then instituted and quadruple coronary bypass and left ventricular aneurysmectomy performed. He made a good recovery and was discharged 14 days later. Two months postoperatively he was asymptomatic and normotensive. Left ventricular function remained poor on echocardiography.This is the first reported case which describes a combination of phaeochromocytoma, critical coronary artery disease and severe left ventricular impairment. Disappointingly there was no improvement in left ventricular function after successful resection of the phaeochromocytoma, suggesting aetiology was ischaemic cardiomyopathy rather than catecholamine excess. We reasoned that a two-stage surgical approach would be fraught with risk: bleeding and severe haemodynamic instability may occur if the cardiac procedure was done first in untreated phaeochromocytoma; conversely, there was a significant risk of potentially fatal cardiac events if the adrenal tumour was resected first. Moreover, had the patient been irreversibly alpha-blocked prior to cardiac surgery, the ability to use adrenergic vasopressor agents to maintain haemodynamic stability post-bypass would have been lost. In such circumstances, we suggest that the strategy adopted here may be optimal.
TEXT PAGES 1UP.indd 17 4/1/08 08:58:22

POSTER PRESENTATIONS
1. Carcinoid crisis during fine needle biopsy of hepatic metastasis: Highlighting a pitfall in practise S H Ahmed, P Dyer, S Roy-Choudhury I Geh, S Karandikar Birmingham Heartlands Hospital, Heart of England NHS Foundation Trust, Birmingham
2. A Case of Primary Amenorrhoea U Ayyagari, N Karavitaki, JAH Wass Department of Endocrinology, Oxford Centre for Diabetes, Endocrinology and Metabolism, Churchill Hospital, Oxford
3. Use of selective embolisation in pre-operative debulking of a mediastinal paraganglioma associated with an SDHB mutation OB Chaudhri1, T Tan1, K Qureshi2, JE Jackson3, A Khagani4, AG Mitchell2,NM Martin1, K Meeran1
Departments of Endocrinology1 and Imaging3, Imperial College Healthcare NHS Trust, London and Departments of Cardiology2 and Cardiothoracic Surgery4, Royal Brompton and Harefield NHS Trust, London
4. Seeking fairness and Cushing’s syndrome R Chaudry, B Field, SM Thomas, JK Powrie, PV Carroll Department of Endocrinology, Guy’s and St. Thomas’ NHS Foundation Trust, London
5. Treatment of a non-functional metastatic somatostatinoma M Druce1, D Spalding2, H Wasan2, TMM Tan1, K Meeran1
1Endocrine Unit, Department of Investigative Medicine, 2Liver, Biliary and Pancreatic Service, Imperial College Healthcare NHS Trust, Hammersmith Hospital, London
6. Case of extreme hypercalcaemia CR Kankara, C Geevarghese, A Melvin, N Morrish, WS Wassif Bedford Hospital NHS Trust, Bedford
7. Successful radio-iodine ablation therapy in amiodarone induced thyrotoxicosis with low thyroid technetium uptake JT George¹, JR Crook², V Jayagopal¹ Department of Endocrinology¹, Department of Cardiology², York Hospital, York
8. Unmasking of diabetes insipidus with prednisolone treatment AH Ghaffar, B McGowan, G Tharakan, R Cox, N Narayan, E Hatfield, K MeeranEndocrine Unit, Department of Investigative Medicine, Imperial College Healthcare NHS Trust, Hammersmith Hospital, Du Cane Road, London
TEXT PAGES 1UP.indd 18 4/1/08 08:58:22

9. Polyuria in pregnancy U Graham1, C Bailie2, DR McCance1,2, CH Courtney1,2
Regional Centre for Endocrinology and Diabetes1, Royal Jubilee Maternity Hospital2 Royal Victoria Hospital, Belfast
10. MEN Variants and an Interesting Family History P Grant Eastbourne District General Hospital, Eastbourne
11. Pan-hypopituitarism and diabetes insipidus as a consequence of metastatic anaplastic lymphoma A HamdaRoyal Free Hospital, London
12. Acute onset of refractory hypertension in the third trimester of pregnancy CE Higham, I Perogamvros, PJ Trainer Department of Endocrinology, Christie Hospital, Manchester
13. Lymphocytic hypophysitis associated with unilateral loss of vision due to inflammation of the optic nerve separate from the pituitary lesion KF Hunt1, JP Miell2, P Riordan-Eva1, SA Aylwin1
1King’s College Hospital NHS Foundation Trust, 2University Hospital Lewisham, London
14. Tereparatide for treatment of hypoparathyroidism J Joharatnam, N Martin, K Meeran Endocrine Unit, Imperial College Health Care NHS Trust, London
15. Pitfalls in the diagnosis of a thyrotrophinoma J Joharatnam1, V Lecamwasam1, F Roncaroli1, A Mehta2, N Mendoza3, N Martin, K Meeran Department of Pathology1, Department of Radiology2, Department of Neurosurgery3, Imperial College Health Care Trust, London
16. Vasoactive intestinal polypeptide secreting pancreatic tumour (VIPoma): long term survival after orthotopic liver transplantation PC Johnston1,JE Ardill2,BM Johnston2, DR McCance1, 2
Regional Centre for Endocrinology and Diabetes1, Neuroendocrine Tumour Group2, Royal Victoria Hospital, Belfast
17. Hypocalcaemia in adulthood: A case of Di-George syndrome P Johnston1, P Morrison2, SJ Hunter1
Regional Centre for Diabetes and Endocrinology1, Department of Clinical Genetics2, Royal Victoria Hospital, Belfast
18. Macroprolactinomas presenting as nasal polyps: A series of three cases PC Johnston, HC Courtney, SJ Hunter, DR McCance Regional Centre for Diabetes and Endocrinology, Royal Victoria Hospital, Belfast
TEXT PAGES 1UP.indd 19 4/1/08 08:58:23

19. Does cyclical acromegaly exist? E Karra, C McHugh, A Panahloo, LJ Seal
St George’s Teaching Hospital, London
20. Androgen secreting tumours, an infrequently diagnosed cause of raised testosteroneS Kohler, N Karavitaki, JAH Wass Department of Endocrinology, Oxford Centre for Diabetes, Endocrinology and Metabolism, Oxford
21. A rare case of reversible painful gynaecomastia due to feminising adrenal cortical carcinoma S Lakshmi, JFoote Department of Endocrinology, Royal Cornwall Hospital, Treliske, Truro Cornwall
22. A case of metastatic paraganglioma presenting 20 years after initial surgery L Leelarathna1, A Crown1, S Aylwin2, KM Schulte2
Royal Sussex County Hospital1, Brighton, Kings College Hospital, London2
23. A hole in one B McGowan, C Caputo, V Lecamwasam, E Hatfied, K Meeran Department of Endocrinology, Charing Cross Hospital, Fulham Palace Road, London
24. Management of a phaeochromocytoma in pregnancy B McGowan1, C Williamson2, K Meeran1, A Banerjee2, L Min3, B Fleming3, D Bassett1, T Tan1
Department of Investigative Science1, Institute of Reproductive and Developmental Biology2, Imperial College, Department of Surgery3,Healthcare NHS Trust, Hammersmith Hospital, London
25. A 123I-MIBG-Positive Gastrointestinal Stromal Tumour: A Case Of (Incomplete) Carney’s Triad KS Myint1, C Mitchell1, KK Balan2, S Coghill3, NV Jamieson4, R Bulusu5
Jennings A6; Chatterjee VKK1; Simpson HL1
Institute of Metabolic Science1, Nuclear Medicine2, Pathology3, Surgery4 and Clinical Oncology5, Addenbrooke’s Hospital, Cambridge; Department of Endocrinology, Queen Elizabeth Hospital, King’s Lynn6
26. Is surgery or medical therapy the most appropriate treatement of a sporadic gastrinoma? GMK Nijher, V Salem, WS Dhillo, JHD Bassett, JF Todd, NM Martin, K Meeran, T Tan Endocrine Unit, Department of Investigative Medicine, Imperial College Healthcare NHS Trust, Hammersmith Hospital, London
TEXT PAGES 1UP.indd 20 4/1/08 08:58:23

27. Ectopic ACTH induced Cushings including ACTH producing Metastasis within the Adrenal P Pusalkar, A Nasruddin, D Russell-Jones Royal Surrey County Hospital, Guildford, Surrey
28. HIV and Adrenal Insufficiency H Rathur, F Rathur, H Soran Manchester Royal Infirmary, Manchester
29. Phaeochromocytoma in Pregnancy A Dilemma for the Endocrinologist, Endocrine Surgeon, Obstetrician and Anaesthetist
MA Saeed1, A Fernandez1, N Karavitaki1, S Gardner2, JAH Wass1
1Department of Endocrinology, Oxford Centre for Diabetes, Endocrinology and Metabolism, Churchill Hospital, Oxford, 2Department of Endocrinology, Stoke Mandeville Hospital, Aylesbury
30. A ‘Big’ deal AH Sam, V Salem, AJ Ogilvie, B Patel, MR Clements Department of Endocrinology and Diabetes, Watford General Hospital
31. Paraganglioma of the urinary tract A Solomon1, P Moshe2, I Shimon3
Endocrinology Institute1, Surgical Oncology2, Endocrinology Institute3,Sheba Medical Centre Tel-Hashomer , Israel
32. Catecholamine secreting tumours - pitfalls in tumour localisation U Srirangalingam, M Matson, R Carpenter, RH Reznek, WM Drake
St Bartholomew's Hospital, West Smithfield, London
33. Unusual presentation of a carcinoid tumour A Swamy1,JDA Clark2
Addenbrooke’s Hospital, Cambridge1, West Suffolk Hospital, Bury St Edmunds2
34. Amiodrone induced thyrotoxic psychosis A Swiecicka Furness General Hospital, Barrow-in-Furness, Cumbria
35. Treatment of Glypressin Induced Hypoglycaemia with Desmopressin Acetate (DDAVP)JM Triay, JM Watson Musgrove Park Hospital, Taunton, Somerset
36. Challenges in parathyroid carcinoma: Never give up W Candy Sze, JP Monson, WM Drake St Bartholomew’s Hospital, West Smithfield, London
37. Two Endocrine Diagnoses for the Price of One B Zalin, K Shotliff Chelsea and Westminster Hospital, Fulham Road, London
TEXT PAGES 1UP.indd 21 4/1/08 08:58:23

38. Successful Treatment Of Adrenal Carcinoma By Thalidomide M Malige1, JD Eaton2, R Hawkins3 and Walmsley D1
Departments of Endocrinology1 and Oncology2, Royal Lancaster Infirmary and of Medical Oncology, Christie Hospital, Manchester3
Notes
TEXT PAGES 1UP.indd 22 4/1/08 08:58:24

Society for Endocrinology 22 Apex Court WoodlandsBradley Stoke Bristol BS32 4JT UK
Contact: Shirine Borbor/Joanne Galer Tel: 01454-642210 Fax: 01454-642222 Email: [email protected] Web: www.endocrinology.org
Society for Endocrinology Company Limited by Guarantee Registered in England No 349408 Registered Office as above Registered Charity No 266813
TEXT PAGES 1UP.indd 23 4/1/08 08:58:24

Ginnie Hall,Aiming high
For adults with GHD, whether childhood- or late-onset in origin.
The major effects of Norditropin® SimpleXx® are stimulation ofskeletal and somatic growth and pronounced influence on thebody's metabolic processes, resulting in an increase in bonemass with prolonged treatment.1
Information about adverse event reporting can be found at www.yellowcard.gov.uk Adverse events should also be reported to Novo Nordisk® – Telephone Novo Nordisk®
Customer Care 0845 6005055.Legal category: POM, CD4.
Please consult the summary of product characteristics before prescribing,particularly in relation to side-effects, precautions and contra-indications.
Reference:1. Norditropin® SimpleXx® SPC, Novo Nordisk® 2006.
Further information is available from: Novo Nordisk UK,Broadfield Park, Brighton Road, Crawley, West Sussex RH11 9RT.Tel: +44 (0) 1293 613555 Fax: +44 (0) 1293 613535 www.novonordisk.co.uk
UK/XX/1107/0003 – November 2007
NNS04J07018x_Journal_Ad_A5_AW_V1 4/12/07 10:44 Page 1
TEXT PAGES 1UP.indd 24 4/1/08 08:58:29