Clinical Case Challenges In Neuro- Optometry I Thomas J. Landgraf, O.D., F.A.A.O.
64
Clinical Case Challenges In Neuro- Optometry I Thomas J. Landgraf, O.D., F.A.A.O.
-
Upload
immanuel-ervin -
Category
Documents
-
view
221 -
download
1
Transcript of Clinical Case Challenges In Neuro- Optometry I Thomas J. Landgraf, O.D., F.A.A.O.
Clinical Case Challenges In Neuro-Optometry I
Thomas J. Landgraf, O.D., F.A.A.O.
“Clinical Case Challenges inNeuro-Optometry”
Thomas Landgraf, O.D., F.A.A.O.Clinical Associate Professor, UMSL College of Optometry
My Background
Graduate of ICO…Chicago
Residency at PCO…Philadelphia
SCO x 15 years…Memphis
Now at UMSL College of Optometry
In terms of Neuro-Eye… Dr. Lawrence Gray at ICO & PCO
My Background
At SCO…Chief of Ocular Disease Goals for this lecture Not an expert Share patient care
experiences Share “optometric
legal consultant” experiences
Resources
Journals and Internet Review of Optometry Review of Ophthalmology Handbook of Ocular Disease
Management Clinical Guide To Ophthalmic Drugs
Neuro-Optometry
Why spend 3 hours on it?
Conditions are both: Vision threatening Life threatening
“True” ocular emergencies
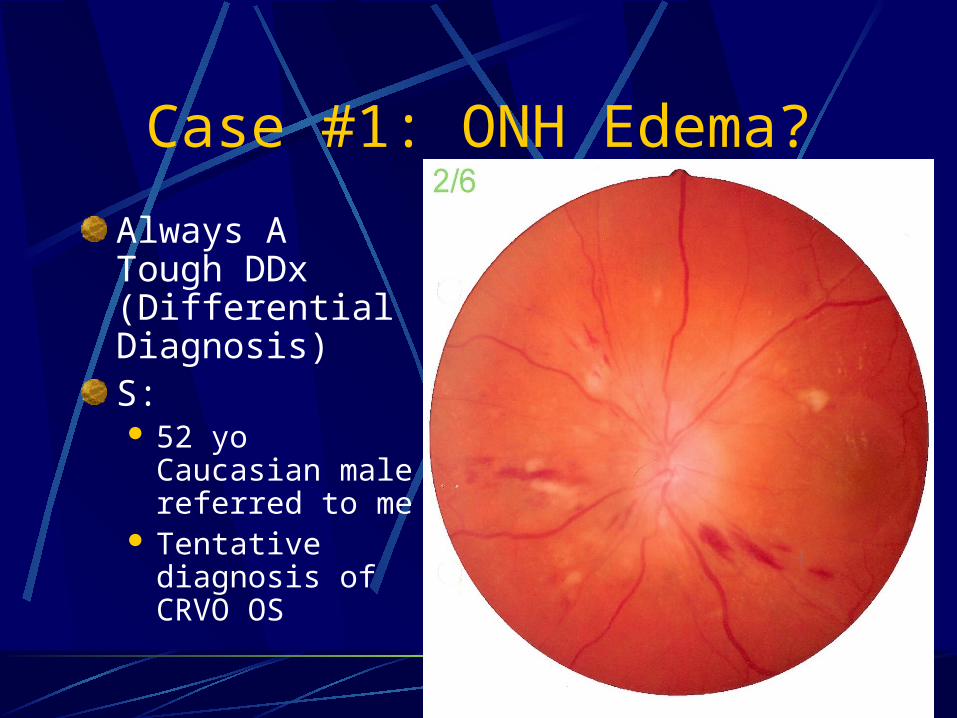
Case #1: ONH Edema?
Always A Tough DDx (Differential Diagnosis)S: 52 yo Caucasian
male referred to me
Tentative diagnosis of CRVO OS
Case #1: ONH Edema?
Always a Tough DDx
S:Painless vision loss OS x 2 weeksProsthetic OD due to traumaNo significant medical or ocular conditons
Low daily dosage of methadoneNicotine patch
Case #1: ONH Edema?
Always a Tough DDxO:BVA OS: 20/400OS pupil round and reactive to lightNormal SLXTonometry 17 mm HgBP: 280/170 RAS: not done at previous
visit
Case #1: ONH Edema?
Always a Tough DDx
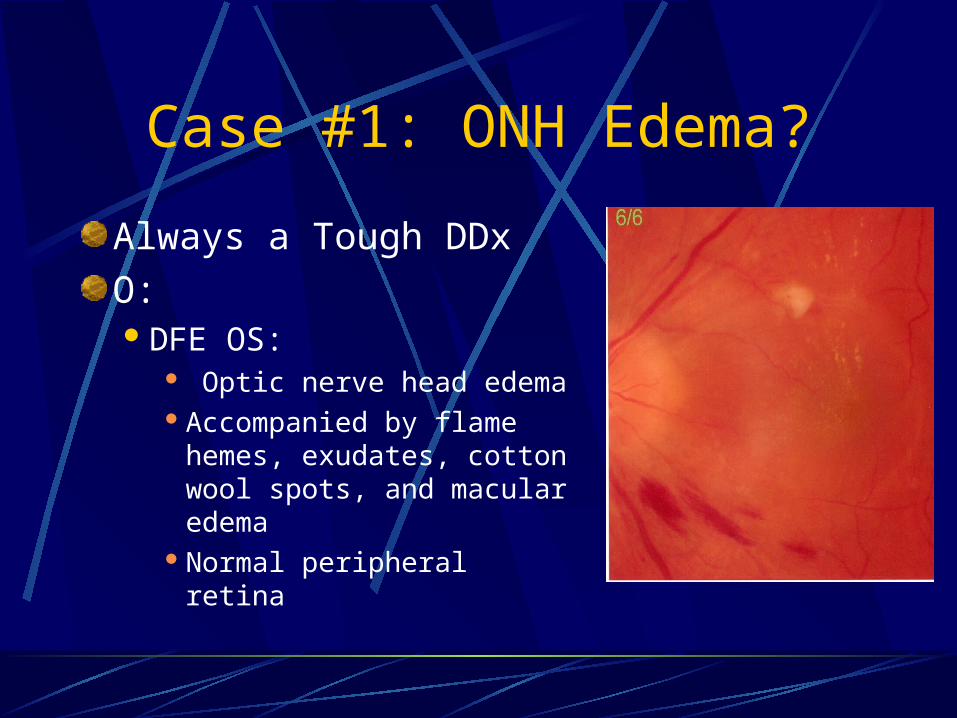
O:DFE OS:
Optic nerve head edemaAccompanied by flame
hemes, exudates, cotton wool spots, and macular edema
Normal peripheral retina
Case #1: ONH Edema?
Always a Tough DDx
A: Malignant Hypertension and Resultant Retinopathy OS
P: Immediate referral to medical center For lowering of BP Referral to retinal specialist
Level Of Comfort Confirmation
Case #1: ONH Edema?
Always a Tough DDx
Follow-up 4 months laterCurrent meds: minoxidil, norvasc,
coumadinHTN and its complicationsNoted improved vision
But some glare, distortion, “wavy lines” in central vision

Case #1: ONH Edema?
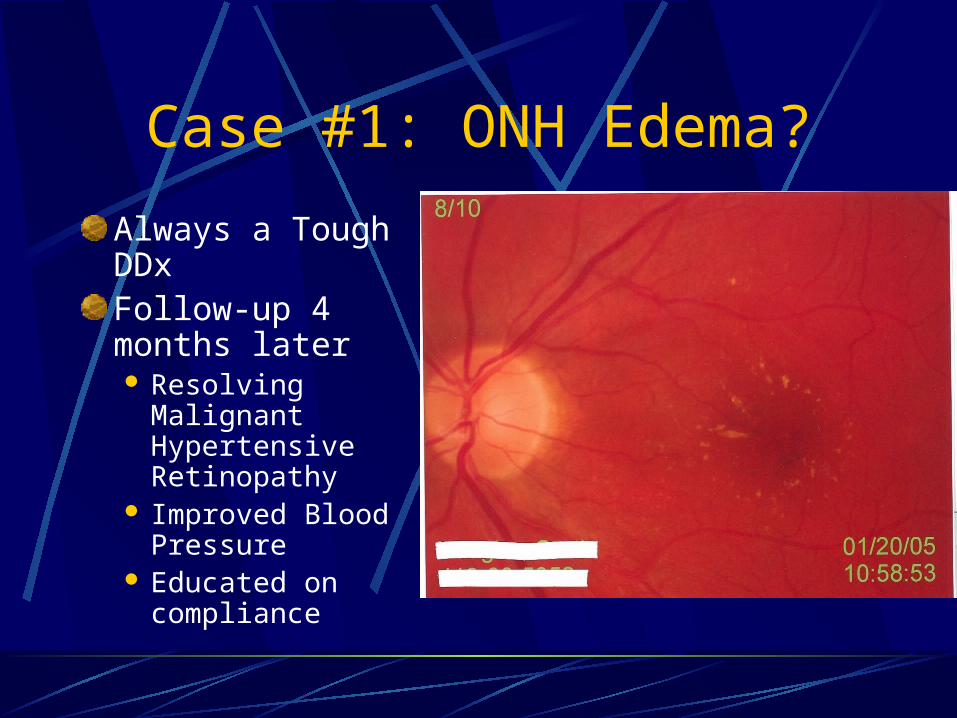
Always a Tough DDxFollow-up 4 months laterBVA OS: 20/20BP: 160/85DFE OS: exudative
macular star, healthy ONH (.2/.2), normal peripheral retina
Case #1: ONH Edema?
Always a Tough DDxFollow-up 4 months later Resolving
Malignant Hypertensive Retinopathy
Improved Blood Pressure
Educated on compliance
Case #1: ONH Edema?
Always a Tough DDx
Bottom LinesPrimary Care OD’s need to take BP’s
Especially on those with retinal vascular disease
Consider typically bilateral retinal conditions
In monocular patients
Case #1: ONH Edema?
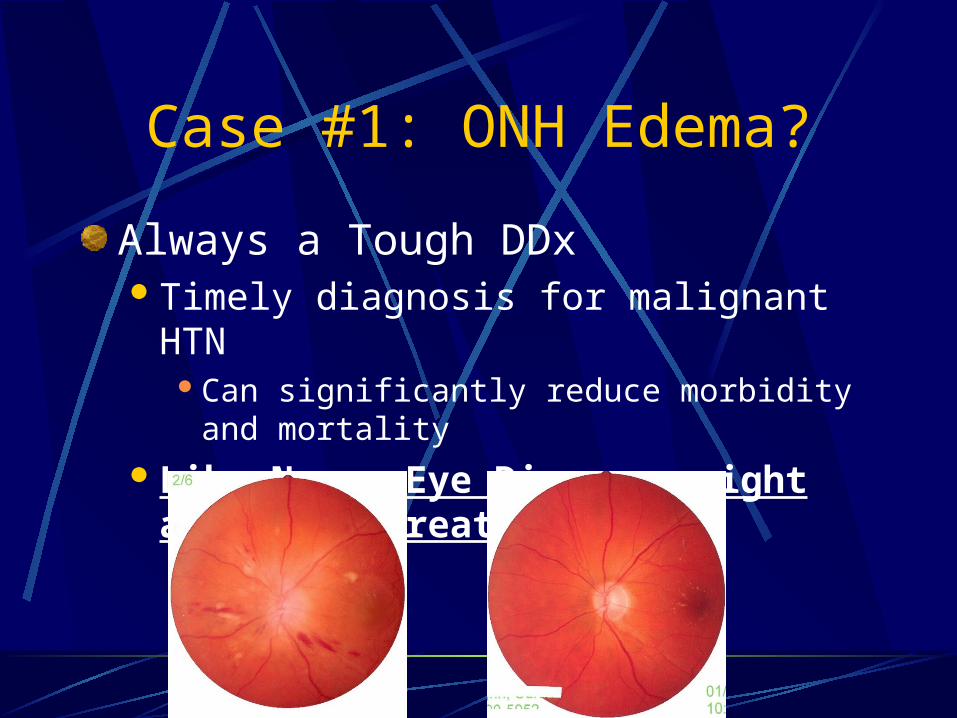
Always a Tough DDxTimely diagnosis for malignant HTN
Can significantly reduce morbidity and mortalityLike Neuro-Eye Disease: sight and life
threatening
Pseudotumor Cerebrii (PTC)
Background “false brain tumor” Increased intracranial pressure
without an intracranial mass Major diagnosis of exclusion: a
true intracranial tumor All patients with papilledema must
have neuro-imaging studies
PTC: Why?
Poor CSF absorption By meninges surrounding brain
and spinal cord Increased intra-abdominal
pressure From obesity elevated intrathoracic pressure decreased venous drainage from
the brain
PTC: Diagnosis
Who? Obese women of childbearing
age Secondary
Obstruction to venous drainage: cerebral venous thrombosis
Exongenous agents: tetracycline, vitamin A, corticosteroids, BCP’s
Medical conditons: lupus, sarcoidosis, anemias, blood dyscrasias
PTC: Diagnosis
Symptoms Bad HA’s: frontal, around the
eyes, pressure-like, throbbing Transient visual loss Intracranial noises: heartbeat or
whooshing sound in ears, tinnitus Vision loss: blur, temporal VF
defect
PTC: Diagnosis
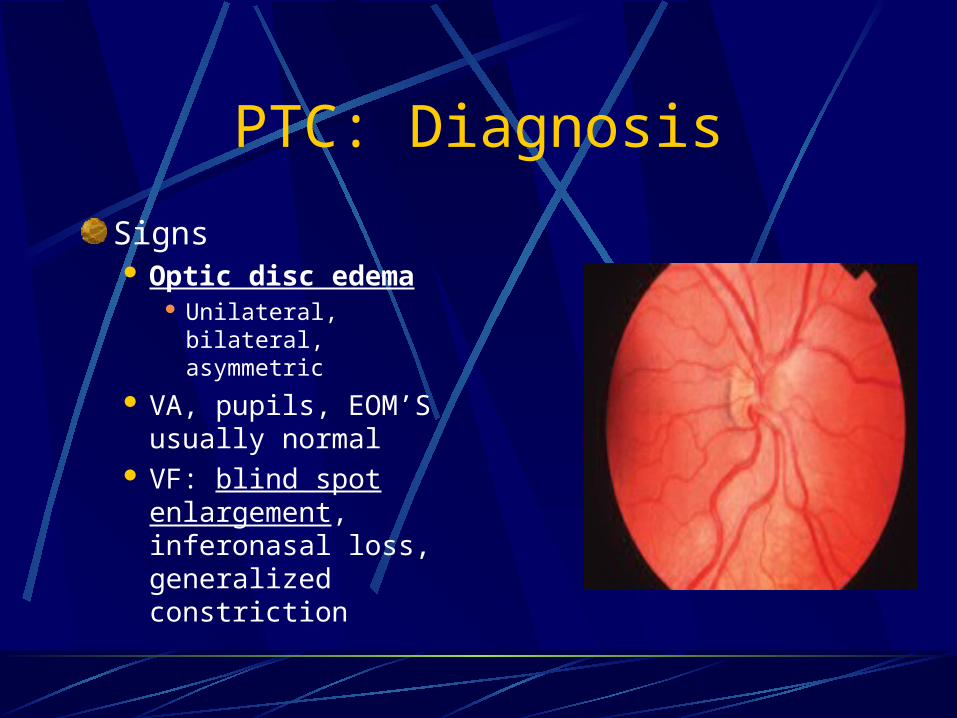
Signs Optic disc edema
Unilateral, bilateral, asymmetric
VA, pupils, EOM’S usually normal
VF: blind spot enlargement, inferonasal loss, generalized constriction
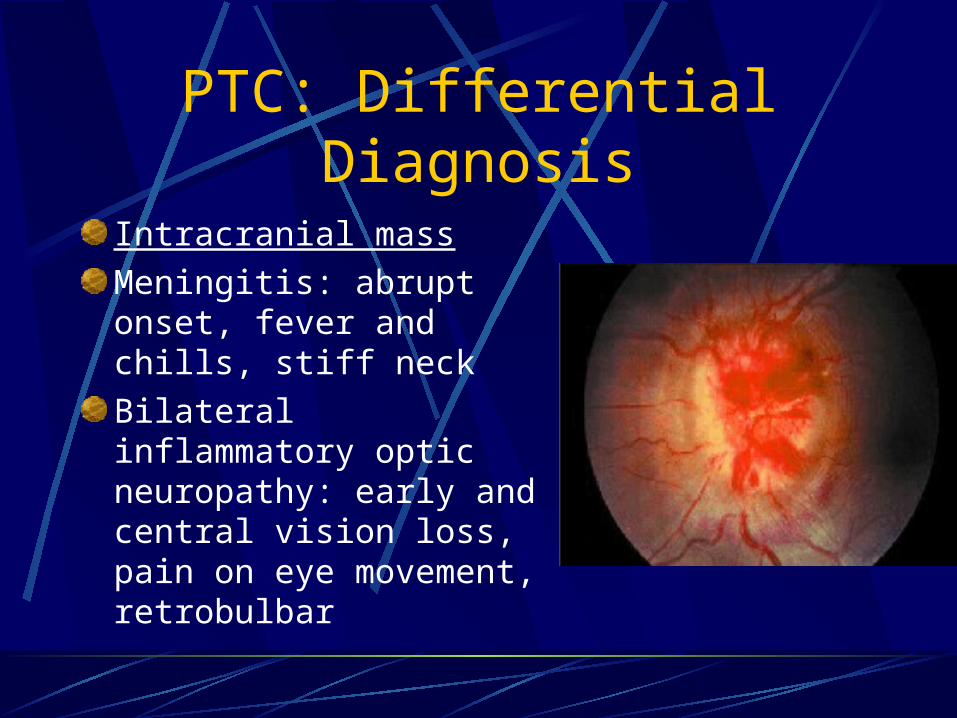
PTC: Differential Diagnosis
Intracranial mass
Meningitis: abrupt onset, fever and chills, stiff neck
Bilateral inflammatory optic neuropathy: early and central vision loss, pain on eye movement, retrobulbar
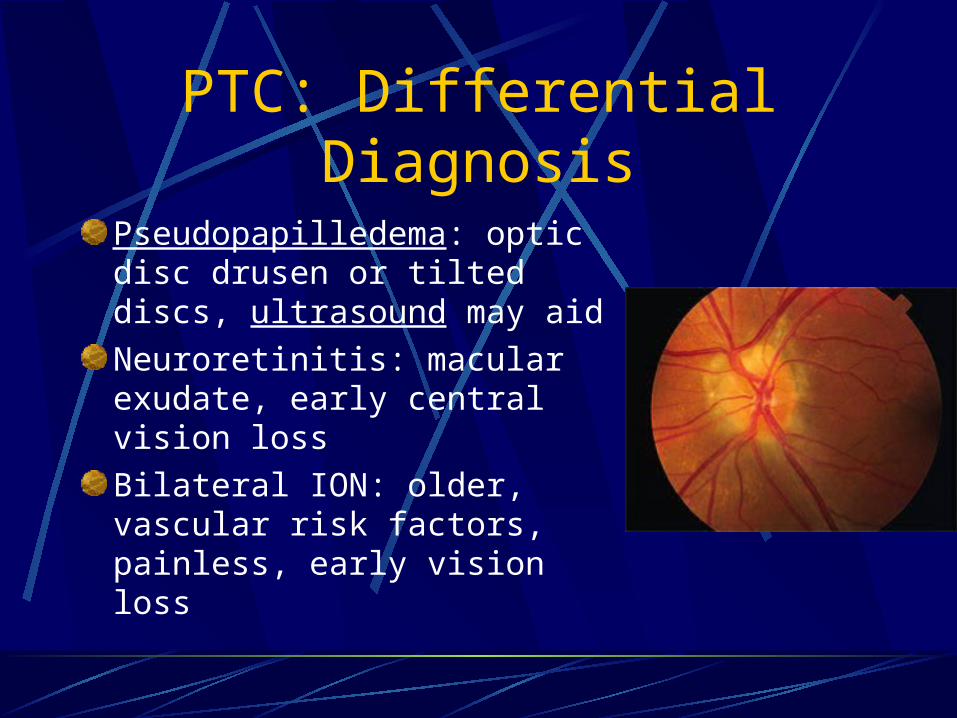
PTC: Differential Diagnosis
Pseudopapilledema: optic disc drusen or tilted discs, ultrasound may aid
Neuroretinitis: macular exudate, early central vision loss
Bilateral ION: older, vascular risk factors, painless, early vision loss
PTC: Ancillary Tests
Optometric In-Office:VF B scan ultrasoundPhotos or optic nerve
imaging
PTC: Ancillary Tests
Neurologist or neuro-eye doc referralNeuroimaging before lumbar puncture
Standard MRI of the brainCT scan with contrast if patient markedly obese
Neuroimaging
Major Scans Used To Evaluate Neuro-Eye DiseaseCT (Computerized tomography)MRI (Magnetic Resonance Imaging)
Neuroimaging
CTGood to view bony abnormalities,
calcifications, acute hemorrhagesValuable to diagnosis of orbital processesTest of choice for thyroid eye disease
Neuroimaging
MRIFar better at characterizing soft tissuesPreferable for most intracranial processesNot subject to bone artifactContrast media and special studies can
sharpenGadolinium is a contrast material that can
increase signal intensity
PTC: Ancillary Tests
Lumbar Puncture Required for the diagnosis of
PTC Neurologist, radiologist or ER
physician Usually > 200 mm
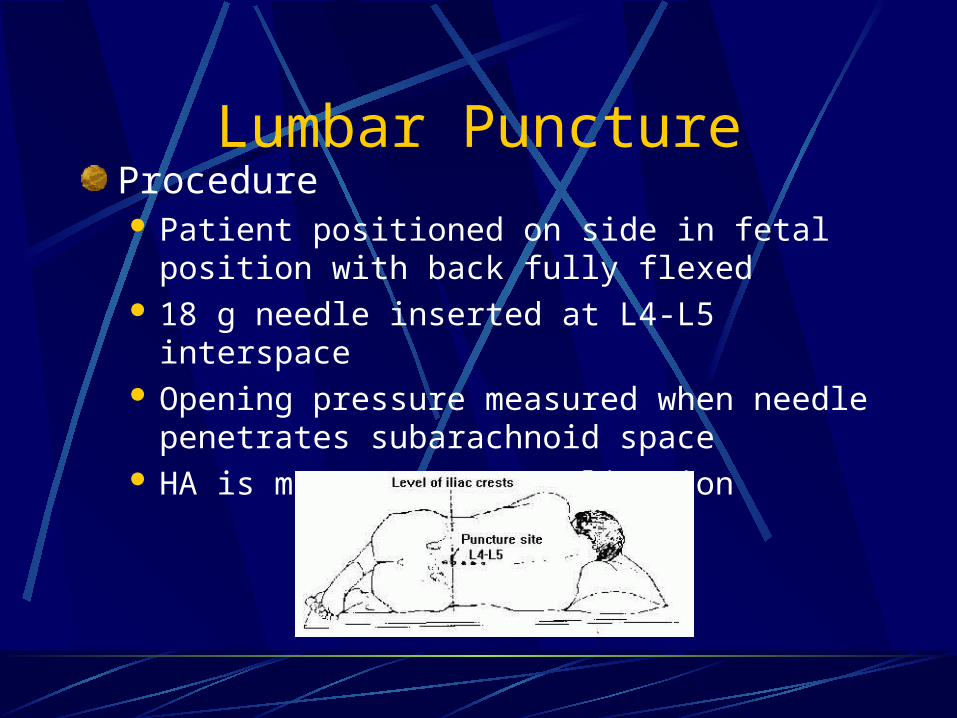
Lumbar PunctureProcedure Patient positioned on side in fetal position with
back fully flexed 18 g needle inserted at L4-L5 interspace Opening pressure measured when needle
penetrates subarachnoid space HA is most common complication
Lumbar Puncture
Opening pressureNormal: 60-80 mm of H20Borderline elevated: 180-210 mm of H20
Lumbar Puncture
CSF evaluationColor
Clear and colorless is normalCloudy: infectionXanthochromic (yellow): subarachnoid
hemorrhageCell count and differential, cytology,
chemical analysis, serologic analysis, microscopy, culture
PTC: Management
“Comanage” with neurologist Initial LP improved signs and sxsVF, DFE, photos or optic nerve imaging
every month x 3 monthsEvery 2-3 months thereafter for about a
year Individual case variability
PTC: Management
“Comanage” with neurologistOther options for some persistent signs
and sxsCAI’s : acetazolamideOther diureticsWeight lossHA management
PTC: Management
Diamox Not just for angle closure Decreased CSF production up to
50% 1-3 grams qd
500 mg bid, tid, qid
Side effects: taste alteration, nausea, fatigue, diarrhea, tingling
Not with sulfa allergies, kidney disease
PTC: Management
Headache management Topamax (topiramate)
Migraine prophylaxis and epilepsy
PTC: HA relief and mild inhibition of carbonic anhydrase, also causes weight loss
Recently: development of angle closure glaucoma from choroidal expansion
PTC: Management
For signs and symptoms unresponsive to LP, severe vision lossCorticosteroidsSurgery
Optic nerve sheath fenestrationCSF diversion (shunt)
PTC: My Clinical Experience
Relatively rare condition? Not at SCO
“Comanagement” turns into MANAGEMENT Optometrists take the time Need to be familiar with ancillary
diagnostic tests and treatment options
Case #2: Monocular Acute Vision Loss In A Golden
GirlS:85 yo Caucasian femaleCx: acute vision loss OD2 weeks earlier
EaracheSore temporal veinsJaw claudication
Past medical hx: non-contributory
Case #2: Golden Girl
O:BVA
LP OD, 20/30 OS+APD ODBP: 150/100No carotid bruitsSLX: NS consistent with 20/30 VA
Case #2: Golden Girl
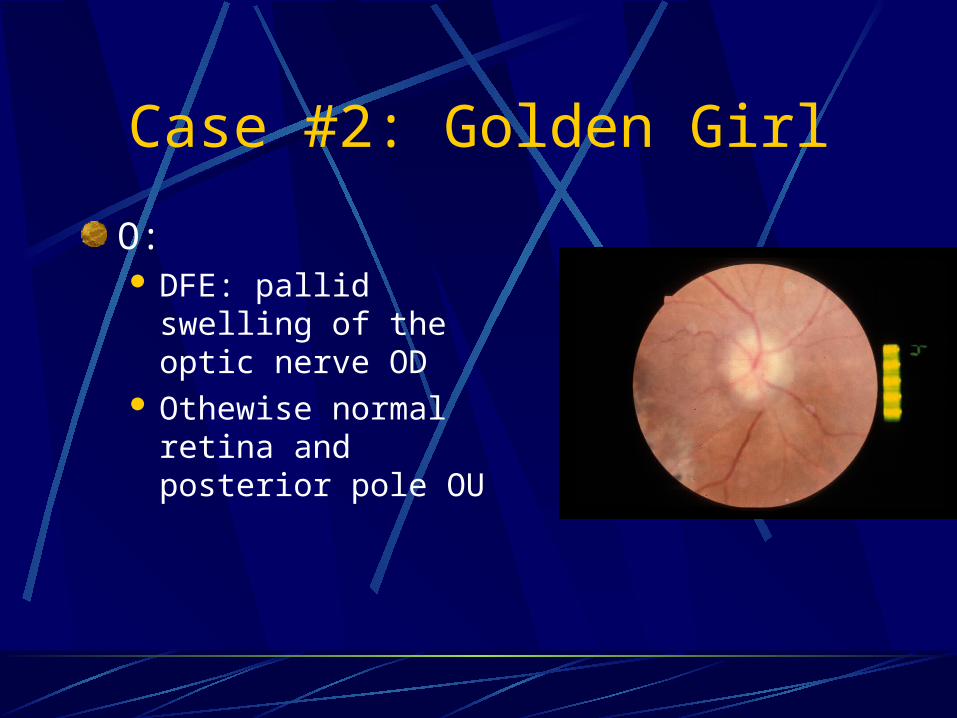
O: DFE: pallid swelling of the
optic nerve OD Othewise normal retina
and posterior pole OU

Case #2: Golden Girl
A: Provisional Diagnosis: Giant Cell
Arteritis OD
P: FLAN:
increased arterial filling time OD Choroidal nonfilling defect OD
80 mg Prednisone po daily
Case #2: Golden Girl
P: R/O all causes of Anterior Ischemic Optic NeuropathyCBC:
Elevated monocyte and platelet countsESR: 44FTA-ABS and VDRL non-reactive
Case #2: Golden Girl
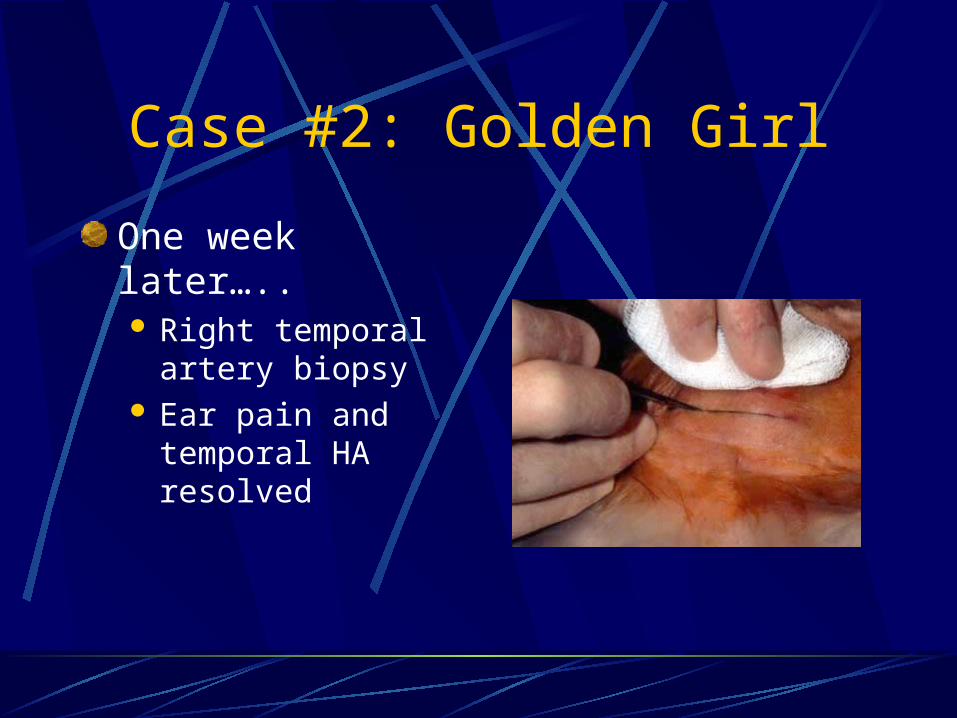
One week later….. Right temporal artery
biopsy Ear pain and
temporal HA resolved
Case #2: Golden Girl
Two weeks later…..ESR: 4Plan:
Monitor with ESRAnd for prednisone side effects
Case #2: Golden Girl
Eventually…..VA did not improve OD
But remained stable OS
Anterior Ischemic Optic Neuropathy (AION)
ArteriticOr…..
Giant Cell ArteritisNomenclature following vision loss
Temporal Arteritis
AION-artertic
BackgroundGranualomatous vasculitis of medium-
sized arteries “True” ocular emergencyThe Goal: Prevention of contralateral vision
loss
AION-arteritic
BackgroundContralateral vision loss
2/3 if untreatedWithin weeks if untreated
AION-arteritic
Why
Granulomatous vasculitis of temporal artery Occlusion of short posterior ciliary arteries (supply anterior optic nerve) AION-artertic
AION-arteritic
Diagnosis: Who?Rose Nylen on the Golden GirlsAverage age of onset = 70 yearsFemale and ScandanavianLower incidence rates
Tennessee & Israel
AION-arteritic
Diagnosis: symptomsUnilateral decreased VA,
temporal HA, scalp tenderness
VA usually < 20/200Amaurosis fugaxAnorexia, fever, malaise,
depressionOnset is variable
AION-arteritic
Clinical FeaturesVasculitis of coronary arteries: MI, CHF,
angina pectorisNeurologic: peripheral neuropathies,
ischemic brain damagePolymyalgia Rheumatica: pain and
stiffness of the neck, shoulders, hips

AION-arteritic
Diagnosis: signs AION-arteritic
Optic nerve edema, hemes, cotton wool spots
APD VF defects: central, altitudinal, arcuate
AION-arteritic
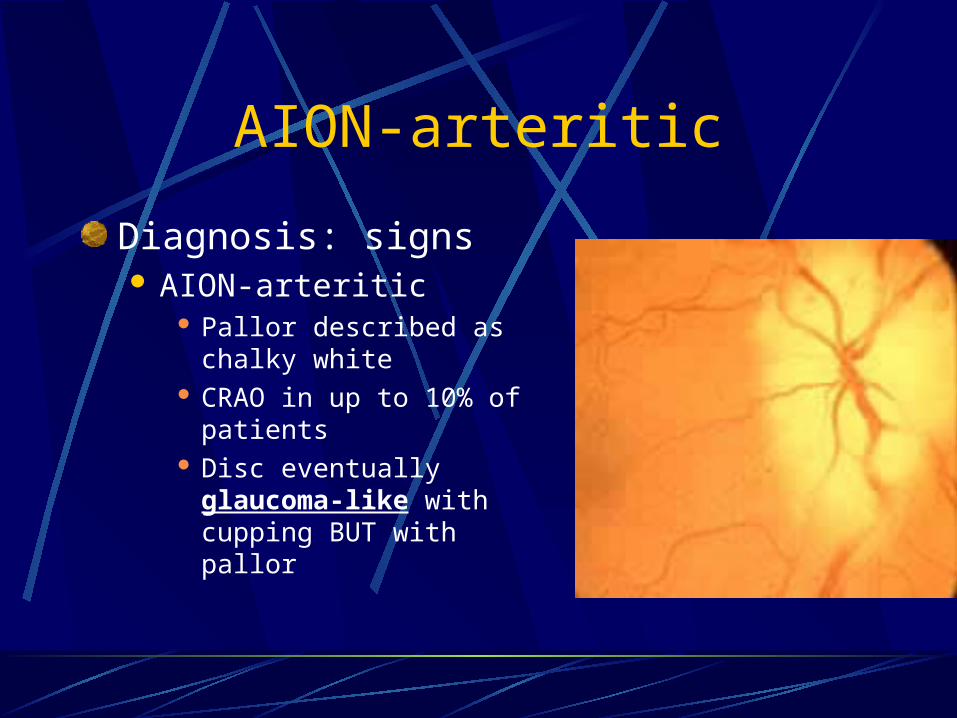
Diagnosis: signs AION-arteritic
Pallor described as chalky white
CRAO in up to 10% of patients Disc eventually glaucoma-
like with cupping BUT with pallor
AION-arteritic
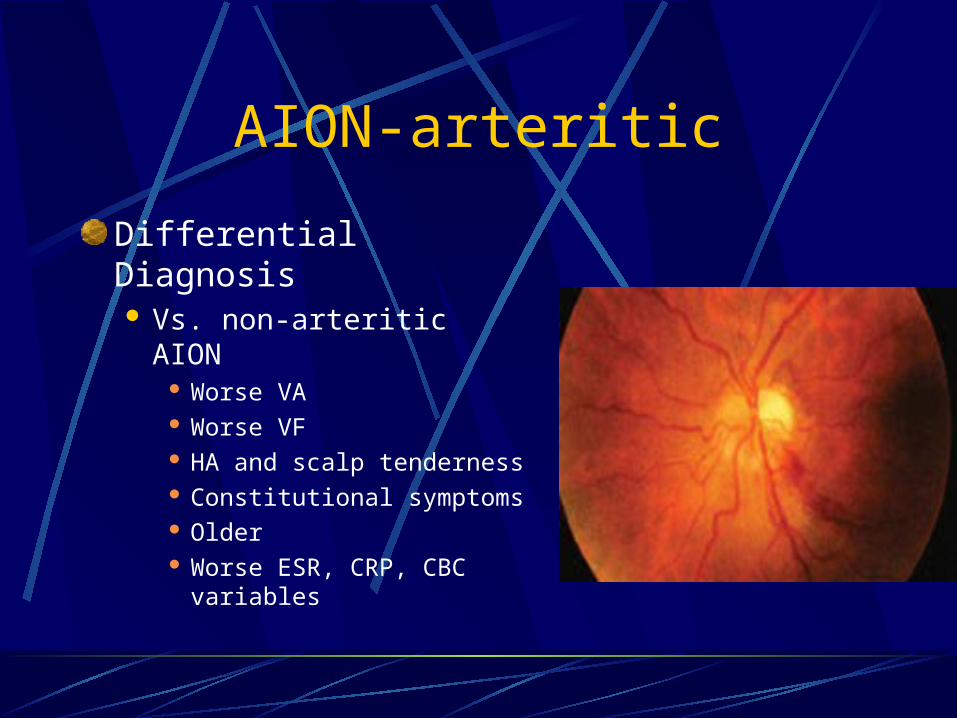
Differential Diagnosis Vs. non-arteritic AION
Worse VA Worse VF HA and scalp tenderness Constitutional symptoms Older Worse ESR, CRP, CBC
variables
AION-arteritic
Ancillary TestsOptometric In-Office
VFOptic nerve imagingPhotosFLAN considered to check for
choroidal perfusion defects
AION-arteritic
Ancillary TestsReferral
ESR (erythrocyte sedimentation rate) Westergren 15% of GCA patients: normal ESR
CRP (C-reactive protein) Elevated in > 91%
Also elevated WBC, platelet counts; IgG anticardiolipin antibodies
AION-arteritic
Ancillary Tests Referral
Temporal artery biopsy Should be performed on all
suspects > 95% sensitive, 100% specific Can be done shortly after
steroid treatment Inflammatory cells in the
muscular walls of the artery
AION-arteritic
Diagnosis: Summary History and clinical
impression ESR and CRP Confirm with
temporal artery biopsy
AION-arteritic
ManagementReferral: neurologist, internist (PCP),
rheumatologistFor suspects or diagnosed:
Systemic steroids
AION-arteritic
ManagementSystemic steroids
Hospital admission1-2 gm IV methylprednisone x 2-3 days 60-100 mg of oral prednisone: tapered very
slowly
AION-arteritic
Management
Systemic steroidsAnecdotal vision recovery?Poor prognosis?No solid support for anti-steroid medications
(Rheumatrex aka methotrexate)
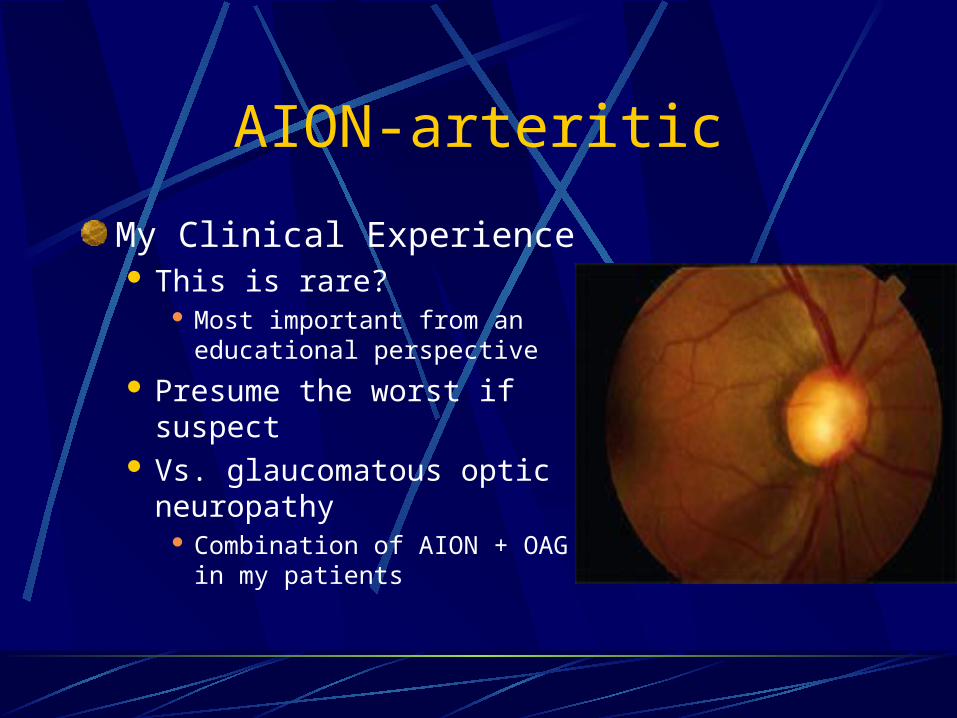
AION-arteritic
My Clinical Experience This is rare?
Most important from an educational perspective
Presume the worst if suspect Vs. glaucomatous optic
neuropathy Combination of AION + OAG in
my patients