
Clinical Aspects of Deep Tissue Pressure Injury · Carolina WOC Nurses: A Descriptive Study."...
33
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org Clinical Aspects of Deep Tissue Pressure Injury Janet Cuddigan, PhD, RN, CWCN, FAAN Associate Professor University of Nebraska Medical Center [email protected]
Transcript of Clinical Aspects of Deep Tissue Pressure Injury · Carolina WOC Nurses: A Descriptive Study."...
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org
Clinical Aspects of Deep Tissue Pressure InjuryJanet Cuddigan, PhD, RN, CWCN, FAANAssociate ProfessorUniversity of Nebraska Medical [email protected]

Disclosures and Disclaimers
National Pressure Ulcer Advisory Panel Board of Directors
International Pressure Ulcer Guideline Development Group
Pressure Ulcer Consultant to NDNQI, Press Ganey (university subcontract)
Paid External Consultations:Elderly Health Promotion, IncHill-Rom

Objectives
1. Identify clinical manifestations and management of pressure and tissue deformation in Deep Tissue Pressure Injury (DTPI).
2. Discuss the results of available clinical research on DTPI.
3. Discuss implications of basic science and clinical research findings on patient care and future research.
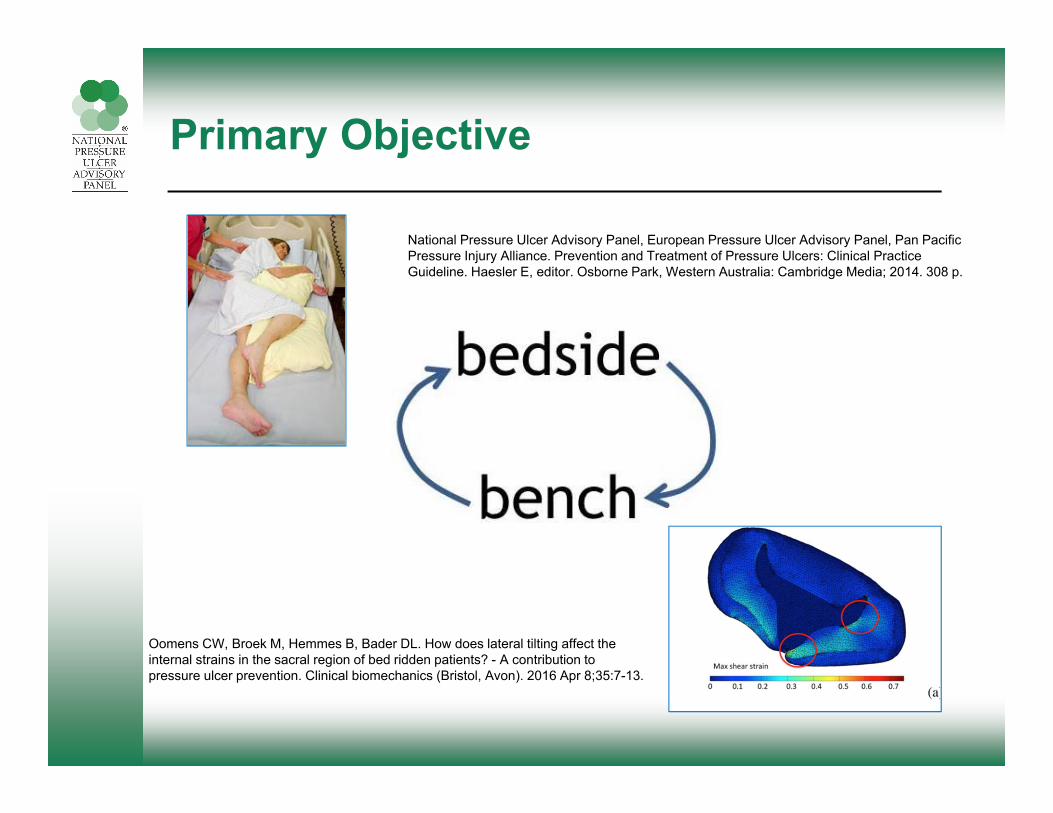
Primary Objective
Oomens CW, Broek M, Hemmes B, Bader DL. How does lateral tilting affect the internal strains in the sacral region of bed ridden patients? - A contribution to pressure ulcer prevention. Clinical biomechanics (Bristol, Avon). 2016 Apr 8;35:7-13.
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Haesler E, editor. Osborne Park, Western Australia: Cambridge Media; 2014. 308 p.

History of DTPI
• Ulcers could erupt from intact skin (Paget, 1874)
• May be purple or yellow from extravasation of blood. The deeper tissues die, muscles, bones. Sloughing follows in the skin and fat and the place is empty (Paget, 1874)
• Ulcers that started in muscle were malignant (Groth, 1942)
• Closed pressure ulcers (Shea, 1975)• 2007 NPUAP Staging System
……albeit with difficulty after much prolonged debate. (Smart, 2013)

Deep Tissue Pressure Injury: Persistent non-blanchable deep red, maroon or purple discoloration (NPUAP Slide Set 2016)
Intact or non-intact skin with localized area of persistent non-blanchable deep red, maroon, purple discoloration or epidermal separation revealing a dark wound bed or blood filled blister. Pain and temperature change often precede skin color changes. Discoloration may appear differently in darkly pigmented skin. This injury results from intense and/or prolonged pressure and shear forces at the bone-muscle interface.
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org

Deep Tissue Pressure Injury – continued(NPUAP Slide Set 2016)
• The wound may evolve rapidly to reveal the actual extent of tissue injury, or may resolve without tissue loss.
• If necrotic tissue, subcutaneous tissue, granulation tissue, fascia, muscle or other underlying structures are visible, this indicates a full thickness pressure injury (Unstageable, Stage 3 or Stage 4).
• Do not use DTPI to describe vascular, traumatic, neuropathic, or dermatologic conditions.
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org7

Evolution of Deep Tissue Pressure Injury(NPUAP Slide Set 2016)
• Day 1 - Classify intact, discolored skin this pressure as a Deep Tissue Pressure Injury
• Day 3 - Classify discolored skin with epidermal blistering as a Deep Tissue Pressure Injury
• Day 10 - If the Deep Tissue Pressure Injury becomes necrotic, classify it as an Unstageable Pressure Injury
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org8
Day 1 - DTPI Day 3 - DTPI Day 10 - Unstageable

Evolution of DTPI in darkly pigmented skin(NPUAP Slide Set 2016)
Due to the thickness of the skin, the epidermal separation will remain intact for a longer period of time. This phase can be mistaken for skin tears.
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org

DTPI Definition – continued(NPUAP Slide Set 2016)
Do not use Deep Tissue Pressure Injury to describe vascular, traumatic, neuropathic, or dermatologic conditions.
Traumatic Bruising
Vasopressor Ischemia Coumadin
Necrosis
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org
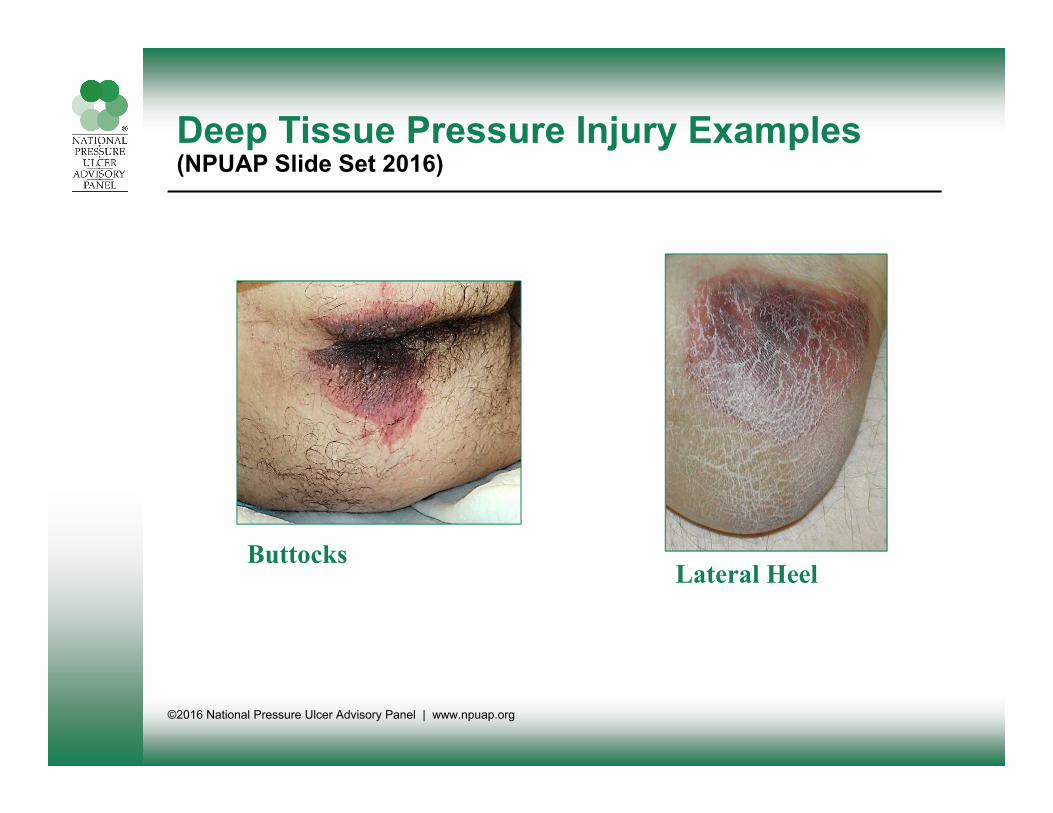
Deep Tissue Pressure Injury Examples(NPUAP Slide Set 2016)
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org
ButtocksLateral Heel

Basic Science Summary
Methods• MRI• Mathematical Modeling • Animal Studies• Cell Cultures• Biochemical Assays
Comparisons• Skin vs. Fat vs. Muscle vs.
Scar• Heel vs. Sacrum• Different surfaces, dressings• Variations in intensity and
duration of pressure-shear• Intermittent vs. continuous• Relative contributions of:
– tissue deformation– ischemia
• Role of reperfusion injuryXiao, 2014

Basic Science: Etiology of DTPI
1. Tissue Deformation2. Ischemia3. Ischemia Reperfusion Injury(Oomens, et al., 2015)

Clinical Aspects: Epidemiology
• Prevalence– 9-12% of pressure injuries in national studies– 1-2% of patients affected
• Risk Factors– Older– More acutely ill– Critical care and surgical units– Immobility– History of a precipitating event approximately 24-72
hours before DTPI discovery– Risk profile similar to other pressure injuries
VanGilder, et al., 2010; Black, et al., 2015; Bergquist-Beringer, et al., 2013;

Clinical Aspects: Epidemiology
• Precipitating Event– “Intense and/or prolonged pressure and shear force”– “Found down on hard surface”– Long OR or procedure time– Immobility– Periods of poor perfusion – Transfer
• Anatomic Distribution– Heels (29-41%)– Sacrum (19-40%)– Buttocks (7-13%)
X
XX

DTPI Evolution

Time between event and purple skin
• Black, et al., 2015– 24-72 hours
• Honaker, et al., 2014– Range: 1-5 days– Mean: 2.4 days
• Farid, et al., 2007– 7 days

18
Evolving DTPI
Early presentation of purple-maroon tissue at 48 hrs
Blister phase at 72-96 hours
Necrotic phase at 7 days
Slide courtesy of Dr. Joyce Black

Buttocks DTPI from being flat are more on the tissues of buttocks
Slide courtesy of Dr. Joyce Black
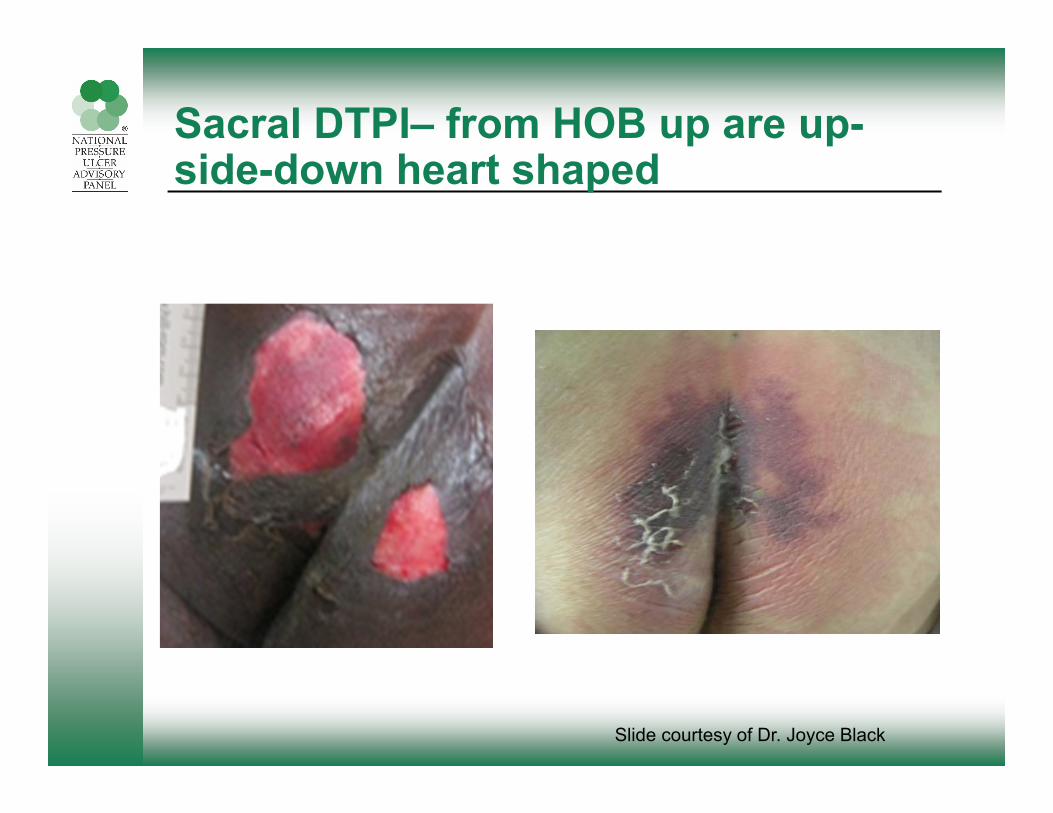
Sacral DTPI– from HOB up are up-side-down heart shaped
Slide courtesy of Dr. Joyce Black
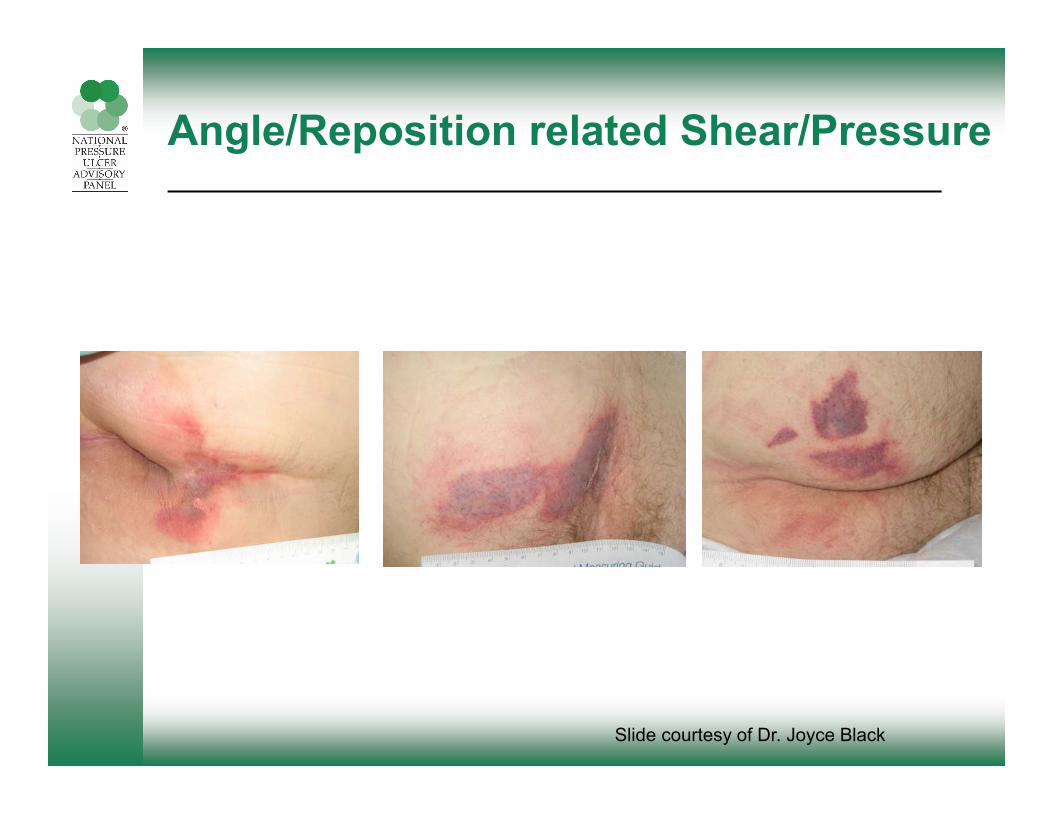
Angle/Reposition related Shear/Pressure
Slide courtesy of Dr. Joyce Black
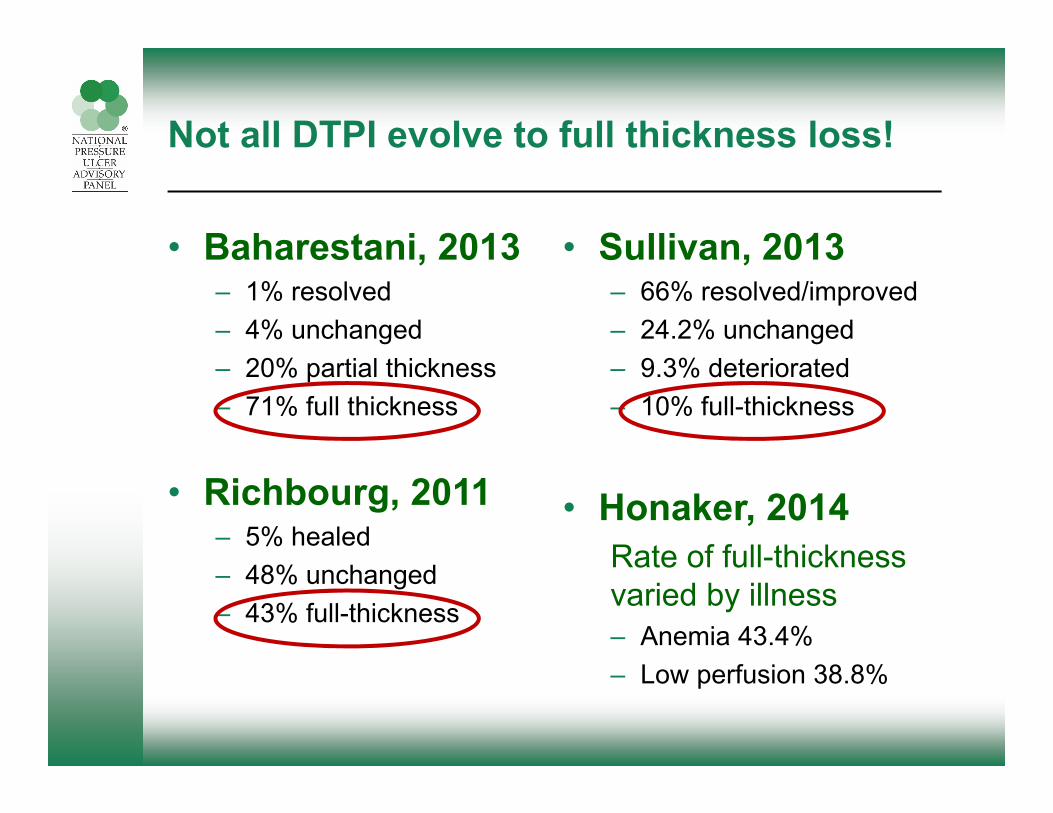
Not all DTPI evolve to full thickness loss!
• Baharestani, 2013– 1% resolved– 4% unchanged– 20% partial thickness– 71% full thickness
• Richbourg, 2011– 5% healed– 48% unchanged– 43% full-thickness
• Sullivan, 2013– 66% resolved/improved– 24.2% unchanged– 9.3% deteriorated– 10% full-thickness
• Honaker, 2014Rate of full-thickness varied by illness– Anemia 43.4%– Low perfusion 38.8%
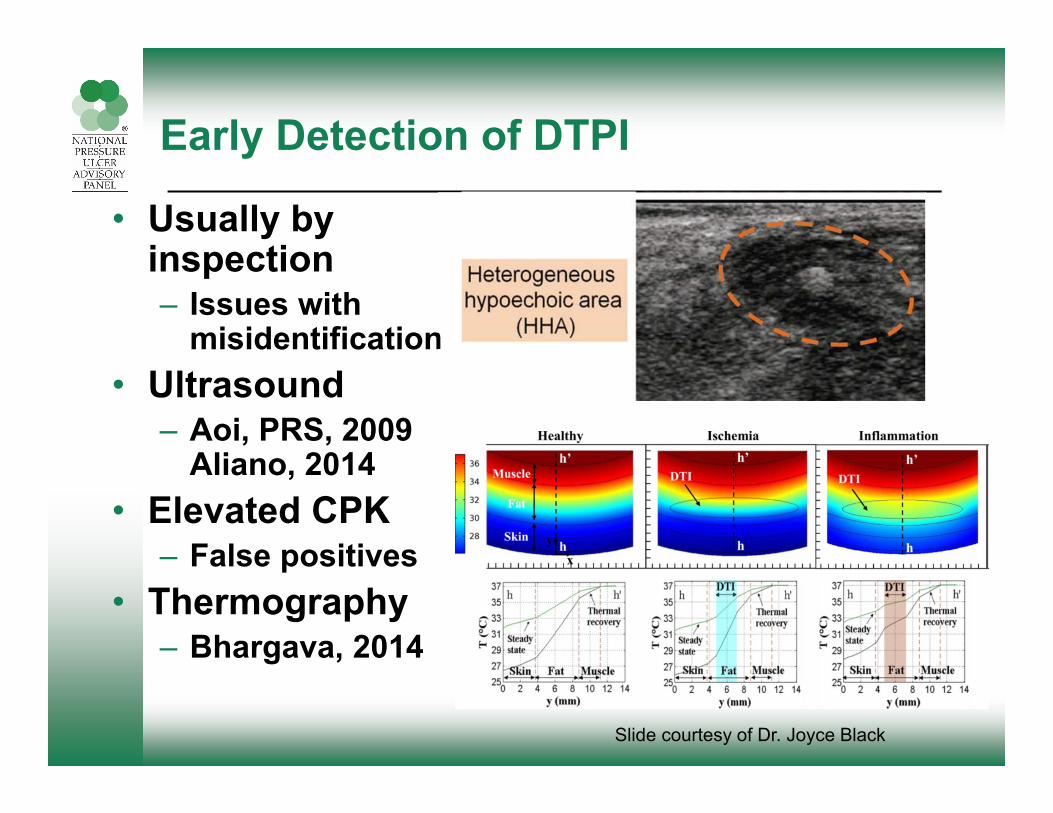
Early Detection of DTPI
• Usually by inspection– Issues with
misidentification• Ultrasound
– Aoi, PRS, 2009Aliano, 2014
• Elevated CPK– False positives
• Thermography– Bhargava, 2014
Slide courtesy of Dr. Joyce Black

Prevention & Treatment
• Relieve pressure completely!– Turn– KEEP OFF!– Support surfaces– Elevate heels – boots
• Maintain perfusion• Maintain nutrition
• Currently under study:– Prophylactic dressing– Non contact low
frequency ultrasound– Electrical stimulation

Healed with Total Offloading
July 15 July 25 July 28
Photo series courtesy of Dr. Denis Drennan
88 year old female with multiple comorbities. Hip fracture on July 1st. 5 x 5 cm blister on July 11th admission to rehabilitation. TOTAL 24/7 offloading.

Healed with Total Offloading
Gradual demarcation
August 10
Fully demarcated
Eschar –16 cm2
August 17
Dry borders, no pain
August 25
Photo series courtesy of Dr. Denis Drennan

Healed with Total Offloading
Shrinking eschar
September 9
Edges of eschar
loosening9 cm
September 22
Small crust
September 29
Photo series courtesy of Dr. Denis Drennan

October 6th

Documentation
• Note time and nature of precipitating event(s).• What was the patient’s position? On what
surface?• Precise descriptions of tissue changes will help
establish time frame.• Name it: Deep Tissue Pressure Injury.• Note natural history and possible outcome.• What measures are you taking to recover
whatever tissue may still be viable?

With Deep Tissue Pressure Injury…..

References
• Ahmetovic, A., V. K. Mushahwar, R. Sommer, D. Schnepf, L. Kawasaki, R. Warwaruk-Rogers, T. Barlott, S. L. Chong, G. Isaacson, S. Kim, M. Ferguson-Pell, R. B. Stein, C. Ho, S. Dukelow and K. M. Chan (2015). "Safety and Feasibility of Intermittent Electrical Stimulation for the Prevention of Deep Tissue Injury." Adv Wound Care (New Rochelle) 4(3): 192-201.
• Ahn, H., L. Cowan, C. Garvan, D. Lyon and J. Stechmiller (2016). "Risk Factors for Pressure Ulcers Including Suspected Deep Tissue Injury in Nursing Home Facility Residents: Analysis of National Minimum Data Set 3.0." Adv Skin Wound Care 29(4): 178-190.
• Baharestani, M. M. (2013). Natural history of suspected deep tissue injuries from clinical manifestation to outcome. 2013 NPUAP Biennial Conference. DTI: The State of the Science. Houston, TX.
• Bergquist-Beringer, S., L. Dong, J. He and N. Dunton (2013). "Pressure ulcers and prevention among acute care hospitals in the United States." Joint Commission Journal on Quality and Patient Safety39(9): 404-414.
• Bhargava, A., A. Chanmugam and C. Herman (2014). "Heat transfer model for deep tissue injury: a step towards an early thermographic diagnostic capability." Diagnostic Pathology 9(1): 36-36.
• Black, J. M., C. T. Brindle and J. S. Honaker (2015). "Differential diagnosis of suspected deep tissue injury." Int Wound J.
• Edsberg, L. E., Black, J. M., M. Goldberg, L. McNichol, L. Moore and M. Sieggreen (2016). "Revised National Pressure Ulcer Advisory Panel Pressure Injury Staging System." J Wound Ostomy Continence Nurs 43(6): 1-13.
• Farid, K. J., C. Winkelman, A. Rizkala and K. Jones (2012). "Using temperature of pressure-related intact discolored areas of skin to detect deep tissue injury: an observational, retrospective, correlational study." Ostomy Wound Manage 58(8): 20-31.

References
• Gefen, A., K. J. Farid and I. Shaywitz (2013). "A review of deep tissue injury development, detection, and prevention: shear savvy." Ostomy Wound Management 59(2): 26-35.
• Higashino, T., G. Nakagami, T. Kadono, Y. Ogawa, S. Iizaka, H. Koyanagi, S. Sasaki, N. Haga and H. Sanada (2014). "Combination of thermographic and ultrasonographic assessments for early detection of deep tissue injury." International Wound Journal 11(5): 509-516.
• Honaker, J., D. Brockopp and K. Moe (2014). "Suspected deep tissue injury profile: a pilot study." AdvSkin Wound Care 27(3): 133-140; quiz 141-132.
• Honaker, J. S., M. R. Forston, E. A. Davis, M. M. Weisner, J. A. Morgan and E. Sacca (2016). "The Effect of Adjunctive Non-Contact Low Frequency Ultrasound on Deep Tissue Pressure Injury." Wound Repair Regen.
• Honaker, J. S., M. R. Forston, E. A. Davis, M. M. Wiesner and J. A. Morgan (2013). "Effects of non contact low-frequency ultrasound on healing of suspected deep tissue injury: A retrospective analysis." International Wound Journal 10(1): 65-72.
• National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014). Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Osborne Park, Western Australia, Cambridge Media.
• Oomens, C. W., D. L. Bader, S. Loerakker and F. Baaijens (2015). "Pressure induced deep tissue injury explained." Ann Biomed Eng 43(2): 297-305.
• Oomens, C. W., M. Broek, B. Hemmes and D. L. Bader (2016). "How does lateral tilting affect the internal strains in the sacral region of bed ridden patients? - A contribution to pressure ulcer prevention." Clin Biomech (Bristol, Avon) 35: 7-13.

References
• Richbourg, L., J. Smith and S. Dunzweiler (2011). "Suspected Deep Tissue Injury Evaluated by North Carolina WOC Nurses: A Descriptive Study." Journal of Wound, Ostomy, and Continence Nursing: Official Publication of the Wound, Ostomy and Continence Nurses Society / WOCN 38(6): 655-660.
• Sullivan, R. (2013). "A Two-year Retrospective Review of Suspected Deep Tissue Injury Evolution in Adult Acute Care Patients." Ostomy Wound Manage 59(9): 30-39.
• Vangilder, C., G. D. Macfarlane, P. Harrison, C. Lachenbruch and S. Meyer (2010). "The demographics of suspected deep tissue injury in the United States: an analysis of the international pressure ulcer prevalence survey 2006-2009." Advances in Skin & Wound Care 23(6): 254-261.
• Xiao, D. Z., S. Y. Wu and A. F. Mak (2014). "Accumulation of loading damage and unloading reperfusion injury--modeling of the propagation of deep tissue ulcers." J Biomech 47(7): 1658-1664.


















