Personality development in clinical social workers : the ...

2016 ABPP Annua l Confe rence & Workshops Chicago, IL
Sa turday , May 14, 2016
Clinical and Forensic Applications of the Personality Assessment Inventory (PAI)
Presented by
Mark A. Ruiz, PhD, ABPP

1
Mark A. Ruiz, PhD ABPP
James A Haley Veterans’ HospitalUniversity of South Florida
Clinical and Forensic Use of the Personality Assessment Inventory (PAI)
Statement of Conflict of Interest
• Dr. Ruiz does not receive any ongoing financial or material support from the publisher (PAR, Inc.) or the author (Dr. Leslie Morey) of the PAI.
• Copyright permissions were obtained from the PAR, Inc., but they had no input regarding the content of this presentation.
• Dr. Ruiz was a paid consultant for the PAI Interpretive Report for Correctional Settings (PAI‐CS) in 2004‐2005. Dr. Ruiz does not receive royalties from this or any PAI product.
• PAR employee from 2000‐2004
Learning Objectives
• Describe major trends in existing PAI research.• Describe and analyze PAI indicators or profile invalidity. • Identify strengths/weaknesses of the PAI as it pertains to clinical evaluations.
• Analyze and interpret specific PAI score configurations. • Interpret PAI results pertaining to opinions of risk, treatment needs, and responsiveness.
• List the strengths and weaknesses of the PAI when used with racial/ethnic minorities.
• Compare and contrast the PAI with other commonly used measures.
Disclosure for Case Studies• The case studies presented here are fictitious. Any resemblance to an actual case(s) is coincidence and unintended.
• APA Ethical Standard 4.07
• Case studies were developed to illustrate clinical issues encountered in real‐world forensic practice.
• Spirit and intent is to capture clinical complexity.
• Please treat case studies as confidential. • Please do not disseminate profiles/case studies.• Copyright and test security protections.
• PAI profiles were reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc.
2
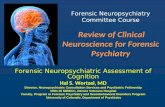
Training Outline• Part 1. Foundation
• Part 2. The Case for Self‐Report Assessment
• Part 3. Evaluation of Response Styles
• Part 4. Evaluation of Risk to Self and Others
• Part 5. Evaluation of Treatment Needs
• Part 6: Evaluation of Treatment ResponsivenessReproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Foundation• Conceptual development (Morey, 1991)
– Emphasis on content validity– Non‐overlapping scales– Rational and empirical development process
• Primary normative samples– Standardization Sample (N = 1,000)
• 85% Caucasian, 48% male, 84% > high school education, 72% between 18‐49 yo.
– Clinical Sample (N = 1,265)• 79% Caucasian, 61% male, 80% > high school education, 86% 18‐49 yo.
– Corrections sample (N = 1,155)• 38% White/Caucasian, 68% male • Education M =11 (SD 3), M age 33.6 (SD 8.9).
Sample
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..

3
Sample
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
T-score
30
40
50
60
70
80
90
100
110T-score
30
40
50
60
70
80
90
100
110
Scale ICN INF NIM PIM SOM ANX ARD DEP MAN PAR SCZ BOR ANT ALC DRG AGG SUI STR NON RXR DOM WRMRaw 6 2 7 12 45 47 34 42 14 26 23 30 7 0 0 3 15 9 7 9 6 14
PAI T 52 47 70 43 84 79 67 79 40 59 62 62 43 41 42 36 74 57 56 40 24 33Corr. T 48 41 61 45 82 73 59 70 38 50 56 52 33 40 33 36 76 47 51 50 20 33
Corr.G. T 47 41 62 44 84 76 62 73 38 51 57 53 33 39 34 36 76 48 52 48 18 34% Complete 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
ICN
INF
NIM
PIM
SOM
ANX
ARD
DEP
MAN
PAR
SCZ BOR
ANTALC
DRG
AGG
SUI
STR
NON
RXR
WRM
PAI Community Norms (N = 1,000) Correctional Norms (N = 1,155) Correctional Norms (Gender)
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Item Content• Items written to capture phenomenology & experience
• Item section• Empirical, Logical/rational, Psychometric
• Expert sorts were conducted during development• Bias review panel• PAI‐A appropriate to adolescents.
• Multiple choice response options
• Readability• Developed at 4th‐grade reading level.
• Mean 8.2 words per item
• Schinka & Borum (1993)• Clinical scales‐ average 4th grade reading level• Validity scales‐ average 5th grade reading level
• Most phrases and vocabulary at 6th grade level.• Recommended 5th‐6th grade completion (regular classes, passing grades)
Response Styles (Rogers, 2008)
Overstated Pathology
Simulated Adjustment Disengaged
NIM MAL RDF ICN INFPIM DEF CDF ?Crit.
4
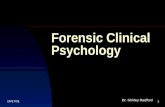
Psychopathology
Internalizing Externalizing Thought Disorder
SOM PAR SCZALC/DRG ANT AGGDEP ANX ARD MAN
SUI/SPI
VPI
Personality
Personality Disorder
InterpersonalBehavior
DOMBOR ANT PAR WRM
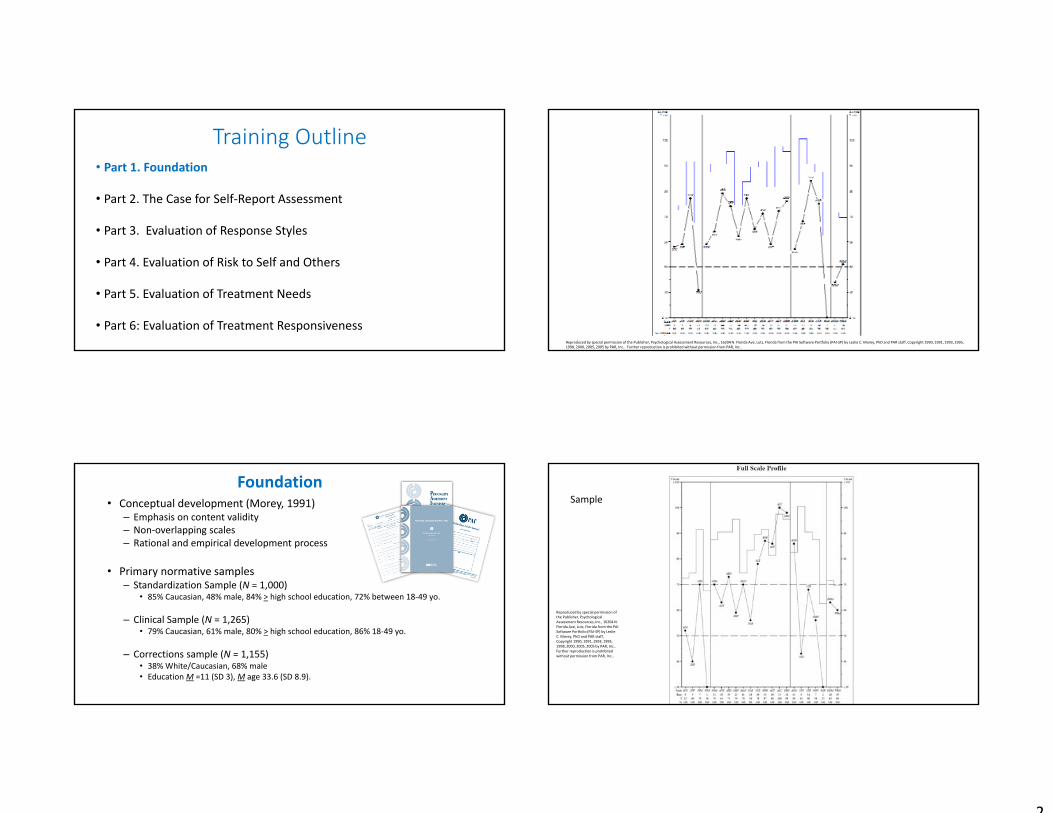
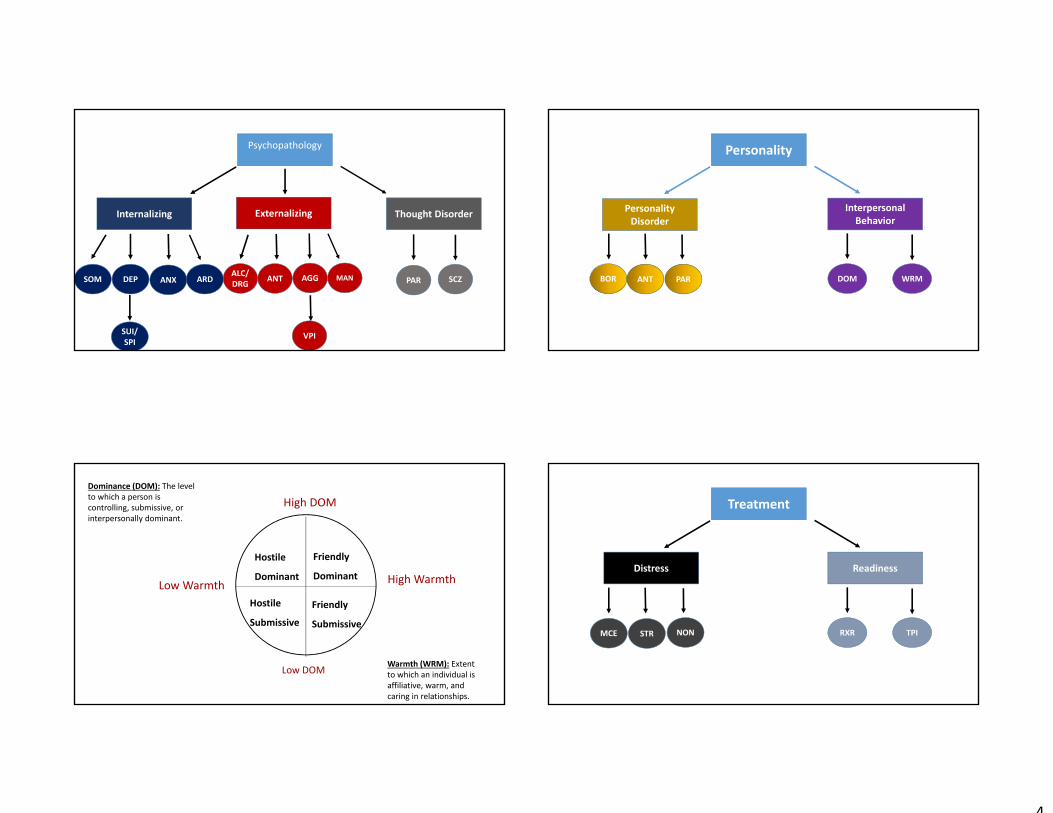
High DOM
Hostile
Dominant
Hostile
Submissive
Friendly
Dominant
Friendly
Submissive
Low Warmth
Low DOM
High Warmth
Dominance (DOM): The level to which a person is controlling, submissive, or interpersonally dominant.
Warmth (WRM): Extent to which an individual is affiliative, warm, and caring in relationships.
Treatment
Distress Readiness
RXRMCE STR NON TPI

5
Training Outline• Part 1. Conceptual Overview
• Part 2. The Case for Self‐Report Assessment
• Part 3. Evaluation of Response Styles
• Part 4. Evaluation of Risk to Self and Others
• Part 5. Evaluation of Treatment Needs
• Part 6: Evaluation of Treatment Responsiveness
Ethical GuidanceAPA Ethical Guidelines & Code of Conduct
• 9.01 Bases for Assessments• Base opinions on information and techniques sufficient to establish the findings.• Provide opinions only after conducting an examination of the individual adequate to support findings.• Explain the sources of information on which conclusions are based. • Use instruments that whose reliability and validity have been established for the population tested.• Use methods that are appropriate to the individual’s language preference.
American Psychological Association (2013)Specialty Guidelines‐Forensic Psychologists
• 9.02. Use of Multiple sources of information • Forensic clinicians avoid relying on one source of data and corroborate important data whenever feasible.
• 10.02 Selection & Use of Assessment Procedures• Forensic practitioners make known that examination results can be affected by factors unique to the forensic context (e.g., response style, situational stress).
American Psychological Association (2002, amended 2010)
Limitations of Rating Instruments• Lack of “field validity” (Murrie et al., 2009)
– N = 333 male offenders undergoing SVP evaluation– PCL scores not valid predictors of sexual re‐offending
• Subset of prolific evaluators did have more valid PCL scores
• Case law review (DeMatteo et al., 2014)– Poor reliability between state/defense experts
• Often greater than 1 SEM• Dichotomous judgments based on PCL‐SV (kappa =. 29).
• Complex judgments require increased specificity– “reasonably good match” “flavor and intent”– Adversarial Allegiance = problem
PCL Total Scores After Experimental Manipulation
0
5
10
15
20
25
30
Case 1 Case 2 Case 3 Case 4
Prosecution Defense
Murrie, Boccaccini, Guarner, & Rufino (2013). Are Forensic Experts Biased by the Side that Retained Them? Psychological Science, 24, 1889‐1897
28‐33% of opposing evaluator pairs had differences >2 SEM

6
Known or Potential Error RatesScale PAI α
(K = 8)PAI-A α
(Clinical)
Negative Impression Management (NIM) .60 .77Positive Impression Management (PIM) .73 .77
Somatic Complaints (SOM) .85 .86Anxiety (ANX) .88 .89Anxiety-Related Disorders (ARD) .79 .73Depression (DEP) .85 .88Mania (MAN) .80 .78Paranoia (PAR) .81 .81Schizophrenia (SCZ) .81 .85Borderline Features (BOR) .85 .87Antisocial Features (ANT) .77 .82Alcohol Problems (ALC) .76 .84Drug Problems (DRG) .73 .85
Scale PAI (K = 8)
PAI-A(clinical)
Aggression (AGG) .83 .89Suicidal Ideation (SUI) .83 .90Stress (STR) .70 .73Nonsupport (NON) .74 .72Treatment Rejection (RXR) .65 .76
Dominance (DOM) .69 .63Warmth (WRM) .75 .73
Standard Operation of the PAI
PAI
Spanish Language Version
PAR Iconnect
PAI Short‐Form
PAI Adolescent
Audio Version
Personality Assessment Inventory‐Adolescent (PAI‐A)
Fewer items than PAI – 264 items versus 344.
Designed for adolescents 12 to 18 years of age. Large community and clinical samples.
PAI items were selected for the PAI‐A based on whether the item retained its original meaning when read by adolescents.
Main strength – Same structure as the PAI.
Main weaknesses – Not developmentally specific; not well‐researched.
7
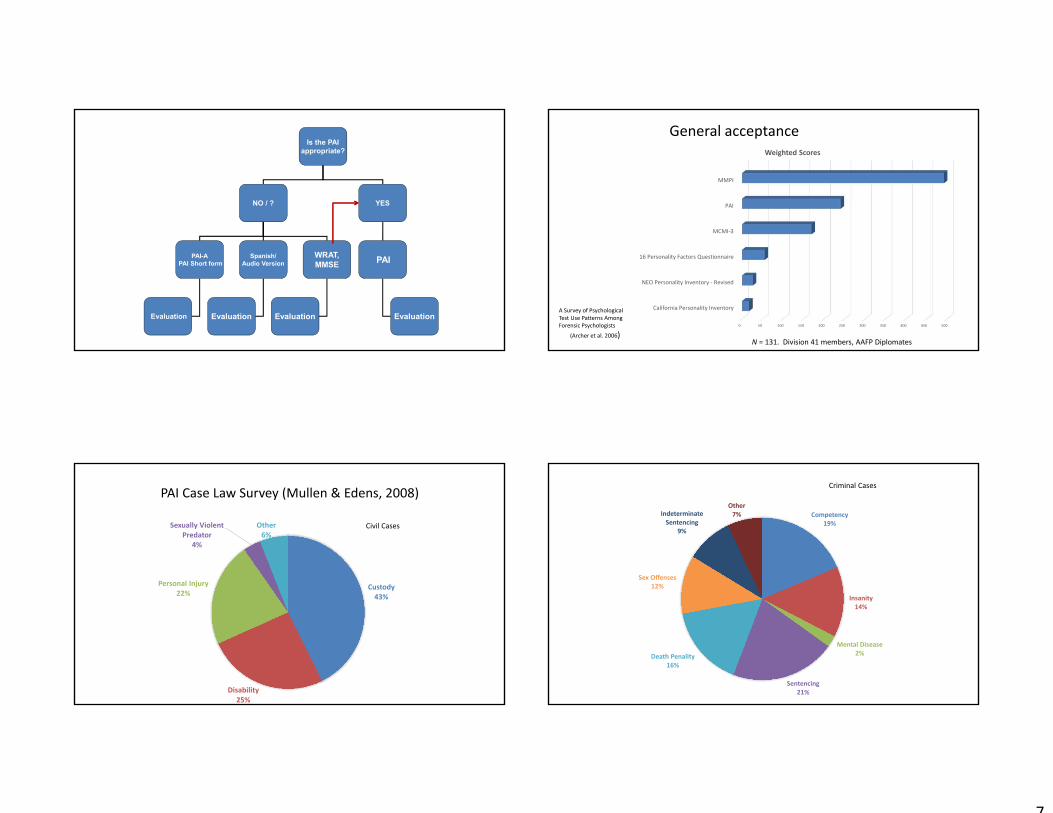
Is the PAIappropriate?
NO / ? YES
PAI-APAI Short form
Spanish/Audio Version PAI
Evaluation
WRAT,MMSE
EvaluationEvaluation Evaluation0 50 100 150 200 250 300 350 400 450 500
California Personality Inventory
NEO Personality Inventory ‐ Revised
16 Personality Factors Questionnaire
MCMI‐3
PAI
MMPI
Weighted Scores
N = 131. Division 41 members, AAFP Diplomates
A Survey of Psychological Test Use Patterns Among Forensic Psychologists
(Archer et al. 2006)
General acceptance
PAI Case Law Survey (Mullen & Edens, 2008)
Custody43%
Disability25%
Personal Injury22%
Sexually Violent Predator
4%
Other6%
Civil CasesCompetency
19%
Insanity14%
Mental Disease2%
Sentencing21%
Death Penality16%
Sex Offenses12%
Indeterminate Sentencing
9%
Other7%
Criminal Cases

8
Training Outline• Part 1. Conceptual Overview
• Part 2. The Case for Self‐Report Assessment
• Part 3. Evaluation of Response Styles
• Part 4. Evaluation of Risk to Self and Others
• Part 5. Evaluation of Treatment Needs
• Part 6: Evaluation of Treatment Responsiveness
Inconsistency (ICN)
• Empirically derived scale that measures the consistency in which a respondent completed items with similar content. – Composed of 10‐item pairs; five which are generally answered
similarly and five which are opposite in meaning.• Item pairs differ in content so that ICN total score is not generally
associated with one disorder.
ICN ICN‐C
Inconsistency‐Corrections Index
(<5% positive)
ICN Interpretation
T-score Interpretative significance
< 64T Respondent answered items consistently. Appropriate attention to item content.
64T-72T Moderate level of inconsistency in responses. May be due to carelessness, confusion, or disorganized attempts at impression management. Interpretive hypotheses must be made with caution.
>73T Significant inconsistency in responses. Individual did not answer items consistently or did not appropriately attend to the item content. Completely random PAI protocols would result in scores at this range. No clinical interpretation is recommended.
Infrequency (INF)• Measures the tendency to respond to items in an atypical
manner. Item content is unusual, but not necessarily bizarre. – Items were selected on the basis of very low endorsement frequencies
in both the Census‐matched community sample AND the Clinical normative sample.
INF

9
INF Interpretation
T-score Interpretative significance
< 60T Individual attended appropriately to item content. Did not answer in grossly atypical ways.
60T-74T Some degree of atypical or unusual responding. Interpretive hypotheses must be made with caution.
>75T Significant degree of atypical or unusual responding. No interpretive hypotheses are recommended.
Identification of Random Responding
(Morey, 2007) Identification rates (%)
Community Clinical Total RandomICN > 64T or INF >71T 13% 21% 99%ICN >64T & INF > 71T 3% 2% 77%
ICN > 73T or INF >75T 6% 7% 94%ICN >73T & INF >75T .2% .2% 43%
2‐3% of individuals in corrections settings had ICN or INF >80T (Ruiz, Poythress, Lilienfeld, Douglas, 2008).
Problem with partial random responding
Clark, Gironda, & Young (2003)
SensitivityBack Random
Responding (BRR) Level
50 100 150 200 250 300 All
ICN > 73T .03 .13 .13 .21 .45 .44 .53
INF > 75T .02 .07 .32 .46 .66 .74 .85
ICN or INF .05 .19 .41 .57 .82 .86 .94
Siefert et al. (2007)
Sensitivity
Specificity BRR‐50 BRR‐100 BRR‐150 BRR‐200
SUI Dif > 5T .65 .65 .79 .82 .91
ALC Dif > 5T .74 .52 .81 .87 .84
Both .88 .32 .65 .72 .77
Negative Impression Management (NIM)
• Measures the extent to which the respondent is presenting an overly negative impression.– Items assess an exaggerated unfavorable presentation. Individual reports bizarre and unlikely symptoms.
• Items were selected, in part, on low endorsement frequencies.
NIM

10
NIM Interpretation
T-score Interpretative significance
< 73T Few indicators of negative response distortion in the protocol.
73T-83T Moderate exaggeration of complaints and problems. Some degree of unlikely/bizarre symptom reporting.
>84T Presentation of an extremely negative distortion. Endorsement of unlikely/bizarre symptoms is evident. May be a “cry for help.” Deliberate distortion is very possible. NIM > 92 = No clinical interpretation.
Malingering Index (MAL)
• Eight indicators that commonly appear in PAI profiles of simulators instructed to feign mental illness.
• Presence of each feature is summed to obtain total score (0‐8)– MAL = 3 (84T)‐ Questions of malingering
– MAL = 5 (111T) – Likely malingering
1.if NIM >= 110T2.if NIM ‐ INF >= 20T3.if INF ‐ ICN >= 154.if (PAR‐P – PAR‐H >= 15) 5.if (PAR‐P – PAR‐R >=15) 6.if (MAN‐I – MAN‐G >=15)7.if (DEP >=85) and (RXR >= 45)8.if (ANT‐E – ANT‐A >= 10)
Rogers Discriminant Function (RDF)
• Weighted combination of 20 PAI scales designed to discriminate simulated profiles from those of legitimate patients (Rogers et al., 1996)– RDF 60T‐ Possible feigning.– RDF 70T – Overt attempt to malinger.– Debates regarding its utility, mostly in relation to poor correspondence to the SIRS (Rogers, Bagby, & Dickens, 1992)
• Does not include NIM.
Effortful/Deliberate Non‐effortful
NIMRDF MAL
MAL RDFNIM .61 .09DEP .40 .18SCZ .51 .16
N = 447. Morey (1996).

11
Detection of Over‐reporting(Hawes & Boccaccini, 2009)
NIM MAL RDF
d k d k d k
Uncoached 1.48 23 1.15 19 1.13 15
Coached 1.59 8 1.00 6 1.65 3
• Larger effects found for simulation studies when compared to criterion groups.
• Larger effects for detecting severe mental illness.• Best overall classification: NIM > 81T; MAL >84T • MMPI‐2 Effect sizes comparing simulators versus genuine patients
(Rogers et al., 2003) : • F scale: d = 2.21• Fp scale: d = 1.90
Clinical Opinion – Weight of the Evidence
Clinical History
Testing Results
Conceptual coherence
Case 1: Amenability to treatment• Referral Question‐ Mental health evaluation for sentencing mitigation and
amenability to drug offender probation and treatment.
• Charge(s): Felony drug possession, Violation of probation (prior drug offense).
• Demographics: Female, single, never married. No children. No high school diploma or GED, school behavior problems. Unemployed.
• Clinical interview highlights: Gang affiliations, possible involvement in gang‐related drug trafficking. Somewhat disengaged from interview.
• Limited history of outpatient counseling‐ no psychiatric medications.
WASI‐II
• FSIQ‐4 = 109 IQ
TCU Drug Screen II
• Elevated impairment • Drug of choice‐opiates, marijuana, alcohol (to lesser extent)
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 1

12
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Positive Impression Management (PIM)
• Measures the level at which a respondent is presenting an overly favorable impression and a denial of problems/symptoms. – Items selected from individuals asked to provide positive impression response sets.
• Items ask respondent to acknowledge relatively minor personal faults.
PIM
PIM InterpretationT-score Interpretative significance
< 44T Individual appears to have answered the items in a candid manner. He/she is not holding back.
44T-56T Individual did not attempt to present self in an overly favorable light. Scores in this range are unusual in clinical settings.
57T-67T Some degree of positive response distortion. Individual has denied common faults that most people acknowledge. Interpretations should be made with caution.
>68T Significant positive response distortion. Respondent portrays him/herself in an unrealistically positive manner. Individual is saying that he/she is free from common flaws that most people admit. No clinical interpretation.
Evaluating Parenting CapacityCarr, Moretti, & Cue (2005)
MMPI-2 L MMPI-2 F MMPI-2 K
PAI PIM .66*** -.50* .73***
PAI NIM -.28 .34 -.72***
n = 28
• Mothers and fathers undergoing parental capacity evaluations.
•Approximately 20% (N = 51) of participants had an invalid PAI protocol.
• Approximately 49% of the sample had an invalid MMPI‐2 profile.
• 64% of participants who had an invalid MMPI‐2 profile had a valid PAI profile.

13
PAI profiles in child custody evaluations
30
40
50
60
70
80
90T SC
ORE
S
PAI SCALE SCORES
Defensiveness Index (DEF)• Eight configural features that appear more commonly in PAI profiles of simulators instructed to “fake good” than in profiles of non‐clinical & clinical samples (Morey, 1996)
• Presence of each feature is summed to obtain total score – 0‐9 (one item double‐weighted)– DEF 70T (raw = 6) = possible defensiveness.
Cashel Discriminant Function (CDF)
• Used college students and jail inmates instructed to “fake good” to construct discriminant function equation of PAI scales that differentiated these from “honest” profiles (Cashel et al., 1995)– Minimal overlap with PIM– Modest correlation with DEF
DEF CDFPIM .56 .06DEP ‐.47 .11SCZ ‐.37 .17
N = 447. Morey (1996).
PIM‐Predicted Scores (Morey & Hopwood, 2007)
• Deviation scores ‐ Technique for quantifying the level of “leakage” in the profile.
• Attempts to untangle the contribution of under‐reporting.
Lack of Insight
Defensive‐ness
True Score
Positive Response Distortion
14
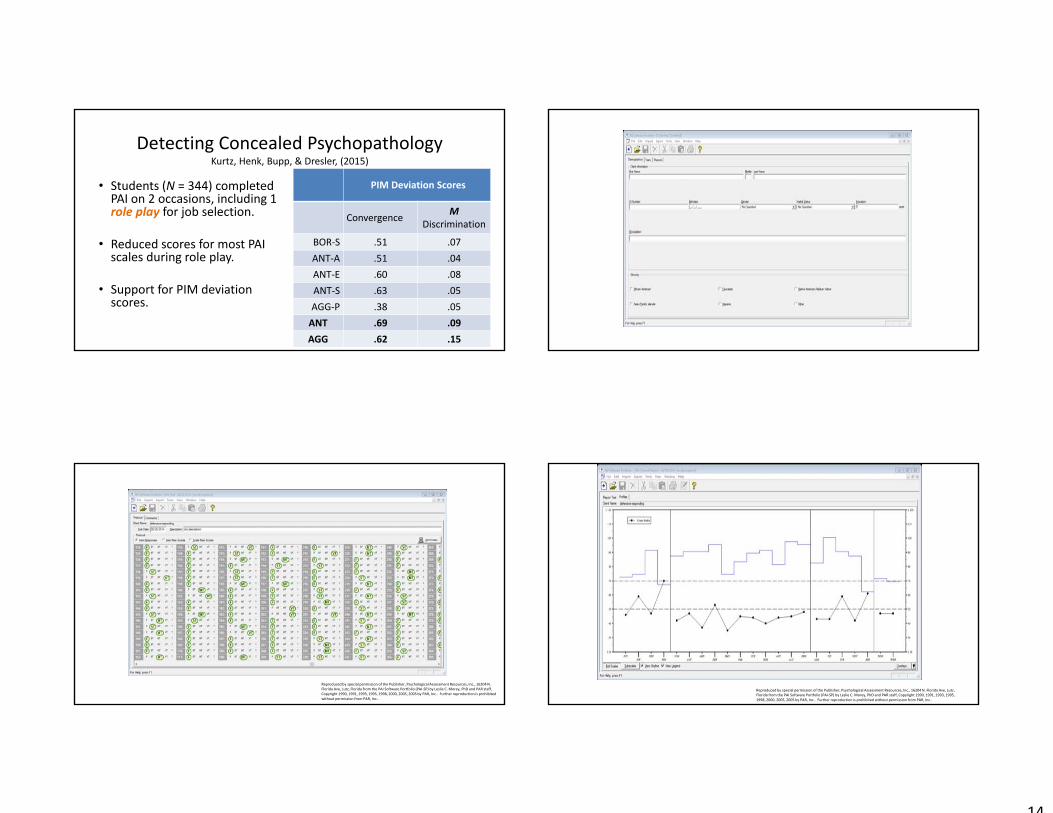
Detecting Concealed PsychopathologyKurtz, Henk, Bupp, & Dresler, (2015)
• Students (N = 344) completed PAI on 2 occasions, including 1 role play for job selection.
• Reduced scores for most PAI scales during role play.
• Support for PIM deviation scores.
PIM Deviation Scores
Convergence M Discrimination
BOR‐S .51 .07ANT‐A .51 .04ANT‐E .60 .08ANT‐S .63 .05AGG‐P .38 .05ANT .69 .09AGG .62 .15
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..

15
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
• Referral Question‐ Risk assessment for sexual re‐offending.
• Charge(s): Lewd and Lascivious acts; Distribution of obscene materials via computer.
• Demographics: Male, Married, 4 children, Professional employment.
• Clinical interview highlights: Remorseful. Focused on saving career. No substance abuse. Superficially cooperative, but the impression is that he is not entirely forthcoming about his past.
• Recent psychiatric hospitalization, emotionally distressed at times.
SVR‐20 Risk Factors
• Relationship difficulties• No sexual deviancy.• Adolescent (late) victim• Unrelated, stranger victim.• No use of force.
Case 2
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibitedwithout permission from PAR, Inc..
Case 2

16
Case 2
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Training Outline• Part 1. Conceptual Overview
• Part 2. The Case for Self‐Report Assessment
• Part 3. Evaluation of Response Styles
• Part 4. Evaluation of Risk to Self and Others
• Part 5. Evaluation of Treatment Needs
• Part 6 Evaluation of Treatment Responsiveness
Risk
Needs
Responsive‐ness
Conceptual Model Guiding Evaluation (Andrews & Bonta, 2010)
Antisocial Features (ANT)• Designed to measure personality and behavioral features of antisocial personality/psychopathy– Measures egocentricity/lack of empathy, risk‐taking behavior, and antisocial cognitions and behaviors.
– Well‐validated predictor for offending and violence.
ANT
AntisocialBehaviors
(ant-a)
Egocentricity(ant-e)
Stimulus-Seeking(ant-s)

17
Can the PAI be a proxy for the PCL‐RDouglas, Guy, Edens, Boer, & Hamilton (2007)
PCL‐R
Factor 1
• Sample 1 (n = 205‐214)• ANT = ‐.07• DRG = ‐.01• DOM = .16
• Sample 2 (n = 60‐85)• ANT = .08• DRG = ‐.05• DOM = .35**
Factor 2
• Sample 1• ANT = .42*• DRG = .48*• DOM = .07
• Sample 2• ANT = .49*• DRG = .35*• DOM = .06
PCL‐R
ANT InterpretationT-score Interpretative significance
< 60T Individual reports being interpersonally considerate and warm; moderate control over impulses.
60T – 69T Moderate degree of impulsivity and risk-taking behavior. Others view them as disinhibited and interpersonally cold and callous.
70T-81T Person reports being impulsive and hostile, and is likely to have a history recklessness and/or antisocial behavior. Not likely to have many close friendships.
>82T Prominent features of antisocial personality disorder. Likely to be unreliable, exploitive, and interpersonally callous. Likely to conflict with authority and have prominent impulsivity and aggression.
Aggression (AGG)• Scale designed to assess cognitive and behavioral manifestations of aggression, anger, and hostility. – Taps fundamental aggressive features that are not necessarily specific to any disorder.
AGG
AggressiveAttitude(agg-a)
Verbal Aggression
(agg-v)
PhysicalAggression
(agg-p)
AGG InterpretationT-score Interpretative significance
< 60T Person has a reasonable control over the expression of anger and hostility. Score <40T may suggest an overly meek person.
60T – 69T Person reports being impatient, irritable, and likely to have a short-temper. May experience excessive anger and is easily provoked.
70T-81T Chronically angry person. Likely to express anger without reservation. Subscale elevations point to how anger is expressed (e.g., verbal, physical).
>82T Clinically significant anger and high potential for aggressive behavior. Individual is overtly hostile and easily provoked, and may have history of violent actions. Functional impairment related to aggressive acting out is likely.

18
High DOM
Hostile
Dominant
Hostile
Submissive
Friendly
Dominant
Friendly
Submissive
Low Warmth
Low DOM
High Warmth
Dominance (DOM): The level to which a person is controlling, submissive, or interpersonally dominant.
Warmth (WRM): Extent to which an individual is affiliative, warm, and caring in relationships.
Violence Potential Index (VPI)
• 20 profile characteristics that have been identified in the literature as risk factors for violence. – Sensation‐seeking– Impulsivity– Substance abuse– Dom > Warmth 10T (Hostile Dominance)
• VPI > 87T moderate risk for violence• VPI >121T significant risk for violence.
Mental Health and Substance Use(Ruiz, Cox, Magyar, & Edens, 2014)
• Externalization• Disinhibition, impulsivity,
excitement‐seeking.
• Substance abuse• Damage to brain circuitry
regulating emotions & decision
making.
Primary Source: Goldstein & Volkow (2002). Drug addiction and its underlying neurobiological basis…. American Journal of Psychiatry.
Re‐Offending Rate 4‐5 years after In‐jail Addiction Treatment
General Offending Rate Violent Offense Rate
r β r βANT .19* .25* .23* .31*
ANT‐A .19* .19 .28* .26*ANT‐E .22* .30* .27* .37*ANT‐S .15 .13 .23* .25*
AGG .14 .10 .12 ‐.04AGG‐A .18* .20 .27* .23*AGG‐V .21* .23* .24* .19AGG‐P .14 .13 .17 .06
N = 124.
PAI Sex Offender Specific Studies
Boccaccini et al. (2010) – ANT and AGG predictive of re‐offending in
sex offenders
Boccaccini et al. (2013) – BOR and ANT predict re‐convictions in a small sample of committed
offenders
Caperton et al. (2004) – ANT/AGG predicted institutional misconduct in a small sex offender sample.
19
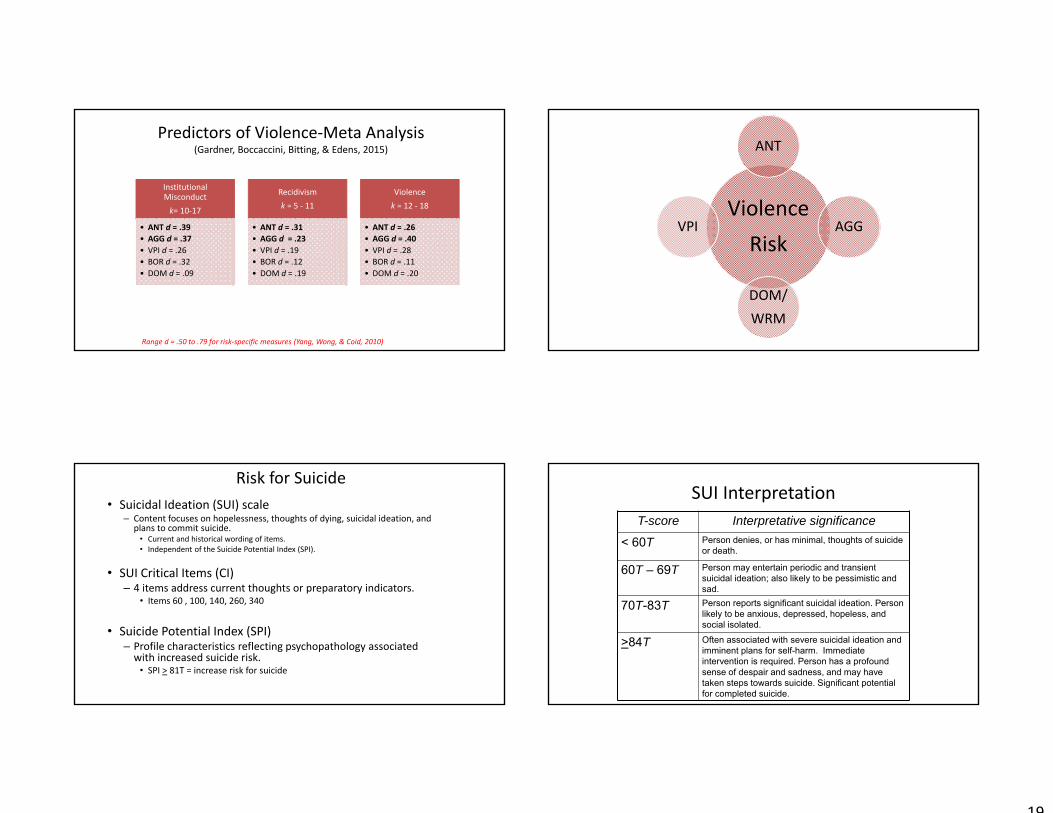
Predictors of Violence‐Meta Analysis(Gardner, Boccaccini, Bitting, & Edens, 2015)
Institutional Misconductk= 10‐17
• ANT d = .39• AGG d = .37 • VPI d = .26• BOR d = .32• DOM d = .09
Recidivismk = 5 ‐ 11
• ANT d = .31• AGG d = .23• VPI d = .19• BOR d = .12• DOM d = .19
Violencek = 12 ‐ 18
• ANT d = .26• AGG d = .40• VPI d = .28• BOR d = .11• DOM d = .20
Range d = .50 to .79 for risk‐specific measures (Yang, Wong, & Coid, 2010)
ViolenceRisk
ANT
AGG
DOM/WRM
VPI
Risk for Suicide• Suicidal Ideation (SUI) scale
– Content focuses on hopelessness, thoughts of dying, suicidal ideation, and plans to commit suicide.
• Current and historical wording of items. • Independent of the Suicide Potential Index (SPI).
• SUI Critical Items (CI)– 4 items address current thoughts or preparatory indicators.
• Items 60 , 100, 140, 260, 340
• Suicide Potential Index (SPI) – Profile characteristics reflecting psychopathology associated with increased suicide risk.
• SPI > 81T = increase risk for suicide
SUI InterpretationT-score Interpretative significance
< 60T Person denies, or has minimal, thoughts of suicide or death.
60T – 69T Person may entertain periodic and transient suicidal ideation; also likely to be pessimistic and sad.
70T-83T Person reports significant suicidal ideation. Person likely to be anxious, depressed, hopeless, and social isolated.
>84T Often associated with severe suicidal ideation and imminent plans for self-harm. Immediate intervention is required. Person has a profound sense of despair and sadness, and may have taken steps towards suicide. Significant potential for completed suicide.
20
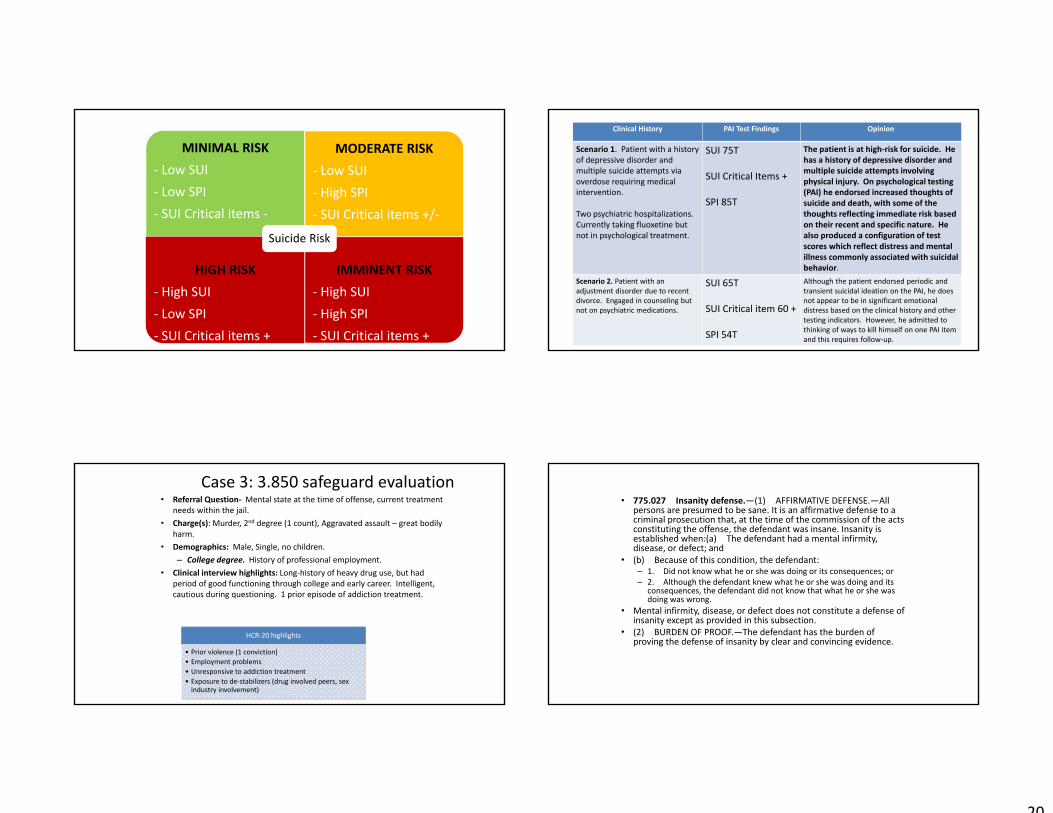
MINIMAL RISK‐ Low SUI‐ Low SPI‐ SUI Critical items ‐
MODERATE RISK‐ Low SUI‐ High SPI‐ SUI Critical items +/‐
HIGH RISK‐ High SUI‐ Low SPI‐ SUI Critical items +
IMMINENT RISK‐ High SUI‐ High SPI‐ SUI Critical items +
Suicide Risk
Clinical History PAI Test Findings Opinion
Scenario 1. Patient with a history of depressive disorder and multiple suicide attempts via overdose requiring medical intervention.
Two psychiatric hospitalizations. Currently taking fluoxetine but not in psychological treatment.
SUI 75T
SUI Critical Items +
SPI 85T
The patient is at high‐risk for suicide. He has a history of depressive disorder and multiple suicide attempts involving physical injury. On psychological testing (PAI) he endorsed increased thoughts of suicide and death, with some of the thoughts reflecting immediate risk based on their recent and specific nature. He also produced a configuration of test scores which reflect distress and mental illness commonly associated with suicidal behavior.
Scenario 2. Patient with an adjustment disorder due to recent divorce. Engaged in counseling but not on psychiatric medications.
SUI 65T
SUI Critical item 60 +
SPI 54T
Although the patient endorsed periodic and transient suicidal ideation on the PAI, he does not appear to be in significant emotional distress based on the clinical history and other testing indicators. However, he admitted to thinking of ways to kill himself on one PAI item and this requires follow‐up.
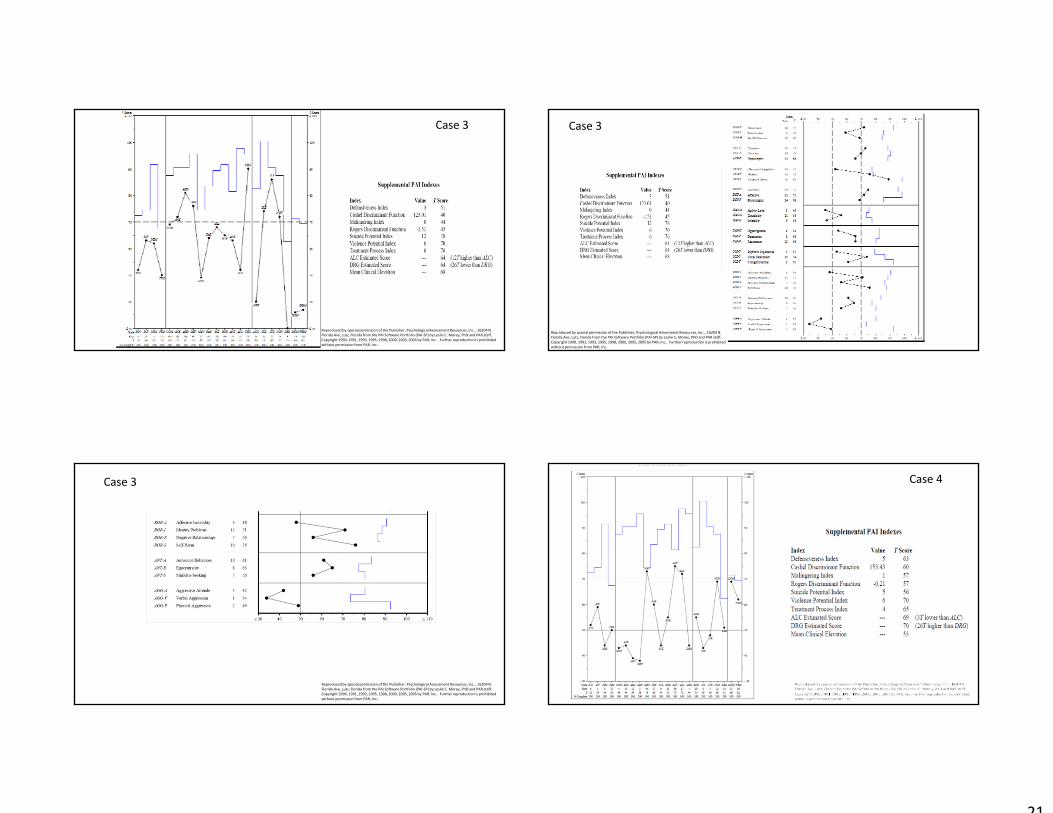
Case 3: 3.850 safeguard evaluation• Referral Question‐ Mental state at the time of offense, current treatment
needs within the jail. • Charge(s): Murder, 2nd degree (1 count), Aggravated assault – great bodily
harm.• Demographics: Male, Single, no children.
– College degree. History of professional employment.• Clinical interview highlights: Long‐history of heavy drug use, but had
period of good functioning through college and early career. Intelligent, cautious during questioning. 1 prior episode of addiction treatment.
HCR‐20 highlights
• Prior violence (1 conviction)• Employment problems• Unresponsive to addiction treatment• Exposure to de‐stabilizers (drug involved peers, sex industry involvement)
• 775.027 Insanity defense.—(1) AFFIRMATIVE DEFENSE.—All persons are presumed to be sane. It is an affirmative defense to a criminal prosecution that, at the time of the commission of the acts constituting the offense, the defendant was insane. Insanity is established when:(a) The defendant had a mental infirmity, disease, or defect; and
• (b) Because of this condition, the defendant:– 1. Did not know what he or she was doing or its consequences; or– 2. Although the defendant knew what he or she was doing and its
consequences, the defendant did not know that what he or she was doing was wrong.
• Mental infirmity, disease, or defect does not constitute a defense of insanity except as provided in this subsection.
• (2) BURDEN OF PROOF.—The defendant has the burden of proving the defense of insanity by clear and convincing evidence.
21
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 3
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 3
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 3
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 4

22
Case 4
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 4
Case 4 Training Outline• Part 1. Conceptual Overview
• Part 2. The Case for Self‐Report Assessment
• Part 3. Evaluation of Response Styles
• Part 4. Evaluation of Risk to Self and Others
• Part 5. Evaluation of Treatment Needs
• Part 6. Evaluation of Treatment Responsiveness

23
Borderline Features (BOR)• Scale designed to measure severe personality disorder often associated with Borderline Personality Disorder. – Includes assessment of emotional dysregulation, identity confusion, poor self‐worth, interpersonal dysfunction, and destructive impulsivity.
BOR
Affective Instability
(bor-a)
Identity Problems
(bor-i)
Negative Relationships
(bor-n)Self-Harm
(bor-s)
Alcohol Problems (ALC)• Scale designed to measure signs and symptoms of alcohol use disorders. – Content includes questions about abstinence, alcohol‐related problems, loss of control of alcohol use, and alcohol cravings.
ALCALC
Estimated
Concurrent Validity of the PAI ALC Scale in College StudentsRuiz, Dickinson, & Pincus (2002)
• Examined relationship between ALC scores and SCID‐IV Alcohol Use Disorder Diagnoses
• Sample = 200 college student drinkers.
• Participants administered protocol individually.
ALC
r AUC
Quantity/Frequency .63**
Binge Drinking .60**
Alcohol Expectancies .47**
Maladaptive Coping .66**
Alcohol Abuse DX .74**
Alcohol Dependence DX .84**
Drug Problems (DRG)• Scale designed to measure signs and symptoms of drug use, abuse, and dependence. – Content focuses on drug‐use history (both prescription and illicit) as well as drug‐related functional impairment.
– Less reliable than the other scales.
DRGDRG
Estimated

24
Addiction in Federal InmatesPatry, Magaletta, Diamond, & Weinman (2010)
• N = 1,120 federal inmates participating U.S. BOP Mental Health Prevalence Project• Data were gathered over an 18‐month period. • 14 different facilities, 3 different security levels. • PAI, administrative, and clinical data were collected on newly admitted inmates.
ALC ALCpr DRG DRGpr
Hx of Addiction Treatment .19* .02 .33* .27*Hx of Mandated Treatment .10* .06 .10* .05Clinician Recommends Tx .20* .02 .34* .29*Substance Use Diagnosis .19* .02 .31* .25*Violent Conviction .11* .11* .04 ‐.03 30
40
50
60
70
80
90
ICN INF NIM PIM SOM ANX ARD DEP MAN PAR SCZ BOR ANT ALC DRG AGG SUI STR NON RXR
PAI profile of 160 individuals in a methadone maintenance treatment
(Alterman et al. 1995)
Anxiety‐Related Disorders (ARD)• Assesses clinical and behavioral manifestations of anxiety disorder symptoms.– Content reflects obsessive‐compulsive thoughts and behaviors, specific and excessive fears, and symptoms related to traumatic stress.
– Subscales are required to clarify full scale elevations.
ARD
Obsessive-compulsive
(ard-o)
Phobias(ard-p)
Traumatic Stress(ard-t)
Depression (DEP)
• Reflects signs and symptoms of depressive disorder.– Item content includes issues about pessimism, negative expectations, unhappiness, and vegetative symptoms.
DEP
Cognitive (dep-c)
Affective(dep-a)
Physiological(dep-p)
SUI?MAN?
25
Schedule for Affective Disorders & Schizophrenia (SADS)
PAI scales ANX DEP MAN PAR SCZ
ANX .65 .63 ‐.04 .41 .23
ARD .40 .48 .02 .44 .32
DEP .45 .67 ‐.02 .46 .11
MAN .00 .20 .31 .47 .37
PAR .18 .33 .04 .53 .26
SCZ .37 .51 .12 .56 .46
N = 80. Participants were referrals to an acute mental health service within an urban correctional facility.
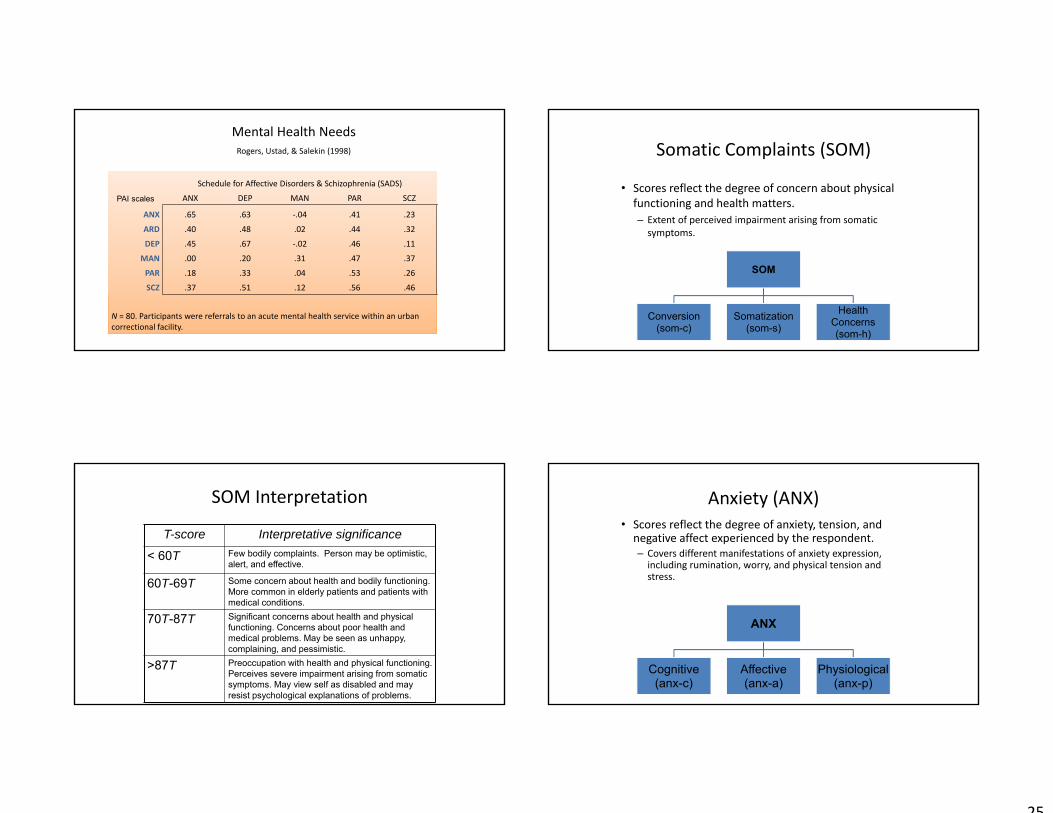
Mental Health NeedsRogers, Ustad, & Salekin (1998) Somatic Complaints (SOM)
• Scores reflect the degree of concern about physical functioning and health matters.– Extent of perceived impairment arising from somatic symptoms.
SOM
Conversion (som-c)
Somatization(som-s)
Health Concerns(som-h)
SOM Interpretation
T-score Interpretative significance
< 60T Few bodily complaints. Person may be optimistic, alert, and effective.
60T-69T Some concern about health and bodily functioning. More common in elderly patients and patients with medical conditions.
70T-87T Significant concerns about health and physical functioning. Concerns about poor health and medical problems. May be seen as unhappy, complaining, and pessimistic.
>87T Preoccupation with health and physical functioning. Perceives severe impairment arising from somatic symptoms. May view self as disabled and may resist psychological explanations of problems.
Anxiety (ANX)• Scores reflect the degree of anxiety, tension, and negative affect experienced by the respondent. – Covers different manifestations of anxiety expression, including rumination, worry, and physical tension and stress.
ANX
Cognitive (anx-c)
Affective(anx-a)
Physiological(anx-p)
26
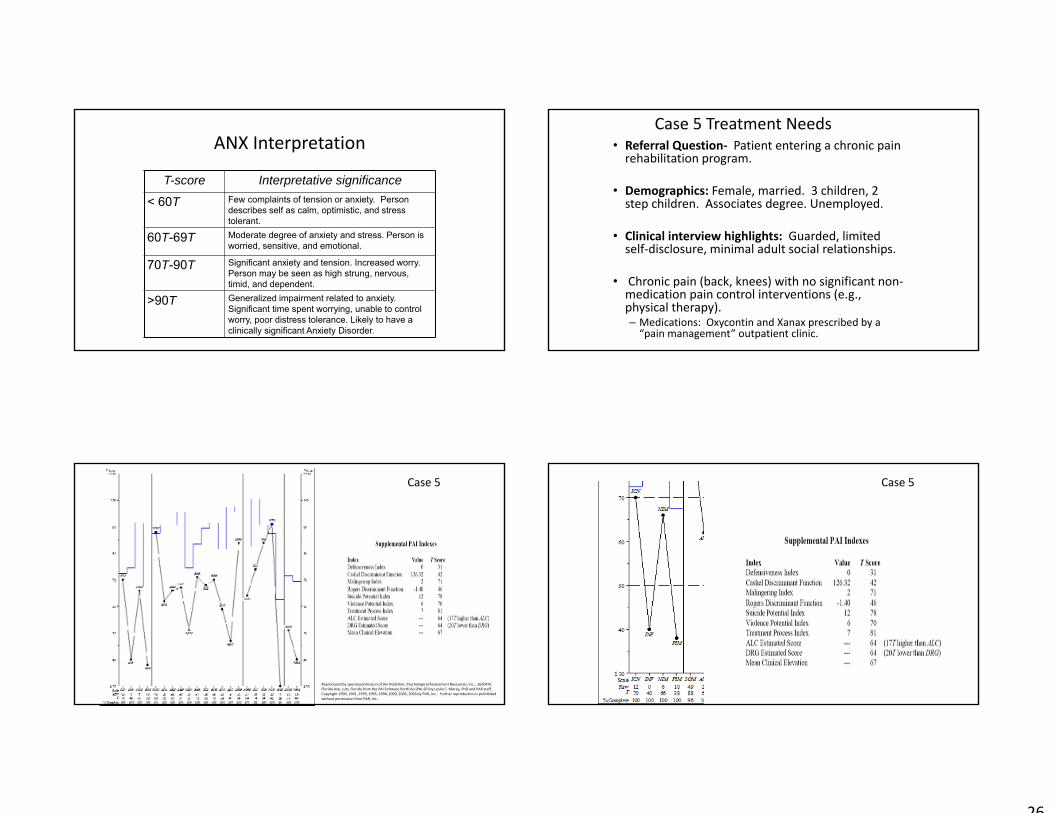
ANX Interpretation
T-score Interpretative significance
< 60T Few complaints of tension or anxiety. Person describes self as calm, optimistic, and stress tolerant.
60T-69T Moderate degree of anxiety and stress. Person is worried, sensitive, and emotional.
70T-90T Significant anxiety and tension. Increased worry. Person may be seen as high strung, nervous, timid, and dependent.
>90T Generalized impairment related to anxiety. Significant time spent worrying, unable to control worry, poor distress tolerance. Likely to have a clinically significant Anxiety Disorder.
Case 5 Treatment Needs• Referral Question‐ Patient entering a chronic pain rehabilitation program.
• Demographics: Female, married. 3 children, 2 step children. Associates degree. Unemployed.
• Clinical interview highlights: Guarded, limited self‐disclosure, minimal adult social relationships.
• Chronic pain (back, knees) with no significant non‐medication pain control interventions (e.g., physical therapy). – Medications: Oxycontin and Xanax prescribed by a “pain management” outpatient clinic.
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 5 Case 5
27
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 5
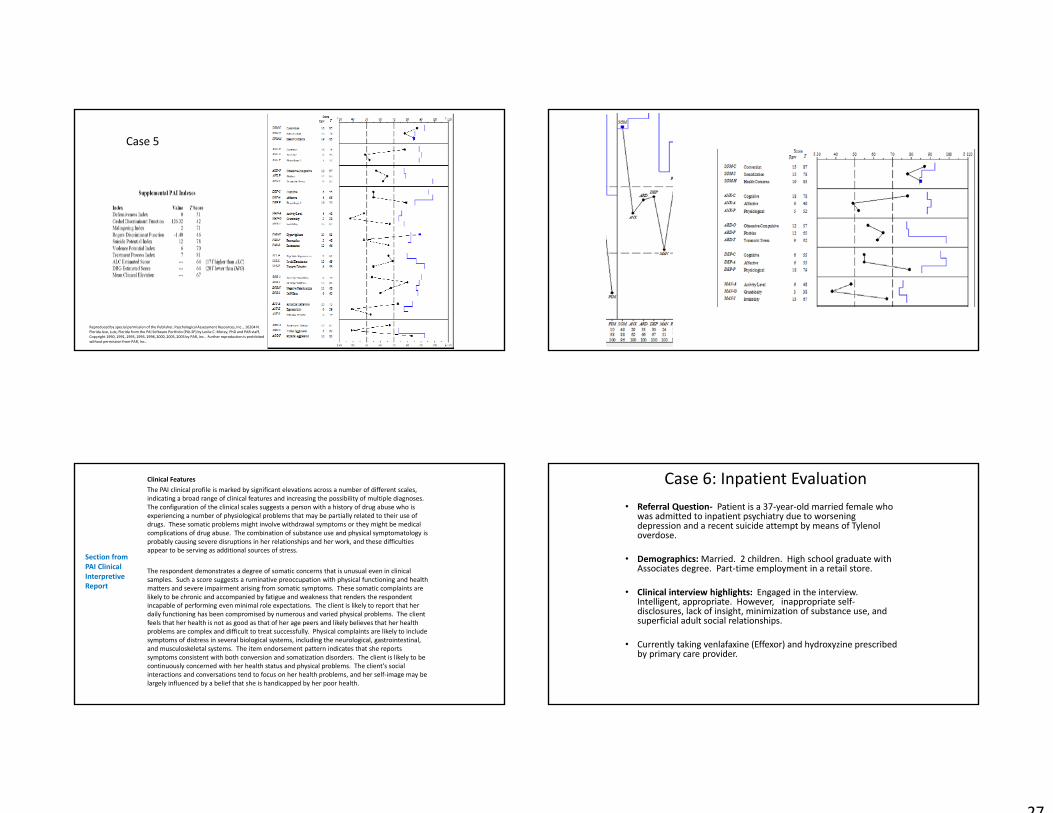
Clinical FeaturesThe PAI clinical profile is marked by significant elevations across a number of different scales, indicating a broad range of clinical features and increasing the possibility of multiple diagnoses. The configuration of the clinical scales suggests a person with a history of drug abuse who is experiencing a number of physiological problems that may be partially related to their use of drugs. These somatic problems might involve withdrawal symptoms or they might be medical complications of drug abuse. The combination of substance use and physical symptomatology is probably causing severe disruptions in her relationships and her work, and these difficulties appear to be serving as additional sources of stress.
The respondent demonstrates a degree of somatic concerns that is unusual even in clinical samples. Such a score suggests a ruminative preoccupation with physical functioning and health matters and severe impairment arising from somatic symptoms. These somatic complaints are likely to be chronic and accompanied by fatigue and weakness that renders the respondent incapable of performing even minimal role expectations. The client is likely to report that her daily functioning has been compromised by numerous and varied physical problems. The client feels that her health is not as good as that of her age peers and likely believes that her health problems are complex and difficult to treat successfully. Physical complaints are likely to include symptoms of distress in several biological systems, including the neurological, gastrointestinal, and musculoskeletal systems. The item endorsement pattern indicates that she reports symptoms consistent with both conversion and somatization disorders. The client is likely to be continuously concerned with her health status and physical problems. The client's social interactions and conversations tend to focus on her health problems, and her self‐image may be largely influenced by a belief that she is handicapped by her poor health.
Section from PAI Clinical Interpretive Report
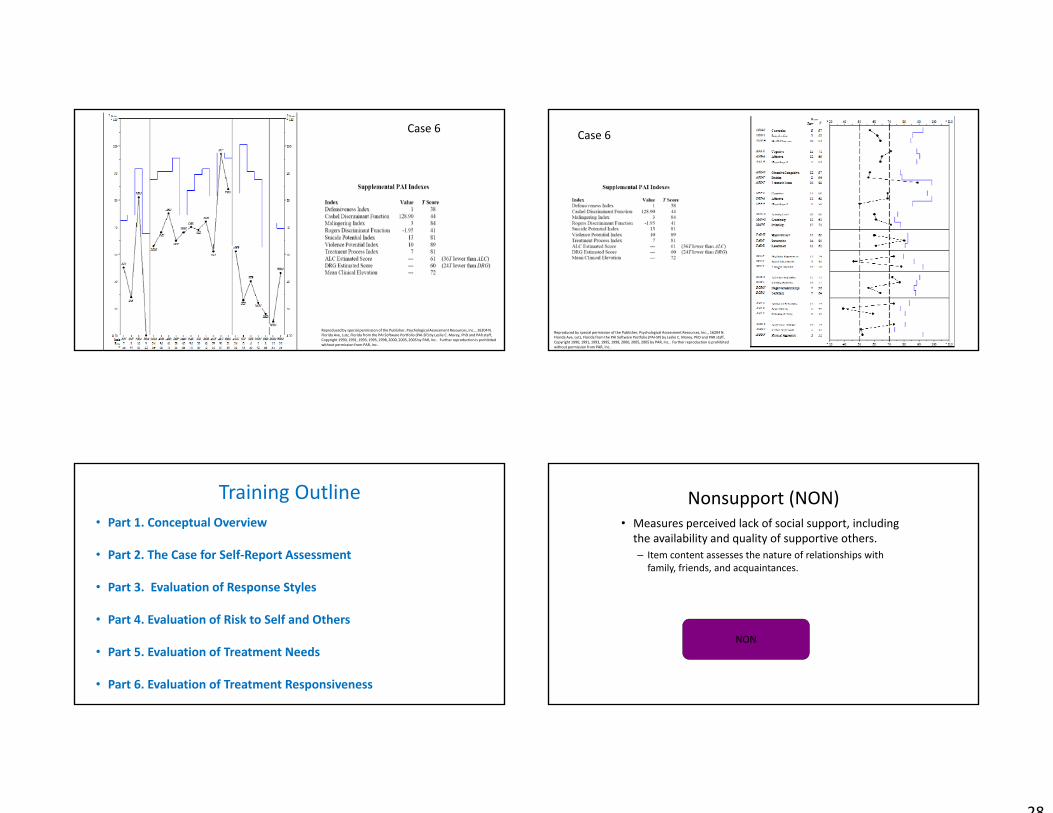
Case 6: Inpatient Evaluation• Referral Question‐ Patient is a 37‐year‐old married female who
was admitted to inpatient psychiatry due to worsening depression and a recent suicide attempt by means of Tylenol overdose.
• Demographics:Married. 2 children. High school graduate with Associates degree. Part‐time employment in a retail store.
• Clinical interview highlights: Engaged in the interview. Intelligent, appropriate. However, inappropriate self‐disclosures, lack of insight, minimization of substance use, and superficial adult social relationships.
• Currently taking venlafaxine (Effexor) and hydroxyzine prescribed by primary care provider.
28
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 6
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 6
Training Outline• Part 1. Conceptual Overview
• Part 2. The Case for Self‐Report Assessment
• Part 3. Evaluation of Response Styles
• Part 4. Evaluation of Risk to Self and Others
• Part 5. Evaluation of Treatment Needs
• Part 6. Evaluation of Treatment Responsiveness
Nonsupport (NON)• Measures perceived lack of social support, including the availability and quality of supportive others.– Item content assesses the nature of relationships with family, friends, and acquaintances.
NON

29
Treatment Rejection (RXR)• Measures attitudes and characteristics associated with an interest for psychological change.– Item assess an unwillingness to change, a refusal to accept responsibility for problems, and a denial of life difficulties.
RXR
Treatment Responsiveness
rpb Base Rate ANT rpb AGG rpb VPI rpb RXR rpbGeneral Infraction 64% .24** .24** .19** .07
Non‐compliance 10% .09 .12 .12 .14*
Major Infraction 19% .28** .19** .18* .02
Caperton et al. (2004). N = 137 male inmates in a sex offender treatment program. About 1.5‐year follow‐up. PAIs administered as part of program assessment.
ANT was found to be the primary predictor of outcomes when controlling for the effects of VPI and AGG.
Is there little reasons to consider AGG and VPI scores beyond ANT when considering the prediction of misconduct?
Treatment Responsiveness cont…
Outcome Odds Ratio 95% CI
General Non‐compliance
AGG > 70T 2.07** 1.26‐3.40
ANT >70T 1.55 .095‐2.53
Disruptive Behavior
AGG > 70T 2.32** 1.38‐3.92
ANT >70T 2.29** 1.25‐4.20
BOR >70T 1.89** 1.11‐3.21
Aggressive Acts
AGG > 70T 2.80** 1.55‐5.05
ANT >70T 2.79** 1.37‐5.69
BOR >70T 1.86** 1.03‐3.37
Magyar, Edens, Lilienfeld, Douglas, Poythress, & Skeem (2012)
• N = 331 male offenders in residential drug treatment.• Prospective data from clinical records and counselor interviews.
Effects also found for Hostile
Dominance
Case 7: Treatment amenability• Referral Question‐ Mental health evaluation for sentencing mitigation.
• Charge(s): Aggravated Child Abuse, Resisting arrest with violence, Violation of probation.
• Demographics: Male. Single, never married. High school graduate, some college.
• Clinical interview highlights: Remorseful, but limited insight. Minimized substance abuse problems.
WASI‐II
• FS IQ‐4 = 101• No verbal or performance differences
HCR‐20 highlights
• Prior violence (x2)• Young age at first violent incident
• Negative attitudes• Plans lack feasibility

30
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 7
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc.., 16204 N. Florida Ave, Lutz, Florida from the PAI Software Portfolio (PAI‐SP) by Leslie C. Morey, PhD and PAR staff, Copyright 1990, 1991, 1993, 1995, 1998, 2000, 2005, 2005 by PAR, Inc.. Further reproduction is prohibited without permission from PAR, Inc..
Case 7