Clinical Anatomy Clinical importance of anatomical ... · Laparoscopic donor nephrectomy has become...
7
Clinical Anatomy Page 1 of 7 Compeng interests: none declared. Conflict of interests: none declared. All authors contributed to the concepon, design, and preparaon of the manuscript, as well as read and approved the final manuscript. All authors abide by the Associaon for Medical Ethics (AME) ethical rules of disclosure. For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25. Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY) Review Abstract Introduction Laparoscopic live donor nephrec- tomy has become a well-accepted practice in most transplant units. However, the variations and complex of renal vasculature may make the surgery even more challenging during laparoscopic donor nephrec- tomy. The aims of this article are to review embryology of the renal vasculature development and the clinical significance of renal vascula- ture anomalies during laparoscopic donor nephrectomy and the conse- quence of kidney transplant. Discussion The results were interpreted and summarised as renal artery develop- ment and its anomalies and renal vein development and its anomalies including associated anomalies of the inferior vena cava. The clinical signifi- cance during laparoscopic donor nephrectomy was explored. The value of computed tomography angiog- raphy was emphasised during live donor work-up and before surgery planning. Conclusion It is paramount for surgeons to have a thorough knowledge of renal vascula- ture development and to readily iden- tify the anomalies of renal vascula- ture on computed tomography angiography prior to laparoscopic donor nephrectomy. The adverse Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy B He 1,2 *, JM Hamdorf 2 bleeding event can be therefore prevented. Introduction Laparoscopic donor nephrectomy has become the standard of care in most transplant centres around the world. It is a unique surgery to predis- pose the surgeons under stress as healthy donors have a major surgery purely for others’ benefits rather than themselves. Renal vessels are known with a wide range of variations that have also been evidenced during live kidney donor work-up in recent years. Most of these variations may otherwise have no clinical signifi- cance other than the surgery for lapa- roscopic donor nephrectomy. These variations can lead to significant surgical complications or even life- threatening events if unrecognised. There are increased reports in the literature identifying variation of renal vasculature during live donor nephrectomy 1–11 . Undoubtedly, a thorough knowledge in under- standing of the embryologic develop- ment and associated anatomy of renal vessel variations will equip the surgeons to anticipate and manage these potential risks successfully to prevent the complications. Therefore, the aims of this review are to explore the embryology of renal vasculature and associated variations and to emphasise the importance during laparoscopic live donor nephrectomy. Discussion The authors have referenced some of their own studies in this review. These referenced studies have been conducted in accordance with the Declaration of Helsinki (1964), and the protocols of these studies have been approved by the relevant ethics committees related to the institution in which they were performed. All human subjects, in these referenced studies, gave informed consent to participate in these studies. Embryology of renal arteries The kidneys ascend to the lumbar region below the adrenal glands during the embryological develop- ment between the sixth and ninth weeks possibly due to differential growth of the lumbar and sacral regions of the embryo. As the kidneys ascend they are vascularised by a succession of transient aortic sprouts that arise at higher levels progres- sively. These arteries do not elongate to follow the ascending kidneys; instead they are degenerated and replaced by successive new arteries. The final pair of arteries forms in the upper lumbar region as the definitive renal arteries. Sometimes, the infe- rior pair of arteries is not degener- ated and becomes an accessory lower pole artery. The kidney may become ectopic in the pelvis if it fails to ascend adequately (Figure 1) The horseshoe kidney may be developed if the lower pole is fused and becomes trapped by the inferior mesenteric artery and thus the kidney cannot ascend to the lumbar region 12 . The origin of intrarenal vascula- ture has not yet been completely understood. It was postulated that the renal vasculature derived exclu- sively from the branches off the aorta and other pre-existing extrarenal vessels. However, there was evidence that the renal vessels may originate within the embryonic kidney from *Corresponding author Email: [email protected] 1 Sir Charles Gairdner Hospital, Hospital Ave- nue, Nedlands, Perth, Australia 2 School of Surgery, The University of Western Australia, Crawley, WA, Perth, Australia
Transcript of Clinical Anatomy Clinical importance of anatomical ... · Laparoscopic donor nephrectomy has become...
Clin
ical
Ana
tom
yPage 1 of 7
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Review
Abstract IntroductionLaparoscopic live donor nephrec-tomy has become a well-accepted practice in most transplant units. However, the variations and complex of renal vasculature may make the surgery even more challenging during laparoscopic donor nephrec-tomy. The aims of this article are to review embryology of the renal vasculature development and the clinical significance of renal vascula-ture anomalies during laparoscopic donor nephrectomy and the conse-quence of kidney transplant. DiscussionThe results were interpreted and summarised as renal artery develop-ment and its anomalies and renal vein development and its anomalies including associated anomalies of the inferior vena cava. The clinical signifi-cance during laparoscopic donor nephrectomy was explored. The value of computed tomography angiog-raphy was emphasised during live donor work-up and before surgery planning.ConclusionIt is paramount for surgeons to have a thorough knowledge of renal vascula-ture development and to readily iden-tify the anomalies of renal vascula-ture on computed tomography angiography prior to laparoscopic donor nephrectomy. The adverse
Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy
B He1,2*, JM Hamdorf2
bleeding event can be therefore prevented.
IntroductionLaparoscopic donor nephrectomy has become the standard of care in most transplant centres around the world. It is a unique surgery to predis-pose the surgeons under stress as healthy donors have a major surgery purely for others’ benefits rather than themselves. Renal vessels are known with a wide range of variations that have also been evidenced during live kidney donor work-up in recent years. Most of these variations may otherwise have no clinical signifi-cance other than the surgery for lapa-roscopic donor nephrectomy. These variations can lead to significant surgical complications or even life-threatening events if unrecognised. There are increased reports in the literature identifying variation of renal vasculature during live donor nephrectomy1–11. Undoubtedly, a thorough knowledge in under-standing of the embryologic develop-ment and associated anatomy of renal vessel variations will equip the surgeons to anticipate and manage these potential risks successfully to prevent the complications. Therefore, the aims of this review are to explore the embryology of renal vasculature and associated variations and to emphasise the importance during laparoscopic live donor nephrectomy.
DiscussionThe authors have referenced some of their own studies in this review. These referenced studies have been conducted in accordance with the Declaration of Helsinki (1964), and
the protocols of these studies have been approved by the relevant ethics committees related to the institution in which they were performed. All human subjects, in these referenced studies, gave informed consent to participate in these studies.
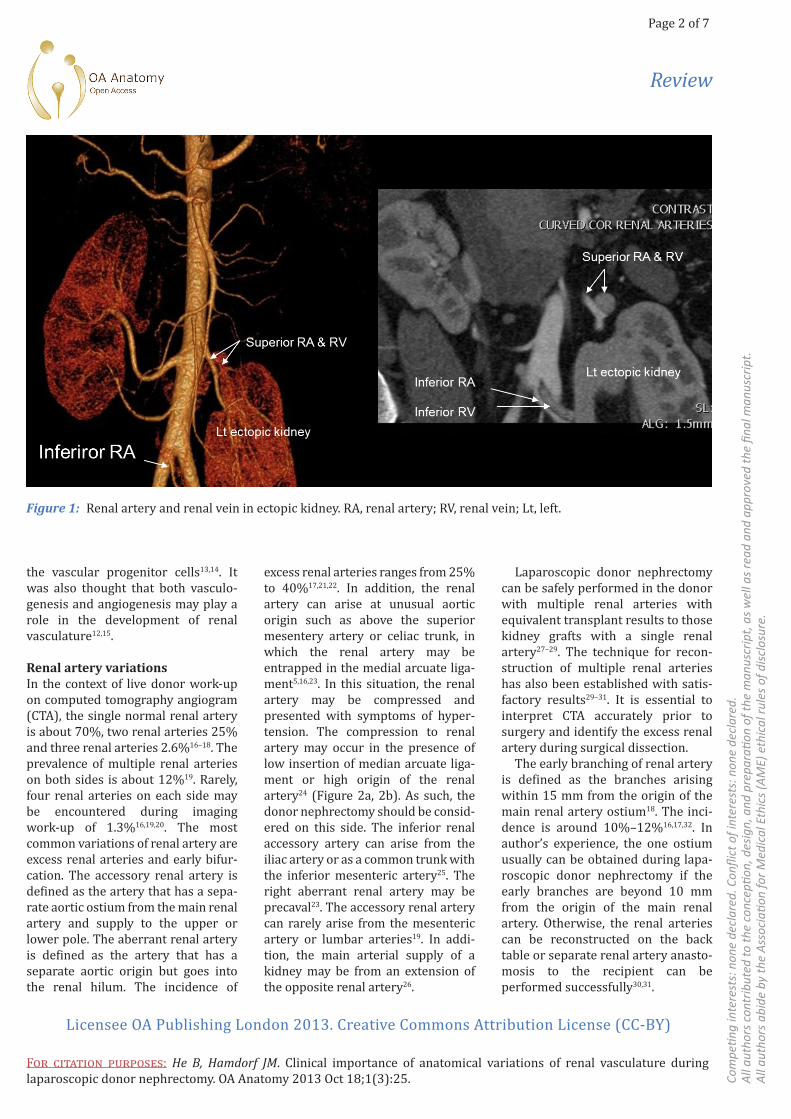
Embryology of renal arteriesThe kidneys ascend to the lumbar region below the adrenal glands during the embryological develop-ment between the sixth and ninth weeks possibly due to differential growth of the lumbar and sacral regions of the embryo. As the kidneys ascend they are vascularised by a succession of transient aortic sprouts that arise at higher levels progres-sively. These arteries do not elongate to follow the ascending kidneys; instead they are degenerated and replaced by successive new arteries. The final pair of arteries forms in the upper lumbar region as the definitive renal arteries. Sometimes, the infe-rior pair of arteries is not degener-ated and becomes an accessory lower pole artery. The kidney may become ectopic in the pelvis if it fails to ascend adequately (Figure 1) The horseshoe kidney may be developed if the lower pole is fused and becomes trapped by the inferior mesenteric artery and thus the kidney cannot ascend to the lumbar region12.
The origin of intrarenal vascula-ture has not yet been completely understood. It was postulated that the renal vasculature derived exclu-sively from the branches off the aorta and other pre-existing extrarenal vessels. However, there was evidence that the renal vessels may originate within the embryonic kidney from
*Corresponding author Email: [email protected] Sir Charles Gairdner Hospital, Hospital Ave-
nue, Nedlands, Perth, Australia2 School of Surgery, The University of Western
Australia, Crawley, WA, Perth, Australia
Page 2 of 7
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Review
the vascular progenitor cells13,14. It was also thought that both vasculo-genesis and angiogenesis may play a role in the development of renal vasculature12,15.
Renal artery variationsIn the context of live donor work-up on computed tomography angiogram (CTA), the single normal renal artery is about 70%, two renal arteries 25% and three renal arteries 2.6%16–18. The prevalence of multiple renal arteries on both sides is about 12%19. Rarely, four renal arteries on each side may be encountered during imaging work-up of 1.3%16,19,20. The most common variations of renal artery are excess renal arteries and early bifur-cation. The accessory renal artery is defined as the artery that has a sepa-rate aortic ostium from the main renal artery and supply to the upper or lower pole. The aberrant renal artery is defined as the artery that has a separate aortic origin but goes into the renal hilum. The incidence of
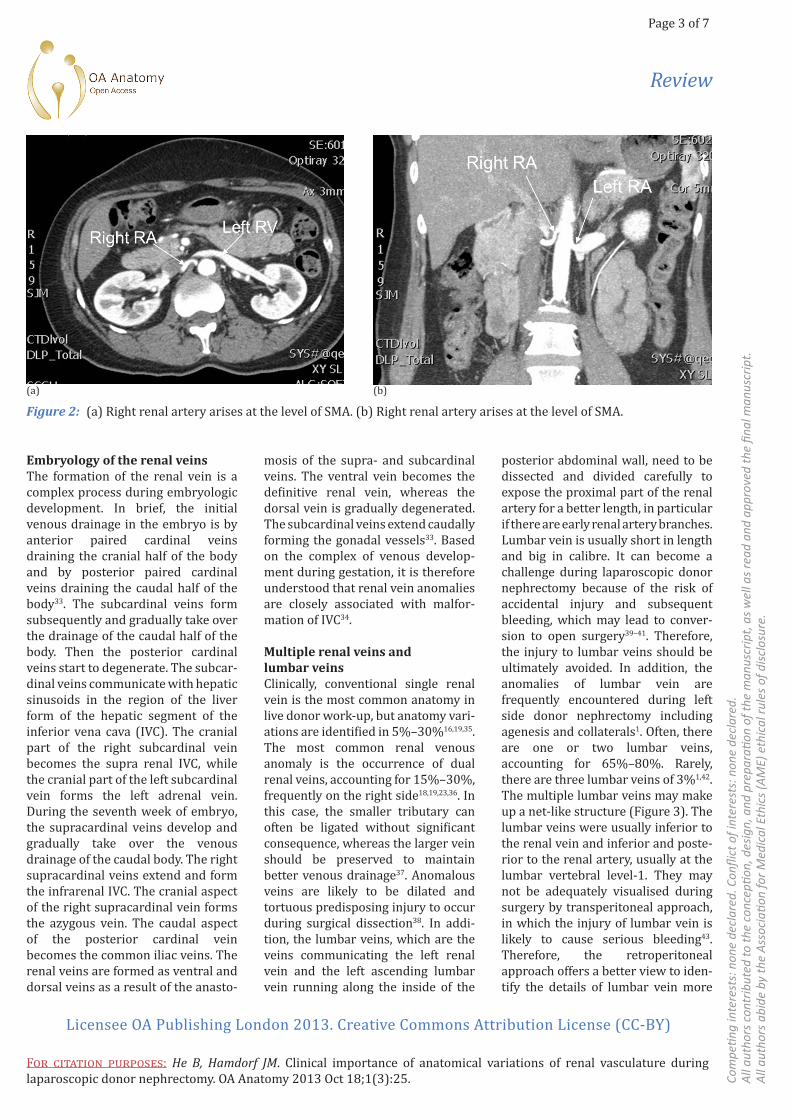
excess renal arteries ranges from 25% to 40%17,21,22. In addition, the renal artery can arise at unusual aortic origin such as above the superior mesentery artery or celiac trunk, in which the renal artery may be entrapped in the medial arcuate liga-ment5,16,23. In this situation, the renal artery may be compressed and presented with symptoms of hyper-tension. The compression to renal artery may occur in the presence of low insertion of median arcuate liga-ment or high origin of the renal artery24 (Figure 2a, 2b). As such, the donor nephrectomy should be consid-ered on this side. The inferior renal accessory artery can arise from the iliac artery or as a common trunk with the inferior mesenteric artery25. The right aberrant renal artery may be precaval23. The accessory renal artery can rarely arise from the mesenteric artery or lumbar arteries19. In addi-tion, the main arterial supply of a kidney may be from an extension of the opposite renal artery26.
Laparoscopic donor nephrectomy can be safely performed in the donor with multiple renal arteries with equivalent transplant results to those kidney grafts with a single renal artery27–29. The technique for recon-struction of multiple renal arteries has also been established with satis-factory results29–31. It is essential to interpret CTA accurately prior to surgery and identify the excess renal artery during surgical dissection.
The early branching of renal artery is defined as the branches arising within 15 mm from the origin of the main renal artery ostium18. The inci-dence is around 10%–12%16,17,32. In author’s experience, the one ostium usually can be obtained during lapa-roscopic donor nephrectomy if the early branches are beyond 10 mm from the origin of the main renal artery. Otherwise, the renal arteries can be reconstructed on the back table or separate renal artery anasto-mosis to the recipient can be performed successfully30,31.
Figure 1: Renal artery and renal vein in ectopic kidney. RA, renal artery; RV, renal vein; Lt, left.
Page 3 of 7
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Review
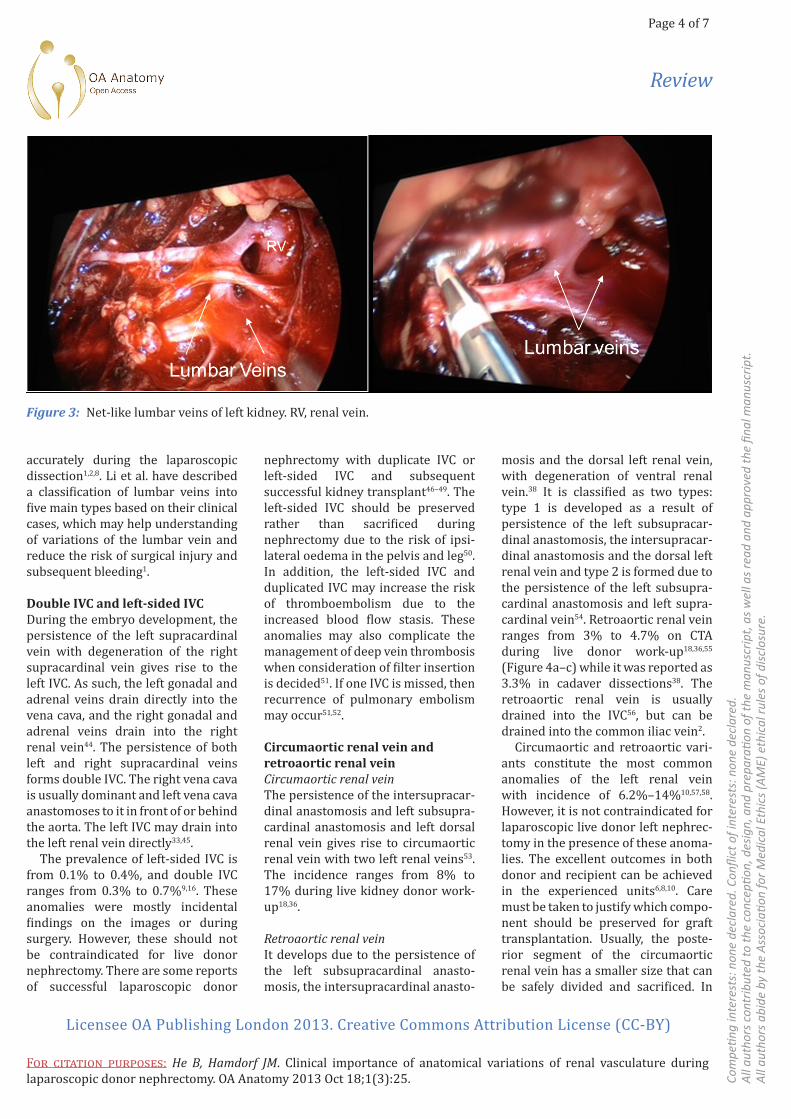
posterior abdominal wall, need to be dissected and divided carefully to expose the proximal part of the renal artery for a better length, in particular if there are early renal artery branches. Lumbar vein is usually short in length and big in calibre. It can become a challenge during laparoscopic donor nephrectomy because of the risk of accidental injury and subsequent bleeding, which may lead to conver-sion to open surgery39–41. Therefore, the injury to lumbar veins should be ultimately avoided. In addition, the anomalies of lumbar vein are frequently encountered during left side donor nephrectomy including agenesis and collaterals1. Often, there are one or two lumbar veins, accounting for 65%–80%. Rarely, there are three lumbar veins of 3%1,42. The multiple lumbar veins may make up a net-like structure (Figure 3). The lumbar veins were usually inferior to the renal vein and inferior and poste-rior to the renal artery, usually at the lumbar vertebral level-1. They may not be adequately visualised during surgery by transperitoneal approach, in which the injury of lumbar vein is likely to cause serious bleeding43. Therefore, the retroperitoneal approach offers a better view to iden-tify the details of lumbar vein more
Embryology of the renal veinsThe formation of the renal vein is a complex process during embryologic development. In brief, the initial venous drainage in the embryo is by anterior paired cardinal veins draining the cranial half of the body and by posterior paired cardinal veins draining the caudal half of the body33. The subcardinal veins form subsequently and gradually take over the drainage of the caudal half of the body. Then the posterior cardinal veins start to degenerate. The subcar-dinal veins communicate with hepatic sinusoids in the region of the liver form of the hepatic segment of the inferior vena cava (IVC). The cranial part of the right subcardinal vein becomes the supra renal IVC, while the cranial part of the left subcardinal vein forms the left adrenal vein. During the seventh week of embryo, the supracardinal veins develop and gradually take over the venous drainage of the caudal body. The right supracardinal veins extend and form the infrarenal IVC. The cranial aspect of the right supracardinal vein forms the azygous vein. The caudal aspect of the posterior cardinal vein becomes the common iliac veins. The renal veins are formed as ventral and dorsal veins as a result of the anasto-
mosis of the supra- and subcardinal veins. The ventral vein becomes the definitive renal vein, whereas the dorsal vein is gradually degenerated. The subcardinal veins extend caudally forming the gonadal vessels33. Based on the complex of venous develop-ment during gestation, it is therefore understood that renal vein anomalies are closely associated with malfor-mation of IVC34.
Multiple renal veins and lumbar veinsClinically, conventional single renal vein is the most common anatomy in live donor work-up, but anatomy vari-ations are identified in 5%–30%16,19,35. The most common renal venous anomaly is the occurrence of dual renal veins, accounting for 15%–30%, frequently on the right side18,19,23,36. In this case, the smaller tributary can often be ligated without significant consequence, whereas the larger vein should be preserved to maintain better venous drainage37. Anomalous veins are likely to be dilated and tortuous predisposing injury to occur during surgical dissection38. In addi-tion, the lumbar veins, which are the veins communicating the left renal vein and the left ascending lumbar vein running along the inside of the
Figure 2: (a) Right renal artery arises at the level of SMA. (b) Right renal artery arises at the level of SMA.(a) (b)
Page 4 of 7
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Review
accurately during the laparoscopic dissection1,2,8. Li et al. have described a classification of lumbar veins into five main types based on their clinical cases, which may help understanding of variations of the lumbar vein and reduce the risk of surgical injury and subsequent bleeding1.
Double IVC and left-sided IVCDuring the embryo development, the persistence of the left supracardinal vein with degeneration of the right supracardinal vein gives rise to the left IVC. As such, the left gonadal and adrenal veins drain directly into the vena cava, and the right gonadal and adrenal veins drain into the right renal vein44. The persistence of both left and right supracardinal veins forms double IVC. The right vena cava is usually dominant and left vena cava anastomoses to it in front of or behind the aorta. The left IVC may drain into the left renal vein directly33,45.
The prevalence of left-sided IVC is from 0.1% to 0.4%, and double IVC ranges from 0.3% to 0.7%9,16. These anomalies were mostly incidental findings on the images or during surgery. However, these should not be contraindicated for live donor nephrectomy. There are some reports of successful laparoscopic donor
nephrectomy with duplicate IVC or left-sided IVC and subsequent successful kidney transplant46–49. The left-sided IVC should be preserved rather than sacrificed during nephrectomy due to the risk of ipsi-lateral oedema in the pelvis and leg50. In addition, the left-sided IVC and duplicated IVC may increase the risk of thromboembolism due to the increased blood flow stasis. These anomalies may also complicate the management of deep vein thrombosis when consideration of filter insertion is decided51. If one IVC is missed, then recurrence of pulmonary embolism may occur51,52.
Circumaortic renal vein and retroaortic renal veinCircumaortic renal veinThe persistence of the intersupracar-dinal anastomosis and left subsupra-cardinal anastomosis and left dorsal renal vein gives rise to circumaortic renal vein with two left renal veins53. The incidence ranges from 8% to 17% during live kidney donor work-up18,36.
Retroaortic renal veinIt develops due to the persistence of the left subsupracardinal anasto-mosis, the intersupracardinal anasto-
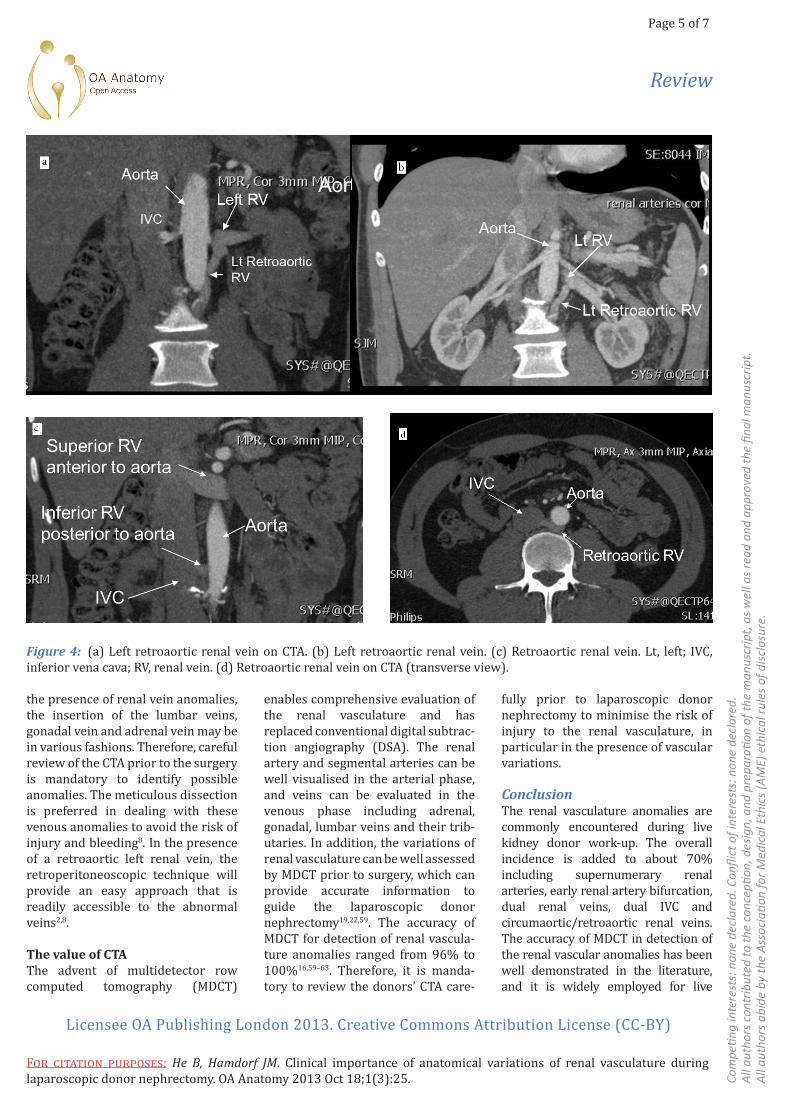
mosis and the dorsal left renal vein, with degeneration of ventral renal vein.38 It is classified as two types: type 1 is developed as a result of persistence of the left subsupracar-dinal anastomosis, the intersupracar-dinal anastomosis and the dorsal left renal vein and type 2 is formed due to the persistence of the left subsupra-cardinal anastomosis and left supra-cardinal vein54. Retroaortic renal vein ranges from 3% to 4.7% on CTA during live donor work-up18,36,55 (Figure 4a–c) while it was reported as 3.3% in cadaver dissections38. The retroaortic renal vein is usually drained into the IVC56, but can be drained into the common iliac vein2.
Circumaortic and retroaortic vari-ants constitute the most common anomalies of the left renal vein with incidence of 6.2%–14%10,57,58. However, it is not contraindicated for laparoscopic live donor left nephrec-tomy in the presence of these anoma-lies. The excellent outcomes in both donor and recipient can be achieved in the experienced units6,8,10. Care must be taken to justify which compo-nent should be preserved for graft transplantation. Usually, the poste-rior segment of the circumaortic renal vein has a smaller size that can be safely divided and sacrificed. In
Figure 3: Net-like lumbar veins of left kidney. RV, renal vein.
Page 5 of 7
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Review
the presence of renal vein anomalies, the insertion of the lumbar veins, gonadal vein and adrenal vein may be in various fashions. Therefore, careful review of the CTA prior to the surgery is mandatory to identify possible anomalies. The meticulous dissection is preferred in dealing with these venous anomalies to avoid the risk of injury and bleeding8. In the presence of a retroaortic left renal vein, the retroperitoneoscopic technique will provide an easy approach that is readily accessible to the abnormal veins2,8.
The value of CTA The advent of multidetector row computed tomography (MDCT)
enables comprehensive evaluation of the renal vasculature and has replaced conventional digital subtrac-tion angiography (DSA). The renal artery and segmental arteries can be well visualised in the arterial phase, and veins can be evaluated in the venous phase including adrenal, gonadal, lumbar veins and their trib-utaries. In addition, the variations of renal vasculature can be well assessed by MDCT prior to surgery, which can provide accurate information to guide the laparoscopic donor nephrectomy19,22,59. The accuracy of MDCT for detection of renal vascula-ture anomalies ranged from 96% to 100%16,59–63. Therefore, it is manda-tory to review the donors’ CTA care-
fully prior to laparoscopic donor nephrectomy to minimise the risk of injury to the renal vasculature, in particular in the presence of vascular variations.
ConclusionThe renal vasculature anomalies are commonly encountered during live kidney donor work-up. The overall incidence is added to about 70% including supernumerary renal arteries, early renal artery bifurcation, dual renal veins, dual IVC and circumaortic/retroaortic renal veins. The accuracy of MDCT in detection of the renal vascular anomalies has been well demonstrated in the literature, and it is widely employed for live
Figure 4: (a) Left retroaortic renal vein on CTA. (b) Left retroaortic renal vein. (c) Retroaortic renal vein. Lt, left; IVC, inferior vena cava; RV, renal vein. (d) Retroaortic renal vein on CTA (transverse view).

Page 6 of 7
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Review
kidney donor work-up. In general, these variations are not contraindi-cated for consideration of laparoscopic donor nephrectomy and consequence of kidney transplant. However, it is paramount for surgeons to have thor-ough knowledge of renal vasculature development and to readily identify these anomalies of renal vasculature on CTA prior to laparoscopic donor nephrectomy. The surgical safety should be analysed on every individual case within the transplant unit. The adverse bleeding event can therefore be prevented.
References1. Li G, Dong J, Lu JS, Zu Q, Yang SX, Li HZ, et al. Anatomical variation of the poste-rior lumbar tributaries of the left renal vein in retroperitoneoscopic left living donor nephrectomy. Int J Urol. 2011; 18:503–9.2. Modi P. Retroperitoneoscopic donor nephrectomy for retroaortic renal vein draining into left common iliac vein. Urology. 2008;71:964–6.3. Wang L, Yang Q, Sheng J, Wu Z, Li M, Liu B, et al. Left laparoscopic radical nephrec-tomy in the presence of a duplicated infe-rior vena cava with complicated anoma-lous tributaries by a transmesocolic approach. Urology. 2012;80:e1–2.4. Rizzari MD, Suszynski TM, Gillingham KJ, Matas AJ, Ibrahim HN. Outcome of living kidney donors left with multiple renal arteries. Clin Transplant. 2012;26:E7–11.5. Lacout A, Thariat J, Marcy PY. Main right renal artery originating from the superior mesenteric artery. Clin Anat. 2012;25:977–8.6. Deak PA, Doros A, Lovro Z, Toronyi E, Kovács JB, Végsö G, et al. The significance of the circumaortic left renal vein and other venous variations in laparoscopic living donor nephrectomies. Transplant Proc. 2011;43:1230–2.7. Rice A, Sethi AS, Sundaram CP. Anoma-lous renal vasculature: a laparoscopic perspective. J Endourol. 2008;22:1577–9.8. Lin CH, Steinberg AP, Ramani AP, Abreu SC, Desai MM, Kaouk J, et al. Laparoscopic live donor nephrectomy in the presence of circumaortic or retroaortic left renal vein. The J Urol. 2004;171:44–6.9. Ang WC, Doyle T, Stringer MD. Left-sided and duplicate inferior vena cava: a
case series and review. Clin Anat. 2013;26:990–1001.10. Mandal AK, Cohen C, Montgomery RA, Kavoussi LR, Ratner LE. Should the indications for laparascopic live donor nephrectomy of the right kidney be the same as for the open procedure? Anoma-lous left renal vasculature is not a contraindiction to laparoscopic left donor nephrectomy. Transplantation. 2001;71: 660–4.11. Fettouh HA. Laparoscopic donor nephrectomy in the presence of vascular anomalies: evaluation of outcome. J Endourol. 2008;22:77–82.12. Wein AJ, Kavoussi LR, Campbell MF. In: Wein AJ, Kavoussi LR, et al. Campbell–Walsh urology. 10th ed. Philadelphia, PA: Elsevier Saunders; 2012.13. Loughna S, Landels E, Woolf AS. Growth factor control of developing kidney endothelial cells. Exp Nephrol. 1996;4:112–8.14. Tufro A, Norwood VF, Carey RM, Gomez RA. Vascular endothelial growth factor induces nephrogenesis and vascu-logenesis. J Am Soc Nephrol. 1999;10: 2125–34.15. Abrahamson DR, Robert B, Hyink DP, St John PL, Daniel TO. Origins and forma-tion of microvasculature in the devel-oping kidney. Kidney Int Suppl. 1998; 67:S7–11.16. Chai JW, Lee W, Yin YH, Jae HJ, Chung JW, Kim HH, et al. CT angiography for living kidney donors: accuracy, cause of misinterpretation and prevalence of vari-ation. Korean J Radiol. 2008;9:333–9.17. Patil UD, Ragavan A, Nadaraj, Murthy K, Shankar R, Bastani B, et al. Helical CT angiography in evaluation of live kidney donors. Nephrol Dial Transplant. 2001; 16:1900–4.18. Pozniak MA, Balison DJ, Lee FT Jr, Tambeaux RH, Uehling DT, Moon TD. CT angiography of potential renal transplant donors. Radiographics. 1998;18:565–87.19. Namasivayam S, Kalra MK, Waldrop SM, Mittal PK, Small WC. Multidetector row CT angiography of living related renal donors: is there a need for venous phase imaging? Eur J Radiol. 2006;59:442–52.20. Miclaus GD, Matusz P. Bilateral quad-ruple renal arteries. Clin Anat. 2012; 25:973–6.21. Neymark E, LaBerge JM, Hirose R, Melzer JS, Kerlan RK Jr, Wilson MW, et al. Arteriographic detection of renovascular disease in potential renal donors: incidence
and effect on donor surgery. Radiology. 2000;214:755–60.22. Rydberg J, Kopecky KK, Tann M, Persohn SA, Leapman SB, Filo RS, et al. Evaluation of prospective living renal donors for laparoscopic nephrectomy with multisection CT: the marriage of minimally invasive imaging with mini-mally invasive surgery. Radiographics. 2001;21 Spec No:S223–36.23. Holden A, Smith A, Dukes P, Pilmore H, Yasutomi M. Assessment of 100 live potential renal donors for laparoscopic nephrectomy with multi-detector row helical CT. Radiology. 2005;237:973–80.24. Sari S, Verim S, Sivrioglu AK, Bozlar U. A rare cause of secondary hypertension: median arcuate ligament compression of the renal artery diagnosed by CT angiog-raphy. BMJ Case Rep. 2013;2013.25. Loukas M, Aparicio S, Beck A, Calderon R, Kennedy M. Rare case of right accessory renal artery originating as a common trunk with the inferior mesen-teric artery: a case report. Clin Anat. 2005;18:530–5.26. Giavroglou C, Kokkinakis H. Main arterial supply of a kidney from the oppo-site renal artery: an unusual case. Acta Radiol. 2005;46:567–8.27. Husted TL, Hanaway MJ, Thomas MJ, Woodle ES, Buell JF. Laparoscopic living donor nephrectomy for kidneys with multiple arteries. Transplant Proc. 2005;37:629–30.28. Kok NF, Dols LF, Hunink MG, Alwayn IP, Tran KT, Weimar W, et al. Complex vascular anatomy in live kidney donation: imaging and consequences for clinical outcome. Transplantation. 2008;85:1760–5.29. Chedid MF, Muthu C, Nyberg SL, Lesnick TG, Kremers WK, Prieto M, et al. Living donor kidney transplantation using laparoscopically procured multiple renal artery kidneys and right kidneys. J Am Coll Surg. 2013;217:144–52; discus-sion 152.30. He B, Mou L, Mitchell A, Delriviere L. Meticulous use of techniques for recon-struction of multiple renal arteries in live donor kidney transplantation. Transplant Proc. 2013;45:1396–8.31. Dean RH, Meacham PW, Weaver FA. Ex vivo renal artery reconstructions: indi-cations and techniques. J Vasc Surg. 1986;4:546-52.32. Sasaki TM, Finelli F, Bugarin E, Fowlkes D, Trollinger J, Barhyte DY, et al.

Page 7 of 7
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
For citation purposes: He B, Hamdorf JM. Clinical importance of anatomical variations of renal vasculature during laparoscopic donor nephrectomy. OA Anatomy 2013 Oct 18;1(3):25.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Review
Is laparoscopic donor nephrectomy the new criterion standard? Arch Surg. 2000;135:943–7.33. Mathews R, Smith PA, Fishman EK, Marshall FF. Anomalies of the inferior vena cava and renal veins: embryologic and surgical considerations. Urology. 1999;53:873–80.34. Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH Jr. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000;20:639–52.35. Olakkengil SA, Rao MM. Evolution of minimally invasive surgery for donor nephrectomy and outcomes. J Soc Lapar-oendosc Surg. 2011;15:208–12.36. Smith PA, Ratner LE, Lynch FC, Corl FM, Fishman EK. Role of CT angiography in the preoperative evaluation for laparo-scopic nephrectomy. Radiographics. 1998;18:589–601.37. Disick GI, Shapiro ME, Miles RA, Munver R. Critical analysis of laparo-scopic donor nephrectomy in the setting of complex renal vasculature: initial expe-rience and intermediate outcomes. J Endourol. 2009;23:451–5.38. Downey RS, Sicard GA, Anderson CB. Major retroperitoneal venous anomalies: surgical considerations. Surgery. 1990; 107:359–65.39. Sundaram CP, Martin GL, Guise A, Bernie J, Bargman V, Milgrom M, et al. Complications after a 5-year experience with laparoscopic donor nephrectomy: the Indiana University experience. Surg Endosc. 2007;21:724–8.40. Hawasli A, Berri R, Meguid A, Le K, Oh H. Total laparoscopic live donor nephrec-tomy: a 6-year experience. Am J Surg. 2006;191:325–9.41. Deak PA, Doros A, Lovro Z, Juhász E, Branstetter G, Kovács JB, et al. Signifi-cance and imaging of lumbar veins and early-branching arteries in planning living-donor laparoscopic nephrectomy: two case reports from 21 months’ experi-ence. Transplant Proc. 2010;42:2347–9.42. Baptista-Silva JC, Verissimo MJ, Castro MJ, Camara AL, Pestana JO.
Anatomical study of the renal veins observed during 342 living-donor nephrectomies. Sao Paulo Med J. 1997;115:1456–9.43. Nicholson ML, Veitch PS. Laparo-scopic live-donor nephrectomy. Nephrol Dial Transplant. 2000;15:1124–6.44. Giordano JM, Trout HH 3rd. Anoma-lies of the inferior vena cava. J Vasc Surg. 1986;3:924–8.45. Friedland GW, deVries PA, Nino-Murcia M, King BF, Leder RA, Stevens S. Congenital anomalies of the inferior vena cava: embryogenesis and MR features. Urol Radiol. 1992;13:237–48.46. Simforoosh N, Beigi FM, Aminsharifi A, Shayaninasab H, Mehrabi S. Left-sided infe-rior vena cava found incidentally during laparoscopic donor nephrectomy: report of three cases. J. Endourol. 2007;21:542–4.47. Nakatani T, Kim T, Naganuma T, Uchida J, Takemoto Y, Sugimura K. Kidney transplants from living related donors having double inferior vena cava. Urol Int. 2004;72:358–60.48. Wu CT, Chiang YJ, Liu KL, Chu SH. Laparoscopic live donor nephrectomy in a patient with duplex inferior vena cava. Transplant Proc. 2004;36:1912–3.49. Fronek JP, Morsy MA, Singh U, Chemla E, Chang RW. Retroperitoneoscopic live donor nephrectomy in a patient with a double inferior vena cava. J Laparoendosc Adv Surg Tech A. 2006;16:378–80.50. Davari HR, Malek-Hosseini SA, Salahi H, Bahador A, Nikeghbalian S, Jalaeian H, et al. Management of infrarenal dupli-cated inferior vena cava during living related kidney transplantation. Transpl Int. 2007;20:478–9.51. Cheng D, Zangan SM. Duplication of the inferior vena cava in a patient presenting for IVC filter placement. J Vasc Access. 2010;11:162–4.52. Nanda S, Bhatt SP, Turki MA. Inferior vena cava anomalies–a common cause of DVT and PE commonly not diagnosed. Am J Med Sci. 2008;335:409–10.53. Davis CJ Jr, Lundberg GD. Retroaortic left renal vein, a relatively frequent anomaly. Am J Clin Pathol. 1968;50:700–3.
54. Kraus GJ, Goerzer HG. MR-angio-graphic diagnosis of an aberrant retroaortic left renal vein and review of the literature. Clin Imaging. 2003; 27:132–4.55. Koc Z, Ulusan S, Oguzkurt L, Tokmak N. Venous variants and anomalies on routine abdominal multi-detector row CT. Eur J Radiol. 2007;61:267–78.56. Karaman B, Koplay M, Ozturk E, Basekim CC, Ogul H, Mutlu H, et al. Retroaortic left renal vein: multidetector computed tomography angiography find-ings and its clinical importance. Acta Radiol. 2007;48:355–60.57. Schmidt GP, Loeweneck H. [Frequency of the retroaortic left renal vein in adults (author’s transl)]. Urol Int. 1975;30: 332–40.58. Trigaux JP, Vandroogenbroek S, De Wispelaere JF, Lacrosse M, Jamart J. Congenital anomalies of the inferior vena cava and left renal vein: evaluation with spiral CT. J Vasc Interv Radiol. 1998;9: 339–45.59. Kawamoto S, Montgomery RA, Lawler LP, Horton KM, Fishman EK. Multi-detector row CT evaluation of living renal donors prior to laparoscopic nephrec-tomy. Radiographics. 2004;24:453–66.60. Kim JK, Park SY, Kim HJ, Kim CS, Ahn HJ, Ahn TY, et al. Living donor kidneys: usefulness of multi-detector row CT for comprehensive evaluation. Radiology. 2003;229:869–76.61. Urban BA, Ratner LE, Fishman EK. Three-dimensional volume-rendered CT angiography of the renal arteries and veins: normal anatomy, variants, and clin-ical applications. Radiographics. 2001; 21:373–86; questionnaire 549–55.62. Turkvatan A, Ozdemir M, Cumhur T, Olcer T. Multidetector CT angiography of renal vasculature: normal anatomy and variants. Eur Radiol. 2009;19:236–44.63. Schlunt LB, Harper JD, Broome DR, Baron PW, Watkins GE, Ojogho ON, et al. Improved detection of renal vascular anatomy using multidetector CT angiog-raphy: is 100% detection possible? J Endourol. 2007;21:12–7.

![Laparoscopic Partial Nephrectomy Current State of the ArtClayman et al described the first successful laparoscopic nephrectomy in 1991 [1]. Since that time, laparoscopic radical nephre](https://static.fdocuments.in/doc/165x107/5fed387e0ff39d41a809e8a1/laparoscopic-partial-nephrectomy-current-state-of-the-art-clayman-et-al-described.jpg)