CLIENT HANDBOOK - Shining Horizons...General Information Shining Horizons Therapeutic Riding...
22
CLIENT HANDBOOK
Transcript of CLIENT HANDBOOK - Shining Horizons...General Information Shining Horizons Therapeutic Riding...
CLIENT HANDBOOK
This booklet contains the following information:
Introduction Page 2
General information Page 3-4
Benefits to riders, Program schedules Page 5
Certification Page 6
Hints from Occupational Therapist Page 7
Emergency accident plan Page 8
Fire plan Page 9
Rider registration and release forms Appendix A
Bodily contact form Appendix B
Stable release form Appendix C
Physician referral form Appendix D
Atlanto-axial x-ray form Appendix E
Stable fire plan/map Appendix F
Summary form Appendix G
Contact information:
Instructors:
Stacey Hope 506-721-3266 (text messages)
506-652-3872 [email protected]
Tomalyn Comeau 506-642-2605 [email protected]
New rider co-ordinator:
Ann Bone 506-721-8468 [email protected]
Parent liaison:
Eric Daley 506-696-6541 [email protected]
General inquiries: [email protected]
Associated sites:
www.cantra.ca, www.shtra.ca and on
www.facebook.com/ShiningHorizonsTherapeuticRidingAssociation
Pg 1

Introduction
Shining Horizons Therapeutic Riding Association (SHTRA) is delighted that
you are interested in finding out more about our organization.
Horseback riding for mentally and physically challenged people is recognized
throughout the world as an excellent form of therapeutic recreation. Riders
benefit from the program by successes in learning, confidence, skills and self
esteem. The SHTRA program is based on longstanding, scientifically based
evidence. On horseback, many riders are able to experience mobility far
beyond their own physical capabilities.
The people that make up SHTRA include instructors, physiotherapists, and
volunteers in many guises: leaders (of the horse), sidewalkers,
parent/caregiver liaisons, volunteer coordinators, fundraisers, and arena
helpers.
Parents and caregivers also play a major role in the operation of SHTRA by
having the rider dressed appropriately for the lesson and the weather
conditions and at the facility at least ten minutes before the lesson is
scheduled to begin. This ensures there will be time to prepare the rider by
having their safety equipment properly fitted. In the event a rider will not be
able to attend a scheduled lesson, please contact the parent liaison or
instructor as soon as possible. It is also important that the parent/caregiver
wear appropriate footwear. Sandals and high heels are not permitted in the
arena. Parents and caregivers must remain on the property during the lesson.
When the facility has a viewing room, this is the recommended waiting area. It
is permissible to wait in the arena if there is no viewing room.
Pg 2
General Information
Shining Horizons Therapeutic Riding Association (SHTRA) was established
in 1996. Our objective is to provide a horseback riding program for mentally
and physically challenged people as a source of enjoyment, therapeutic
exercise, and recreational sport. SHTRA currently operates out of Foshay
South Eventing Inc., 21 Gallagher Road, Lakeside, NB E5N 7K2.
Basic criteria for rider eligibility:
Must have a disability, either physical or cognitive
Must be able to stay on the horse for the entire lesson
Parent/caregiver must be able to stay for the entire lesson
Must have permission from attending physician
Must have specific goals that will improve physical, cognitive and/or
psychosocial impairments
Must not display inappropriate behaviours which could lead to placing
self or others at risk
Must be able to tolerate all approved safety equipment for the entire
lesson
For information on rider eligibility and space availability please contact the
‘New rider co-ordinator’ (information found on page 1).
For any rider who requires an Epi-Pen®, it must be brought to each lesson
and be immediately available if needed.
Appendices A, B, C, D, G and if applicable E, must be completed in their
entirety and submitted, following the rider’s tentative acceptance into the
program, 2 weeks prior to attending the first lesson.
Because SHTRA is a charitable organization, there is a cost associated for
the lessons. For information on the cost, please contact our ‘New rider
coordinator’ (information found on page 1).
Pg 3
Unless otherwise arranged, fees are required to be paid by the beginning of
each session. This allows for purchase or replacement of required
equipment.
If you require financial assistance, there are several local programs that
accept applications for supplementing recreational activities.
Recreation NB-Inclusive Recreation Activity Fund: Exclusive to
persons with disabilities. www.recreationnb.ca/programs-and-initiatives
PRO Kids: Assists with cultural and sport/recreation activities and is
exclusive to low income families. www.prokidssj.ca/main.html
Canadian Tire Jumpstart: Similar to and administered by SJ PRO
Kids. Exclusive to low income families to reduce financial barriers to
sport participation. Contact SJ PRO Kids manager for more
information. [email protected]
Kidsport : A provincial program administered by Sport NB to assist low
income families in reducing financial barriers exclusively to sport
participation in areas where similar organizations do not exist.
www.kidsportcanada.ca/new-brunswick/
Pg 4
Benefits to Riders Being a rider in a therapeutic riding program gives a sense of
achievement, as riders improve their physical condition and all around well
being. There is a strong positive attitude. The program makes it possible
for mentally and physically challenged persons to enjoy a unique form of
therapy and recreation.
Horseback riding for mentally and physically challenged persons is
recognized throughout the world as an excellent form of therapeutic
recreation. Riders benefit from the program by successes in learning,
confidence, skills and self esteem. The SHTRA program is based on
longstanding, scientifically based evidence. On horseback, many riders are
able to experience mobility far beyond their own physical capabilities.
I acknowledge the risks and potential for risks of a horseback riding
program. However the possible benefits are greater than the risk assumed.
Program Schedule
There are two sessions of five to eight weeks each year, one in the
spring, and one in the fall. Lessons are given on Tuesday through Friday
evenings, and on Saturday mornings. Lessons are between thirty and
sixty minutes in duration, and there are between three to five lessons per
day. Lessons are dependent on the soundness of the horse(s), and
availability of volunteers. Unfortunately for these reasons, it may
sometimes be necessary to cancel a lesson. The parent or caregiver will
be notified by either the instructor or a parent liaison in the event of a
cancellation. If the rider will be unable to attend a lesson, please notify the
instructor or a parent liaison as soon as possible. Fees are non-
refundable once a session has started.
Pg 5
Certification
Canadian Therapeutic Riding Association (CanTRA) is the governing
body for therapeutic riding organizations across Canada. They set forth
a set of strict rules and guidelines regarding the facility, the instructors
and the volunteers.
The facility must undergo a rigid safety inspection every five years. The
local organization pays a fee for this inspection, and also pays liability
insurance to CanTRA. All instructors and volunteers must undergo a
criminal background check.
Instructors must act as a volunteer for a minimum of 50 hours
before they can begin the training program. They must complete a
rigorous training program and then pass certification by CanTRA to be
allowed to teach in a therapeutic riding program. The instructors also
attend workshops on a regular basis to keep current with their
counterparts across Canada, and ensure they have the latest ‘best
practice’ information for this field.
Volunteers in the SHTRA undergo a thorough training program to
ensure the safety of the riders. They attend training sessions where they
are taught safe handling practices for the rider and the horse, facility
safety rules, and specialized procedures to follow in the event of a fire or
accident. They are taught how to ensure the safety of the rider both on
the ground, and on the horse, and to monitor their condition. They
respect the confidentiality of the riders and their parents/caregivers and
do not discuss them outside the facility or the needs of the lesson. They
are considerate of other people’s conditions and do not wear products
that may trigger allergic reactions such as scented or latex products.
Pg 6

Helpful Hints From Occupational Therapists
1. The rate of progress of a rider is measured in months or years.
2. The rate of progress of a rider is not always a reflection on the instructor
or team of volunteers. It is frequently dependent on the disability.
3. Be aware of the rider’s endurance as fatigue may occur, resulting in a
negative outcome, both physically and mentally. Relaxation, enjoyment
and learning to ride go hand in hand.
4. A change of activity will keep the rider engaged.
5. Keep to the basics since the rider must learn balance and gain
confidence. Have the rider keep one hand on the pommel strap at the
trot since using the reins for balance does not encourage a proper seat
for any rider.
6. Encourage and praise the effort as much as the action.
7. A change of horse is often for therapeutic reasons, and the rider should
not feel demoted.
8. Do not compare riders to each other. Each rider’s progress will be
different.
9. The support that each rider requires is unique to that individual.
10.Touching and supporting the rider is an intimate action and should be
done with the greatest respect for the rider’s dignity and sense of
personal ability.
Pg 7
Emergency Accident Plan
The following is the procedure to be followed in the event of an accident or
unusual occurrence during a lesson:
1. The Instructor will call the entire ride to a halt.
2. Each leader and all sidewalkers will stay with their assigned horse and
rider.
3. The Instructor will go to the rider in difficulty.
4. The Instructor will determine which sidewalkers should assist, and only
the Instructor will give directions and instructions. Parents/caregivers
and spectators may be requested to help.
5. The Instructor will send for a first aid kit and blanket if necessary.
6. Depending on the severity of the incident, no one is to move the rider or
remove their helmet. A volunteer may be requested to call 911 for an
ambulance.
7. The Instructor should stay with the rider in difficulty, and if the incident is
more than a minor injury, the remaining riders should be dismounted.
The Instructor will decide if they need to stay with the rider in difficulty,
or supervise the dismounting.
8. If the injury is minor, the rider in difficulty may sit out for a while, and the
lesson will continue for other riders. The injured rider may continue the
lesson, or wait until the next lesson to resume riding.
9. When a rider has fallen, it is imperative that they go to the hospital, or
be checked by either their attending physician.
10. The Instructor will always complete an incident report. If the
parent/caregiver or rider refuses medical attention, this must be noted
on the incident form.
It is crucial that everyone involved remains calm, and follows the
Instructor’s directions.
Pg 8
Action in the Event of a Fire
The following is the procedure to be followed in the event of a fire on the
property:
1. The person who discovers the fire is to advise the Instructor and stable
management or staff and call 911 immediately.
2. The Instructor will call the ride to a halt, and commence the evacuation
process for the riders, volunteers, and horses in use.
3. If the riders are mounted, volunteers are to remove the riders from the
horses, under supervision of the Instructor. Under emergency
conditions, use of the mounting block is not necessary. Riders can be
lifted or helped to slide off. Riders, volunteers and parents are to
proceed to the parking area beside the barn. From the arena, exit via
the arena doors. Do not go through the barn. Sidewalker volunteers are
to remain with the rider at all times.
4. Assigned leaders of horses are to bring the animals they are
responsible for outdoors, and remove the tack and place them in a
paddock, unless otherwise instructed.
5. Instructor must ensure the call to 911 has been made, and designate a
person to direct the fire department responders to the location of the
fire.
6. Fire fighting by volunteers is only to be under taken with direction from
the Instructor or stable management.
7. Perform a head count to ensure all people have been evacuated.
It is crucial that everyone involved remains calm, and follows the
Instructor’s directions.
Pg 9
Rider Registration Form
Rider Information:
Name: _____________________________ Date of Birth:________
Address: ______________________________________________
Phone: (h)____________ (c)______________(w)______________
Email: ________________________________________________
Parent/Caregiver: _______________________________________
Address: ______________________________________________
Phone: (h)____________ (c)______________(w)______________
Email: ________________________________________________
Emergency contact:
1. Name: _____________________________ Phone: __________
2. Name: _____________________________ Phone: __________
LIABILITY RELEASE
__________________________________________(name) would like to
participate in the Shining Horizons Therapeutic Riding Program. I
acknowledge the risks and potential for risk in horseback riding. However I
feel that the possible benefits to myself/ my child/ my ward are greater than
the risk assumed. I hereby intend to be legally bound for myself, my heirs
and assigns, executors or administrators, waive and release forever, all
claims for damage against the Shining Horizons Therapeutic Riding
Program, it’s Board of Directors, Instructors, Therapists, Aids, Volunteers
and/or Employees for any and all injuries and/or losses that I/ my child/ my
ward may sustain while participating in Shining Horizons Therapeutic
Riding Program.
Signature:_______________________________ Date:______________
Witness:________________________________ Date:______________
Appendix A: Pg 1
Photo Release Form I hereby consent to authorize the use and reproduction, by Shining
Horizons Therapeutic Riding Association, of any and all photographs
and/or any other audiovisual materials taken of me/ my child/ my ward, for
promotional printed material, educational activities, exhibitions, or for any
other use for the benefit of the program.
Signature (rider, parent or caregiver):__________________________
Date:____________________________________________________
Appendix A: Pg 2
Consent for Release of Information Form
I hereby authorize ___________________________ (person or facility) to
release information from the records of ___________________________
(prospective rider’s name). The information is to be released to Shining
Horizons Therapeutic Riding Program for the purpose of developing a
Therapeutic Riding Program for the above named prospective rider.
The information to be released is indicated below.
Medical history Yes ( ) No ( )
Physiotherapy evaluation, assessment and program plan Yes ( ) No ( )
Occupational therapy evaluation,assessment and program planYes( )No( )
Speech therapy evaluation, assessment and program plan Yes ( ) No ( )
Classroom Individual Education Plan (I. E. P.) Yes ( ) No ( )
Other________________________________________ Yes ( ) No ( )
Signature (rider, parent or caregiver):____________________________
Date:______________________________________________________
Appendix A: Pg 3
Information Release Form
I hereby authorize Shining Horizons Therapeutic Riding Program to
release to it’s instructors and helpers such information as may be
necessary to conduct a beneficial and safe Therapeutic Riding Program.
Name of rider:____________________________________________
Signature (rider, parent or caregiver):__________________________
Relationship to the rider: ____________________________________
Witness:_________________________________________________
Date:____________________________________________________
Appendix A: Pg 4
DEGREE OF BODILY CONTACT WHEN WORKING WITH RIDERS
Due to the nature of the activity at Shining Horizons Therapeutic Riding Association, it
is understood that instructors and trained volunteers will need to assist the majority of
riders when mounting or riding a horse.
It may be necessary to lift a rider onto the horse, or correct posture by placing hands
at the front or back of the trunk of the rider, or to correct leg and hand positions.
It is understood that this is part of the therapy/recreation sessions to which
parents/caregivers and riders have consented.
During riding lessons it may be necessary to quickly remove the rider from the horse
due to safety concerns. This is done for the well being of all concerned, and may
involve two volunteers lifting the rider.
Any bodily contact provided by the trained staff or personal care workers is in the
interest of providing a safe and fun environment for the riders and will be undertaken
with the utmost discretion.
Many of the riders who participate in the Shining Horizons Therapeutic Riding program
like to give hugs. This will be monitored by the staff so that other riders will not be
placed in an embarrassing situation and behaviour will be monitored as deemed
necessary by the staff.
I have read and understood and agree to the terms above.
Rider:__________________________ Parent/guardian:__________________
Witness:_______________________ Date:___________________________
Appendix B

Appendix C: Pg 1

Appendix C: Pg 2

Physician Referral Form
Prospective Rider Information:
Name:_______________________________________________
Date of Birth:__________________________________________
Address:______________________________________________
Phone: (h)____________ (c)______________(w)_____________
Parent/Caregiver:_______________________________________
Living arrangement: Home ( ) Other ( ) Details:______________
______________________________________________________
Medical background:
Primary diagnosis:_______________________________________
Secondary diagnosis:_____________________________________
Height:_____________ Weight:____________ Gender:__________
Diabetic:___________ Insulin:_____________ Epileptic:_________
If epileptic, frequency of seizures:____________________________
Date of last seizure: ______________________________________
Medications and indications:________________________________
_______________________________________________________
Communicable diseases: Yes( ) No( ) If yes, details:____________
________________________________________________________
Surgery and dates: ________________________________________
________________________________________________________
Appendix D: Pg 1
General physical condition:
Ambulatory: Yes( ) No( ) Details:____________________________
________________________________________________________
Muscle tone: (Spasticity, flaccidity, etc.)
Tone in upper extremities: ___________________________________
Tone in lower extremities: ___________________________________
Tone in trunk: ____________________________________________
Balance: Sitting__________ Standing__________ Walking_________
Communication: Spoken__________ Sign language_______________
Speech: Good ___________ Fair____________ Poor______________
Ability to understand: Good ________ Fair _________ Poor _________
Sensory function: Sight _________ Hearing_______ Tactile_________
Continence: _______________________________________________
Allergies:__________________________________________________
Comments:________________________________________________
_________________________________________________________
Physician’s Permission:
I hereby give my permission for the above individual, _______________
to participate in the Shining Horizons Therapeutic Riding Program.
Physician’s name (print):______________________________________
Physician’s signature: ________________________________________
Date:______________________________________________________
Physician’s address: _________________________________________
_________________________________________________________
Phone: _____________________ Fax: ________________________
Note: It is important that this form be filled out completely and in detail, in order for the
instructor and physiotherapist to match the rider with the mount.
Appendix D: Pg 2
ATLANTO-AXIAL X-RAY VERIFICATION FOR RIDERS
WITH DOWN SYNDROME
Rider Information:
Rider: _____________________________ Date of Birth:________
Address: ______________________________________________
Phone: (h)____________ (c)______________(w)______________
Height: ____________________ Weight: ____________________
Physician Information:
Physician: _____________________________________________
Phone:______________________ Fax: _____________________
Date of X-ray: __________________________________________
Result of X-ray:__________________________________________
Physician’s signature:_____________________________________
Date: __________________________________________________
Note: Due to the nature of this activity, persons diagnosed with Down Syndrome
cannot be accepted for riding instruction without proof of a negative diagnostic X-ray
for Atlanto-Axial instability. This form must be accompanied by a signed and dated
statement from a qualified physician giving the date and result of the diagnostic X-ray.
Appendix E
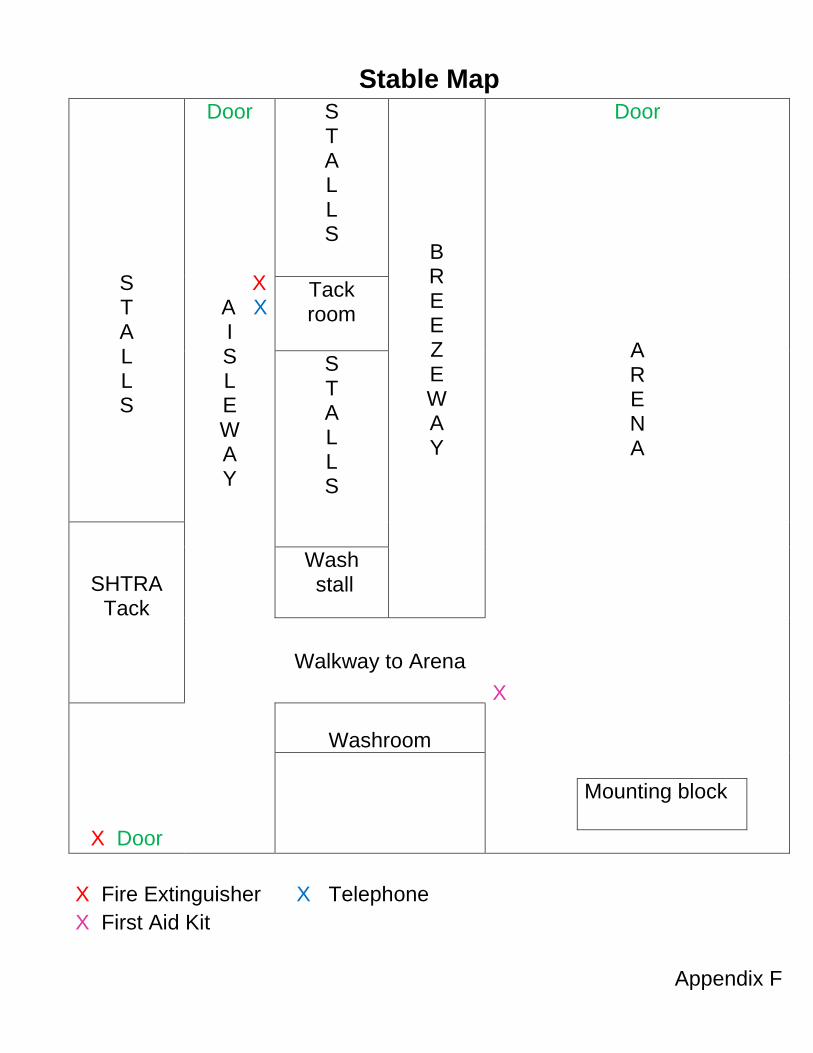
Stable Map
S T A L L S
Door
X A X
I S L E W A Y
S T A L L S
B R E E Z E W A Y
Door
A R E N A
X
Mounting block
Tack room
S T A L L S
SHTRA Tack
Wash stall
Walkway to Arena
X Door
Washroom
X Fire Extinguisher X Telephone
X First Aid Kit
Appendix F
SUMMARY FORM
Rider:_______________________________________________ (To be submitted at least two weeks before first scheduled lesson)
I have attached the completed applicable forms:
Rider registration and release forms Stable release form
Bodily contact form Physician referral form
Atlanto-axial x-ray form (If applicable)
I have paid or made payment arrangements (receipt attached):
o Cash o Certified cheque
o Money order o E payment
o Other( Please specify):
Because there is a waiting list, I understand not having the above information
and funding in place may cause my application to be delayed, to allow the
other applicants access to the program.
I have read the Shining Horizons Therapeutic Riding Association Rider
handbook, and understand and agree to the content.
_______________________________________________________ (Name, print and sign)
_______________________________________________________ (Witness, print and sign)
_______________________________________________________ (Date)
Appendix G