Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
8
EDUCATIONAL OBJECTIVE: Readers will dierentiate the pharmacology, eectiveness, and uses o the thienopyridine drugs Prasugrel for acute coronary syndromes: Faster , more potent, but higher bleeding risk AbstrAct Prasugrel (Efent) has been approved or reducing the risk o thrombotic complications in patients with acute coronary syndromes who are to undergo percutaneous coronary intervention. In a large clinical trial (N Engl J Med 2007; 357:2001–2005), prasugrel was superior to clopidogrel (Plavix), another drug o its class, in this situ‑ ation. However , bleeding complications we re more re‑ quent with prasugrel, and so this drug should be avoided in patients at higher risk o bleeding. Key Points The thienopyridines—ticlopidine (Ticlid), clopidogrel (Plavix), and now prasugrel—reduce the risk o death rom and serious complications o acute coronary syn‑ dromes by inhibiting platelet aggregation. Compared with clopidogrel, prasugrel is more potent, aster in onset, and more consistent in inhibiting plate‑ lets. Prasugrel should be avoided in patients at higher risk o bleeding, including those with a history o stroke or transient ischemic att ack, those age 75 or older , or those who weigh less than 60 kg. CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009 707 P rasugrel (Efnt) i mo potnt nd conitnt in it ct thn copido (Pvix), th pvntin mo thombotic vnt—bt t pic o mo bdin. Th- o, th d mt b ppopity ctd o th individ ptint. Ov th t 9 y, th thinopyidin— ticopidin (T icid), copido, nd now p- —hv bcom nti too o tt- in ct coony yndom. Th ndyin mchnim o ct coony yndom i thomboi, cd by pt o thocotic pq. 1 Accodiny, ntithombotic nt—piin, hpin, ow- moc-wiht hpin, ycopotin IIb/III inhibito, th dict thombin inhibito bivi- din (Aniomx), nd thinopyidin—hv bn hown to dc th ik o mjo d- v cdic otcom in thi ttin. In thi tic, w viw th phmcooy nd vidnc o ctivn o th thinopyi- din d, ocin on p, th tt thinopyidin to b ppovd by th US Food nd D Adminittion (FDA). Thienopyridines inhibiT plaTeleT acTiva Tion and aggregaTion Thinopyidin pod tht qi con- vion by hptic cytochom P450 nzym. Th ctiv mtboit bind iviby to ptt P2Y12 cpto. Conqnty, thy pmnnty bock inin mditd by ptt dnoin diphopht-P2Y12 cp- to, thby inhibitin ycopotin IIb/III cpto ctivtion nd ptt tion. cUrrent DrUG tHerAPy doi:10.3949/ccjm.76a.09116 CREDIT CME Lawrence D. Lazar, MD Department o Cardiovascular Medicine, Cleveland Clinic a. MichaeL Lincoff, MD Proessor o Medicine; Vice Chairman, Depart‑ ment o Cardiovascular Medicine; Director, Center or Clinical Research, Lerner Research Institute; Director, Cleveland Clinic Coordinat‑ ing Center or Clinical Research, Department o Cardiovascular Medicine, Cleveland Clinic
-
Upload
vansal-liu -
Category
Documents
-
view
218 -
download
0
Transcript of Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 1/8
EDUCATIONAL OBJECTIVE: Readers will di erentiate the pharmacology, e ectiveness, and uses o thethienopyridine drugs
Prasugrel for acute coronarysyndromes: Faster, more potent,but higher bleeding risk
AbstrActPrasugrel (E fent) has been approved or reducing therisk o thrombotic complications in patients with acutecoronary syndromes who are to undergo percutaneouscoronary intervention. In a large clinical trial (N Engl JMed 2007; 357:2001–2005), prasugrel was superior toclopidogrel (Plavix), another drug o its class, in this situ‑ation. However, bleeding complications were more re‑quent with prasugrel, and so this drug should be avoidedin patients at higher risk o bleeding.
Key PointsThe thienopyridines—ticlopidine (Ticlid), clopidogrel(Plavix), and now prasugrel—reduce the risk o death
rom and serious complications o acute coronary syn‑dromes by inhibiting platelet aggregation.
Compared with clopidogrel, prasugrel is more potent,aster in onset, and more consistent in inhibiting plate‑
lets.
Prasugrel should be avoided in patients at higher risko bleeding, including those with a history o stroke ortransient ischemic attack, those age 75 or older, or thosewho weigh less than 60 kg.
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009 707
P rasugrel (E f nt) i mo pot nt ndcon i t nt in it ct th n c opido(P vix), th p v ntin mo th ombotic
v nt —b t t p ic o mo b din . Tho , th d m t b pp op i t y o th individ p ti nt.
Ov th t 9 y , th thi nopy idintic opidin (Tic id), c opido , nd now p
—h v b com nti too oin c t co on y ynd om .
Th nd yin m ch ni m o cco on y ynd om i th ombo i , c d
pt o th o c otic p q .1 Acco din y,ntith ombotic nt — pi in, h p in, owmo c -w i ht h p in, ycop ot in IIb/Iinhibito , th di ct th ombin inhibito biv i-
din (An iom x), nd thi nopy idin —h v b n hown to d c th i k o m jo
v c di c o tcom in thi ttin .In thi tic , w vi w th ph m co o
nd vid nc o ctiv n o th thi nopydin d , oc in on p , th thi nopy idin to b pp ov d by th US Food
nd D Admini t tion (FDA).
Thienopyridines inhibiT plaTeleTacTivaTion and aggregaTion
Thi nopy idin p od th t q i cv ion by h p tic cytoch om P450 nzymTh ctiv m t bo it bind i v ib y p t t P2Y12 c pto . Con q nt y, thp m n nt y b ock i n in m di t d p t t d no in dipho ph t -P2Y12 cto , th by inhibitin ycop ot in IIb/III
c pto ctiv tion nd p t t tio
cUrrent DrUG tHerAPy
doi:10.3949/ccjm.76a.09116
CREDITCME
Lawrence D. Lazar, MDDepartment o Cardiovascular Medicine,Cleveland Clinic
a. MichaeL Lincoff, MDPro essor o Medicine; Vice Chairman, Depart‑ment o Cardiovascular Medicine; Director,Center or Clinical Research, Lerner ResearchInstitute; Director, Cleveland Clinic Coordinat‑ing Center or Clinical Research, Department o Cardiovascular Medicine, Cleveland Clinic

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 2/8
708 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009
PrAsUGrel
A pi in, in cont t, inhibit p t t byb ockin th th ombox n -m di t d p thw y.Th o , th combin tion o pi in p thi nopy idin h n dditiv ct.2
Th ct o thi nopy idin on p t t ii v ib . Th o , tho h th h - io p ’ ctiv m t bo it i 3.7 ho , itinhibito y ct t o 96 ho , nti yth tim o h th body’ ci c tin p t -
t to b p c d.
Ticlopidine,The irsT Thienopyridine
Tic opidin w th f t thi nopy idin to bpp ov d by th FDA. It initi t di inn t b n in w m , th i d i n did
not c o p ti nt to conc nt y c ivpi in, nd th y how d w th t tic opi-
din w bo t b n fci pi in. Con -q nt y, th t di h d itt imp ct on c ini-c p ctic .3
In pivot t i ,4 p ti nt who c iv dco on y t nt w ndomiz d to t w d
c iv ith th combin tion o tic opidinp pi in o ntico tion th py withh p in, ph np oco mon ( co m in d iv -tiv v i b in E op ), nd pi in. At 30d y , n i ch mic comp ic tion (d th, myo-c di in ction [MI], p t int v ntion)h d occ d in 6.2% o th ntico -tion th py o p v 1.6% o th tic opidin
o p, i k d ction o 75%. R t o t ntocc ion, MI, nd v c iz tion w80% to 85% ow in th tic odipin o p.Thi t dy p v d th w y o wid p d o thi nopy idin .
Tic opidin ’ w imit d, how v , by 2.4% incid nc o io n ocytop nind c o th ombocytop nic p p .
bene iT o clopidogrel
A tho h p i th oc o thi vi w,th t i o p comp d it fc cywith th t o c opido . F th mo , m nyp ti nt ho d ti c iv c opido ndnot p , o it i impo t nt to b mi iwith th vid nc o c opido ’ b n ft.
Onc pp ov d o c inic , c opidow b tit t d o tic opidin in p ti nt n-
d oin co on y t ntin on th b i o t d-
i howin it to b t t ctiv tpidin nd mo to b . A i o t ic opido w don in p ti nt c o t m o i k o p , om tho t hi h i
co on y h t di to tho p ntin wST- v tion MI. Th tim o p t tm nt inth t di n d om 3 ho to 6 d y bp c t n o co on y int v ntion, nd thd tion o t tm nt o owin int v nti
n d om 30 d y to 1 y .
c -sT- tt m
The CURE trial 2 (C opido in Un-t b An in to P v nt R c nt Ev nt
p b i h d in 2001, t b i h d c opido th py o n t b i ch mic ynd om
wh th t t d m dic y o with viz tion. In th t t i , 12,562 p ti nt with
c t co on y ynd om witho t ST vtion (i , n t b n in o non-ST- v tionMI), d fn d by ct oc dio phic ch n
o po itiv c di c m k , w ndiz d to c iv c opido ( 300-m o dido o ow d by 75-m m int n nc doo p c bo o m n d tion o 9 monthA p ti nt o c iv d pi in 75 m to m d i y.
Th compo it o tcom o d th omc diov c c , non t MI, o occ d in 20% w p ti nt t t d wic opido th n with p c bo (9.3% v11.4%). Th b n ft w imi in p ti nt
nd oin v c iz tion comp d wtho t t d m dic y.
A tho h th w i nifc nt y moc o m jo b din in th c opido
o p th n in th p c bo o p (3.7% v2.7%), th n mb o pi od o i -th
nin b din o h mo h ic t ok wm .
PCI-CURE 5 w b t dy o th CUREt i in p ti nt who nd w nt p c t no co on y int v ntion. P ti nt w pt t d with c opido o p c bo o mo 6 d y b o th p oc d . A t wth y c iv d c opido p pi in
nb ind d hion o 2 to 4 w k , nd thth ndomiz d t dy d w m d m n o 8 month .
Si nifc nt y w dv v nt o
c d in th c opido o p t i
clop dogreland prasugrelare prodrugs
ha requ reonvers on
by P450enzymes

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 3/8
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009 709
lAzAr AnD linco
th tim o th int v ntion, 1 month t ,nd 8 month t .
c sT- t t Mi
The CLARITY-TIMI 28 trial 6 (C o-pido Adj nctiv R p ion Th -py—Th ombo y i in Myoc di In ction28) how d th t ddin c opido ( 300-m
o din do , th n 75 m d i y) to pi in b n-ftt d p ti nt with ST- v tion MI c ivin
fb ino ytic th py. At 30 d y , c diov cd th, c nt MI, o nt v c iz -tion h d occ d in 11.6% o th c opido
o p v 14.1% o th p c bo o p, t -ti tic y i nifc nt di nc . Th t o m jo o mino b din w no hi h in thc opido o p th n in th p c bo o p,
n p ci y m k b fndin in p ti ntc ivin th ombo ytic th py.
PCI-CLARITY. 7 Abo t h o th p -ti nt in th CLARITY t i tim t y nd -w nt p c t n o co on y int v ntion
t fb ino ytic th py, with t po t d th PCI-CLARITY b t dy. Lik tho in
PCI-CURE, th p ti nt w ndomiz dto c iv p t tm nt with ith c opid-o o p c bo b o th p oc d , in thi
t dy o m di n o 3 d y . Both o p -c iv d c opido t w d. At 30 d y om
ndomiz tion, th o tcom o c diov cd th, MI, o t ok h d occ d in 7.5% o th c opido o p comp d with 12.0% o th p c bo o p, which w t ti tic y i -nifc nt, witho t ny i nifc nt xc in th
t o m jo o mino b din . COMMIT 8 (th C opido nd M to-p o o in Myoc di In ction T i ) o
how d c opido to b b n fci in p ti ntwith c t MI. Thi t i inc d d mo th n45,000 p ti nt in Chin with c t MI, 93%o whom h d ST- m nt v tion. In con-t t to CLARITY, in COMMIT b y moth n h o th p ti nt c iv d fb ino y i ,
w th n 5% p oc d d to p c t n o in-t v ntion , nd no o din do w iv n:p ti nt in th c opido o p c iv d 75m /d y om th o t t.
At 15 d y , th incid nc o d th, in c-tion, o t ok w 9.2% with c opido com-p d with 10.1% with p c bo, m b t t -ti tic y i nifc nt di nc . A in, th t
o m jo b din w not i nifc nt y hi h ,
ith ov o in p ti nt ov 70.O not , p ti nt ov 75 w x-
c d d om CLARITY, nd m ntion d, noo din do w d in COMMIT. Th , o
p ti nt c ivin fb ino y i who ov 75, th i no vid nc to ppo t th tyo o din do , nd c opido ho d b
t t d t 75 m d i y.
c tt t t
The CREDO trial 9 (C opido o thR d ction o Ev nt D in Ob v tion) win p ti nt d o ctiv p c t n oco on y int v ntion. Th to 24 ho b -
o th p oc d , th p ti nt c iv d ith 300-m o din do o c opido o p -
c bo; t w d, p ti nt c iv d c opid-o 75 m /d y o 28 d y . A p ti nt o
c iv d pi in.A c opido o din do 3 to 24 ho
b o th int v ntion did not p od c t ti tic y i nifc nt d ction in i ch micv nt , tho h po t hoc b o p n y i
t d th t p ti nt who c iv d th o d-in do b tw n 6 nd 24 ho b o didb n ft, with tiv i k d ction o 38.6%in th compo it nd point (P = .051).
A t 28 d y , th p ti nt who h d -c iv d th c opido o din do w con-tin d on c opido , whi tho in th p -c bo o p w witch d b ck to p c bo. At1 y , th inv ti to o nd i nifc nt y
ow t o th compo it nd point withth p o on d co o c opido (8.5% v11.5%). In summary, th t di o nd c opid-o to b b n fci in b o d p ct m o co on y di . S b o p n y tth t p t tm nt b o p c t n o co o-n y int v ntion p ovid ddition b n-
ft, p tic y i c opido i iv n t t6 ho in dv nc (th tim n c y oc opido to c b t nti p t t inhi-bition).
soMe paTienTs respond lessTo clopidogrel
Th v o p t t inhibition ind c d byc opido v i . In di nt t di , th
q ncy o c opido “non pon iv n ”
clop dogrels benef aln a spe rum
o oronaryd sease

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 4/8
710 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009
PrAsUGrel
n d om 5% to 56% o p ti nt , d p nd-in on which t t nd which c to vw d. Th di t ib tion o pon toc opido i wid nd ft no m i n
c v .10A ction o th pop tion c i
n th t m y cco nt o om o th in-t p ti nt v i tion in p t t inhibition withc opido . C i o d c d- nctionCYP2C19 — pp oxim t y 30% o p o-p in on t dy—h v i nifc nt y ow v-
o th ctiv m t bo it o c opido , p t t inhibition om c opido th py,
nd 53% hi h t o d th om c dio-v c c , MI, o t ok .11
prasugrel,The newesT Thienopyridine
P , FDA- pp ov d in J y 2009 o tht tm nt o c t co on y ynd om , i iv-
n in n o o din do o 60 m o ow dby n o m int n nc do o 10 m d i y.
p m A not d p vio y, th thi nopy idin p od th t q i h p tic conv ion to
x t ntip t t ct . Metabolism. P ’ h p tic ctiv -tion invo v in t p, in cont t to thm tip - t p p oc q i d o ctiv tiono c opido . C opido i p im i y hyd o-
yz d by int tin nd p m t to nin ctiv t min m t bo it , with th id
nhyd o iz d d nd oin two- t p m -t bo i m th t d p nd on cytoch om P450
nzym . P i o xt n iv y hyd o-yz d by th t , b t th int m di t
p od ct i th n m t bo iz d in in t pto th ctiv hyd y compo nd, m in y byCYP3A4 nd CYP2B6.
Th , bo t 80% o n o y b o b ddo o p i conv t d to ctiv d ,comp d with on y 10% to 20% o b o b dc opido . Time to peak effect. With c opido ,m xim inhibition o p t t tion oc-c 3 to 5 d y t t tin th py with 75m d i y witho t o din do , b t within 4to 6 ho i o din do o 300 to 600 mi iv n. In cont t, p o din do
p od c mo th n 80% o it p t t inhibi-
to y ct by 30 min t , nd p k ctivity ob v d within 4 ho .12 Th p t t inhibi-tion ind c d by p t 30 min t
dmini t tion i comp b to th p k
ct o c opido t 6 ho .13 Dose-response. P ’ inhibition op t t tion i do - t d.
P i bo t 10 tim mo potth n c opido nd 100 tim mo pot nth n tic opidin . Th , t tm nt with 5 mo p t in inhibition o p
ctivity (di t ib t d in i n c v ) vimi to th t p od c d by 75 m o c opid
o . On th oth h nd, v n m int n ncdo o 150 m o c opido inhibit p t
ctivity to d th n 10 m o p (46% v 61%),14 o c opido pp
to ch p t o p t t inhibition thp c n ov com .
At th pp ov d do o p , inbition o p t t tion i i nifc n
t nd th w “non ponth n with c opido . Interactions. D th t inhibit CYP3A4do not inhibit th fc cy o p , bth y c n inhibit th t o c opido . Somcommon y d d th t h v thi
th t tin ( , to v t in [Lipito ]) th m c o id ntibiotic ( , yth omycin)F th mo , wh p oton p mp inhibto h v b n hown to dimini h th co c opido by d cin th o m tionit ctiv m t bo it , no ch ct h bnot d with p .
p 2 t : t t m
A ph 2 t i comp d th pm n ( o din do /d i y m int n nc doo 40 m /7.5 m , 60 m /10 m , nd 60 m /15m ) nd t nd d c opido th py (30m /75 m ) in p ti nt nd oin ctiv o
nt p c t n o co on y int v ntion15 No i nifc nt di nc in o tcom w in th o p c ivin th th p
im n . How v , mo “minim b dv nt ” (d fn d by th c it i o th TIMI
t i 16) occ d with hi h-do p thwith ow -do p o with c opido
din to o th int m di t -do p im n (60-m o din do , 10-
d i y m int n nc ) o t t i .
Pla elenh b on bylop dogrel
var es w dely,n par dueo gene
polymorph sms

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 5/8
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009 711
lAzAr AnD linco
Anoth ph 2 t i ndomiz d 201 p -ti nt nd oin ctiv p c t n o co o-n y int v ntion to c iv p 60 m /10m o c opido 600 m /150 m .14 In p -
ti nt , th o din do w iv n bo t 1 hob o c di c c th t iz tion. A oon 30min t t th o din do , p t t in-hibition w p io with p (31% v5% inhibition o p t t tion), nd it
m in d i nifc nt y hi h t 6 ho (75%v 32%) nd d in th m int n nc ph(61% v 46%).
p 3 t :TriTon-TiMi 38On y on ph 3 t i o p h b ncomp t d: TRITON-TIMI 38 (th T i to A -
Imp ov m nt in Th p tic O tcom byOptimizin P t t Inhibition With P -
—Th ombo y i in Myoc di In ction),17 which n o d d t with mod t - i k tohi h- i k c t co on y ynd om ch d dto nd o p c t n o co on y int v n-tion. In thi t i , 10,074 p ti nt w n-
o d who h d mod t - to hi h- i k n t -b n in o non-ST- v tion MI, nd 3,534p ti nt w n o d who h d ST- v tionMI.
P ti nt w ndomiz d to c iv p - ( 60-m o din do , th n 10 m d i y)
o c opido ( 300-m o din do , th n 75m d i y) nd w t t d o 6 to 15 month .A p ti nt o c iv d pi in.
Th p im y nd point, compo it o d th om c diov c c , non tMI, o non t t ok , occ d in i nifc nt-
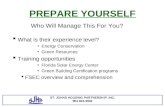
y w p ti nt t t d with p th nwith c opido (9.9% v 12.1%,P < .001)(Table 1 ). Mo t o th b n ft w d to w-
non t MI d in th o ow- p p iod(7.4% v 9.7%, P < .001). Addition y, thp o p h d i nifc nt y ow to t nt th ombo i comp d with th c opi-do o p (1.1% v 2.4%;P < .001).
Th b n ft c m t p ic o mob din . O tho p ti nt who did not n-d o co on y t y byp tin , mo
xp i nc d b din in th p o pth n in th c opido o p (2.4% v 1.8%,P = .03), inc din hi h t o i -th t-
nin b din (1.4% v 0.89%,P = .01) nd
t b din (0.4% v 0.1%,P = .002). Mo
p ti nt di contin d p b c o h mo h (2.5% v 1.4%,P < .001). In p -ti nt who p oc d d to co on y t y by-p tin , th t o m jo b din w
mo th n o tim hi h in tho who -c iv d p th n in tho who c iv dc opido (13.4% v 3.2%,P < .001).
A hi h t o dv v nt t d toco on c nc w o not d in p ti nt t t-
d with p , tho h th tho -t thi m y h v t d om th t on
ntip t t ct o p b in in mot mo to m dic tt ntion d to b din .
Ov d th t did not di i nif-c nt y b tw n th t tm nt o p .
In po t hoc n y i ,18 p w -p io to c opido in p v ntin i ch mic
v nt both d in th f t 3 d y o owinndomiz tion (th “ o din ph ”) nd o
th m ind o th t i (th “m int n ncph ”). Wh b din i k w imiwith th two d d in th o din ph ,p w b q nt y oci t d withmo b din d in th m int n nc ph .
C t in p ti nt b o p h d no n t b n-ft o v n d h m om p com-
p d with c opido .17 P ti nt with p vi-o t ok o t n i nt i ch mic tt ck h dn t h m om p (h z d tio 1.54,P = .04) nd how d t on t nd tow d
t t o m jo b din (P = .06). P -ti nt 75 nd o d nd tho w i hin th n 60 k h d no n t b n ft om p .
c t P i c nt y p ic d t 18% mo th nc opido , with v who p ic ppi o $6.65 o p 10 m comp d with$5.63 o c opido 75 m . (P 10-mpi co t $6.33 t d to .com o $7.60 tCVS; c opido 75-m pi co t $5.33 td to .com o $6.43 t CVS.) Th p t nton c opido xpi in Nov mb 2011, -t which th p ic di nti i xp ct d tob com i nifc nt y t .
Ticagrelor, a reversible oral agenT
Tic o , th f t v ib o P2Y12 c p-to nt oni t, i n t n tiv to thi nopy i-din th py o c t co on y ynd om .
Tic o i q ick y b o b d, do not
Prasugrels as e e v
a 30 m nu esas lop dogrel
s a 4 o 6hours

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 6/8
712 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009
PrAsUGrel
Prasugreldosage:A 60-mgload ng dose,
hen 10 mg/day
q i m t bo ic ctiv tion, nd h pidntip t t ct nd o t o ct, which
c o y o ow d - xpo v . In ndomiz d cont o d t i in p ti nt with
c t co on y ynd om with o witho t ST-
m nt v tion, t tm nt with tic o
comp d with c opido t d in iic nt d ction in d th om v c cMI, o t ok (9.8% v 11.7%).19
Giv n it v ib ct on p t t bition, tic o m y b p d in p ti
who co on y n tomy i nknown nd
Table 1
triton-tiMi 38: G a f a u m d gw h p a ug v p d gend poinT prasugrel clopidogrel P value
e f t
Primary end point(non atal MI, death rom cardiovascular causes,or non atal stroke)
9.9% 12.1% < .001
Non atal MI 7.3% 9.5% < .001
Death rom cardiovascular causes 2.1% 2.4% .31
Non atal stroke 1.0% 1.0% .93
Stent thrombosisb 1.1% 2.4% < .001
Death rom any cause 3.0% 3.2% .64
b m tNon‑CABG‑related TIMI major bleedingc 2.4% 1.8% .03
Li e‑threatening bleeding 1.4% 0.9% .01
Major or minor TIMI bleedingc 5.0% 3.8% .002
Bleeding requiring trans usions 4.0% 3.0% < .001
CABG‑related TIMI major bleedingd 13.4% 3.2% < .001
TRITON‑TIMI 38: The Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial In arction 38; CABG: coronary artery bypass gra ting. Percentages are Kaplan‑Meier estimates o therate o the end point at 15 months. .a E fcacy end points are based on the intention‑to‑treat population (prasugrel N = 6,813, clopidogrel N = 6,795), while complica‑tion numbers are or patients who received at least one dose o the study drug (prasugrel N = 6,741, clopidogrel N = 6,716) and orend points occurring within 7 days a ter the study drug was discontinued or occurring within a longer period i the end point wasbelieved by the local investigator to be related to the use o the study drug.b Stent thrombosis was defned as defnite or probable thrombosis, according to the Academic Research Consortium; the numbers o patients at risk were all patients whose index procedure included at least one intracoronary stent: 6,422 patients in each o the twotreatment groups.cTIMI major bleeding is defned as a drop in hemoglobin concentration o 5 g/dL or more, intracranial hemorrhage, or cardiac tam‑
ponnade. Minor bleeding is a drop in hemoglobin o 3 to 4.9 g/dL.d For major bleeding related to CABG, the total number o patients were all patients who had received at least one dose o prasugrelor clopidogrel be ore undergoing CABG: 179 and 189, respectively.
ADAptED FROM WIVIOtt SD, BRAUNWALD E, MCCABE CH, Et AL. pRASUgREL VERSUS CLOpIDOgREL IN pAtIENtS WItH ACUtE CORONARy SyNDROMES. N ENgL J MED 2007; 357:2001–2015. WItH pERMISSION FROM tHE MASSACHUSEttS MEDICAL SOCIEty.

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 7/8
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009 713
lAzAr AnD linco
o whom co on y t y byp tin id m d p ob b . It i ti nd oin t i
nd i not y t pp ov d.
TaKe-hoMe poinTs
P i mo pot nt, mo pid in on-t, nd mo con i t nt in inhibitin p t t
tion th n c opido . A c inict i 17 o nd p to b p io to c opi-do o p ti nt with mod t - to hi h- i k
c t co on y ynd om with hi h p ob bi -ity o nd oin p c t n o co on y in-t v ntion.
w , ?P ho d b iv n t n io phyto p ti nt with non-ST- v tion c tco on y ynd om o t p nt tion top ti nt with ST- v tion MI. Wh n d
o p nn d p c t n o co on y int -v ntion, p ho d b iv n t t30 min t b o th int v ntion, wdon in ph 2 t i ( tho h it o tin
in thi it tion i not comm nd d— b ow).
It i iv n in on -tim o din do o 60 m by mo th nd th n m int in d with10 m by mo th onc d i y o t t 1y . (At t 9 month o t tm nt with thi nopy idin i indic t d o p ti nt with
c t co on y ynd om who m dic yt t d, nd t t 1 y i indic t d o ow-in nt o ctiv p c t n o co on yint v ntion, inc din b oon n iop ty
nd p c m nt o b -m t o d - tint nt.)
w t ?Fo now, p ho d b void d in -vo o c opido in p ti nt t hi h i k o b din . It i c y cont indic t d in p -ti nt with p io t n i nt i ch mic tt ck o
t ok , o whom th i k o io b dinm to b p ohibitiv . It ho d n y b
void d in p ti nt 75 nd o d , tho hit mi ht b con id d in tho t p tic yhi h i k o t nt th ombo i , ch thowith di b t o p io MI. In p ti nt w i h-in th n 60 k , th p ck in t dvi
d c d do (5 m ), tho h c inic vi-
d nc o thi p ctic i ckin .
A y t, w h v no d t in th t p - i to in combin tion with f-
b ino ytic nt , o p ti nt on th ombo yticth py o c t MI ho d contin to -
c iv c opido t tin imm di t y ty i . F th mo , in p ti nt who p oc d dto co on y t y byp tin , th to m jo b din w mo th n o timhi h in th p o p th n in thc opido o p in th TRITON-TIMI 38t i .17 No thi nopy idin ho d b iv n top ti nt ik y to p oc d to co on y t ybyp tin .
On y c opido h vid nc ppo tinit n t n tiv to pi in o p ti ntwith th o c otic di who c nnot to -
t pi in. N ith d h vid nc o o p im y p v ntion.
ot t t Prior to angiography. Indic tion op c nt y imit d by th n -
ow cop o th t i d t . TRITON-TIMI38,17 th on y t i comp t d to d t ,
ndomiz d p ti nt to c iv p on yt th i co on y n tomy w known,
xc pt o ST- v tion MI p ti nt . It inknown wh th th b n ft o p
wi o tw i h th hi h i k o b din inp ti nt with c t co on y ynd om whodo not p oc d to p c t n o co on y in-t v ntion .
A c inic t i i c nt y nd w ycomp in p with c opido in10,000 p ti nt with c t co on y yn-d om who wi b m dic y m n d with-o t p nn d v c iz tion: A Comp i ono P nd C opido in Ac t Co o-n y Synd om S bj ct (TRILOGY ACS),C inic T i . ov Id ntif : NCT00699998.Th t i h n tim t d comp tion d t o M ch 2011.
In c o non-ST- v tion c t co o-n y ynd om , it i on b to w it to
iv thi nopy idin nti t th co on yn tomy h b n d fn d, i n io phy wi
b comp t d oon t p nt tion. Fox mp , 1-ho d y b o ivin p -
ti d iv ntip t t th py moq ick y th n ivin c opido on p n-t tion. I on d y xp ct d b o
n io phy, how v , th p ti nt ho d b
Prasugrels on ra-nd a edn pa en s
w h pr or tiAor s roke

8/4/2019 Cleveland Clinic Journal of Medicine 2009 LAZAR 707 14
http://slidepdf.com/reader/full/cleveland-clinic-journal-of-medicine-2009-lazar-707-14 8/8
714 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 • NUMBER 12 DECEMBER 2009
PrAsUGrel
iv n o din do o c opido “ p ont,”in cco d nc with id in p b i h d byth Am ic n Co o C dio o y, Am i-c n H t A oci tion, nd E op n Soci ty
o C dio o y,20 which comm nd t tin thi nopy idin y d in ho pit iz tionb d on t i d t with c opido . Patients undergoing elective percutane-ous coronary intervention t ow i k
o t nt th ombo i nd oth i ch mic comp ic tion , o it i po ib th t th b n fto p wo d not o tw i h th i kth p ti nt . Th , p c nnot y
b comm nd d o o tin ctiv pt n o co on y int v ntion xc pt in in-divid c in which th int v ntion i
th t th p ti nt m y b t hi h i kth ombo i .
re erences1. Y ghi z ri ns Y, br unst in Jb, ask ri a, Ston PH . Un-
stable angina pectoris. N Engl J Med 2000; 342:101–114.2. Yusuf S, Zh o F, M ht SR, Chro vicius S, Tognoni G,
Fox KK; C opidogr in Unst angin to Pr v nt R -curr nt ev nts Tri Inv stig tors . E ects o clopidogrelin addition to aspirin in patients with acute coronary
syndromes without ST-segment elevation. N Engl J Med2001; 345:494–502.3. b s no F, Rizzon P, Vio i F, t . Antiplatelet treat-
ment with ticlopidine in unstable angina. A controlledmulticenter clinical trial. The Studio della Ticlopidinanell'Angina Instabile Group. Circulation 1990; 82:17–26.
4. Schömig a, N um nn FJ, K str ti a, t . A randomizedcomparison o antiplatelet and anticoagulant therapya ter the placement o coronary-artery stents. N Engl JMed 1996; 334:1084–1089.
5. M ht SR, Yusuf S, P t rs RJG, t ; C opidogr in Un-st angin to Pr v nt R curr nt ev nts Tri (CURe)Inv stig tors . E ects o pretreatment with clopidogreland aspirin ollowed by long-term therapy in patientsundergoing percutaneous coronary intervention: thePCI-CURE study. Lancet 2001; 358:527–533.
6. S tin MS, C nnon CP, Gi son CM, t ; ClaRITY-TIMI28 Inv stig tors . Addition o clopidogrel to aspirin andfbrinolytic therapy or myocardial in arction with ST-segment elevation. N Engl J Med 2005; 352:1179–1189.
7. S tin MS, C nnon CP, Gi son CM, t ; C opi-dogr s adjunctiv R p rfusion Th r py (ClaRITY)-Throm o ysis in Myoc rdi Inf rction (TIMI) 28Inv stig tors . E ect o clopidogrel pretreatmentbe ore percutaneous coronary intervention in patientswith ST-elevation myocardial in arction treated withfbrinolytics: the PCI-CLARITY study. JAMA 2005:294:1224–1232.
8. Ch n ZM, Ji ng lX, Ch n YP, t ; COMMIT (C Opidogrnd M topro o in Myoc rdi Inf rction Tri ) co or -
tiv group . Addition o clopidogrel to aspirin in 45,852patients with acute myocardial in arction: randomisedplacebo-controlled trial. Lancet 2005; 366:1607–1621.
9. St inhu SR, b rg r Pb, M nn JT 3rd, t ; CReDOInv stig tors . Clopidogrel or the reduction o eventsduring observation. Early and sustained dual oralantiplatelet therapy ollowing percutaneous coronaryintervention: a randomized controlled trial. JAMA 2002;288:2411–2420.
10. S r ru ny Vl, St inhu SR, b rg r Pb, M inin aI,bh tt Dl, Topo eJ . Variability in platelet responsivenessto clopidogrel among 544 individuals. J Am Coll Cardiol2005; 45:246–251.
11. M g Jl, C os Sl, Wiviott SD, t . Cytochrome P-450polymorphisms and response to clopidogrel. N Engl JMed 2009; 360:354–362.
12. H ft G, Os nd JI, Worth y SG, t . Acute antithrom-botic e ect o a ront-loaded regimen o clopidogrel
in patients with atherosclerosis on aspirin. ArteriosclerThromb Vasc Biol 2000; 20:2316–2321.
13. W r kkody GJ, J ku owski Ja, br ndt JT, t . Com-parison o speed o onset o platelet inhibition a terloading doses o clopidogrel versus prasugrel in healthyvolunteers and correlation with responder status. Am JCardiol 2007; 100:331–336.
14. Wiviott SD, Tr nk D, Fr ing r al, t ; PRINCIPle-
TIMI 44 Inv stig tors . Prasugrel compared with highloading- and maintenance-dose clopidogrel in patientswith planned percutaneous coronary intervention: thePrasugrel in Comparison to Clopidogrel or Inhibitiono Platelet Activation and Aggregation-Thrombolysisin Myocardial In arction 44 trial. Circulation 2007;116:2923–2932.
15. Wiviott SD, antm n eM, Wint rs KJ, t ; JUMbO-TIMI26 Inv stig tors . Randomized comparison o prasug-rel (CS-747, LY640315), a novel thienopyridine P2Y12antagonist, with clopidogrel in percutaneous coronaryintervention: results o the Joint Utilization o Medica-tions to Block Platelets Optimally (JUMBO)-TIMI 26 Trial.Circulation 2005; 111:3366–3373.
16. bovi eG, T rrin Ml, Stump DC, t . Hemorrhagicevents during therapy with recombinant tissue-typeplasminogen activator, heparin, and aspirin or acutemyocardial in arction. Results o the Thrombolysis inMyocardial In arction (TIMI) Phase II Trial. Ann InternMed 1991; 115:256–265.
17. Wiviott SD, br unw d e, McC CH, t ; TRITON-TIMI 38 Inv stig tors . Prasugrel versus clopidogrel inpatients with acute coronary syndromes. N Engl J Med2007; 357:2001–2015.
18. antm n eM, Wiviott SD, Murphy Sa, t . Early andlate benefts o prasugrel in patients with acute coro-nary syndromes undergoing percutaneous coronaryintervention: a TRITON-TIMI 38 (TRial to Assess Improve-ment in Therapeutic Outcomes by Optimizing PlateletInhibitioN with Prasugrel-Thrombolysis In Myocardial In-
arction) analysis. J Am Coll Cardiol 2008; 51:2028–2033.19. W ntin l, b ck r RC, bud j a, t ; PlaTO Inv stig -
tors, Fr ij a, Thorsén M . Ticagrelor versus clopidogrel inpatients with acute coronary syndromes. N Engl J Med2009; 361:1045–1057.
20. br unw d e, antm n eM, b s y JW, t . ACC/ AHA 2002 guideline update or the management opatients with unstable angina and non–ST-segmentelevation myocardial in arction—summary article*1:A report o the American College o Cardiology/ American Heart Association task orce on practiceguidelines (Committee on the Management o Pa-tients With Unstable Angina). J Am Coll Cardiol 2002;40:1366–1374.
ADDRESS : Lawrence D. Lazar, MD, Department of Cardiovas-cular Medicine, Cleveland Clinic, J2-3, 9500 Euclid Avenue,Cleveland, OH 44195; e-mail [email protected].