Classic AEDs John M. Pellock, MD Professor and Chairman Division of Child Neurology Virginia...
33
Classic AEDs John M. Pellock, MD Professor and Chairman Division of Child Neurology Virginia Commonwealth University Medical College of Virginia Hospitals Richmond, Virginia
-
Upload
darleen-peters -
Category
Documents
-
view
221 -
download
0
Transcript of Classic AEDs John M. Pellock, MD Professor and Chairman Division of Child Neurology Virginia...
Classic AEDs
John M. Pellock, MDProfessor and Chairman
Division of Child NeurologyVirginia Commonwealth University
Medical College of Virginia HospitalsRichmond, Virginia
Older AEDs
Phenobarbital (1912)
Phenytoin (1938)
Ethosuximide (1960)
Carbamazepine (1974)
Valproic acid (1978)
Bromides
Benzodiazepines
First-Line Therapy Early 20th Century
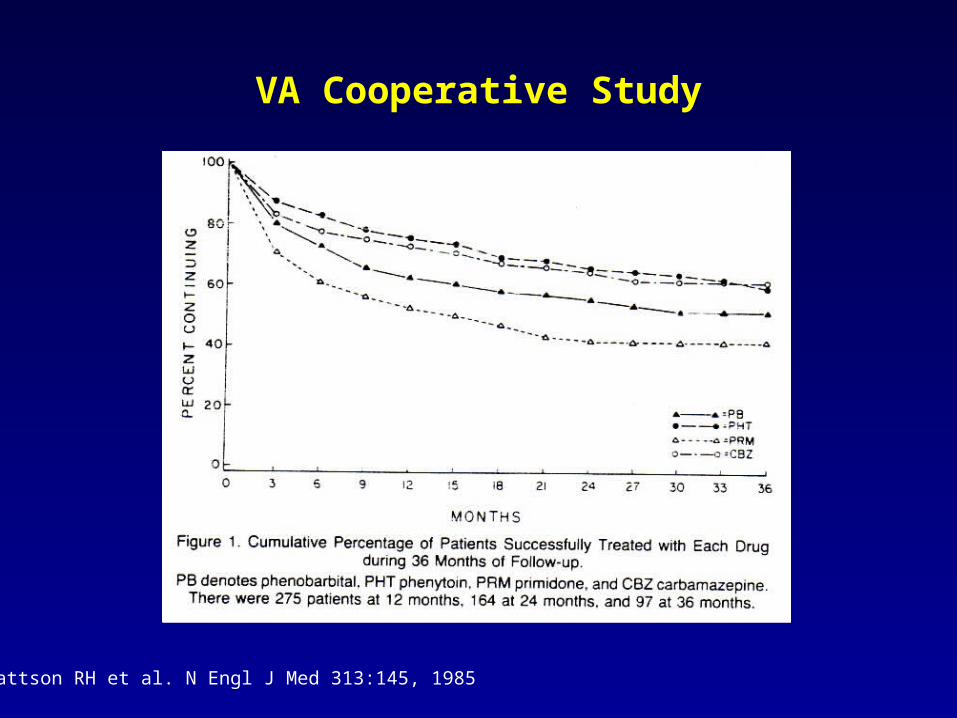
Mattson RH et al. N Engl J Med 313:145, 1985
VA Cooperative Study

Toxicity of Classic AEDs
M de Silva (Lancet 1996) randomized 167 children with partial or tonic-clonic seizures
6 of 10 children assigned to phenobarbital had behavioral or cognitive adverse events
Only 15 children had adverse effects requiring withdrawal
Phenytoin: 2 with drowsiness; 1 each skin rash, hirsutism and blood dyscrasia
Carbamazepine: 1 each drowsiness and blood dyscrasia
VPA: 1 each behavioral and tremor
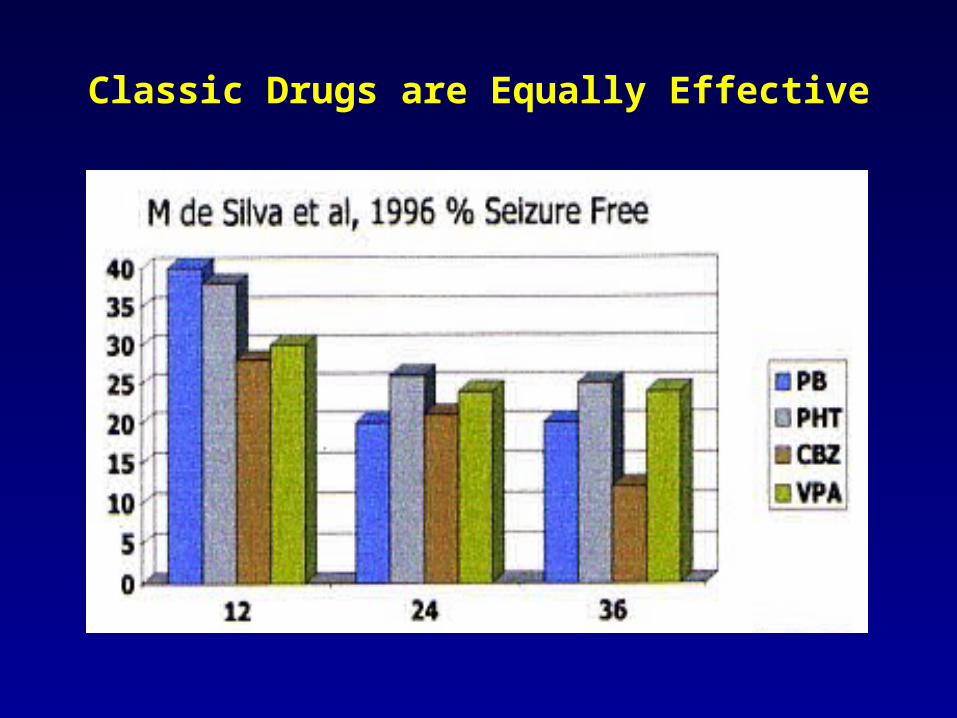
Classic Drugs are Equally Effective
AED Selection
Seizure type and syndrome
Neonatal seizures
Infantile spasms
Generalized epilepsies
Partial-onset
AED efficacy
AED toxicity
Need for monitoring
Ease of dosing and compliance issues
Underlying medical conditions
Medication interactions
Urgency of initiating therapy
Cost

Carbamazepine
Carbamazepine
Dose: 10-35 mg/kg/day (bid-qid)
Elimination
>85% hepatic
Major pathway CYP3A4
Active metabolite 10-11 epoxide, metabolized by epoxide hydrolase (may be increased out of proportion to total level)
Autoinduction
Clearance can increase by 300% over first 3-5 wks
May need 3 to 4x / day dosing in children
Carbamazepine: Adverse Effects
10% with transient leukopenia
Risk of aplastic anemia and agranulocytosis 5-8x risk in general population Mid-1980s, 31 cases thrombocytopenia 10 cases agranulocytosis 27 cases aplastic anemia 8 cases pancytopenia
Rash reported in 17% pts; 10% have been life-threatening Incidence of rash increased with age: 5% at 0-6 yrs, 15.4% at >7 yrs
Hepatotoxicity 20 cases of clinical significance reported by mid-1980s Hepatotoxicity reversible, but recurs with re-administration of drug
Dose related neurotoxic effects: dizziness, somnolence, ataxia, diplopia, blurred vision, nausea
Carbamazepine: Drug Interactions
Enzyme inducer Effects on thyroid and sex hormones Effects on vitamin D metabolism
Multiple drug interactions
Increase CBZ Azole antifungals, cimetidine, delaviridine, diltiazem,
clarithromycin, erythromycin, fluoxetine, INH, NNRTIs, omeprazole, PIs, propoxyphene, verapamil, caffeine, grapefruit juice
Decrease CBZ FBM, desmethyldiazepam, PB, PHT, loxapine
Increase epoxide levels FBM, VPA
Levels rise with CBZ
Chlorothiazide, MAO inhibitors, lithium, perphenazine, acenocoumarol, digitalis glycosides, furosemide and INH
No significant clinical interaction
Phenobarbital, primidone
Levels decrease with CBZ
Antipsychotics (haloperidol, alprazolam, clozapine, trazadone – clinically insignificant with olanzapine)
Azole antifungals, calcium chennel blockers, cyclosporine, FBM, VPA, narcotics, neuromuscular blockers, NNRTIs, oral contraceptives, PIs, theophylline, TGB, tricyclics, VPA, warfarin, ZNS
Benzodiazepines
Carbamazepine: Drug Interactions

Schachter S. Exp Opin Invest Drugs 8:1, 1999
Oxcarbazepine Metabolic Pathway:No Epoxide, No Autoinduction
NH2O
NH2O
O
NH2O
OH
NH2O
Gluc O
NH2O
O
NH2O
OH OH
Oxcarbazepine
Carbamazepine
Reduction Conjugation
Oxidation Hydrolysis
MHD
10, 11-Epoxide
No autoinduction
Autoinduction
N N
NN N
N
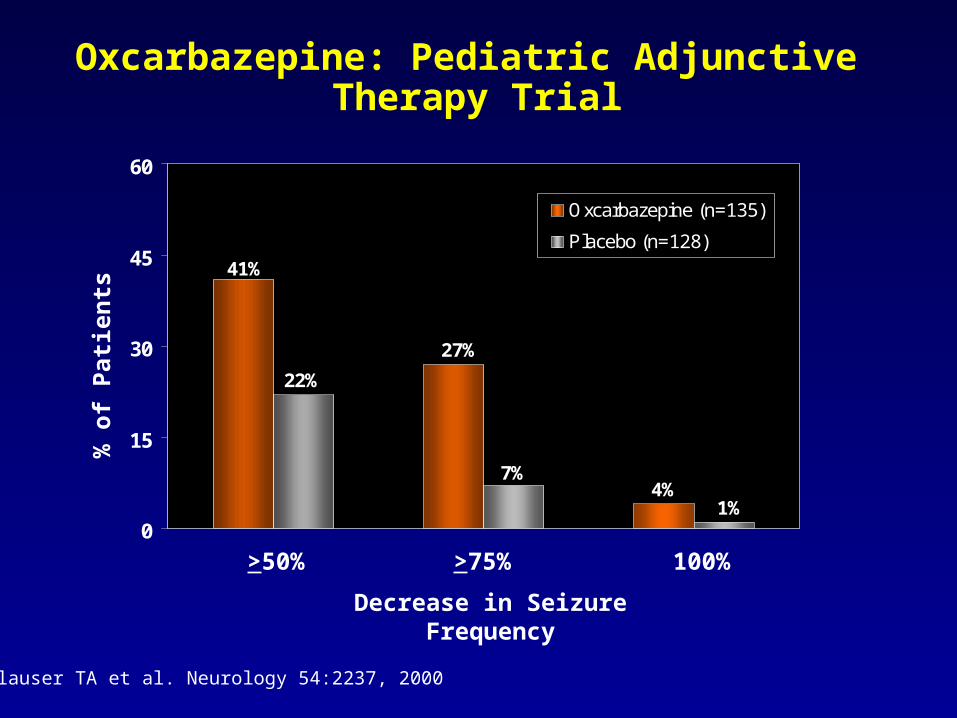
Oxcarbazepine: Pediatric Adjunctive Therapy Trial
Glauser TA et al. Neurology 54:2237, 2000
41%
27%
4%
22%
7%
1%0
15
30
45
60
Oxcarbazepine (n=135)
Placebo (n=128)
% o
f P
atie
nts
Decrease in Seizure Frequency
>50% >75% 100%

Safety of Oxcarbazepine: Hyponatremia
Incidence of clinically significant hyponatremia
(Na <125 mmol/L) in clinical trials: 2.5%
Most (79%) were receiving concomitant Na-depleting medications
Hyponatremia usually asymptomatic
TRILEPTAL® prescribing information
Safety of Oxcarbazepine: Hypersensitivity
25-30% hypersensitive to CBZ will experience similar reaction to OXC
Prevention of hypersensitivity reactions
Ask about prior adverse experiences with CBZ
If patient has history of hypersensitivity with CBZ, use OXC only if benefit justifies risk
Discontinue OXC immediately if signs or symptoms
of hypersensitivity develop
TRILEPTAL® prescribing information
Dosing Guidelines:Pediatric Adjunctive Therapy
Approved product labeling recommendations
Starting dose: 8-10 mg/kg/day (not to exceed 600 mg/day); titrate to target dose over 2 wks
Target dose based on weight 20-29 kg 900 mg/day 29.1-39 kg 1200 mg/day >39 kg 1800 mg/day
Clinical experience
Improved tolerability with lower starting dose and slower titration
Starting dose: 4-5 mg/kg/day increased weekly by 4-5 mg/kg/day to target dose of 20 mg/kg/day in approximately 4 wks
Phenobarbital
Used in neonatal seizures, and potentially useful for severe epilepsy acknowledging its cognitive, depressive, and behavioral side effects
Formulations: 30, 60, and 100 mg tabs; 20 mg / 5 mL elixir
Doses Half-life
Neonates, 3-4 mg/kg/day 43-217 hrs
Infants, 4-5 mg/kg/day
Children, 2-3 mg/kg/day 35-73 hrs
Adults, 0.5-1 mg/kg/day 56-140 hrs
Slow taper to discontinue

Phenobarbital: Adverse Effects
Neurotoxic effects Sedation, dizziness, mood change,
insomnia, hyperkinesia (children, elderly) Cognitive dysfunction
Others Osteomalacia Peripheral neuropathy Dupuytren’s contraction Frozen shoulder
Idiosyncratic Skin rash Hepatotoxicity Blood dyscrasia
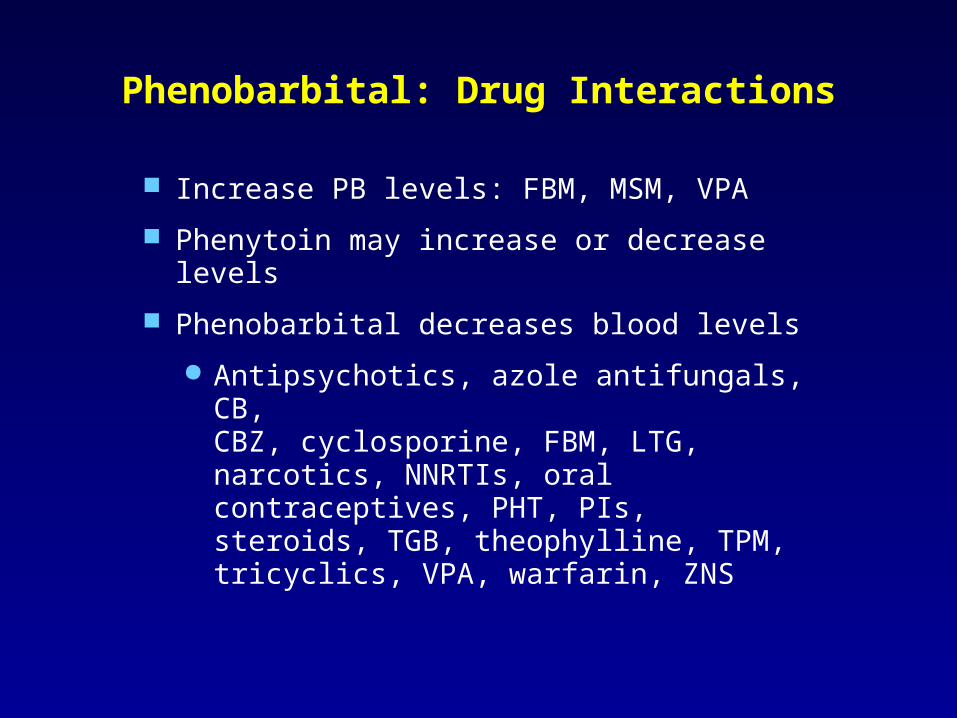
Phenobarbital: Drug Interactions
Increase PB levels: FBM, MSM, VPA
Phenytoin may increase or decrease levels
Phenobarbital decreases blood levels
Antipsychotics, azole antifungals, CB, CBZ, cyclosporine, FBM, LTG, narcotics, NNRTIs, oral contraceptives, PHT, PIs, steroids, TGB, theophylline, TPM, tricyclics, VPA, warfarin, ZNS
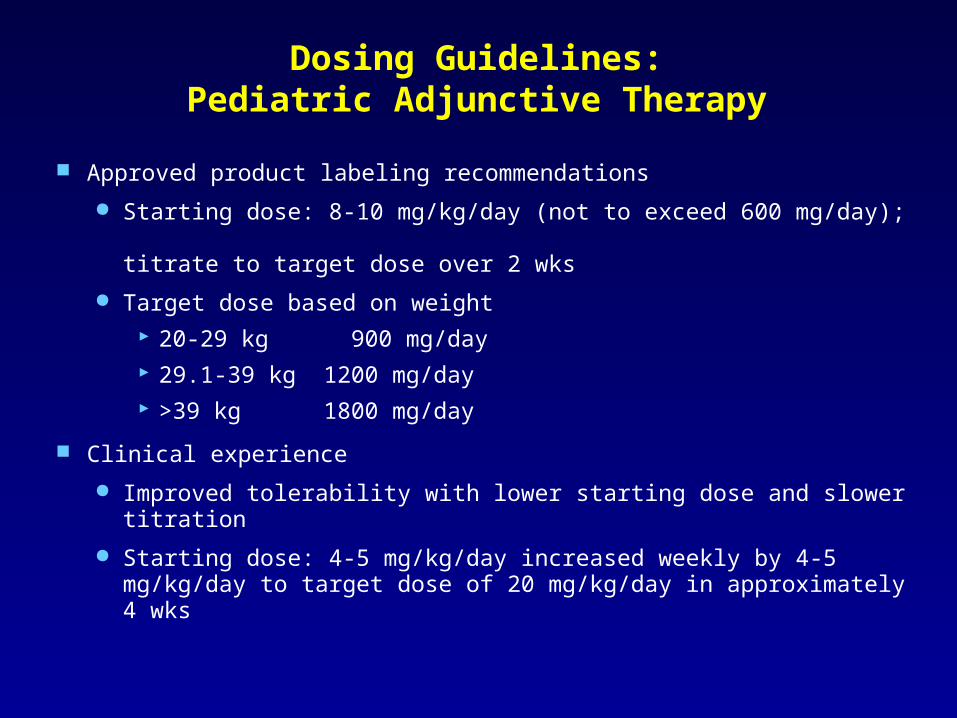
Dosing Guidelines:Pediatric Adjunctive Therapy
Approved product labeling recommendations
Starting dose: 8-10 mg/kg/day (not to exceed 600 mg/day); titrate to target dose over 2 wks
Target dose based on weight 20-29 kg 900 mg/day 29.1-39 kg 1200 mg/day >39 kg 1800 mg/day
Clinical experience
Improved tolerability with lower starting dose and slower titration
Starting dose: 4-5 mg/kg/day increased weekly by 4-5 mg/kg/day to target dose of 20 mg/kg/day in approximately 4 wks
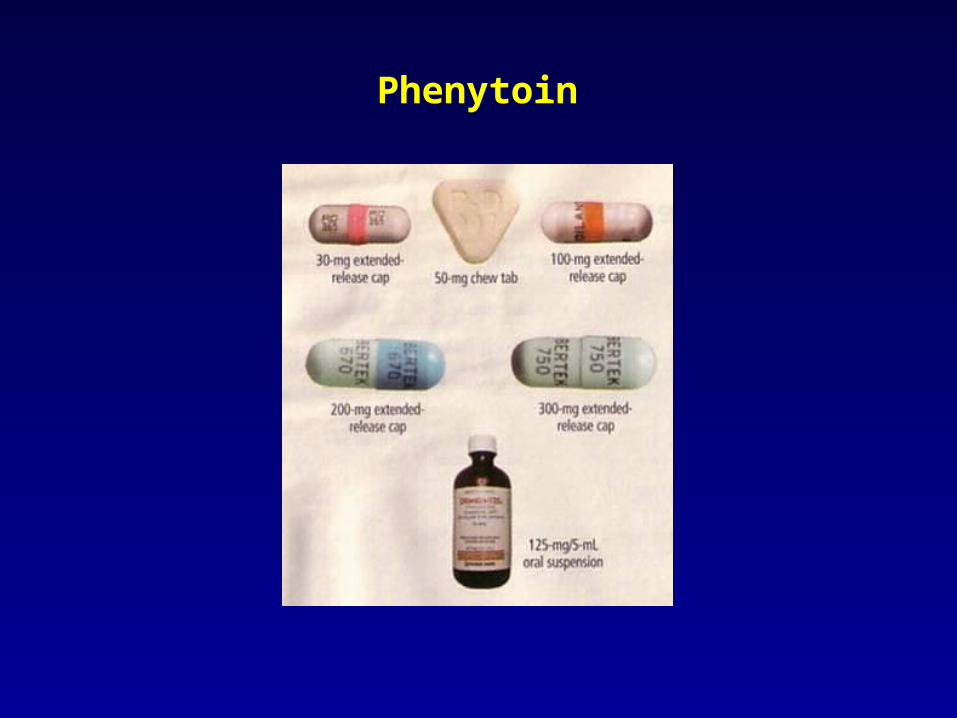
Phenytoin
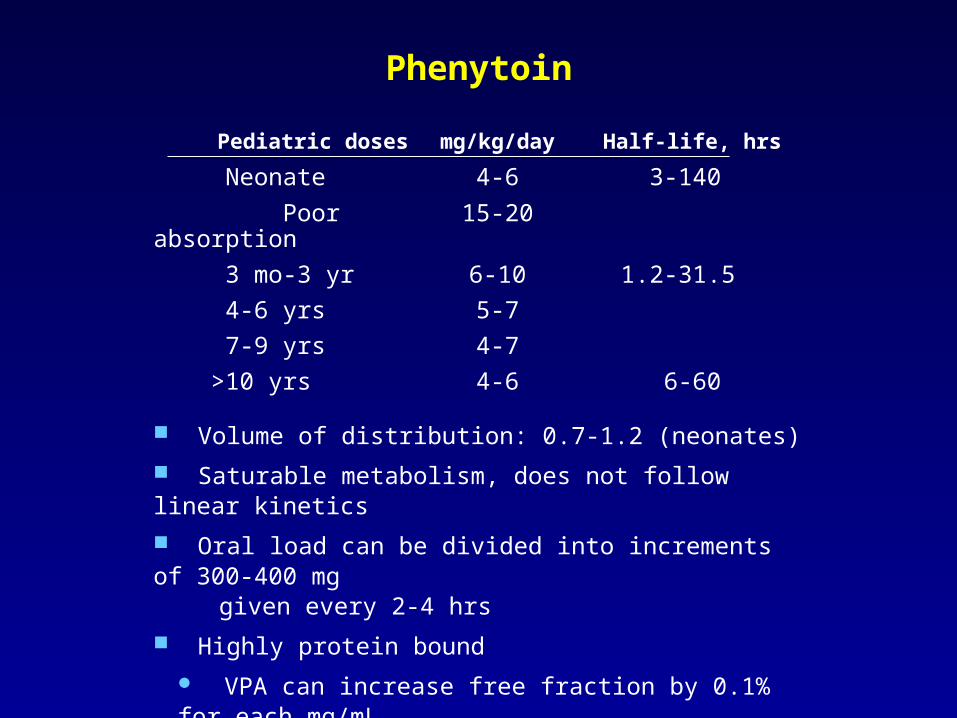
Phenytoin
Pediatric doses mg/kg/day Half-life, hrs
Neonate 4-6 3-140
Poor absorption 15-20
3 mo-3 yr 6-10 1.2-31.5
4-6 yrs 5-7
7-9 yrs 4-7
>10 yrs 4-6 6-60
Volume of distribution: 0.7-1.2 (neonates)
Saturable metabolism, does not follow linear kinetics
Oral load can be divided into increments of 300-400 mg given every 2-4 hrs
Highly protein bound
VPA can increase free fraction by 0.1% for each mg/mL At VPA levels of 100, free phenytoin can be 20% of total
Phenytoin: Adverse Effects and Drug Interactions
Side effects: nystagmus, ataxia, dizziness, hirsuitism, gingival hyperplasia, peripheral neuropathy, osteomalacia, folate deficiency
Idiosyncratic Skin rash Hepatotoxicity Blood dyscrasia Lymphadenopathy
Increase PHT levels: amiodarone, cimetidine, diltiazem, FBM, fluconazole, fluoxetine, INH, MSM, omeprazole, OXC, PB, ritonavir, ticlopidine, TPM, VPA
Decrease PHT levels: antacids, CBZ, ciprofloxacin, PB, sucralfate
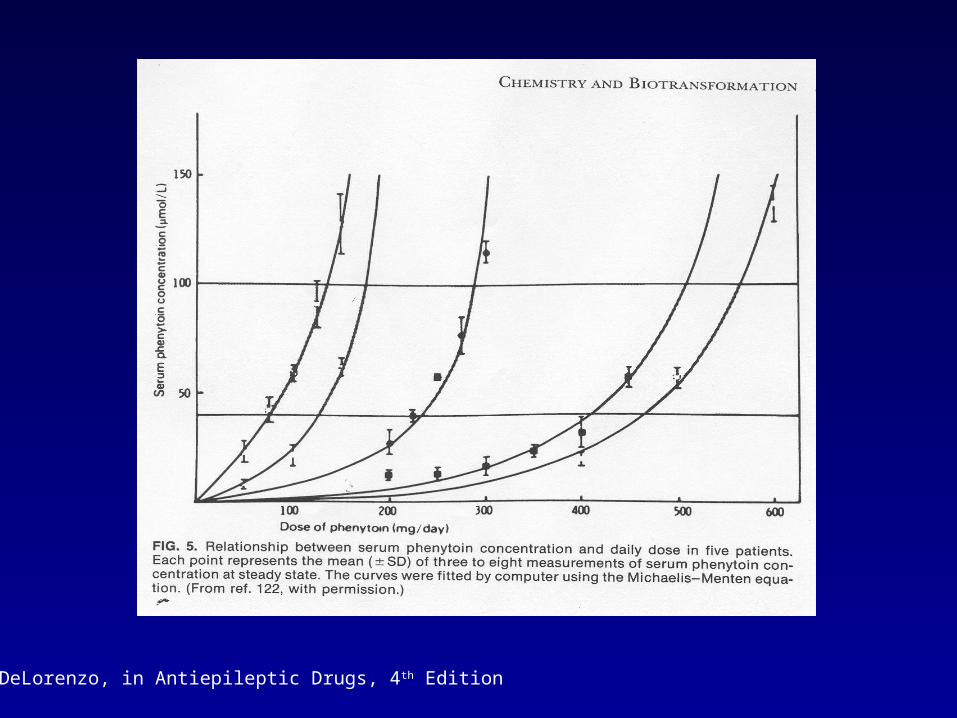
R. DeLorenzo, in Antiepileptic Drugs, 4th Edition

Ethosuximide
Useful for absence attacks of childhood absence epilepsy and for atypical absence
Formulations: 250 mg capsule and 250 mg/5 mL solution
Common pediatric dose: 10-15 mg/kg/day (initial);15-40 mg/kg/day (maintenance) qd – tid
Increased doses can decrease GI side effects
Adverse effects: GI distress, nausea, anorexia, drowsiness, HA, dizziness, hiccups, behavioral changes (rare psychotic reactions)
Idiosyncratic: skin rash, blood dyscrasia
VPA may increase levels; CBZ, PB, PHT decrease levels
Valproic Acid
Valproic Acid
Different spectrum of usefulness (generalized, absence, atonic, myoclonic [Lennox-Gastaut] seizures)
Used in bipolar and schizoaffective disorders
Common pediatric doses: 15-60 mg/kg/day
Elimination: hepatic metabolism (>95%), glucuronidation (20-50%), beta-oxidation (40%), CYP (minor)
Adverse reactions: hepatotoxicity (highest risk in those <2 yrs and on multiple AEDs), pancreatitis, and blood dyscrasia Bleeding with and without thrombocytopenia Osteomalacia Polycystic ovary syndrome (anovulatory cycles) Teratogenicity
Valproate: Drug Interactions
High protein binding
Inhibits biotransformation of PB, ethosuximide, LTG, carbamazepine epoxide, free PHT
Increased levels of CCB, FBM, zidovudine
Increase VPA levels: ASA, FBM, fluoxetine, INH
Decrease VPA levels: CBZ, LTG, PB, PHT, ritonavir
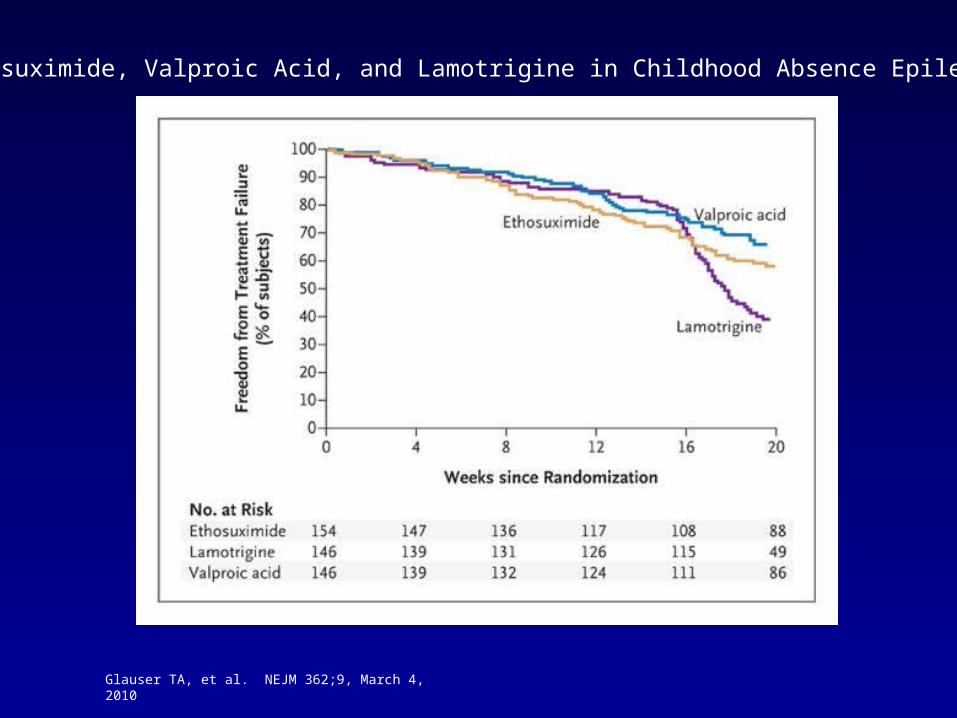
Glauser TA, et al. NEJM 362;9, March 4, 2010
Ethosuximide, Valproic Acid, and Lamotrigine in Childhood Absence Epilepsy

Benzodiazepines
Highly protein bound: 80-90%
Used to treat status
Rectal dizaepam and oral Intensol used to treat prolonged seizures in intractable seizure disorders and clusters; also available for patients with infrequent seizures
Tolerance precludes broad use for chronic seizures
Care must be taken to prevent psychosis and seizure exacerbation during withdrawal
Use of Drug Level Monitoring:Always Have a Question!
Establish “baseline” effective concentrations
Evaluate potential causes for lack of efficacy “Fast metabolizers” Noncompliance
Evaluate potential causes for toxicity
Altered drug utilization as consequence of physiological conditions (puberty, geriatrics)
“Slow metabolizers”
Altered drug utilization as consequence of pathological conditions (renal failure, liver failure)
Drug-drug interactions
Switching AED preparations

Use of Drug Level Monitoring:Always Have a Question!
Evaluate potential causes for loss of efficacy
Altered drug utilization as consequence of physiological conditions (e.g. neonates, infants, young children)
Altered drug utilization as consequence of pathological conditions
Change in formulation
Drug-drug interaction
Judge “room to move” or when to change AEDs
Minimize predictable problems (PHT, VPA)