
Classes 3 & 4 OP poisoning and Anticholinergics
51
ORGANOPHOSPHATE POISONING Dr.U.P.Rathnakar MD.DIH.PGDHM www.scribd.com www.pharmacologyfordummies.blogspot.com
-
Upload
druprathnakarmddihpgdhm -
Category
Documents
-
view
115 -
download
1
description
Theory class for MBBS
Transcript of Classes 3 & 4 OP poisoning and Anticholinergics

ORGANOPHOSPHATEPOISONING
Dr.U.P.RathnakarMD.DIH.PGDHM
www.scribd.comwww.pharmacologyfordummies.blogspot.com

What is the link?• Cholinergic drugs
[Agonists of Ach Rec.]Cholinomimitics OR
Directly acting cholinergics OR
Indirectly acting Cholinomimitics
Musc.Rec.Antagonists
Antagonists at N.M.Junction
Anti-Cholinesterases
Antagonists Anti-cholinergics
N.M.Blockers
Ganglion blockers

Anticholinesterases[Indirectly acting cholinergics]
Reversible anticholinesterases Carbamates Acridine
Tacrine.• Physostigmine• Neostigmine• Pyridostigmine• Edrophonium• Ambenonium• Demecarium• Rivastigmine, • Donepezil, • Galantamine.

Organophosphates: Carbamates:• Echothiophate Carbaryl*• Parathion* Propoxur*• Malathion*• Diazinon*• Tabun#• Sarin#• Soman#
*Insecticides # Nerve gases-chemical warfare
Irreversible anticholinesterases
Anticholinesterases[Indirectly acting cholinergics]

Carbamylation [Therapeutic] and Phosphorylation [Poisoning]
ReactionVery Slow
Orirreversible

REVERSIBLE ANTICHOLINESTERASES-USES
MIOTIC
• Glaucoma• Reverse the effect of mydriatics• Alternated with mydriatics-to
break irido-corneal adhesions

REVERSIBLE ANTICHOLINESTERASES-USES
• Postoperative paralytic ileus/urinary retension
[Neostigmine]• Postoperative decurarization [Neostigmine
preceded by Atropine]• Cobra bite [Neostigmine+Atropine]• Belladona [Atropine] poisoning-Physostigmine• Alzheimer’s disease-Tacrine, rivastgmine,
donepezil, galantamine [cerebroselective]• Drug over dosage-e.g. TCA
• Myasthenia gravis

Irreversible anticholinesterases
Organophosphates• Echothiophate –used in glaucoma• Parathion • Malathion• Diazinon• Tabun• Sarin • Soman
Insecticides
Nerve gases

Entry into body
• Transdermal• Inhaled• Ingested

Mechanism Of Action
Organophosphorous compounds bind to acetylcholinesterase overabundance of acetylcholine in the synapse Compound undergoes a conformational change
(aging) renders the enzyme irreversibly resistant to reactivation.
Carbamate Compounds unlike organophosphates, are transient
cholinesterase inhibitors.
OP Poisoning
• Occupational• Accidental• Homicidal• Suicidal• Chemical warfare

Clinical Features (Acute Toxicity)
Paralysis

Types of toxicity
• Acute cholinergic syndrome• Intermediate syndrome• Delayed Neurotoxicity• Warfare

Clinical Features (Acute Toxicity)
• Generally manifests in minutes to hours • Evidence of cholinergic excess• Parasympathetic-Sympathetic-Nicotinic
SLUDGe =Salivation, Lacrimation, Urination, Defecation, Gastric Emptying.
BBB= Bradycardia, Bronchorrhea,
Bronchospasm.
DUMBELLS= Diarrhea , Diaphoresis
UrinationMiosis Bradycardia Emesis LacrimationLethargySalivation
TREATMENT
A - B – C
• Airway: Bronchoconstriction• Breathing: Paralysis of resp.muscles• Circulation: Hypotension Vs Hypertension

TREATMENTAcute
• General supportive measures: • Termination of exposure, copious washing , airway,
respiration , oxygen, DIAZEPAM, tt shock• Anticholinergics Atropine i.v.
- Sufficent doses i.v. [For muscarinic effects]-till atropinization-maintained for 1-2 weeks
• Cholinesterase reactivators• Pralidoxime - Sufficiently early i.v.
[For Nicotinic effects]

Oximes-MOA
ReactionVery Slow
Orirreversible
Oximes attach to anionic site
Oxime + Phosphorous
Oxime –phosphate diffuses
Pralidoxime[2-PAM]ObidoximeDiacetyl-monoxime[DAM]
[Cholinesterase reactivators]

Oximes
• Ineffective against carbamates-Anionic site is not free
• Contra indicated-intrinsic anti-ChE activity• More effective at nicotinic • Poor in muscarunic sites• Not at all in CNS-does not cross BBB• Not effective after phosphorylated enzyme under
goes aging• Atropine is the DOC-Oxime is secondary drug

Chronic OP poisoning
• Fluorine compounds• Polyneuritis and demyelination of nerves• Sensory loss → Motor loss → LMN palsy →
Spasticity → Upper motor neurone paralysis• Mechanism → not inhibition of ChE• Takes years to recover

Nerve agents [Nerve gases]
•These chemicals are liquid at room temperature,
•Phosphorus-containing• organic chemicals (organophosphates)•Weapons of mass destruction

Nerve gases[Anticholinesterases]

Gulf war syndrome
• Approximately 250,000 of the 697,000 veterans who served in the 1991 Gulf War are afflicted with enduring chronic multi-symptom illness,
• A wide range of acute and chronic symptoms have included fatigue, loss of muscle control, headaches, dizziness and loss of balance, memory problems, muscle and joint pain, indigestion, skin problems, immune system problems, and birth defects.
• Nerve Gas??• Pyridostigmine??

Nerve gases
• Miosis, profuse salivation, convulsions, involuntary urination and defecation and eventual death by asphyxiation
• Nerve agents can also be absorbed through the skin
• Or portal of entry into the body is the respiratory system
• Protection-full body suit in addition to a respirator.

Dr.U.P.RathnakarMD.DIH.PGDHM
www.scribd.comwww.pharmacologyfordummies.blogspot.com
Anticholinergics[Cholinoceptor antagonists]

What is the link?• Cholinergic drugs
[Agonists of Ach Rec.]Cholinomimitics OR
Directly acting cholinergics OR
Indirectly acting Cholinomimitics
Musc.Rec.Antagonists
Antagonists at N.M.Junction
Drugs act like ACh Act at sites & receptors
Where Ach acts
Ganglia-NNSk.muscles-NMHeart,Lungs,
Int.]MuscEye, Sweat
glands]M12345Inhibit degradation of AchBy AChE[Cholinesterase] Anti-Cholinesterases Increase duration of
Action of ACh
Antagonists Anti-cholinergics
N.M.Blockers
Ganglion blockers

ANTICHOLINERGICS
Competitive antagonists of acetylcholine at cholinergic sites

Site of action of anti-cholinergics
Antimuscarinics
Ganglionic blockers
NM Blockers
Semisynthetic derivatives
•Homatropine•Atropine methonitrate•Hyoscine butyl bromide•Ipratropium bromide•Tiotropium bromide
Synthetic compounds
•MydriaticsCycclopentolate& Tropicamide
•Antisecretory-antispasmodicsQuaternaryPropatheline, Glycopyrrolate
TertiaryDicyclomine, Pirenzepine
•AntiparkinsonianTrihexyphenydyl, Biperiden, Benztropine
•VasicoselectiveOxybutynin, Flavoxate
Natural alkaloids
•Atropine•Scopolamine[Hyoscine]
Anticholinergic drugs[Classification]
SOURCE AND CHEMISTRY
• Atropine -Atropa belladonna Or Datura stramonium-tertiary amine
• Scopolamine (hyoscine) -Hyoscyamus niger, • Tertiary derivatives- used -effects on the eye or the
CNS[mydriatrics or antiparkinsonians]• Quaternary amines -more peripheral effects with
reduced CNS effects[Antispasmodics]• Antihistaminic -antipsychotic -antidepressant - have
similar structures • Hence antimuscarinic side effects.• .

Pharmacokinetics
ABSORPTION • Natural alkaloids and most tertiary
antimuscarinic drugs are well absorbed from the gut and conjunctival membranes.
• Even absorbed across the skin (transdermal route-scopolamine).
• Only 10–30% of a dose of a quaternary drug is absorbed after oral administration,

Pharmacokinetics
• DISTRIBUTION • Atropine and tertiary agents are widely distributed in the body.
• Significant levels –in CNS within 30 minutes to 1 hour, and this can limit the dose tolerated when the drug is taken for its peripheral effects.
• Scopolamine is rapidly and fully distributed into the CNS where it has greater effects than most other antimuscarinic drugs.
• Quaternary derivatives are poorly taken up by the brain and therefore are relatively free—at low doses—of CNS effects.

Pharmacokinetics
• METABOLISM AND EXCRETION • Atropine-Rapid phase is 2 hours and that of the slow phase
is approximately 13 hours. • About 50% of the dose is excreted unchanged in the urine.
• The drug's effect on parasympathetic function declines rapidly in all organs except the eye. Effects on the iris and ciliary muscle persist for 72 hours.
Pharmacodynamics
• Atropine causes reversible (surmountable) blockade of cholinomimetic actions at muscarinic receptors;
• Muscarinic antagonists not just neutral compounds that occupy the receptor and prevent agonist binding.
• Muscarinic receptors are constitutively active,• Drugs that block the actions of acetylcholine are inverse
agonists • Shift the equilibrium to the inactive state of the receptor. • Muscarinic blocking drugs that are inverse agonists
include atropine, pirenzepine, trihexyphenidyl,

Tissue selectivity
• Most sensitive to atropine are the salivary, bronchial, and sweat glands.
• Secretion of acid by the gastric parietal cells is the least sensitive.
• Atropine is highly selective for muscarinic receptors. • Its potency at nicotinic receptors is much lower, • Atropine does not distinguish among the M1, M2, and M3
subgroups of muscarinic receptors. • Quaternary- Poor absorption, do not cross BBB, more
nicotinic and ganglionic actions, longer acting• Differences between Atropine and Scopolamine????

Systemic Effects
CNS
• Medullary-Excitation• Vestibular-depression• Basal ganglion-↓Cholinergic
activity• High doses-Disorientation,
hallucination, coma
Eye
• Passive mydriasis• Cycloplegia• Reduce lacrimal secretion
• Belladona!!!• The name belladonna derives from the alleged
use of this preparation by Italian women to dilate their pupils
• Modern-day fashion models are known to use this same device for visual appeal
• WHEN A ADRENERGIC STIMULANT IS GIVEN- THE DILATOR PUPILLAE MUSCLE CONTRACTS LEADING TO
• MYDRIASIS.• ACTIVE MYDRIASIS.• [No cycloplegia]• [Light reflex ++]
• ANTICHOLINERGICS-UN-OPPOSED ACTION OF THE DILATOR PUPILLAE
- MYDRIASIS. - PASSIVE MYDRIASIS• [Cycloplegia++]• [No light rehlex]
Active and PassiveMydriasis


ActiveMydriasis
PassivePassive mydriasis
Drug Adrenergic Anticholinergic
Muscles Contraction of dilator
Paralysis of constrictor
Cycloplegia Absent Present
Light reflex Present Absent
Conjuctival vessels
Constricted No effect
IOT Decreased or no change
Increased

Systemic EffectsCVS
• Tachycardia-M2 blockade
• Transient initial bradycardia- [Not central action]
• Most blood vessels receive no direct innervation from the parasympathetic system.
• All vessels contain endothelial muscarinic receptors that mediate vasodilation
• These receptors are blocked by antimuscarinic drugs.
[Efect of injected esters]
• At toxic doses, and in some individuals at normal doses, antimuscarinic agents cause cutaneous vasodilation, especially in the upper portion of the body. The mechanism is unknown.
• Cholinergic system not involved in vascular tone
• Tachycardia Vs Direct vasodilation=Net effect

Systemic EffectsRS
• Bronchodilation and decreased secretions
• COPD and preanesthesia
• Can not completely abolish activity[Enteric nervous system]
• Salivary secretion effectively blocked
• Gastric-only basal secretion• Not intestinal and
pancreatic secretions[Hormonal control]
GIT

Systemic EffectsGUT
• Relaxes smooth muscle of the ureters and bladder wall and slows voiding
• Can precipitate urinary retention in men who have prostatic hyperplasia
• Atropine suppresses thermoregulatory sweating
• Body temperature is elevated-therapeutic doses in children
Sweat glands
Atropine toxicity
• Hot as a hare, • Blind as a bat, • Dry as a bone, • Red as a beet,
• Mad as a hatter.

Anticholinergics –Clinical applications
• Mydriatic & Cycloplegic• Respiratory disorders-COPD• CVS disorders• GIT disorders• Disorders of urinary system• Parkinsonism• Motion sickness• Preanesthetic
Drug Onset Duration Remarks
Atropine 30-40 Mts 1 week Useful in childrenHigh ciliary tone
Homatropine 45-60 Mts 1-3 days Unsatisfactory in children
Cyclopentolate 30-60 Mts 1 day Behavioral abnormalities in children[Absorption]
Tropicamide 20-40 Mts 3-6 H Unreliable cycloplegic
Mydriasis-Anticholinergics
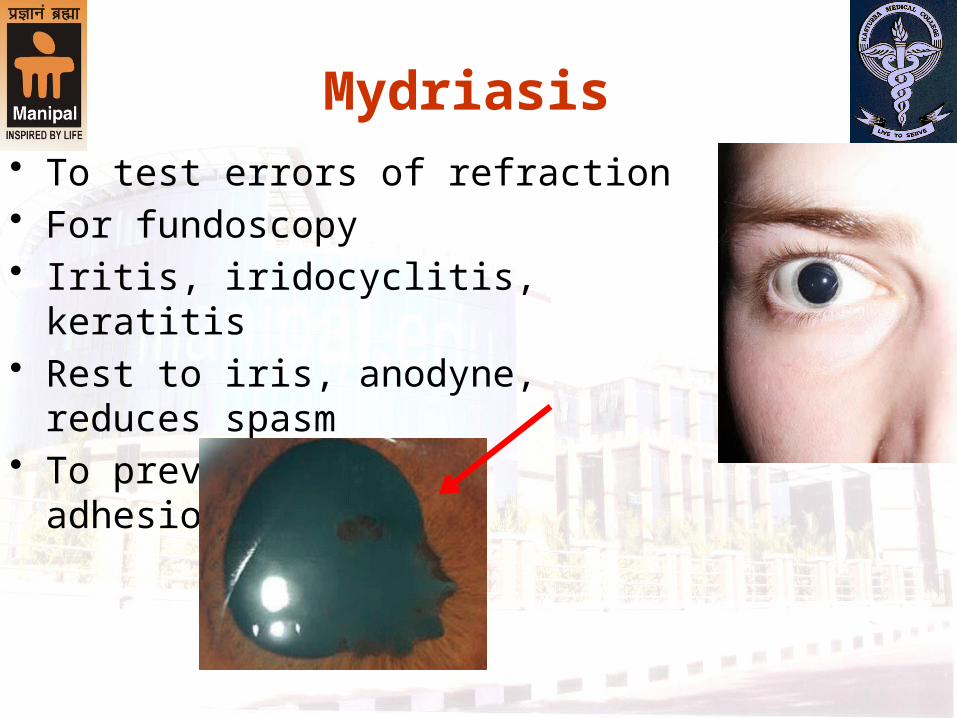
Mydriasis• To test errors of refraction• For fundoscopy• Iritis, iridocyclitis, keratitis• Rest to iris, anodyne, reduces spasm• To prevent/break adhesions[Synechiae]

Respiratory disorders[Ipratropium & Tiotropium]
• COPD & Bronchitis• Less effective in B.Asthma• Orally-dries secretions, • Mucociliary clearance is affected• Inhalational route• Combined with adrenergic agonists

Cardiovascular disorders
• Increased vagal tone- Bradycardia- MI, Digitalis toxicity
• Chaga’s disease-Antibodies to M2 rec.

GIT & Genito-urinary disorders[Antispasmodic]
• Peptic ulcer-not common[Propantheline, oxyphenonium]
• Traveller’s diarrhoea• Intestinal colic, dysmenorrhoea
[Dicyclomine]• Urinary incontinence
[Oxybutynin, Darifenacin , solifenacin, Tolterodine and fesoterodine ]
• Valethamate-Cx dialation
Preanesthetic
• Prior admin.with irritant GA[Ether]• To reduce secretions & prevent
laryngospasm [????]• With Halothane[Sensitizes the heart]• To prevent arrhythmias• To reduce vasovagal reflexes• Atropine & Glycopyrrolate
Atropine

CNS action
Motion sickness• Hyoscine-oral & Transdermal• Prophylactically• Not effective in other vomiting
Parkinsonism• Trihexyphenydyl, procyclidine,Biperiden• In mild cases

Toxicity and DI
Management of Toxicity• Gastric lavage [if ingested] with KMNO4• Cold sponging• Dark room• Physostigmine i.v.• Diazepam
DI
Delays gastric emptying-delays absorption
Antihistaminics, TCA-additive effects


















