
CKWCB-13-04b_OBC_CSS_Exec_Summary_-_Amended_Final_version_ii_24-12-12__2_
35
Outline Business Case for the development of a Clinical Services Strategy Executive Summary – Public Document The Mid Yorkshire Hospitals NHS Trust 24 December 2012
-
Upload
nhs-kirklees -
Category
Documents
-
view
214 -
download
1
description
http://www.kirklees.nhs.uk/fileadmin/documents/meetings/10_January_2013/CKWCB-13-04b_OBC_CSS_Exec_Summary_-_Amended_Final_version_ii_24-12-12__2_.pdf
Transcript of CKWCB-13-04b_OBC_CSS_Exec_Summary_-_Amended_Final_version_ii_24-12-12__2_

Outline Business Case for the development of a Clinical Services Strategy
Executive Summary – Public Document
The Mid Yorkshire Hospitals NHS Trust
24 December 2012

Version 16 OBC: Clinical Services Strategy – Executive Summary
ii
Version 16 OBC: Clinical Services Strategy – Executive Summary
iii
Contents
1 Executive summary (ES)............................................................................................... v
1.1 Introduction .......................................................................................................... v
1.2 Trust profile ........................................................................................................ vi
1.3 Case for change ................................................................................................. xii
1.4 The Strategic Options ........................................................................................ xvi
1.5 Evaluation of the Strategic Options ................................................................ xxvii
1.6 Models of Care for the Preferred Option ......................................................... xxxi
1.7 Procurement .................................................................................................... xxxi
1.8 Affordability Analysis of the Preferred Option ................................................ xxxii
1.9 Project Management ...................................................................................... xxxii
1.10 Stakeholder Engagement and Consultation................................................... xxxv
1.11 Support for the Clinical Services Strategy ...................................................... xxxv
1.12 Conclusion ...................................................................................................... xxxv
Figures
Figure 1 –Trust hospital locations and neighbouring sites ....................................................... viii
Figure 2 – MYHT Hospital Site Distances and Travel Times ................................................... viii
Figure 3 – Trust Activity – 2011/12 ........................................................................................... ix
Figure 4 - Financial data ........................................................................................................... ix
Figure 5 – Services Provided by Division .................................................................................. x
Figure 6 – WTEs at 31st March 2012 by Divisions and Corporate Groups ............................... xi
Figure 7 – Summary Health Profiles: Wakefield and Kirklees ................................................. xiii
Figure 8 – Elements of the Clinical Services Strategy ............................................................ xvii
Figure 9 - CIP breakeven analysis ........................................................................................... xix
Figure 10 –Current location of Services ................................................................................... xxi
Figure 11 – Proposed service locations – Option 1 ................................................................ xxii
Figure 12 – Proposed service locations – Option 2 ............................................................... xxiii
Figure 13 – Service Changes by Option ................................................................................ xxiv
Figure 14 – Current and Modelled Bed Numbers .................................................................. xxvi
Figure 15 – The Option Appraisal Process .......................................................................... xxviii
Figure 16 – Non-financial Appraisal Benefit Criteria ............................................................ xxviii
Figure 17 - Summary of Option Appraisal ............................................................................... xxx
Figure 18 – Preferred Option Capital Funding Profile ............................................................. xxx
Figure 19 – Project Milestones.............................................................................................. xxxii
Figure 20 – Clinical Services Strategy Governance Structure ............................................. xxxiv

Version 16 OBC: Clinical Services Strategy – Executive Summary
iv
Version 16 OBC: Clinical Services Strategy – Executive Summary
v
1 Executive summary (ES)
1.1 Introduction
1.1.1 This Outline Business Case (OBC) presents the case for developing a Clinical Services Strategy for the Mid Yorkshire Hospitals NHS Trust (MYHT). The case addresses the acute services that the Trust provides to the populations of Wakefield and District and North Kirklees and also includes plans to deliver care outside of hospital and the provision of health care across the whole health and social care economy.
1.1.2 The need for a Clinical Services Strategy stems from the challenges that the Mid Yorkshire health economy is facing which are having an impact on quality, sustainability and financial viability across all sectors. These challenges are:
Clinical Safety and Sustainability – there are safety and sustainability risks facing hospital local services, and a very real risk that some services will become unsafe or not sustainable
Demographic Changes – the needs and demographic changes of the different communities served by the Trust across local communities
Clinical Dependencies – maintaining important clinical linkages between hospital services (e.g. the clinical links between obstetrics and neonates, and the medical cover arrangements between neonates and paediatrics)
Loss of Market Share to other Providers – patients from Mid Yorkshire choosing other providers which can provide better access to outpatient appointments.
Specialist Commissioning – future loss of Trust services which are unable to meet SCG guidance or have to be provided for populations greater than 500k
Medical Workforce – issues such as restrictions in working hours for junior doctors, reduced opportunities for international recruitment and a medical training programme resulting in earlier specialisation and a narrower expertise set and in some specialties smaller numbers of available staff
Quality Governance and External scrutiny – an environment of increasing external scrutiny of health services, including from Monitor and the Care Quality Commission and the implications of the Health and Social Care Act
Use of Hospital Facilities and Estate - the revenue implications from previous capital investment and the need to ensure capacity is in the right place to support the changing demand for services
Socio-political environment – the prolonged debate on the future shape of hospital services without resolution: the current risks are getting harder to manage and the opportunities for solving them are reducing
1.1.3 In the context of focussing on the provision of care outside of hospital, the above challenges have driven the overarching objective for the reconfiguration of hospital services, which is to secure high quality, safe and sustainable hospital services in Mid Yorkshire. With this in mind the Trust and its commissioning partners have reviewed the different options for where services could be located on each site. Specific consideration has been made to delivering a clinically safe model of care i.e. maintaining key clinical adjacencies, ensuring there is capacity in the right location, supporting longer term national strategic developments for specialist services and providing value for money whilst ensuring affordability in the immediate and longer term.
1.1.4 This document sets out the case for change and the process undertaken to identify a short list of service configuration options. It describes the option appraisal process to evaluate each of the short listed options and to conclude on a preferred service configuration. The document then considers the procurement and financial consequences of the preferred option in more detail and concludes by describing how the project will be
Version 16 OBC: Clinical Services Strategy – Executive Summary
vi
managed through to completion. When this OBC is approved, the preferred service configuration will be subject to public consultation across Wakefield District and North Kirklees.
1.1.5 The clinical service strategy programme was established in the summer of 2012 with the overarching objective to address the following challenges facing the local health economy:
Making services safer now and in the future;
Making services sustainable now and in the future;
Making services financially viable in the medium and long terms.
1.1.6 This document has arisen from:
The Mid Yorkshire Health and Social Care partnership Transformation Programme and work streams, focusing on out of hospital care, long term conditions, urgent care and children’s and maternity services;
Previous reviews of the Mid Yorkshire health system undertaken by the national Clinical Advisory Team (NCAT);
A detailed feasibility study including a capacity validation exercise undertaken by the Trust and clinical commissioners.
1.2 Trust profile
1.2.1 The Mid Yorkshire Hospitals NHS Trust was formed in 2002 and is responsible for three major acute hospitals, serving a population of approximately 550,000 people. In April 2010, the Trust took over responsibility for providing community services for the population of Wakefield District.
1.2.2 The Trust’s Values were developed by our staff and set out how we will work with our partners, communities and patients;
Caring and compassionate – we care about everything we do, everyone who uses our services, the colleagues and partners we work with, our Trust and the NHS. We aim to put patients first in everything we do and look for ways to make people’s lives better.
Commitment to the highest standards of patient care – we take personal and collective responsibility to always do the very best that we can to provide the best services and best patient experience.
Improving and innovating – we strive to be a learning organisation, always looking for ways to improve what we do. We encourage involvement, value contributions and listen to and positively act on feedback.
Respect – we embrace diversity, value and respect everyone as an individual and treat others as they would wish to be treated. We are open and honest and act with professionalism, courtesy and integrity at all times.
1.2.3 Our aim is to place Mid Yorkshire within the top 10% of NHS organisations against all standards between now and 2015. We will make the necessary improvements and reduce our costs to ensure that local people have access to the best possible services now and in the future.
1.2.4 In 2010, the Trust started providing community therapy services and intermediate care services. In April 2011, the Trust further expanded to provide community health services for the Wakefield district to include adult community nursing and children’s and families’ health services to become a new integrated care organisation for local people.
Version 16 OBC: Clinical Services Strategy – Executive Summary
vii
1.2.5 Nine key sites are central to the delivery of the Trust's services1, which are:
Pinderfields Hospital (715 beds - new PFI hospital).
Dewsbury & District Hospital (412 beds).
Pontefract Hospital (64 beds - new PFI hospital).
Clayton Hospital (due for closure by 31st December 2012).
Queen Elizabeth House (26 beds - intermediate care).
Kingsdale (28 beds – intermediate care purchased from BUPA)
Monument House (24 beds - intermediate care).
Newstead House (community dental).
Castleford and Normanton District Hospital (community services)
1.2.6 The Trust has 1,191 hospital beds, including critical care, across the three main acute sites and there are also 78 beds in intermediate care facilities.
Catchment Population
1.2.7 The Trust provides services to the people of Wakefield, Pontefract and the towns of Castleford, Normanton, Featherstone and Knottingley, and North Kirklees (Batley, Birstall, Cleckheaton, Dewsbury, Heckmondwike, Liversedge, Gomersal and Mirfield). The population of Wakefield and Pontefract is approximately 322,000 with North Kirklees being approximately 177,347. These are the Trust's core catchment areas.
1.2.8 The Trust has hospital sites in Wakefield District and North Kirklees. Figure 1 shows the location of the Trust's hospital sites providing acute services in relation to each other and other local NHS and private providers.
1 Community service provision takes place in over 70 community settings.
Version 16 OBC: Clinical Services Strategy – Executive Summary
viii
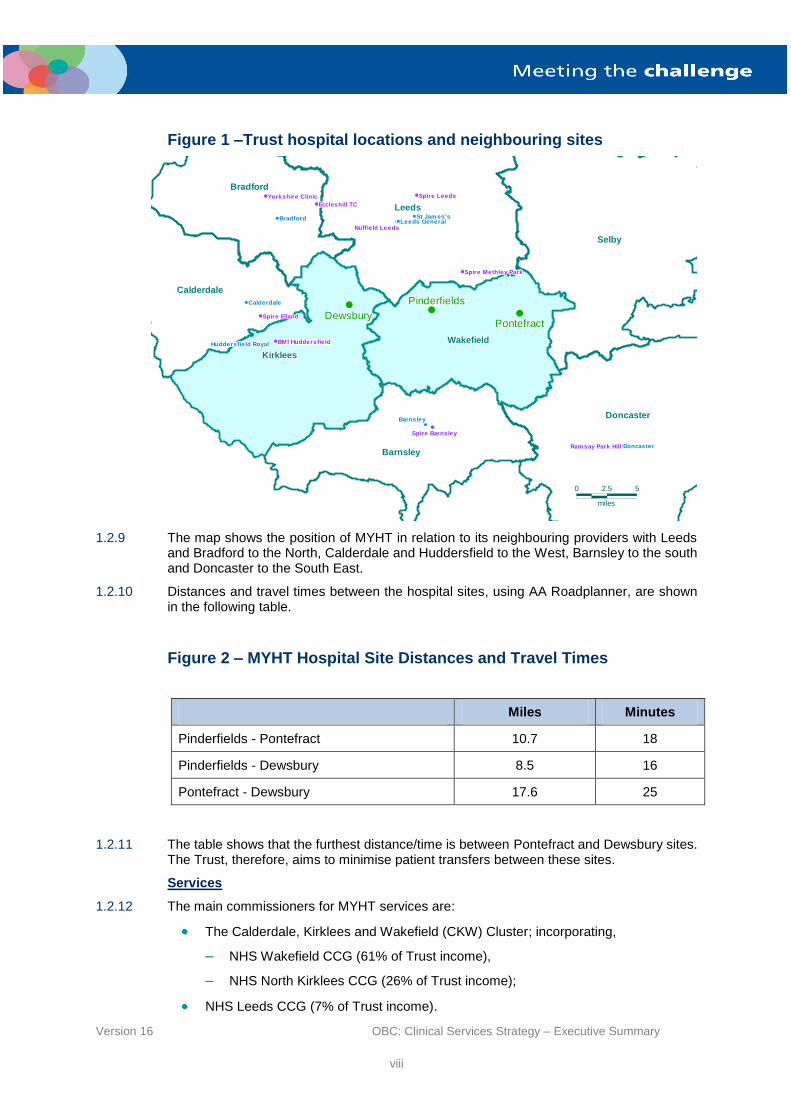
Figure 1 –Trust hospital locations and neighbouring sites
1.2.9 The map shows the position of MYHT in relation to its neighbouring providers with Leeds and Bradford to the North, Calderdale and Huddersfield to the West, Barnsley to the south and Doncaster to the South East.
1.2.10 Distances and travel times between the hospital sites, using AA Roadplanner, are shown in the following table.
Figure 2 – MYHT Hospital Site Distances and Travel Times
Miles Minutes
Pinderfields - Pontefract 10.7 18
Pinderfields - Dewsbury 8.5 16
Pontefract - Dewsbury 17.6 25
1.2.11 The table shows that the furthest distance/time is between Pontefract and Dewsbury sites. The Trust, therefore, aims to minimise patient transfers between these sites.
Services
1.2.12 The main commissioners for MYHT services are:
The Calderdale, Kirklees and Wakefield (CKW) Cluster; incorporating,
– NHS Wakefield CCG (61% of Trust income),
– NHS North Kirklees CCG (26% of Trust income);
NHS Leeds CCG (7% of Trust income).
0000000000000000000000000000000000000000000000000 2.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.52.5 5555555555555555555555555555555555555555555555555
milesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmilesmiles
LeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeeds
BarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsley
BradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradford
KirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirklees
WakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefieldWakefield
CalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdale
SelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelbySelby
DoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncaster
Nuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield LeedsNuffield Leeds
Spire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire BarnsleySpire Barnsley
Spire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley ParkSpire Methley Park
Eccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TCEccleshill TC
Yorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire ClinicYorkshire Clinic
Spire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire EllandSpire Elland
BMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI HuddersfieldBMI Huddersfield
Ramsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park HillRamsay Park Hill
Spire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire LeedsSpire Leeds
Leeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds GeneralLeeds General
BarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsley
BradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradfordBradford
CalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdale
Huddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield RoyalHuddersfield Royal
DoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncaster
St Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es'sSt Jam es's
DewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsburyDewsbury
PinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfieldsPinderfields
PontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefractPontefract

Version 16 OBC: Clinical Services Strategy – Executive Summary
ix
1.2.13 The Trust provides a full range of secondary acute services with the addition of plastic surgery, burns treatment and spinal injuries. Its activity in 2011/12 is summarised in the table below.
Figure 3 – Trust Activity – 2011/12
Medical Surgical Integrated Care (including Women’s and Children’s and
Clinical Support Services)
Total
Day Case 21,263 28,497 4,438 54,198
Elective FCEs 1,848 10,601 1,758 14,207
Elective Bed days and zero LOS
10,001 26,271 2,803 39,075
Non elective FCEs 54,520 19,674 31,899 106,093
Non-elective bed days and zero LOS
238,207 62,954 42,568 343,729
Financial Position
1.2.14 The financial position of MYHT has been a matter of significant scrutiny during 2011/12 and 2012/13. In 2011/12, the Trust reported a £19.2m deficit which comprised both underlying matters and non-recurrent costs and income.
1.2.15 An external review on strategic viability was commissioned by Yorkshire and Humber SHA in 2011, which led to the development of a number of five initial options. However, once the scale of the challenges became clear, a more radical solution was required and two options were then taken forward for development, which now form the basis of this OBC for the Clinical Services Strategy (CSS).
1.2.16 In 2012/13, the Trust set a deficit budget of £26.0m which represented an assessment of its ability to deliver 5.4% CIPs in-year and included healthcare economy support of £10m.
1.2.17 The following table identifies the key financial information for the Trust. 2
Figure 4 - Financial data
2010/11
Actual
£m
2011/12
Actual
£m
2012/13
Forecast
£m
Turnover 432.0 457.0 434.5
Operational Surplus (deficit) 2.5 (19.2) (26.0)
Cash balance at year end 15.2 3.5 12.6
2 Financial data is as per restated accounts
Version 16 OBC: Clinical Services Strategy – Executive Summary
x
2010/11
Actual
£m
2011/12
Actual
£m
2012/13
Forecast
£m
External Financing Limit – under / (over) shoot Met Not Met Planned Met
3.5% Capital Absorption Limit Met Met Met
Capital Resource Limit – Total Met Met Met
Reference Costs 109 111 n/a
Operational Profile
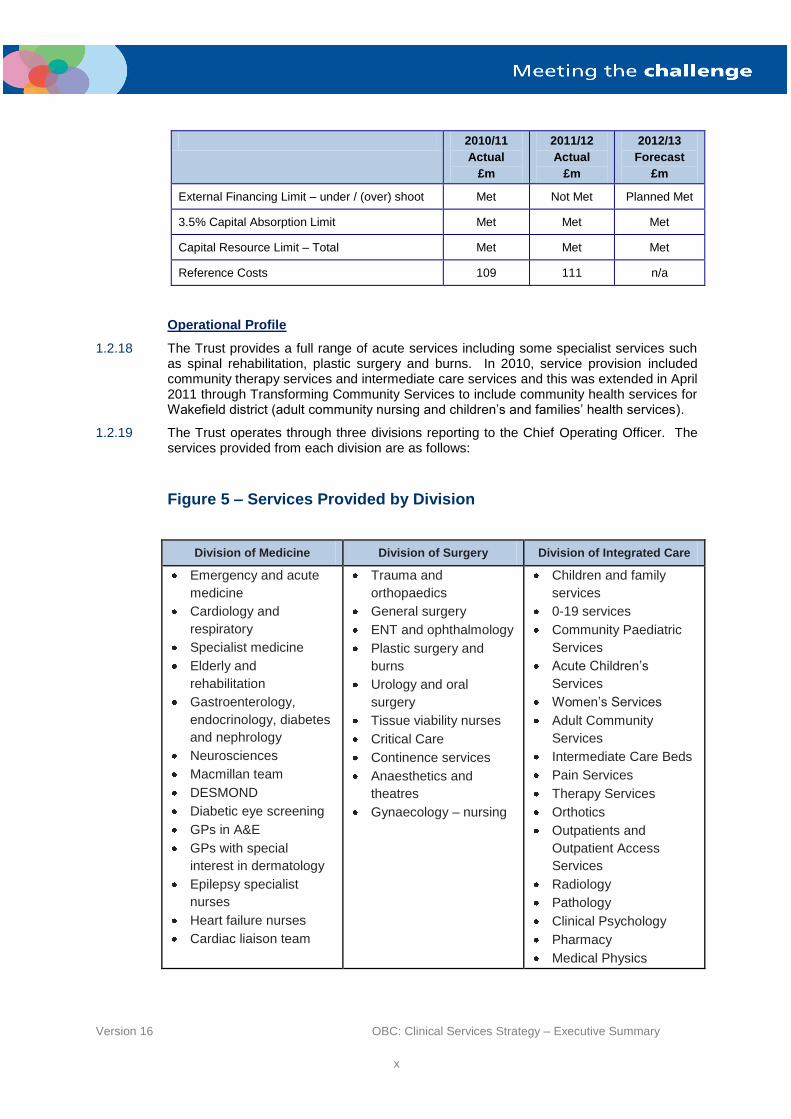
1.2.18 The Trust provides a full range of acute services including some specialist services such as spinal rehabilitation, plastic surgery and burns. In 2010, service provision included community therapy services and intermediate care services and this was extended in April 2011 through Transforming Community Services to include community health services for Wakefield district (adult community nursing and children’s and families’ health services).
1.2.19 The Trust operates through three divisions reporting to the Chief Operating Officer. The services provided from each division are as follows:
Figure 5 – Services Provided by Division
Division of Medicine Division of Surgery Division of Integrated Care
Emergency and acute
medicine
Cardiology and
respiratory
Specialist medicine
Elderly and
rehabilitation
Gastroenterology,
endocrinology, diabetes
and nephrology
Neurosciences
Macmillan team
DESMOND
Diabetic eye screening
GPs in A&E
GPs with special
interest in dermatology
Epilepsy specialist
nurses
Heart failure nurses
Cardiac liaison team
Trauma and
orthopaedics
General surgery
ENT and ophthalmology
Plastic surgery and
burns
Urology and oral
surgery
Tissue viability nurses
Critical Care
Continence services
Anaesthetics and
theatres
Gynaecology – nursing
Children and family
services
0-19 services
Community Paediatric
Services
Acute Children’s
Services
Women’s Services
Adult Community
Services
Intermediate Care Beds
Pain Services
Therapy Services
Orthotics
Outpatients and
Outpatient Access
Services
Radiology
Pathology
Clinical Psychology
Pharmacy
Medical Physics

Version 16 OBC: Clinical Services Strategy – Executive Summary
xi
Staff Profile
1.2.20 A summary of the number of Whole Time Equivalent (WTE) employees employed by the Trust as at 31
st March 2012 by Division, Corporate Services and site is shown in the
following table.
Figure 6 – WTEs at 31st March 2012 by Divisions and Corporate Groups
Staff Group Division of Medicine
Division of Surgery
Division of Integrated
Care
Corporate Services
Site Services
Grand Total
Medical and Dental 296.3 294.9 175.7 3.0 769.9
Nursing & Midwifery Registered
877.6 545.5 766.5 46.5 39.7 2,236.1
Allied Health Professionals
6.0 7.4 473.6 487.0
Healthcare Scientists 26.0 12.4 129.0 167.4
Additional professional, scientific and technical
7.8 70.9 94.8 5.1 178.6
Admin and clerical 234.8 188.4 385.2 361.7 51.4 1,221.5
Additional Clinical Services
397.8 245.0 535.9 27.1 1,205.8
Estates & Ancillary 7.7 84.5 14.0 5.0 415.5 526.7
Senior Managers 8.0 11.0 17.5 45.0 13.1 94.6
Total 1,862.0 1,459.9 2,592.2 493.4 480.1 6,887.6
1.2.21 The Trust employs over 6,800 staff (Whole Time Equivalents) following the integration of Wakefield Community services in 2011. The Trust formally launched a 90 day consultation in May on measures to reduce workforce costs which is resulting in a reduction in headcount and paybill.
Trust Estate
1.2.22 In April 2011, the Hospitals Development Project was completed with the new hospitals at Pinderfields and Pontefract becoming fully operational. As a result, over 90% of the buildings’ physical condition at Pinderfields is at level A as are just fewer than 80% of those at Pontefract. Most of the buildings on the Pinderfields site are fully occupied, however, some of the facilities at Pontefract are under-utilised.
1.2.23 Approximately 80% of the building stock at Dewsbury is less than 30 years old and 65% of the physical condition is at level B, which is satisfactory. However, 98% of buildings at Clayton are at level C or below. The Trust is to close Clayton Hospital by 31
st December
2012. In addition, the South side of Pontefract Hospital, which comprises buildings of a poor standard, will be closed at the same time.
1.2.24 The Trust has completed a utilisation review of Pontefract Hospital and has agreed plans to improve utilisation by increasing the range of services to be provided. The proposed services have been agreed by the Wakefield District commissioners. Some of these changes have already been implemented.

Version 16 OBC: Clinical Services Strategy – Executive Summary
xii
1.3 Case for change
1.3.1 There are six key reasons for making significant changes in the way healthcare is delivered in Mid Yorkshire:
Reason one: the need to adopt new models of care and best practice which can deliver better outcomes for patients and deliver safe and excellent quality services;
Reason two: the need to improve the health of people in Wakefield and North Kirklees and ensure healthcare services are meeting public expectations;
Reason three: the population is rising and ageing leading to greater and different demands on health services;
Reason four: hospital is not always the answer; more care can be delivered in community settings than ever before and patients benefit from care closer to home;
Reason five: there are workforce challenges which currently prevent delivery of the best quality care and optimal patient outcomes; and
Reason six: the need to make best use of taxpayers’ money.
1.3.2 The greatest priority is to ensure that safe and excellent quality services are provided to the population of MYHT in to the long term.
1.3.3 The prime focus of the strategy is to ensure the future sustainability of acute services taking into consideration key factors such as the changing medical workforce and junior doctor training together with new service standards and specialist commissioning requirements.
1.3.4 In addition there is a need to contribute significantly to the financial viability of the Trust for the future.
Commissioning Strategies
1.3.5 NHS Wakefield CCG and NHS North Kirklees CCG have written a strategic commissioning vision document: “Meeting the challenge – our strategic commissioning vision” (see Annex 1). The vision is:
“To improve the standard of Urgent Care in Wakefield and North Kirklees through the development of care closer to home and a high quality, clinically safe system that is easy for both patients and professionals to navigate through and provides outstanding value
for money”.
1.3.6 The joint commitment of the CCGs translates into five key themes:
Improved access to high quality, responsive primary care – to make out-of-hospital care the first point of call for most people;
Rapid response to urgent needs – so that fewer patients need to access hospital inpatient
emergency care;
Providers (social and health) – working together with the patient at the centre to proactively manage LTCs, the elderly and end-of-life care out of hospital;
Simplified planned care pathways – that ensure larger proportion of care is not delivered in a hospital setting;
Appropriate time in hospital – when admitted, with early supported discharge into well organised community / social care.
1.3.7 In order to transform the whole health and social care system the commissioners have developed a set of deliverable plans, designed to co-ordinate a series of cross-organisational initiatives. These focus on the following service areas:
Urgent care services;
Version 16 OBC: Clinical Services Strategy – Executive Summary
xiii
Care closer to home;
Children’s and young people service models.
Population
1.3.8 In Wakefield, the population is forecast to grow in line with England, rising by 2.8% over the next five years. Population growth will be highest in those aged 65 and over, with an increase of around 14.4%. The projected growth in the Kirklees population over the next five years is 3.8% with a similar forecast for a proportionately greater increase in those over 65, around 14.3%. The elderly are the heaviest users of health care services.
1.3.9 The Trust serves an area with significant social deprivation. The Index of Multiple Deprivation (IMD) in 2010:
Ranks Kirklees as the 77th most deprived district in England (out of 326 districts)
and 58th most deprived local authority in England (out of 354 local authorities);
Ranks Wakefield as the 67th most deprived district in England (out of 326 districts)
and ranked 66th most deprived local authority in England (out of 354 authorities).
1.3.10 Kirklees has 28% of its population on the most deprived national quintile and 12.2% of the population in the least deprived quintile. Similarly, Wakefield District has 28.8% of its population in the most deprived national quintile and 8.3% of the population in the least deprived quintile
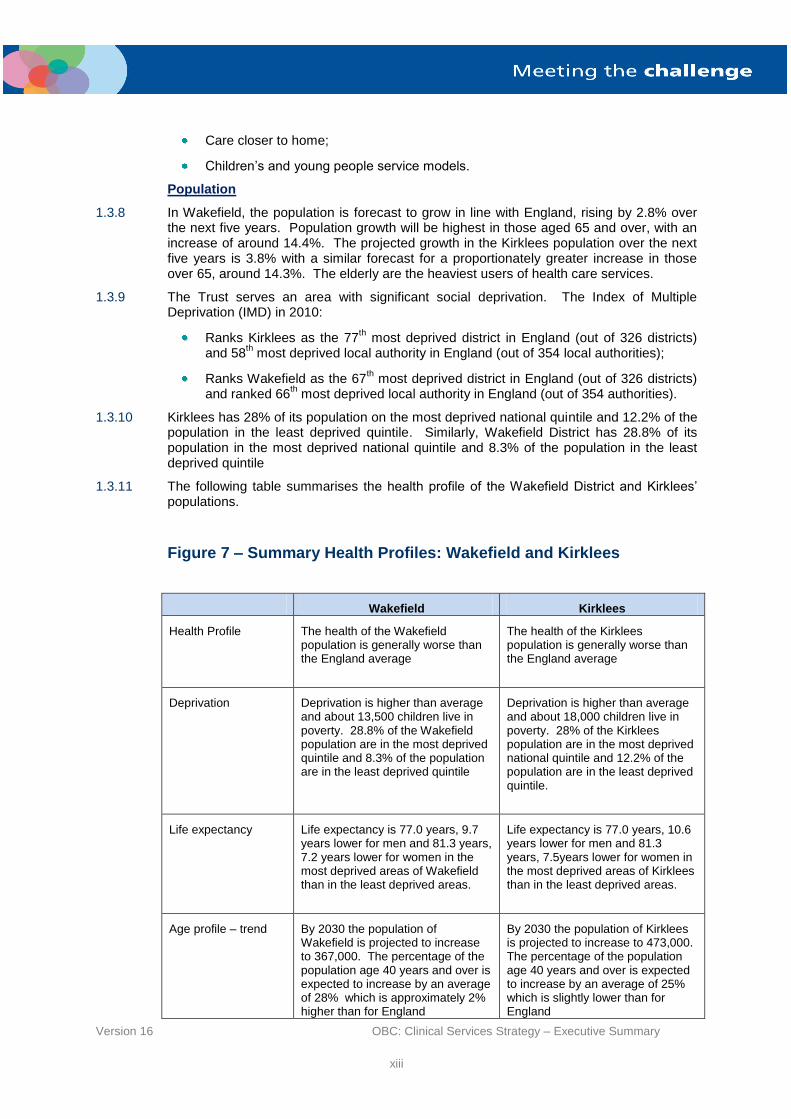
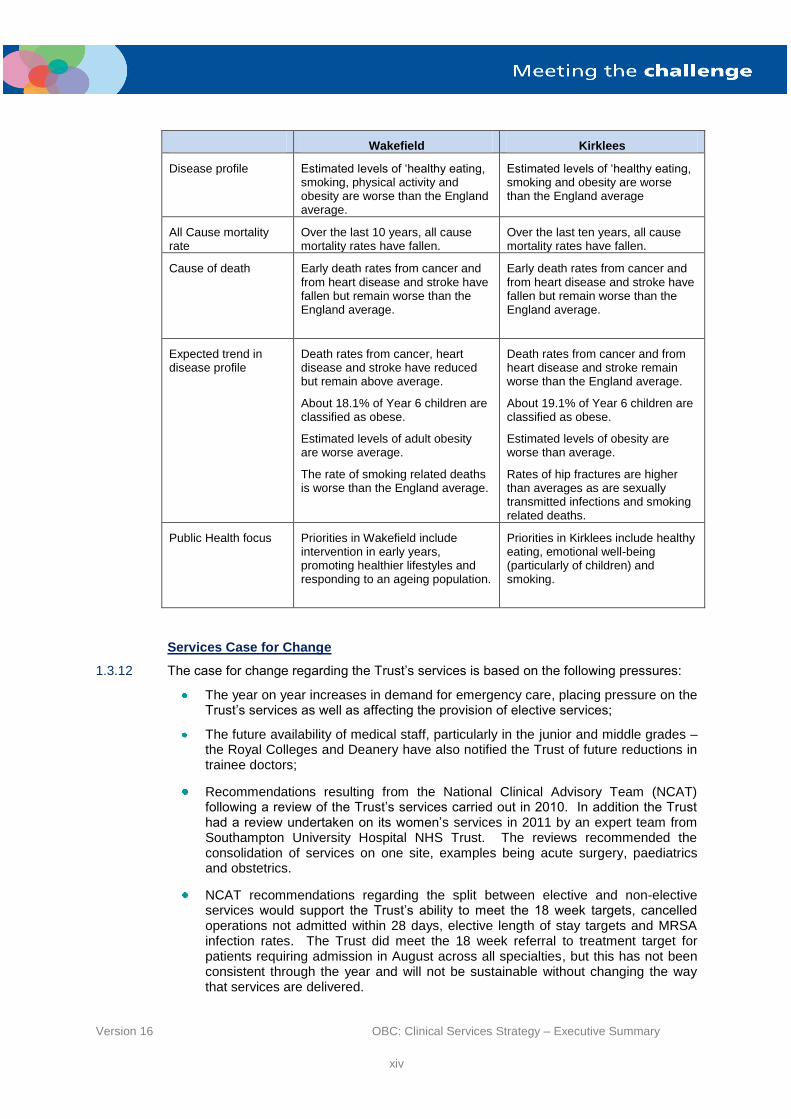
1.3.11 The following table summarises the health profile of the Wakefield District and Kirklees’ populations.
Figure 7 – Summary Health Profiles: Wakefield and Kirklees
Wakefield Kirklees
Health Profile The health of the Wakefield population is generally worse than the England average
The health of the Kirklees population is generally worse than the England average
Deprivation Deprivation is higher than average and about 13,500 children live in poverty. 28.8% of the Wakefield population are in the most deprived quintile and 8.3% of the population are in the least deprived quintile
Deprivation is higher than average and about 18,000 children live in poverty. 28% of the Kirklees population are in the most deprived national quintile and 12.2% of the population are in the least deprived quintile.
Life expectancy Life expectancy is 77.0 years, 9.7 years lower for men and 81.3 years, 7.2 years lower for women in the most deprived areas of Wakefield than in the least deprived areas.
Life expectancy is 77.0 years, 10.6 years lower for men and 81.3 years, 7.5years lower for women in the most deprived areas of Kirklees than in the least deprived areas.
Age profile – trend By 2030 the population of Wakefield is projected to increase to 367,000. The percentage of the population age 40 years and over is expected to increase by an average of 28% which is approximately 2% higher than for England
By 2030 the population of Kirklees is projected to increase to 473,000. The percentage of the population age 40 years and over is expected to increase by an average of 25% which is slightly lower than for England
Version 16 OBC: Clinical Services Strategy – Executive Summary
xiv
Wakefield Kirklees
Disease profile Estimated levels of ‘healthy eating, smoking, physical activity and obesity are worse than the England average.
Estimated levels of ‘healthy eating, smoking and obesity are worse than the England average
All Cause mortality rate
Over the last 10 years, all cause mortality rates have fallen.
Over the last ten years, all cause mortality rates have fallen.
Cause of death Early death rates from cancer and from heart disease and stroke have fallen but remain worse than the England average.
Early death rates from cancer and from heart disease and stroke have fallen but remain worse than the England average.
Expected trend in disease profile
Death rates from cancer, heart disease and stroke have reduced but remain above average.
About 18.1% of Year 6 children are classified as obese.
Estimated levels of adult obesity are worse average.
The rate of smoking related deaths is worse than the England average.
Death rates from cancer and from heart disease and stroke remain worse than the England average.
About 19.1% of Year 6 children are classified as obese.
Estimated levels of obesity are worse than average.
Rates of hip fractures are higher than averages as are sexually transmitted infections and smoking related deaths.
Public Health focus Priorities in Wakefield include intervention in early years, promoting healthier lifestyles and responding to an ageing population.
Priorities in Kirklees include healthy eating, emotional well-being (particularly of children) and smoking.
Services Case for Change
1.3.12 The case for change regarding the Trust’s services is based on the following pressures:
The year on year increases in demand for emergency care, placing pressure on the Trust’s services as well as affecting the provision of elective services;
The future availability of medical staff, particularly in the junior and middle grades – the Royal Colleges and Deanery have also notified the Trust of future reductions in trainee doctors;
Recommendations resulting from the National Clinical Advisory Team (NCAT) following a review of the Trust’s services carried out in 2010. In addition the Trust had a review undertaken on its women’s services in 2011 by an expert team from Southampton University Hospital NHS Trust. The reviews recommended the consolidation of services on one site, examples being acute surgery, paediatrics and obstetrics.
NCAT recommendations regarding the split between elective and non-elective services would support the Trust’s ability to meet the 18 week targets, cancelled operations not admitted within 28 days, elective length of stay targets and MRSA infection rates. The Trust did meet the 18 week referral to treatment target for patients requiring admission in August across all specialties, but this has not been consistent through the year and will not be sustainable without changing the way that services are delivered.
Version 16 OBC: Clinical Services Strategy – Executive Summary
xv
Care outside of Hospital
1.3.13 The Trust is committed to working in partnership with the wider health and social care economy to develop integrated services. This has been helped by the transfer of the community services provided to the population of Wakefield District, formerly provided by NHS Wakefield in April 2011.
1.3.14 A transformation programme has been established, overseen by the Mid Yorkshire Health and Social Care Partnership Programme Board, and will encompass:
Urgent Care;
Care outside of hospital (including Long Term Conditions, the Frail Elderly, End of Life Care; and
Children’s and Maternity Services.
1.3.15 The transformation agenda has a clear aspiration for more integrated models of care and a focus on the provision of care outside of hospital as much as best practice, realising benefits such as:
Improved patient experience and efficiency through hospital avoidance;
Reduced length of stay;
A reduction in unnecessary re-admissions;
Improved experience for service users, carers and families, particularly where the acute/hospital episode may not be provided at a local hospital;
Delivery of continually improving quality of care and value for money/cost improvements;
Delivery of services which are designed around the needs of patients; and
Improved partnership working across clinical services and clinicians.
Finance
1.3.16 In common with the NHS acute sector, the national efficiency requirement of 5% per annum to 2014/15 and 4.2% per annum beyond presents a material financial challenge to MYHT.
1.3.17 The Trust has undertaken a high level assessment of its financial position which includes the national efficiency requirements. The Trust has established a 6% per annum CIP which presents the highest level of annual efficiency considered to be achievable. Additionally, it has worked with commissioners to understand the high level impact of QIPP on income and costs.
1.3.18 The Trust estimates that, should it proceed to 2016/17 without reconfiguration, then a residual deficit would remain of circa £20m. The reconfiguration of clinical services is expected to provide some significant opportunities for realising efficiencies.
1.3.19 The scale of the financial challenge over the planning period is summarised as follows:
Cost improvement challenges - £120m
Reductions related to QIPP - £11m
Resolution of the residual deficit at 2016/17 - £20m.
1.3.20 The potential reconfiguration of services presents opportunities to increase efficiency and reduce costs in particular via:
Economies of scale through consolidation and centralisation;

Version 16 OBC: Clinical Services Strategy – Executive Summary
xvi
Efficiencies for the Trust and the health economy through changes to patient pathways, specialisation and improving outcomes
Staffing
1.3.21 The Trust recognises that the current staffing structures will need to change to meet with current developments in the health care provision. Drivers for this change are:
Shift towards an increase in consultant-led and consultant-delivered care;
Integration of secondary care and community services;
Development of care outside of hospital;
Royal College recommendations, for example, reduction in inpatient sites (Royal College of Paediatrics), national cancer guidelines regarding colorectal services and access to appropriately trained medical staff within defined timescales;
Opportunity to introduce new roles to either replace or supplement medical posts such as Neonatal Nurse Practitioners at enhanced or advanced levels; Advanced Nurse Practitioners in varying specialties such as Paediatrics, Orthopaedics and Physician’s Assistants;
Reliance on expensive locums to cover gaps in rotas. In common with other trusts, MYHT has experienced continuing difficulties in recruiting medical staff, particularly to mid-grade posts. As a result, it is experiencing high costs for use of locum staff and had to change the status of the ED at Pontefract to an 8am to 8pm service to cope with the shortages. A temporary solution has been found and the ED is now working on a 24 hour basis with GP staffing from 8pm to 8am. Shortages of middle grade staff are also acute in paediatrics, obstetrics, ENT and ophthalmology;
A reduction in medical training grade posts. In September 2011 the Deanery notified the Trust of planned reductions in training posts for 2012 and 2013.
1.3.22 The Trust has identified the following risks relating to future workforce supply:
A reduction in medical training posts - in September 2011 the Deanery notified the Trust of planned reductions in training posts for 2012 and 2013;
Increasing reliance on locums – with the above shortages the Trust is increasingly having to rely on locums with the resulting increase in costs;
Inability to recruit to non-training posts.
1.3.23 As a result of the above risks, the Trust needs to consider alternative methods of providing care including more consultants, advanced nursing roles and centralisation of surgical services to take account of the loss of training posts.
1.3.24 Clinical options for reconfiguring services will, therefore, need to take into account the current shortages and planned reductions in training posts to ensure the long term sustainability of services.
1.4 The Strategic Options
Strategic Vision
1.4.1 The strategic vision of the organisation is to operate as an integrated care organisation, delivering comprehensive models of care across community and hospital pathways which offer better patient outcomes and experience and improved efficiency and productivity, working closely with the wider health and social care economy to develop care pathways that provide services to patients in the right place, at the right time by the right people.
1.4.2 The Clinical Services Strategy consists of a combination of prevention and enablement, care outside of hospital and quality hospital care focussed on:
Improving health;

Version 16 OBC: Clinical Services Strategy – Executive Summary
xvii
Integrating hospital & community services;
Creating centres of excellence;
An interdependency between sites and services;
Working in partnerships; and
Ensuring clinically and financial viability.
Figure 8 – Elements of the Clinical Services Strategy
1.4.3 The Trust Board has agreed five strategic goals that will underpin its strategy going forward.
Driving improvement in service quality, safety and performance so that we always compare well with the best organisations;
Promoting better ways of working between community and hospital services so that people are treated in the best place for them, by staff who have the most appropriate skills;
Investing in customer care so that people’s experience of using our services is the best it can be;
Encouraging lifelong learning and research to develop a skilled and motivated workforce;
Working as part of the wider health and social care community to improve
opportunity and life chances for the population.
1.4.4 Successful delivery of this vision will require increased efficiency in both hospital and community services achieved through the elimination of duplication, optimising use of resources and ensuring people are cared for in the most appropriate setting by the most appropriate clinical team.
Prevention and
enablement
Quality
hospital care
Care outside of hospital

Version 16 OBC: Clinical Services Strategy – Executive Summary
xviii
Objectives and Constraints
1.4.5 The Clinical Service Strategy (CSS) objectives are:
To achieve better clinical outcomes and clinical sustainability by concentrating clinical capability and optimising volumes of activity.
To improve efficiency and productivity to support long term financial viability by enabling more efficient flows of non-elective work by best use of available resources, delivering 18 week referral to treatment, delivering services on multiple
sites only when clinically necessary.
To ensure safe and appropriate patient travelling times.
To deliver benefits as quickly as possible.
1.4.6 The agreed constraints were:
Patient safety must be assured.
Services must be viable in terms of workforce, including the necessary support services, for example critical care.
Scenarios must be clinically endorsed by the Medical Director, Divisional Directors and Chief Nursing Officer and reflect national guidance and key local recommendations, for example NICE, NCAT and GP consortia Chairs.
Scenarios must minimise the need for additional capacity.
Scenarios must maximise the utilisation of the PFI capacity.
Scenarios must not result in overall cost increases to the Trust unless there is robust evidence that they will increase Trust income by more than cost increases.
Pinderfields must be the major trauma site.
Care Outside of Hospital
1.4.7 The proposals for care outside of hospital apply equally to the options under consideration. The planning assumptions underpinning the OBC are predicated on a greater proportion of activity taking place in other settings in future, either within primary care, in the community or in people’s homes, as well as increased emphasis on self-care and promoting independence.
1.4.8 Work is currently underway by NHS North Kirklees CCG and NHS Wakefield CCG to assess the scope and scale of transformation planned over the next five years based on:
Assessment of delivery of transformation to date
Joint strategic needs assessments
Epidemiology, demography
Workforce and financial projections
The clinical service strategy
1.4.9 Details of the transformation programmes will be developed over the coming months. MYHT is committed to working in partnership with the CCGs, the local authorities and other providers to develop and deliver the whole system transformation programme
1.4.10 Programmes have been developed for:
Adult Community services using a proposed Discharge to Access model.
Urgent Care where the aims are to reduce Emergency Department attendances and emergency admissions through increasing capacity within primary care in areas such as access and long term condition care planning.
Version 16 OBC: Clinical Services Strategy – Executive Summary
xix
Children’s services where care pathways will be designed to address specific conditions such as the provision of intravenous injections in the community, diarrhoea and vomiting, respiratory conditions and long term conditions.
End of Life Care where community services are being developed to improve end of life care for patients, ensuring that patients receive palliative care needs in the community rather than in an acute hospital bed.
Technology ensuring patients have access to up to date information about services as they are introduced, increased use of telehealth and developing a technology infrastructure to support the development of the new care pathways.
1.4.11 Specific examples that are in development include:
A proposed care pathway for discharge to assess with locality intermediate tier teams and Acute Community Nursing teams, focussing on the provision of services to GP Clusters;
The Primary Care Transformation Scheme aimed at reducing attendances and ED by 8% with resulting reductions in emergency admissions of 14%; and
A recently- launched rapid response service for patients receiving End of Life Care, which will extend the provision of hospice care out of hours.
Hospital Configuration – the Strategic Options
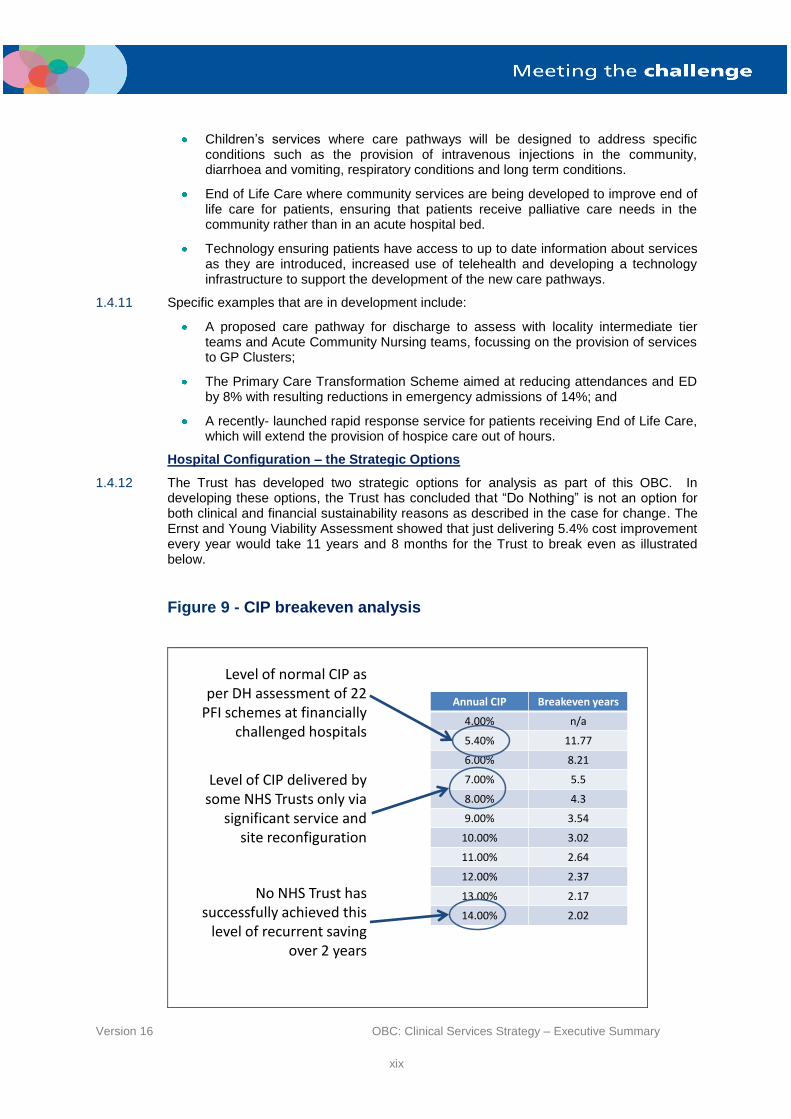
1.4.12 The Trust has developed two strategic options for analysis as part of this OBC. In developing these options, the Trust has concluded that “Do Nothing” is not an option for both clinical and financial sustainability reasons as described in the case for change. The Ernst and Young Viability Assessment showed that just delivering 5.4% cost improvement every year would take 11 years and 8 months for the Trust to break even as illustrated below.
Figure 9 - CIP breakeven analysis
Level of CIP delivered by some NHS Trusts only via
significant service and site reconfiguration
Annual CIP Breakeven years
4.00% n/a
5.40% 11.77
6.00% 8.21
7.00% 5.5
8.00% 4.3
9.00% 3.54
10.00% 3.02
11.00% 2.64
12.00% 2.37
13.00% 2.17
14.00% 2.02
No NHS Trust has successfully achieved this
level of recurrent saving over 2 years
Level of normal CIP as per DH assessment of 22
PFI schemes at financially challenged hospitals

Version 16 OBC: Clinical Services Strategy – Executive Summary
xx
1.4.13 The two service configuration options are:
Option 1 – service changes developed to deliver clinical sustainability in the most challenged areas only (i.e. the option that resolves the Pontefract ED and consolidates paediatrics, consultant led obstetrics and acute and elective general and colorectal surgery onto the Pinderfields site); and
Option 2 – radical service changes developed to deliver clinical, performance and contributes significantly to financial sustainability (i.e. delivering a different model of care from the three hospital sites).
1.4.14 Common to both options will be the proposed reconfiguration of services at Pontefract which has been the subject of a site utilisation review, completed in May 2012. In addition, there are proposed changes for the 2012/13 financial year that will not compromise any future service configurations. These are:
Developing specialist ophthalmology and orthopaedic elective treatment centres at Pontefract, maintaining the current centres for both services at Dewsbury; and
Relocation of (sub-regional) neurological rehabilitation services from Pinderfields to Dewsbury.
1.4.15 As option 1 achieves clinical sustainability in the specified services only, it can be regarded as the minimum changes necessary to ensure the Trust operates a clinically safe service in line with the minimum requirements set out in the NCAT review. However, it does not address the longer term challenges of ensuring the clinical sustainability of all services such as Emergency Care. As such, it can be regarded as the “Do Minimum” option.
1.4.16 The following table shows the service configurations for the current and future configurations under Options 1 and 2.
1.4.17 For the purposes of clarity, this document will refer to two different types of Emergency Department:
An Emergency Care Centre (ECC) – a department which will provide Consultant delivered 24/7 care with full resuscitation facilities, receiving critically ill and injured patients; and
An Emergency Care Unit (ECU) - a department that will receive, without the need for an appointment, walk in patients and selected ambulance attendances by protocol. Opening times to be agreed and care will be delivered by a mix of doctor and nurse practitioners, likely to be consultant presence during the day with 24 hour consultant-led oversight and supervision, but not necessarily on site. There will be an ability to resuscitate sick patients prior to transfer when required.
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxi
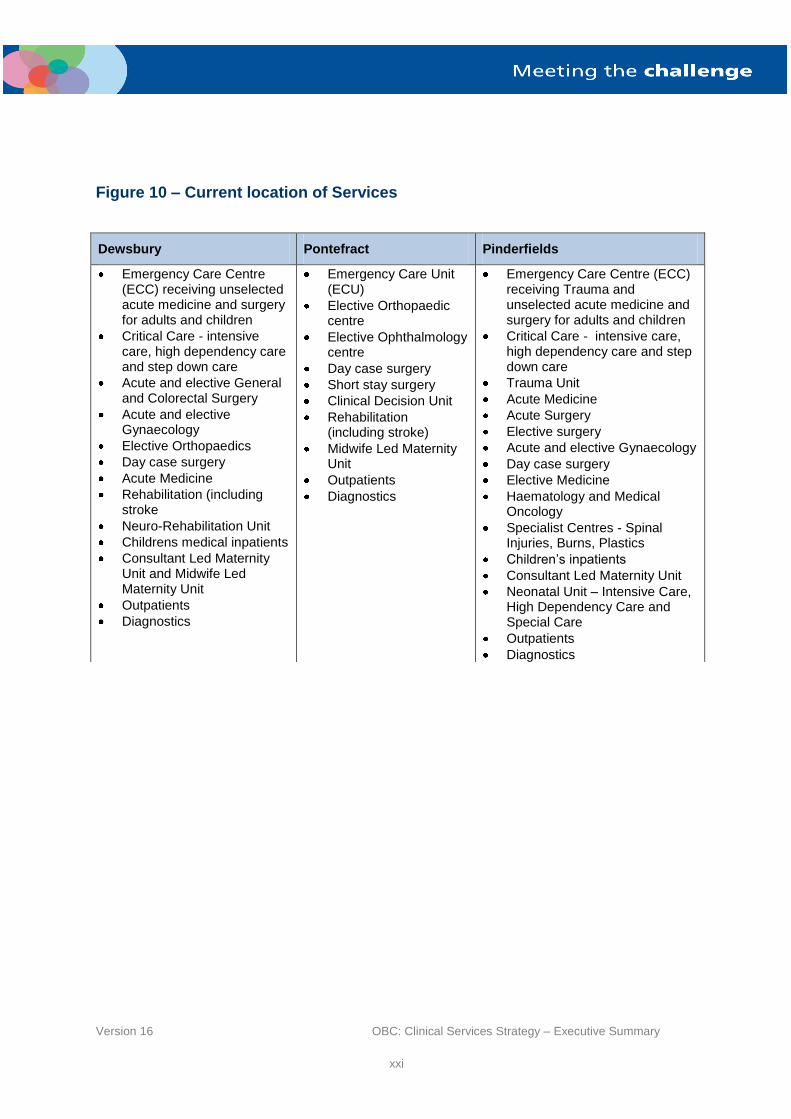
Figure 10 – Current location of Services
Dewsbury Pontefract Pinderfields
Emergency Care Centre (ECC) receiving unselected acute medicine and surgery for adults and children
Critical Care - intensive care, high dependency care and step down care
Acute and elective General and Colorectal Surgery
Acute and elective Gynaecology
Elective Orthopaedics
Day case surgery
Acute Medicine
Rehabilitation (including stroke
Neuro-Rehabilitation Unit
Childrens medical inpatients
Consultant Led Maternity Unit and Midwife Led Maternity Unit
Outpatients
Diagnostics
Emergency Care Unit (ECU)
Elective Orthopaedic centre
Elective Ophthalmology centre
Day case surgery
Short stay surgery
Clinical Decision Unit
Rehabilitation (including stroke)
Midwife Led Maternity Unit
Outpatients
Diagnostics
Emergency Care Centre (ECC) receiving Trauma and unselected acute medicine and surgery for adults and children
Critical Care - intensive care, high dependency care and step down care
Trauma Unit
Acute Medicine
Acute Surgery
Elective surgery
Acute and elective Gynaecology
Day case surgery
Elective Medicine
Haematology and Medical Oncology
Specialist Centres - Spinal Injuries, Burns, Plastics
Children’s inpatients
Consultant Led Maternity Unit
Neonatal Unit – Intensive Care, High Dependency Care and Special Care
Outpatients
Diagnostics

Version 16 OBC: Clinical Services Strategy – Executive Summary
xxii
Figure 11 – Proposed service locations – Option 1
Dewsbury Pontefract Pinderfields
Emergency Care Centre (ECC) receiving unselected acute medicine and surgery for adults and children
Critical Care - intensive care, high dependency care and step down care
Elective Surgery (apart from General and Colorectal Surgery)
Elective Gynaecology
Day case surgery
Acute Medicine
Rehabilitation (including stroke
Neuro-Rehabilitation Unit
Midwife Led Maternity Unit
Outpatients
Diagnostics
Emergency Care Unit (ECU)
Elective Orthopaedic centre
Elective Ophthalmology centre
Day case surgery
Short stay surgery
Clinical Decision Unit
Medical Investigation Unit
Rehabilitation (including stroke)
Midwife Led Maternity Unit
Outpatients
Diagnostics
Emergency Care Centre (ECC) receiving Trauma and unselected acute medicine and surgery for adults and children
Critical Care - intensive care, high dependency care and step down care
Trauma Unit
Acute Medicine
Acute Surgery
Elective surgery
Acute and elective Gynaecology
Day case surgery
Elective Medicine
Haematology and Medical Oncology
Specialist Centres - Spinal Injuries, Burns, Plastics
Children’s inpatients
Consultant Led Maternity Unit
Neonatal Unit – Intensive Care, High Dependency Care and Special Care
Outpatients
Diagnostics

Version 16 OBC: Clinical Services Strategy – Executive Summary
xxiii
Figure 12 – Proposed service locations – Option 2
Dewsbury Pontefract Pinderfields
Emergency Care Unit (ECU)
Elective surgery (not requiring Critical Care)
Elective Gynaecology
Elective Orthopaedic centre
Elective Ophthalmology centre
Day case surgery
Clinical Decision Unit
Medical Investigation Unit
Step up/down
Rehabilitation (including stroke)
Neuro-Rehabilitation Unit
Midwife Led Maternity Unit
Outpatients
Diagnostics
Allows for the development of a primary/secondary care ‘Health Campus’
Emergency Care Unit
Elective Orthopaedic centre
Elective Ophthalmology centre
Day case surgery
Short stay surgery
Clinical Decision Unit
Rehabilitation (including stroke)
Midwife Led Maternity Unit
Outpatients
Diagnostics
Emergency Care Centre (ECC) receiving Trauma and unselected acute medicine and surgery for adults and children.
Critical Care - intensive care, high dependency care and step down care
Trauma Unit
cute Medicine
Acute Surgery
Acute and elective Gynaecology
Elective surgery requiring critical care support
Day case surgery
Haematology and Medical Oncology
Specialist Centres - Spinal Injuries, Burns, Plastics
Children’s inpatients
Consultant Led and Midwife Led Maternity Units
Neonatal Unit – Intensive Care, High Dependency Care and Special Care
Outpatients
Diagnostics
Allows for the development of a primary / secondary care Health Campus
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxiv
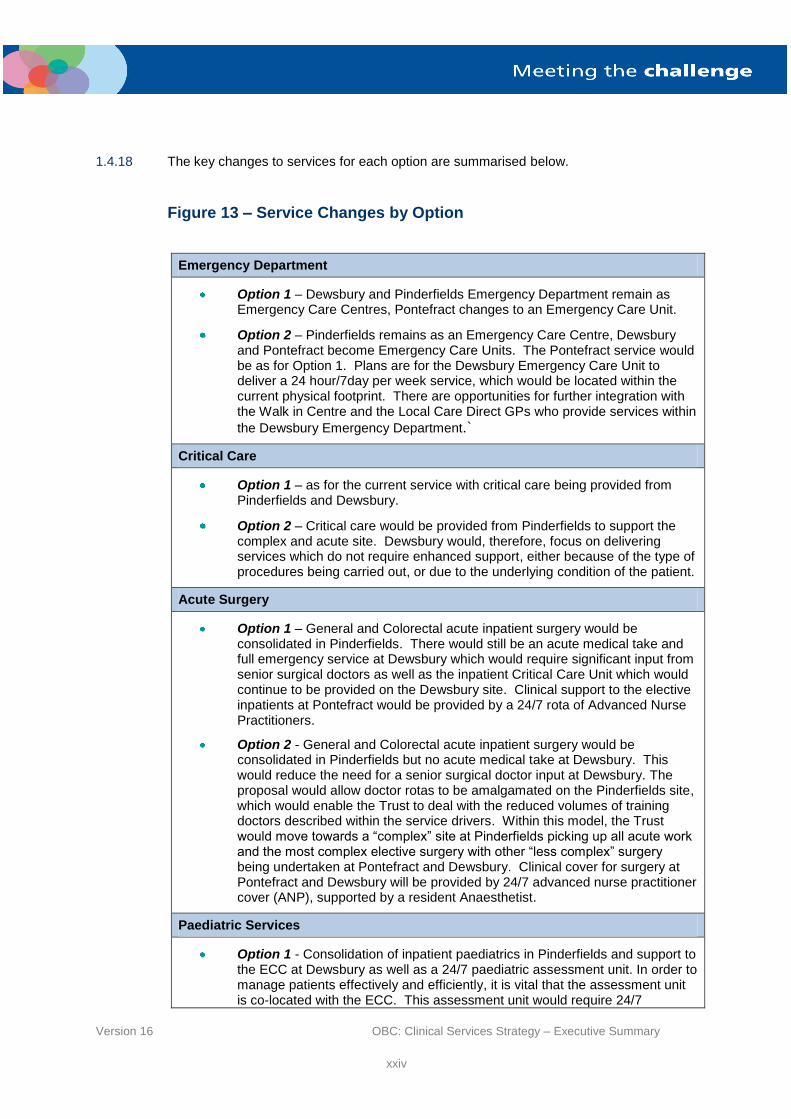
1.4.18 The key changes to services for each option are summarised below.
Figure 13 – Service Changes by Option
Emergency Department
Option 1 – Dewsbury and Pinderfields Emergency Department remain as Emergency Care Centres, Pontefract changes to an Emergency Care Unit.
Option 2 – Pinderfields remains as an Emergency Care Centre, Dewsbury and Pontefract become Emergency Care Units. The Pontefract service would be as for Option 1. Plans are for the Dewsbury Emergency Care Unit to deliver a 24 hour/7day per week service, which would be located within the current physical footprint. There are opportunities for further integration with the Walk in Centre and the Local Care Direct GPs who provide services within
the Dewsbury Emergency Department.`
Critical Care
Option 1 – as for the current service with critical care being provided from Pinderfields and Dewsbury.
Option 2 – Critical care would be provided from Pinderfields to support the complex and acute site. Dewsbury would, therefore, focus on delivering services which do not require enhanced support, either because of the type of procedures being carried out, or due to the underlying condition of the patient.
Acute Surgery
Option 1 – General and Colorectal acute inpatient surgery would be consolidated in Pinderfields. There would still be an acute medical take and full emergency service at Dewsbury which would require significant input from senior surgical doctors as well as the inpatient Critical Care Unit which would continue to be provided on the Dewsbury site. Clinical support to the elective inpatients at Pontefract would be provided by a 24/7 rota of Advanced Nurse Practitioners.
Option 2 - General and Colorectal acute inpatient surgery would be consolidated in Pinderfields but no acute medical take at Dewsbury. This would reduce the need for a senior surgical doctor input at Dewsbury. The proposal would allow doctor rotas to be amalgamated on the Pinderfields site, which would enable the Trust to deal with the reduced volumes of training doctors described within the service drivers. Within this model, the Trust would move towards a “complex” site at Pinderfields picking up all acute work and the most complex elective surgery with other “less complex” surgery being undertaken at Pontefract and Dewsbury. Clinical cover for surgery at Pontefract and Dewsbury will be provided by 24/7 advanced nurse practitioner cover (ANP), supported by a resident Anaesthetist.
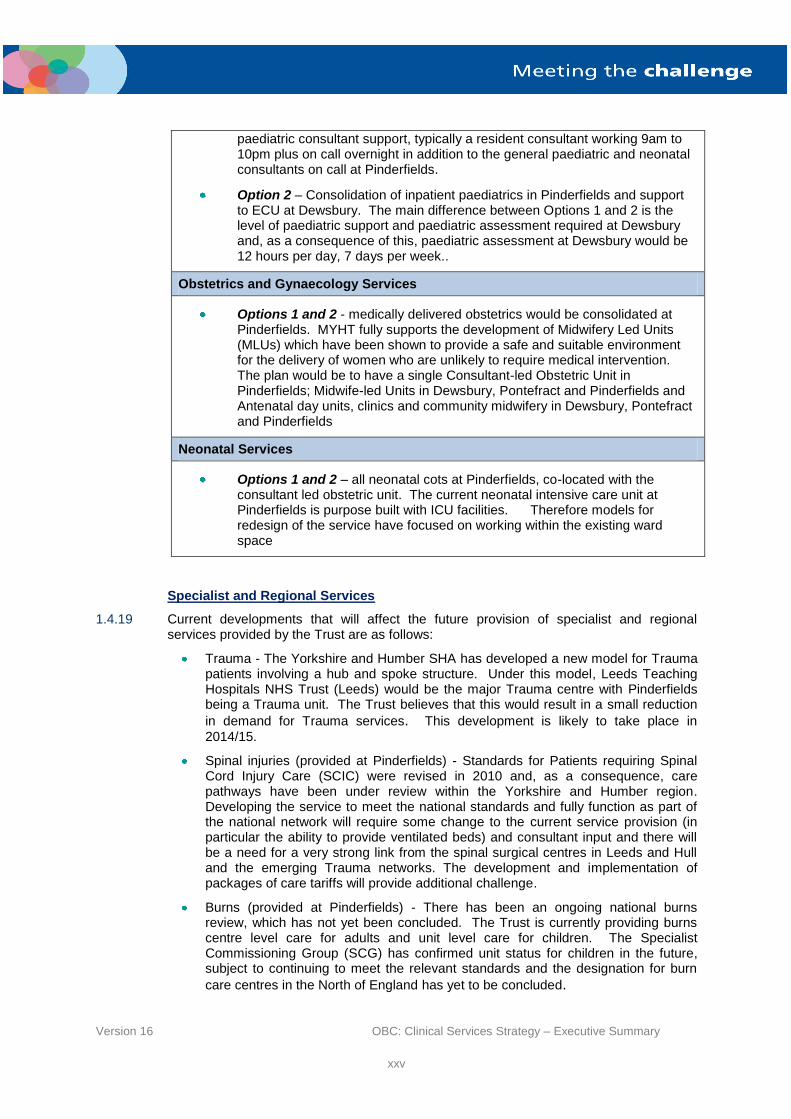
Paediatric Services
Option 1 - Consolidation of inpatient paediatrics in Pinderfields and support to the ECC at Dewsbury as well as a 24/7 paediatric assessment unit. In order to manage patients effectively and efficiently, it is vital that the assessment unit is co-located with the ECC. This assessment unit would require 24/7
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxv
paediatric consultant support, typically a resident consultant working 9am to 10pm plus on call overnight in addition to the general paediatric and neonatal consultants on call at Pinderfields.
Option 2 – Consolidation of inpatient paediatrics in Pinderfields and support to ECU at Dewsbury. The main difference between Options 1 and 2 is the level of paediatric support and paediatric assessment required at Dewsbury and, as a consequence of this, paediatric assessment at Dewsbury would be 12 hours per day, 7 days per week..
Obstetrics and Gynaecology Services
Options 1 and 2 - medically delivered obstetrics would be consolidated at Pinderfields. MYHT fully supports the development of Midwifery Led Units (MLUs) which have been shown to provide a safe and suitable environment for the delivery of women who are unlikely to require medical intervention. The plan would be to have a single Consultant-led Obstetric Unit in Pinderfields; Midwife-led Units in Dewsbury, Pontefract and Pinderfields and Antenatal day units, clinics and community midwifery in Dewsbury, Pontefract and Pinderfields
Neonatal Services
Options 1 and 2 – all neonatal cots at Pinderfields, co-located with the consultant led obstetric unit. The current neonatal intensive care unit at Pinderfields is purpose built with ICU facilities. Therefore models for redesign of the service have focused on working within the existing ward space
Specialist and Regional Services
1.4.19 Current developments that will affect the future provision of specialist and regional services provided by the Trust are as follows:
Trauma - The Yorkshire and Humber SHA has developed a new model for Trauma patients involving a hub and spoke structure. Under this model, Leeds Teaching Hospitals NHS Trust (Leeds) would be the major Trauma centre with Pinderfields being a Trauma unit. The Trust believes that this would result in a small reduction
in demand for Trauma services. This development is likely to take place in
2014/15.
Spinal injuries (provided at Pinderfields) - Standards for Patients requiring Spinal Cord Injury Care (SCIC) were revised in 2010 and, as a consequence, care pathways have been under review within the Yorkshire and Humber region. Developing the service to meet the national standards and fully function as part of the national network will require some change to the current service provision (in particular the ability to provide ventilated beds) and consultant input and there will be a need for a very strong link from the spinal surgical centres in Leeds and Hull and the emerging Trauma networks. The development and implementation of packages of care tariffs will provide additional challenge.
Burns (provided at Pinderfields) - There has been an ongoing national burns review, which has not yet been concluded. The Trust is currently providing burns centre level care for adults and unit level care for children. The Specialist Commissioning Group (SCG) has confirmed unit status for children in the future, subject to continuing to meet the relevant standards and the designation for burn
care centres in the North of England has yet to be concluded.
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxvi
Vascular Services - The Yorkshire and Humber vascular review determined that there would be a Leeds/MYHT provider partnership with the major arterial work being undertaken in Leeds. A formal agreement is in development with regard to the case mix spilt between the two sites. The key issue is the continued provision of vascular and interventional radiology support to the other specialties that require this at the Trust.
Neonatal Services - The SCG has stated that the broad direction of travel around neonatal services is generally for greater centralisation so the rationing of services on to the Pinderfields site would be regarded as a more robust model of delivery.
Bone and Marrow Transplantation - There is a need to work closely with Leeds to ensure that national standards continue to be met.
Capacity Planning – Implication for Beds
1.4.20 In order to understand the effects of the reconfiguration options on the bed numbers required at each hospital site, the Trust carried out a modelling exercise to determine the bed numbers required at each site. The Trust’s activity data has been analysed through a bed capacity and demand model which allows key assumptions to be changed such as length of stay, bed occupancy etc. The model also includes a software application using the Geographical Information Systems (GIS), which assesses the potential changes to patient and ambulance choice of hospital if services were re-configured and centralised.
1.4.21 Based on this, the Trust has included a “drivetime” analysis in the model to consider the potential shift of services that could result from the reconfiguration of services. The drivetime methodology enables the Trust to derive a proportion of activity that might more realistically flow to alternative providers as a result of the change. The Trust is, therefore, able to quantify the potential loss of activity overall.
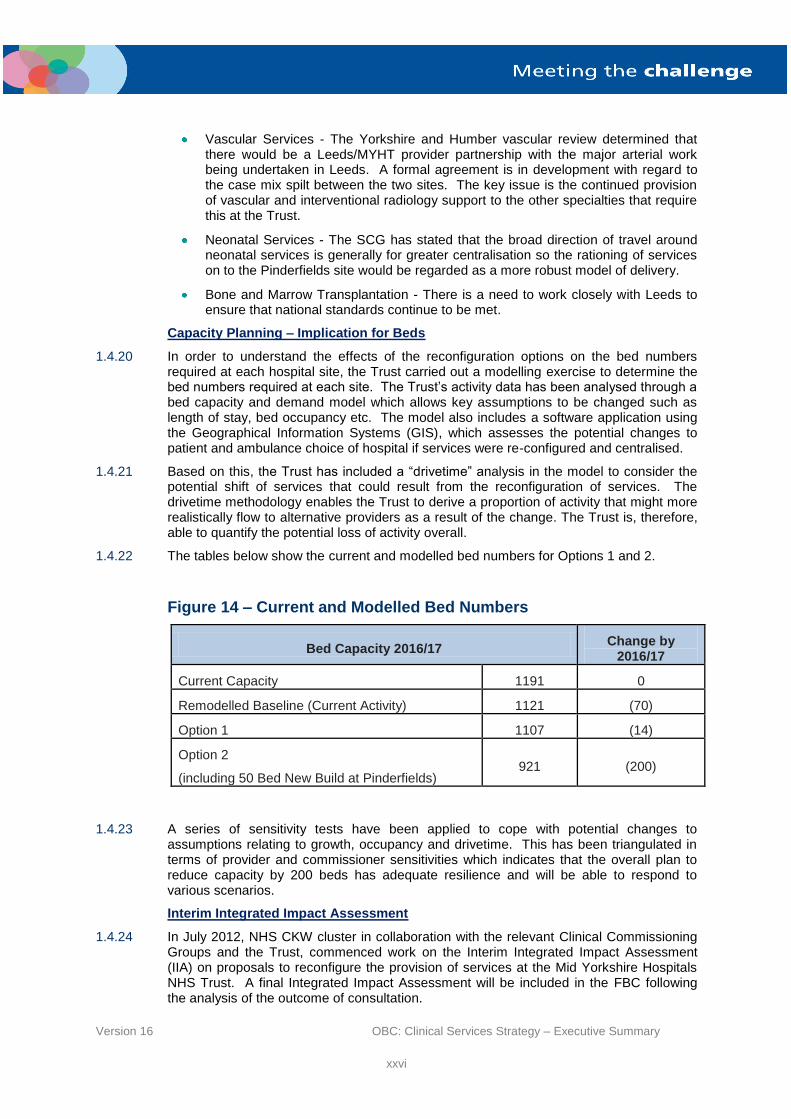
1.4.22 The tables below show the current and modelled bed numbers for Options 1 and 2.
Figure 14 – Current and Modelled Bed Numbers
Bed Capacity 2016/17 Change by
2016/17
Current Capacity 1191 0
Remodelled Baseline (Current Activity) 1121 (70)
Option 1 1107 (14)
Option 2
(including 50 Bed New Build at Pinderfields) 921 (200)
1.4.23 A series of sensitivity tests have been applied to cope with potential changes to assumptions relating to growth, occupancy and drivetime. This has been triangulated in terms of provider and commissioner sensitivities which indicates that the overall plan to reduce capacity by 200 beds has adequate resilience and will be able to respond to various scenarios.
Interim Integrated Impact Assessment
1.4.24 In July 2012, NHS CKW cluster in collaboration with the relevant Clinical Commissioning Groups and the Trust, commenced work on the Interim Integrated Impact Assessment (IIA) on proposals to reconfigure the provision of services at the Mid Yorkshire Hospitals NHS Trust. A final Integrated Impact Assessment will be included in the FBC following the analysis of the outcome of consultation.
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxvii
1.4.25 The objective of the IIA is to identify the positive and negative effects of the proposed reconfiguration of health services at the Mid Yorkshire Hospitals NHS Trust in the following areas:
Health outcomes
Access to services - (Travel Analysis)
Equality Groups - (those protected characteristics outlined in the Equality Act 2010).
1.4.26 The final IIA will also include the impact of the proposed changes and the carbon footprint.
1.4.27 Key conclusions drawn from the IIA are that:
The service changes for Option 1 would allow clinical sustainability for key pressured services. This option would affect fewer equality groups than Option 2.
However, Option 2 would allow radical service changes and deliver improved clinical performance and financial sustainability. The centralisation of acute services at Pinderfields and elective services at Dewsbury and Pontefract ensures having the right staff in the right place at the right time. Evidence suggests that centralisation of services would improve staffing ratios and the availability of round the clock treatment, thereby improving clinical outcomes for patients. The proposal will lead to higher levels of safety and quality of care for patients.
1.4.28 A copy of the interim report is provided in Appendix H.
1.5 Evaluation of the Strategic Options
1.5.1 In order to assess the performance of each option, the Trust carried out an Option Appraisal. Each option was subjected to three analyses:
A non – financial appraisal where the qualitative features of each option are assessed against a set of criteria derived from the strategic objectives;
An economic analysis where the lifetime costs of each option are compared to see which option has the lowest economic cost;
A risk assessment where the performance of each option is assessed against an agreed set of risks.
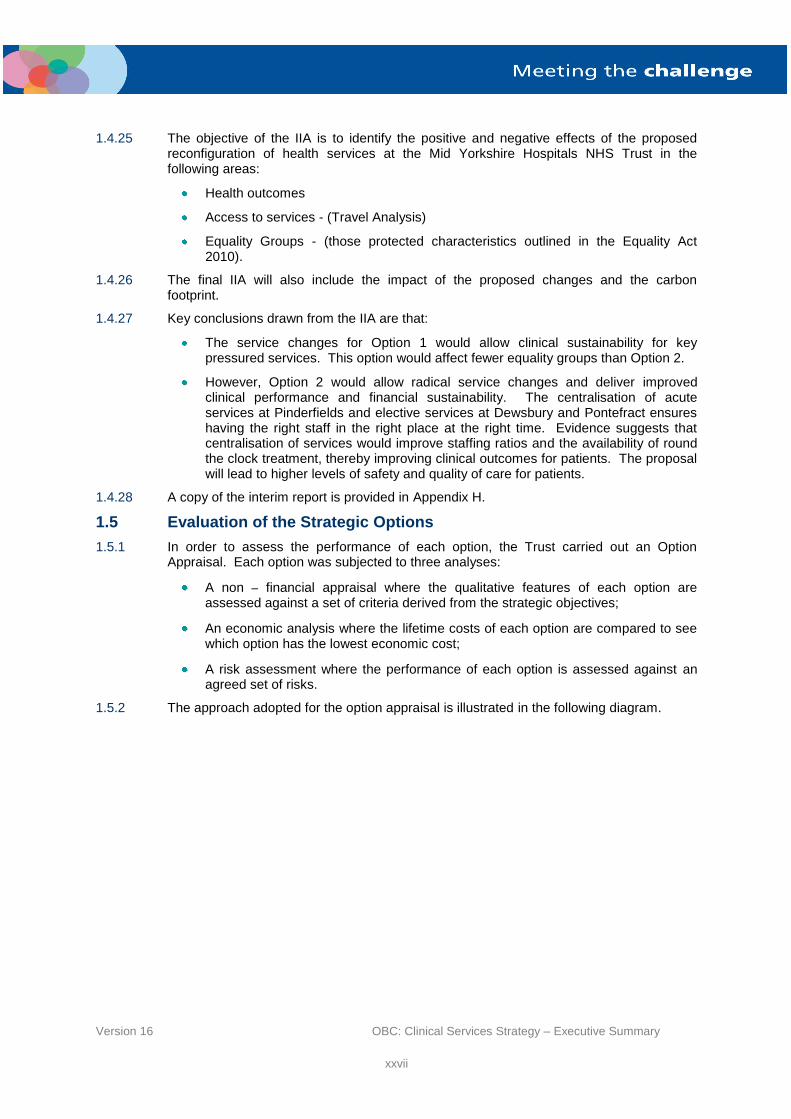
1.5.2 The approach adopted for the option appraisal is illustrated in the following diagram.
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxviii
Figure 15 – The Option Appraisal Process
1.5.3 The Trust wished to ensure that its stakeholders were involved in the option appraisal process, particularly in the non-financial appraisal. It introduced the process, and the rationale behind the need for reconfiguration, to stakeholders at a stakeholder engagement workshop held at the National Coal Mining Museum on 22
nd June 2012. The
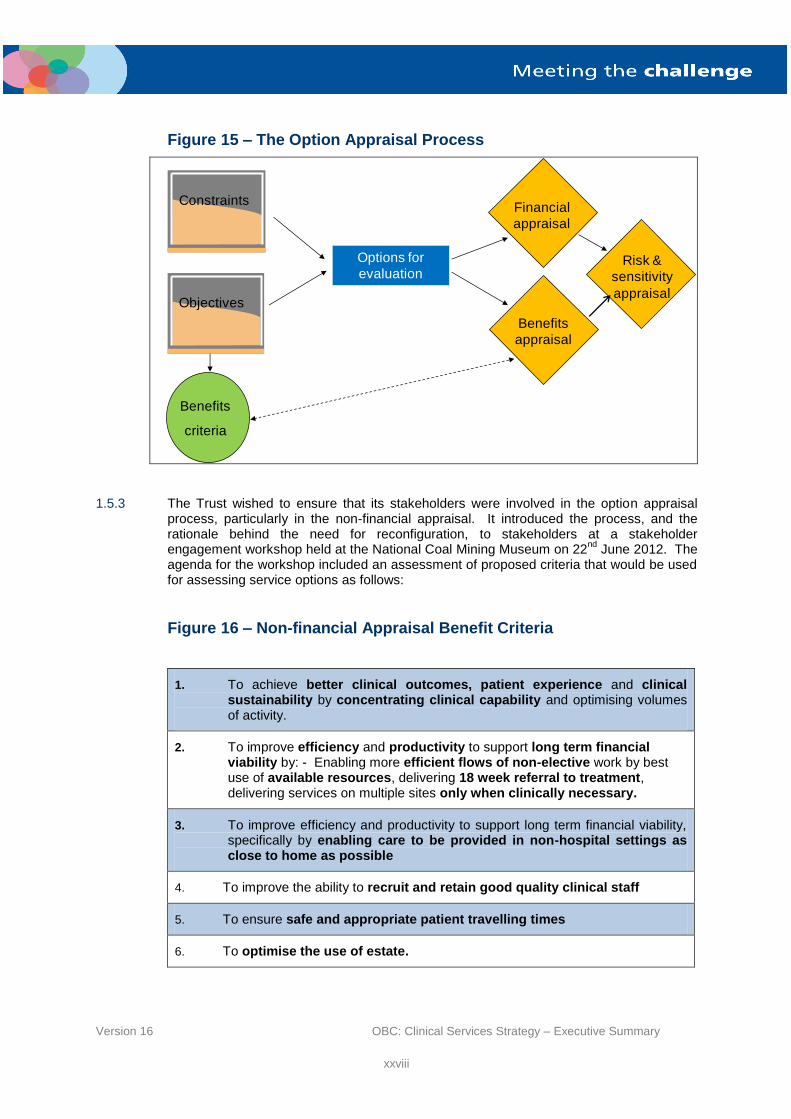
agenda for the workshop included an assessment of proposed criteria that would be used for assessing service options as follows:
Figure 16 – Non-financial Appraisal Benefit Criteria
1. To achieve better clinical outcomes, patient experience and clinical sustainability by concentrating clinical capability and optimising volumes of activity.
2. To improve efficiency and productivity to support long term financial viability by: - Enabling more efficient flows of non-elective work by best use of available resources, delivering 18 week referral to treatment, delivering services on multiple sites only when clinically necessary.
3. To improve efficiency and productivity to support long term financial viability, specifically by enabling care to be provided in non-hospital settings as close to home as possible
4. To improve the ability to recruit and retain good quality clinical staff
5. To ensure safe and appropriate patient travelling times
6. To optimise the use of estate.
Constraints
Objectives
Options for
evaluation
Benefits
criteria
Financial
appraisal
Risk &
sensitivity
appraisal
Benefits
appraisal
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxix
1.5.4 The workshop involved the participation of stakeholders involved in the service development including representatives from:
Service commissioners (including the SCG);
Service users;
Clinicians (from primary and secondary care);
Social services;
Local authorities;
Yorkshire Ambulance Service (YAS);
NHS managers from the Mid Yorkshire health community.
1.5.5 The workshop:
Set out the issues which led to the current situation and reasons why there is a need for the transformation of services;
Described the option appraisal process and the proposed criteria to be used to evaluate options;
Ranked and weighted the evaluation criteria in order of importance;
Agreed any sensitivity tests where alternative rankings and / or weights were considered important; and
Held group discussions around specified service areas to assess the requirements and potential issues around service configurations.
1.5.6 A further workshop was held on 10th July 2012 to score the two options against the
agreed ranked and weighted criteria from the previous workshop.
1.5.7 Following these workshops, further meetings took place with NHS North Kirklees CCG and patient reference groups, including the LINks, in Wakefield and Kirklees to obtain their views of the outcome of the workshops and to receive their comments. These views resulted in further sensitivity tests being carried out on the ranking of the criteria and the scoring of the options. None of the sensitivity tests resulted in a change to the ranking of the options in the non-financial appraisal.
1.5.8 The overall results of the workshop weighted scores, together with the outcome of the economic analysis and risk scoring, are summarised in the following table.
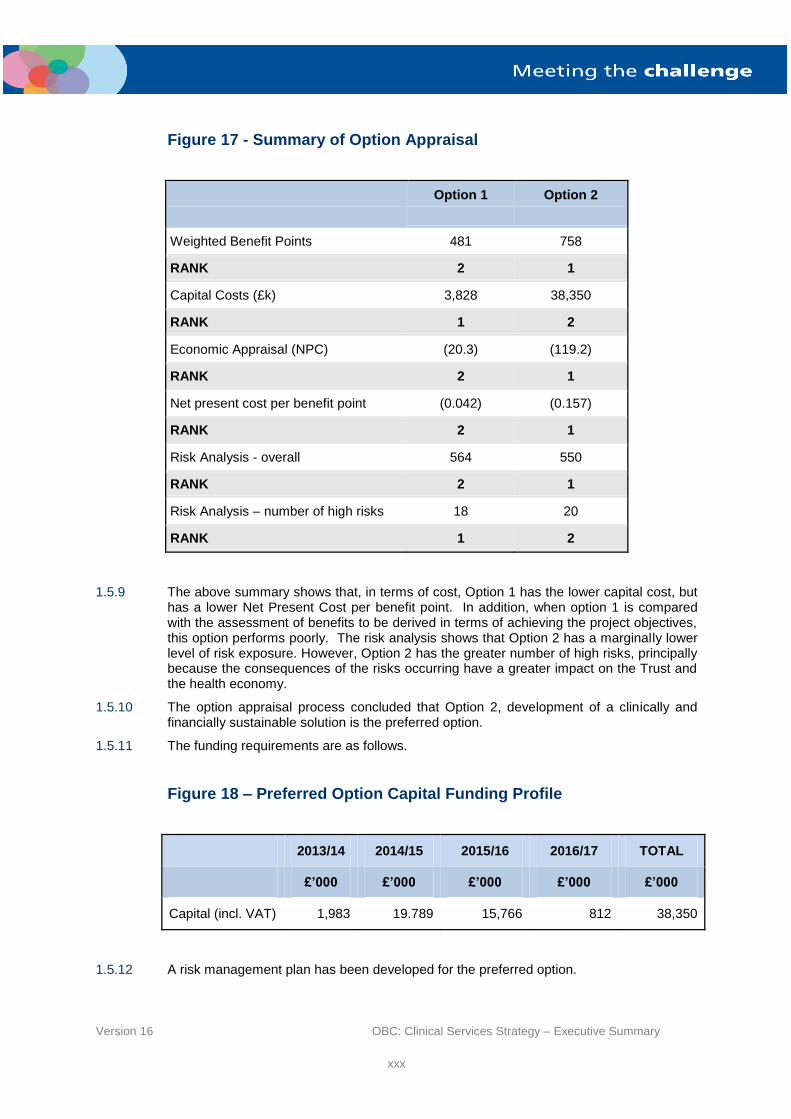
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxx
Figure 17 - Summary of Option Appraisal
Option 1
Option 2
Weighted Benefit Points 481 758
RANK 2 1
Capital Costs (£k) 3,828 38,350
RANK 1 2
Economic Appraisal (NPC) (20.3) (119.2)
RANK 2 1
Net present cost per benefit point (0.042) (0.157)
RANK 2 1
Risk Analysis - overall 564 550
RANK 2 1
Risk Analysis – number of high risks 18 20
RANK 1 2
1.5.9 The above summary shows that, in terms of cost, Option 1 has the lower capital cost, but has a lower Net Present Cost per benefit point. In addition, when option 1 is compared with the assessment of benefits to be derived in terms of achieving the project objectives, this option performs poorly. The risk analysis shows that Option 2 has a marginally lower level of risk exposure. However, Option 2 has the greater number of high risks, principally because the consequences of the risks occurring have a greater impact on the Trust and the health economy.
1.5.10 The option appraisal process concluded that Option 2, development of a clinically and financially sustainable solution is the preferred option.
1.5.11 The funding requirements are as follows.
Figure 18 – Preferred Option Capital Funding Profile
2013/14 2014/15 2015/16 2016/17 TOTAL
£’000 £’000 £’000 £’000 £’000
Capital (incl. VAT) 1,983 19.789 15,766 812 38,350
1.5.12 A risk management plan has been developed for the preferred option.

Version 16 OBC: Clinical Services Strategy – Executive Summary
xxxi
1.6 Models of Care for the Preferred Option
1.6.1 The Trust has embarked on a detailed programme to re-design patient pathways in key areas of service provision. The development of the pathways uses the 5 step approach used by the NHS Institute and which is described in the Care Pathway Toolkit taken from the Clinical Governance Website (November 2011).
1.6.2 The four key areas of change are:
The provision of urgent assessment;
The separation of acute and elective activity;
The provision of inpatient maternity services; and
The provision of inpatient paediatric services.
1.6.3 Eight care pathways have been developed jointly by primary and secondary care clinicians to begin to describe how the patient journey will be different in the future under the preferred option. The pathways cover:
Acute surgery;
Heart failure;
Frail elderly (falls);
Long term conditions (COPD); and
End of life care.
Elective orthopaedics;
Maternity;
Paediatrics.
1.6.4 The eight pathways were chosen to serve a number of purposes:
To provide a joint understanding of the new care pathways to meet concerns that may arise from the National Clinical Advisory Team, members of the public etc – for example the impact of the proposed changes for children and women in labour;
To describe the benefit of the preferred option on the reduction to length of stay in hospital – e.g. elective Orthopaedics;
To describe how hospital admission might be avoided altogether or early discharge
facilitated – e.g. frail elderly and long term conditions.
1.6.5 Models of care for the three hospitals and additional care pathways across the health and social care economy will be developed in more detail for the Full Business Case. There is a planned programme in place to continue to bring together primary and secondary care clinicians to robustly describe and plan for the transformational change that will deliver a sustainable health and social economy, providing safe, quality care to patients into the future;
1.7 Procurement
1.7.1 The Trust has undertaken a review of procurement options for the capital required to secure facilities to deliver the preferred option. A major consideration is the modifications that would be required within the current PFI – funded buildings as well as those on Trust-owned facilities.
1.7.2 The Trust has concluded that a mix of procurement strategies based on using the current PFI partner for internal developments within the PFI buildings and Procure 21+ for other developments will offer the best flexibility, value for money and outcomes.
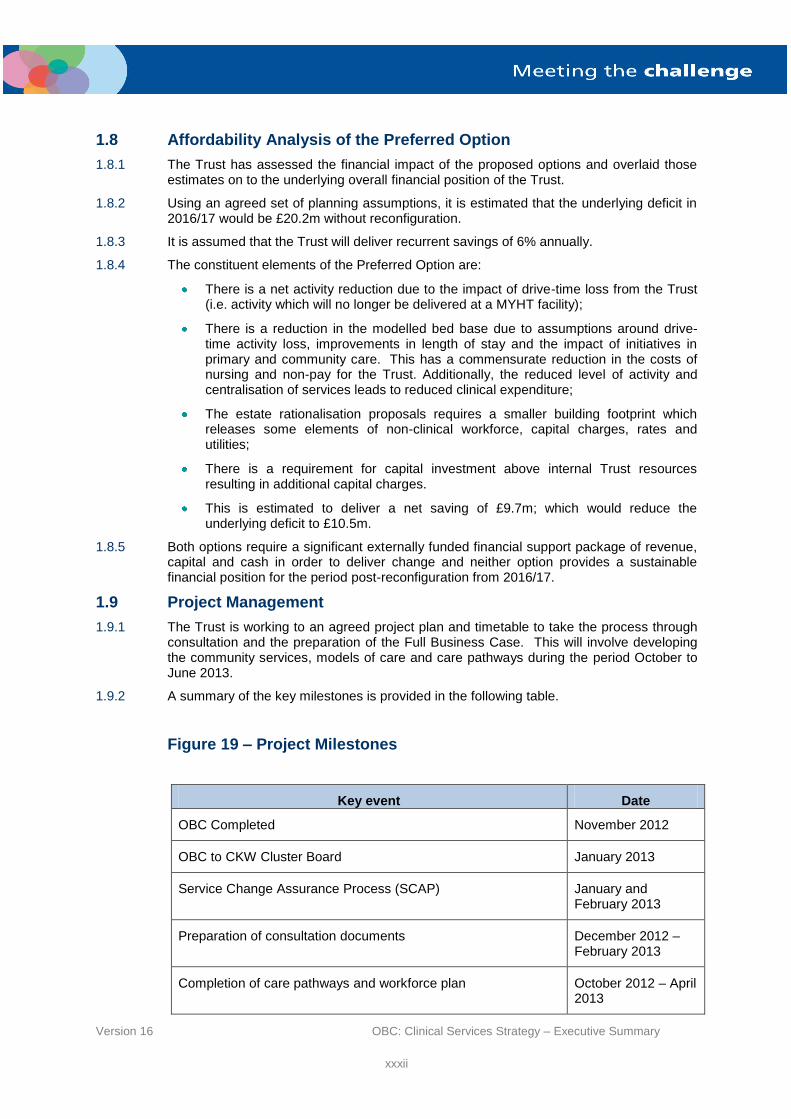
Version 16 OBC: Clinical Services Strategy – Executive Summary
xxxii
1.8 Affordability Analysis of the Preferred Option
1.8.1 The Trust has assessed the financial impact of the proposed options and overlaid those estimates on to the underlying overall financial position of the Trust.
1.8.2 Using an agreed set of planning assumptions, it is estimated that the underlying deficit in 2016/17 would be £20.2m without reconfiguration.
1.8.3 It is assumed that the Trust will deliver recurrent savings of 6% annually.
1.8.4 The constituent elements of the Preferred Option are:
There is a net activity reduction due to the impact of drive-time loss from the Trust (i.e. activity which will no longer be delivered at a MYHT facility);
There is a reduction in the modelled bed base due to assumptions around drive-time activity loss, improvements in length of stay and the impact of initiatives in primary and community care. This has a commensurate reduction in the costs of nursing and non-pay for the Trust. Additionally, the reduced level of activity and centralisation of services leads to reduced clinical expenditure;
The estate rationalisation proposals requires a smaller building footprint which releases some elements of non-clinical workforce, capital charges, rates and utilities;
There is a requirement for capital investment above internal Trust resources resulting in additional capital charges.
This is estimated to deliver a net saving of £9.7m; which would reduce the underlying deficit to £10.5m.
1.8.5 Both options require a significant externally funded financial support package of revenue, capital and cash in order to deliver change and neither option provides a sustainable financial position for the period post-reconfiguration from 2016/17.
1.9 Project Management
1.9.1 The Trust is working to an agreed project plan and timetable to take the process through consultation and the preparation of the Full Business Case. This will involve developing the community services, models of care and care pathways during the period October to June 2013.
1.9.2 A summary of the key milestones is provided in the following table.
Figure 19 – Project Milestones
Key event Date
OBC Completed November 2012
OBC to CKW Cluster Board January 2013
Service Change Assurance Process (SCAP) January and February 2013
Preparation of consultation documents December 2012 – February 2013
Completion of care pathways and workforce plan October 2012 – April 2013

Version 16 OBC: Clinical Services Strategy – Executive Summary
xxxiii
Key event Date
Public Consultation on proposed Clinical Services Strategy March – May 2013
Consultation analysis complete June 2013
Update of Strategic and Economic Cases complete June 2013
Completion of Financial Case (affordability analysis) June 2013
Completion of FBC July 2013
1.9.3 The health economy has developed a governance structure, overseen by the Programme Office, to be taken forward that will ensure sufficient input from key stakeholders, including clinicians and GP commissioners. This structure is shown in the following figure.

Version 16 OBC: Clinical Services Strategy – Executive Summary
xxxiv
Figure 20 – Clinical Services Strategy Governance Structure
Calderdale Kirklees and Wakefield (CKW) Cluster Board
(Monthly Update)
Project Team
Caroline Griffiths – Director of Corporate Planning & Projects
Dr Simon Enright – Clinical Lead CSS / Consultant Anaesthetist
Michele Ezro – Associate Director of Strategy
Joanne Dale – Associate Director of Operations
Andrew Wiles – Project Manager
Louise Wood – Project Administrator
Louise Wood – Project Personal Assistant
MYHT Trust Board
(Monthly Update)
NHS Wakefield CCG
(Monthly Update)
NHS North Kirklees CCG
(Monthly Update)
MYHT Executive Directors
(Weekly Update)
MYHT Clinical Executive
Group
(Weekly Update)
MY Health and Social Care Programme Board
(Monthly Update)
Project Executive
(Monthly Update)
CSS Group
(Fortnightly Update)
Urgent Care
Programme
Board
Out of Hospital Care Programme
Board
Children and Young People Programme
Board
Clinical Reference
Group
(Monthly Update)

Version 16 OBC: Clinical Services Strategy – Executive Summary
xxxv
1.10 Stakeholder Engagement and Consultation
1.10.1 A Stakeholder Engagement and Consultation Plan has been prepared and this is provided in Appendix S. The plan has been prepared jointly by MYHT and the commissioners.
1.10.2 Development of the clinical services strategy has been managed as part of a whole system transformational programme led by a Programme Board which includes representatives of the SHA/Trust Development Authority, commissioners, social care, community social enterprise and mental health providers. Partner providers are also involved in developing options and service redesign through the project management arrangements for specific services.
1.10.3 There has been a comprehensive communications and engagement programme jointly led by the Trust and commissioners, including a joint OSC panel which has been in place since autumn 2011, regular briefing of local authority members, Health and Well being Boards, the LINKs and a series of smaller public engagement events.
1.10.4 The future organisational form for Mid Yorkshire Hospitals has been under review since it was agreed that, due to the scale of the financial recovery programme, it would not be possible to seek authorisation as a Foundation Trust by April 2014. However, the Trust Development Authority has indicated that the Trust should continue to progress plans for clinical service reconfiguration ahead of a decision on the future governance arrangements for the Trust.
1.11 Support for the Clinical Services Strategy
1.11.1 The CKW Cluster, NHS Wakefield CCG and North Kirklees CCG have been involved in developing the options through the Mid Yorkshire Health and Social Care Partnership Programme Board and are leading on the Service Change Assurance Process.
1.11.2 Wakefield Metropolitan District Council have indicated their support to the direction of travel for the Clinical Services Strategy.
1.11.3 Yorkshire Ambulance Service has been involved in the discussions prior to the development of the two options and have confirmed their understanding of the proposed service changes. The plan is to consider the implications of the preferred option in more detail for the FBC.
1.12 Conclusion
1.12.1 MYHT believes that the Clinical Services Strategy proposed in this Outline Business Case, together with the preferred option for reconfiguring hospital services, will ensure a clinically sustainable service, and deliver financial improvements going forward. It will also support the implementation of the initiatives put forward to provide more effective care outside of hospital and ensure that patient care is provided in the most appropriate setting.
1.12.2 Support for this OBC will allow MYHT and its commissioners to progress the CSS further through consultation and development of a Full Business Case prior to implementation of the proposals contained in this document.


















