Ckd
28
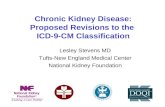
AHA Scientific Statement 1 C hronic kidney disease (CKD) is frequently encoun- tered among patients presenting with acute coro- nary syndrome (ACS). Recent data from the National Cardiovascular Data Registry–Acute Coronary Treatment and Intervention Outcomes Network (NCDR-ACTION) reported CKD (defined as estimated creatinine clearance [CrCl] <60 mL·min −1 ·1.73 m −2 ) prevalence rates of 30.5% among patients presenting with ST-segment–elevation myocardial infarction (STEMI) and 42.9% among patients present- ing with non–ST-segment–elevation myocardial infarction (NSTEMI). 1 The presence of CKD among patients presenting with ACS has been associated with worse outcomes, including higher rates of mortality and bleeding. 2–4 Despite the increased risk for adverse outcomes, CKD patients presenting with ACS are less likely to receive evidence-based therapies, including medications. 1 In addition, patients with CKD have been under- represented in randomized controlled trials of ACS pharmaco- therapy. 5,6 Thus, the net effect is a relative lack of evidence and potential for uncertainty in selecting medications in this high- risk population. The purpose of this scientific statement is to provide a comprehensive review of the published literature and provide recommendations on the use of evidence-based pharmacotherapies in CKD patients presenting with ACS. Background and CKD Staging It has been appreciated now for more than a decade that CKD is a powerful independent predictor of cardiovascular mor- bidity, cardiovascular mortality, and all-cause mortality. The systematic classification of CKD in large part is based on the efforts of Andrew Levey and colleagues, who published the K/DOQI (Kidney Disease Outcomes Quality Initiative) clini- cal practice guidelines for CKD. 7 The original schema some- what arbitrarily defined stages 1 to 5 CKD on the basis of estimated glomerular filtration rate (eGFR) in the following manner: Stage 1, eGFR ≥90 mL·min −1 ·1.73 m −2 (with evi- dence of kidney damage present, such as albuminuria); stage 2, eGFR <90 but ≥60 (with evidence of kidney damage such as albuminuria); stage 3, eGFR <60 but ≥30; stage 4, eGFR <30 but ≥15; and stage 5, eGFR <15 or undergoing dialysis. 7 An additional modification was made to create a stage 3a (eGFR 45–59 mL·min −1 ·1.73 m −2 ) and stage 3b (eGFR 30–44 mL·min −1 ·1.73 m −2 ). Most recently, based on the stepwise association of albuminuria with increased rates of CKD progression, cardiovascular mortality, and total mortality, the Kidney Disease: Improving Global Outcomes (KDIGO) group has recommended altering the classification scheme to include urinary albumin excretion (Figure 1). 8 (Circulation. 2015;131:000-000. DOI: 10.1161/CIR.0000000000000183.) © 2015 American Heart Association, Inc. Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIR.0000000000000183 The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest. This statement was approved by the American Heart Association Science Advisory and Coordinating Committee on September 15, 2014. A copy of the document is available at http://my.americanheart.org/statements by selecting either the “By Topic” link or the “By Publication Date” link. To purchase additional reprints, call 843-216-2533 or e-mail [email protected]. The American Heart Association requests that this document be cited as follows: Washam JB, Herzog CA, Beitelshees AL, Cohen MG, Henry TD, Kapur NK, Mega JL, Menon V, Page RL 2nd, Newby LK; on behalf of the American Heart Association Clinical Pharmacology Committee of the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, Council on Functional Genomics and Translational Biology, Council on the Kidney in Cardiovascular Disease, and Council on Quality of Care and Outcomes Research. Pharmacotherapy in chronic kidney disease patients presenting with acute coronary syndrome: a scientific statement from the American Heart Association. Circulation. 2015;131:•••–•••. Expert peer review of AHA Scientific Statements is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelines development, visit http://my.americanheart.org/statements and select the “Policies and Development” link. Permissions: Multiple copies, modification, alteration, enhancement, and/or distribution of this document are not permitted without the express permission of the American Heart Association. Instructions for obtaining permission are located at http://www.heart.org/HEARTORG/General/Copyright- Permission-Guidelines_UCM_300404_Article.jsp. A link to the “Copyright Permissions Request Form” appears on the right side of the page. Pharmacotherapy in Chronic Kidney Disease Patients Presenting With Acute Coronary Syndrome A Scientific Statement From the American Heart Association Jeffrey B. Washam, PharmD, FAHA, Chair; Charles A. Herzog, MD, FAHA; Amber L. Beitelshees, PharmD, MPH, FAHA; Mauricio G. Cohen, MD; Timothy D. Henry, MD; Navin K. Kapur, MD; Jessica L. Mega, MD, MPH, FAHA; Venu Menon, MD, FAHA; Robert L. Page II, PharmD, MSPH, FAHA; L. Kristin Newby, MD, MHS, FAHA, Co-Chair; on behalf of the American Heart Association Clinical Pharmacology Committee of the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, Council on Functional Genomics and Translational Biology, Council on the Kidney in Cardiovascular Disease, and Council on Quality of Care and Outcomes Research by guest on March 22, 2015 http://circ.ahajournals.org/ Downloaded from
-
Upload
brenda-karina -
Category
Documents
-
view
219 -
download
6
description
chronic kidney
Transcript of Ckd
-
AHA Scientific Statement
1
Chronic kidney disease (CKD) is frequently encoun-tered among patients presenting with acute coro-nary syndrome (ACS). Recent data from the National Cardiovascular Data RegistryAcute Coronary Treatment and Intervention Outcomes Network (NCDR-ACTION) reported CKD (defined as estimated creatinine clearance [CrCl]
-
2 Circulation March 24, 2015
As shown in Figure 2, there is a stepwise incremental age-standardized risk for all-cause mortality, cardiovascu-lar events, and hospitalization associated with diminishing renal function.9 Compared with patients with eGFR 60 mLmin11.73 m2, the adjusted hazard for death among patients with eGFR 15 to 29 mLmin11.73 m2 is more than 3-fold higher, and nearly 6 times higher for patients with eGFR 2.5 mg/dL), and 274 777 non-CKD patients.14 Those with advanced CKD and dialysis were less likely to have chest pain on admission (40.4% and 41.1%, respectively) than those without CKD (61.6%). Similar observations were made in the SWEDEHEART registry [Swedish Web System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies]; however, up to two thirds of patients with stage 4 and 5 CKD in that registry had chest pain at presentation.15 The USRDS-NRMI study also showed that MI patients with advanced CKD and those undergoing dialysis more often had a diagnosis at presentation other than ACS (44% and 47.7%, respectively) compared with patients without CKD (25.8%). Compared with patients without CKD, patients with advanced CKD were also less likely to have ST-segment elevation (15.9% versus 32.5%, respectively) but more likely to have heart failure on presentation (52.2% versus 27.2%, respec-tively) and a higher rate of in-hospital mortality (23% versus 12.6%, respectively).10 Similar differences existed between those with advanced CKD and those undergoing dialysis. The distribution of electrocardiographic presentations varies according to severity of CKD, with fewer STEMIs and more NSTEMI and left bundle branch block among populations with increasingly worse renal function (Figure 3).11,15
An additional consideration in the diagnosis of ACS in patients with CKD is the interpretation of cardiac biomark-ers. Chronic troponin elevations in clinically stable patients with renal failure have been observed and likely represent nonischemic myocardial injury.16 In spite of these chronic troponin elevations in a population of patients with CKD, the National Association of Clinical Biochemistry labora-tory medicine practice guidelines recommend the use of troponins for the diagnosis of MI in patients with CKD pre-senting with symptoms or electrocardiographic changes sug-gestive of myocardial ischemia.17 These guidelines, along with other expert writing groups, advise the importance of a dynamic change in troponin values after presentation in the
Prognosis of CKD by GFRand Albuminuria Categories:
KDIGO 2012
Persistent albuminuria categoriesDescription and range
A1 A2 A3
GFR
cat
egor
ies
(ml/m
in/ 1.
73m2
)D
escr
iptio
n an
d ra
nge
G1 Normal or high 90
G2 Mildly decreased 60-89
G3a 45-59
G3b 30-44
G4 Severely decreased 15-29
G5 Kidney failure 300 mg/g>30 mg/mmol
30-300 mg/g3-30 mg/mmol
-
Washam et al Pharmacotherapy in CKD Patients With ACS 3
identification of acute MI (AMI) in patients with end-stage renal disease (ESRD), who more frequently have chronically elevated troponin levels.1618
This striking difference in clinical presentation and electro-cardiographic findings has implications for correct diagnosis and subsequent treatment. It has been a subject of great atten-tion that the use of evidence-based therapy is lower among patients with CKD.13,1921 Not only are those with ACS and CKD less likely to receive evidence-based therapies, the atypical clinical presentation of these patients makes it less likely that they will be correctly identified as having ACS on
presentation (and thus would not be considered for appropri-ate therapeutic interventions).
Methods of Estimating Renal Function for Drug Dosing
Whereas the Modification of Diet in Renal Disease (MDRD) equation is widely used for CKD diagnosis and staging, the Cockcroft-Gault (CG) equation has been the most commonly used equation to estimate renal function for dose adjustment of medications.22 Although these equations have limitations, both the CG and MDRD equations have been shown to cor-relate relatively well with measured glomerular filtration rate (GFR),22 but differences in medication dose recommendations have been reported depending on which equation is used.2325 An analysis of the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines (CRUSADE) registry was conducted to compare the CG and MDRD equa-tions with regard to the recommended doses of eptifibatide, tirofiban, and enoxaparin.23 Results of this analysis showed a 20% difference in CKD classification between the 2 equa-tions. The proportion of patients classified as having normal/mild CKD (eGFR 60 mL/min), moderate CKD (eGFR 3059 mL/min), and severe CKD (eGFR
-
4 Circulation March 24, 2015
A pooled analysis of 16 710 patients enrolled in the Thrombolysis in Myocardial Infarction (TIMI)-10A, TIMI-10B, TIMI-14, and Intravenous NPA for the Treatment of Infarcting Myocardium Early (InTIME-II) trials was con-ducted to assess the impact of baseline renal function (SCr and CrCl) on outcomes in patients receiving fibrinolytic therapy.30 A stepwise increase in mortality was seen with worsening renal
function, and rates of intracranial hemorrhage increased with worsening renal function (0.6%, 0.8%, 1.8%, and 3.0% for normal, mildly impaired, moderately impaired, and severely impaired CrCl, respectively; P
-
Washam et al Pharmacotherapy in CKD Patients With ACS 5
and colleagues conducted an observational analysis to assess the prognostic significance of baseline SCr in a study of 352 STEMI patients receiving fibrinolytic therapy.31 In this study, there was no association between baseline SCr and TIMI flow grade after fibrinolytic administration; however, there was a
significant increase in mortality among patients with renal dysfunction (P
-
6 Circulation March 24, 2015
severe (eGFR
-
Washam et al Pharmacotherapy in CKD Patients With ACS 7
vascular events (nonfatal MI, nonfatal stroke, or vascular death) by 41% (standard error, 16%). There was no signifi-cant increase in extracranial bleeds, although the absolute number was small (2% in antiplatelet-treated patients versus 2.3% in control subjects).37
Most of the published observational data show similar ben-efits of aspirin therapy in ACS patients across the spectrum of renal function (Table 3). However, one study did find a signifi-cant interaction between discharge aspirin therapy and renal function, with an attenuated benefit with increasing degree of
Table 3. Summary of Aspirin Studies in Patients With ACS and CKD
Study Study Design Population End Points Results
Antithrombotic Trialists Collaboration37
Meta-analysis of randomized trials
287 studies involving 135 000 patients in comparisons of antiplatelet therapy versus control and 77 000 in comparisons of different antiplatelet regimens. The number of hemodialysis patients who received antiplatelet treatment was 1333, whereas the number of hemodialysis patients who received control was 1371.
Serious vascular event (nonfatal MI, nonfatal stroke, or vascular death
Absolute reduction in the risk of serious vascular event in patients with previous MI was 36 (SE 5) per 1000 treated for 2 y and 38 (SE 5) per 1000 treated for 1 mo with AMI. Among individuals undergoing hemodialysis, antiplatelet therapy produced a 41% (SE 16%) proportional reduction in serious vascular events and no significant increase in extracranial bleeds (2% in antiplatelet vs 2.3% in control).
Keough-Ryan et al32
Observational cohort
5549 consecutive patients with ACS surviving to hospital discharge. Renal function classified into normal, >80 mLmin11.73 m2) n=1430; mild CRI, 6080 mLmin11.73 m2 (n=2018); moderate CRI, 3059 mLmin11.73 m2 (n=1795); and severe CRI, 81.5 mL/min (n=524), 63.1 to 81.5 (n=421), 46.2 to 63.1 (n=421), 46.2 not undergoing dialysis (n=310), and chronic dialysis (n=47)
In-hospital mortality Adjusted RR reduction for the combination of in-hospital aspirin and -blocker was 80%, 74.9%, 69%, 64.3%, and 77.9% across the quartiles of corrected creatinine clearance, respectively
Berger et al19 Observational, retrospective analysis of CCP and USRDS
AMI patients: 145 740 patients without ESRD and 1025 patients with ESRD receiving dialysis
Mortality (30 d) Aspirin therapy was associated with a 50% relative reduction in mortality in those receiving dialysis (P
-
8 Circulation March 24, 2015
renal dysfunction.32 Although not conducted in ACS patients per se, the United Kingdom Heart and Renal Protection Study and the Dialysis Outcomes and Practice Patterns Study both showed no increased bleeding risk with aspirin therapy among patients receiving hemodialysis, which provides further support for the safety of aspirin in patients with CKD.40,41 Collectively, the available data suggest that aspirin therapy is safe and effec-tive in ACS patients with CKD and should be used in these patients to reduce the risk of death and vascular events.
Clopidogrel, Prasugrel, and TicagrelorCurrent guidelines recommend the use of a P2Y12 receptor inhibitor across the spectrum of ACS presentations.26,42 Data evaluating P2Y12 receptor inhibitors in patients with ESRD are limited, and such information is available predominantly for individuals with moderate or no CKD. Data on the use of P2Y12 receptor inhibitors in ACS patients with CKD are sum-marized in Table 4. The Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) trial randomized patients with an ACS without ST-segment elevation to either a 300-mg loading dose of clopidogrel followed by 75 mg per day or placebo. Based on tertiles of renal function, the rela-tive risks (RR) and 95% CIs for the primary composite out-come associated with clopidogrel versus placebo were 0.74 (0.600.93) in the upper third, 0.68 (0.560.84) in the middle third, and 0.89 (0.761.05) in the lower third, with a Pinteraction of 0.11.43,44 In the Clopidogrel for the Reduction of Events During Observation (CREDO, a trial of patients undergoing planned PCI or coronary angiogram)45,46 and the Clopidogrel as Adjunctive Reperfusion TherapyThrombolysis in Myocardial Infarction 28 (CLARITY-TIMI 28) trial (a trial of patients with STEMI),47,48 there was a qualitative decline in the efficacy of clopidogrel versus placebo as renal func-tion worsened; the HRs (95% CIs) across renal function were 0.42 (0.260.69), 0.80 (0.511.25), and 1.42 (0.812.45) in CREDO and 0.6 (0.400.90), 0.6 (0.400.70), and 1.0 (0.701.6) in CLARITY-TIMI 28. In a substudy of the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance (CHARISMA) trial, among patients with and without diabetic nephropathy, the HRs (95% CIs) for clopidogrel versus placebo were 0.9 (0.801.0) for those without diabetic nephropathy and 1.1 (0.801.6) for those with diabetic nephropathy.52,53
In terms of safety, more bleeding occurred with clopido-grel than placebo overall; however, there was no signifi-cant interaction based on renal function in CURE, CREDO, or CLARITY-TIMI 28. Within the CHARISMA analysis, the frequency of severe bleeding according to the Global Utilization of Streptokinase and tPA for Occluded Arteries (GUSTO) definition among patients with diabetic nephropa-thy was nonsignificantly higher with clopidogrel than with placebo (2.6% versus 1.5%, P=0.075). In patients without dia-betic nephropathy, there was no difference in GUSTO severe bleeding between patients randomized to clopidogrel versus placebo (1.5% versus 1.3%, P=0.28).53
Prasugrel and ticagrelor are P2Y12 inhibitors that exhibit a more rapid onset, higher degrees of platelet inhibi-tion, and less interpatient variability than clopidogrel. The Trial to Assess Improvement in Therapeutic Outcomes by
Optimizing Platelet Inhibition With PrasugrelThrombolysis in Myocardial Infarction (TRITONTIMI 38) randomized subjects who presented with moderate- to high-risk ACS with scheduled PCI to either prasugrel or clopidogrel. Within this study, the risk reduction associated with prasugrel versus clopidogrel was 20% among those with CrCl 60 mL/min and 14% among those with CrCl
-
Washam et al Pharmacotherapy in CKD Patients With ACS 9
respectively.54,55 In addition, eptifibatide is contraindicated in patients requiring dialysis.54
Abciximab is cleared via the reticuloendothelial system, and no current recommendations exist for dose adjustment for patients with CKD. Data from randomized trials and observa-tional studies on the clinical outcomes of ACS patients with CKD receiving a GP IIb/IIIa receptor antagonist are summa-rized in Table 5.
When used at the time of PCI in ACS patients with CKD, outcomes with the use of GP IIb/IIIa receptor antagonists have been variable. A subgroup analysis of the Enhanced Suppression of the Platelet IIb/IIIa Receptor With Integrilin Therapy (ESPRIT) trial showed the treatment effect of eptifibatide was maintained among those with CrCl 81.3 mL/min), middle tertile (6481.2 mL/min), lower tertile (
-
10 Circulation March 24, 2015
Observational cohorts of ACS patients receiving GP IIb/IIIa receptor antagonists at the time of PCI have provided addi-tional insight into use in patients with CKD. Best et al57 assessed patients undergoing PCI in a large registry that divided patients into 3 categories according to creatinine clearance: >70, 5069, or
-
Washam et al Pharmacotherapy in CKD Patients With ACS 11
Freeman et al59 Observational, cohort study
889 patients with ACS, including 310 patients with renal insufficiency defined as CrCl*
-
12 Circulation March 24, 2015
patients undergoing PCI who received abciximab.60 Of the 1040 patients included, 44 were classified as having renal insufficiency. The authors reported no significant differences in the rates of in-hospital mortality or nonfatal major adverse cardiac events among patients with renal insufficiency com-pared with those without, although major bleeding occurred more frequently among patients with renal insufficiency (4.5% versus 0.6%; P=0.003). Although limited data are available on the comparative safety and effectiveness of dif-ferent GP IIb/IIIa receptor antagonists among patients with CKD, a subgroup analysis of the Do Tirofiban and ReoPro Give Similar Efficacy Outcome (TARGET) trial compared the outcomes of patients with renal insufficiency undergoing PCI who received either abciximab or tirofiban.61 The 4623 patients with a baseline SCr level available were divided into CrCl quartiles (114 mL/min). Although the rates of both ischemic and bleeding events were higher among patients with lower creatinine clear-ances, there was no interaction between the assigned GP IIb/IIIa receptor antagonist, CrCl, and clinical outcome.
An analysis of the Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) trial provided outcome data on the upstream use of GP IIb/IIIa receptor antagonists among patients presenting with ACS.56 This analysis showed tirofi-ban therapy to be effective in reducing ischemic events, with no evidence of treatment-by-CrCl interaction. Additionally, although decreasing renal function (P
-
Washam et al Pharmacotherapy in CKD Patients With ACS 13
Table 6. Summary of Enoxaparin Studies in Patients With ACS and CKD
Study Study Design Population End Points Results
ESSENCE-TIMI 11B65
Pooled subgroup analysis of 2 RCTs
7081 NSTE ACS patients enrolled in ESSENCE (n=3171) and TIMI 11B (n=3910) randomized to enoxaparin or UFH. CrCl 30 mL/min was an exclusion in 1 trial (ESSENCE), whereas SCr >2.0 mg/dL was an exclusion in the other (TIMI 11B). Severe renal impairment (CrCl* 30 mL/min) was found in 74 UFH-treated patients and 69 patients receiving enoxaparin (2%). The enoxaparin dose was 1 mg/kg every 12 h.
All-cause death, recurrent MI, and urgent revas-cularization at 43 d
In patients with CrCl 60 mL/min (n=7194), 3160 mL/min (n=3705), 30 mL/min (n=982). In the 3 renal function groups, LMWH was used in 30%, 31%, and 30%, respectively, whereas UFH was used in 22%, 24%, and 28%, respectively.
Mortality (30 d) Worsening renal function was an independent predictor of 30-d mortality and in-hospital major bleeding. Rates of 30-d mortality were significantly lower with LMWH alone than with UFH alone in patients with CrCl >60 mL/min and in those with CrCl 3160 mL/min. No significant difference was seen in patients with CrCl 90 (n=7462), >60 to 90 (n=7203), 3060 (n=3671), and 90 mL/min, 0.78 (0.660.92) for CrCl >60 to 90 mL/min, 0.94 (0.781.12) for CrCl 3060 mL/min, and 0.74 (0.38 1.44) for CrCl 90 mL/min, 1.91 (1.30 2.82) for CrCl >60 to 90 mL/min, 1.73 (1.112.70) for CrCl 3060 mL/min, and 3.60 (0.6719.21) for CrCl
-
14 Circulation March 24, 2015
the treatment effects of enoxaparin and UFH.65 Severe renal impairment was identified in 2% of patients in this pooled analysis. There was no statistically significant difference between enoxaparin and UFH with regard to the rates of occurrence of the primary composite end point (18.8% ver-sus 32.4%, respectively; P=0.12) or major hemorrhage (7.5% versus 5.8%, respectively; P=0.56) among patients with CrCl 30 mL/min. The association of CKD with outcomes among patients enrolled in the Superior Yield of the New Strategy of Enoxaparin, Revascularization, and Glycoprotein IIb/IIIa Inhibitors (SYNERGY) trial who received either enoxapa-rin or UFH was also assessed.68 Patients were placed into 3 groups based on CrCl:
-
Washam et al Pharmacotherapy in CKD Patients With ACS 15
significantly lower in the group receiving fondaparinux (2.4% versus 9.9%, P=0.001).75 Although the rates of major bleeding were lower with fondaparinux across all quartiles of estimated GFR, the difference was most marked among patients with a GFR 90mL/min) or mildly impaired renal function (CrCl >60 mL/min), the pharmacoki-netics of bivalirudin are linear, with an elimination half-life of 25 minutes. The elimination half-life is increased to 34 to 57 minutes in patients with moderate to severe renal impairment (CrCl between 10 and 59 mL/min) and 3.5 hours in patients with renal failure necessitating hemodialysis.7678 For patients with renal insufficiency, the product labeling recommends no reduction in the bolus dose for any degree of renal impair-ment, although the infusion dose of bivalirudin may need to be reduced and anticoagulant status monitored in patients with renal impairment (Table 1).28 Data from randomized trials and observational studies on the use of bivalirudin in ACS patients with CKD are shown in Table 7.
A meta-analysis79 of 3 randomized trials comparing bivali-rudin with UFH at the time of PCI (majority ACS) strati-fied by CrCl >90 mL/min (n=1578), CrCl 90 to 60 mL/min (n=2163), CrCl 59 to 30 mL/min (n=1255), and CrCl
-
16 Circulation March 24, 2015
Table 7. Summary of Bivalirudin Studies in Patients With ACS and CKD
Study Study Design Population End Points Results
Chew et al79 Meta-analysis of 3 trials: the Bivalirudin Angioplasty Study, CACHET trial and REPLACE-1
The trials included patients undergoing PCI receiving bivalirudin or UFH during PCI. Patients were stratified by CrCl* into groups: CrCl >90 mL/min (n=1578), CrCl 6090 mL/min (n=2163), CrCl 3059 mL/min (n=1255), and CrCl 3 mg/dL were excluded from the trials. The indication for PCI was UA in 65% of patients in this analysis.
Primary efficacy end point: composite of death, MI, or urgent revascularization
Adverse ischemic and bleeding events increased with worsening renal function. The ORs (95% CIs) for reduction of the composite ischemic end point with bivalirudin in the 4 CrCl strata were 0.79 (0.521.18), 0.73 (0.530.99), 0.77 (0.55-1.07), and 0.81 (0.125.23), respectively.
Bleeding (definition varied by trial)
The ORs (95% CIs) for reduction in bleeding events were 0.45 (0.210.96), 0.40 (0.091.86), and 0.46 (0.30-0.70) for patients in the CrCl >90 mL/min, CrCl 6090 mL/min, and CrCl 3059 mL/min groups, respectively. The absence of bleeding events in the CrCl 4 mg/dL. In this analysis, patients were grouped based on CrCl*: CrCl 60 mL/min (n=4824) and CrCl
-
Washam et al Pharmacotherapy in CKD Patients With ACS 17
with CrCl
-
18 Circulation March 24, 2015
Table 8. Summary of -Blocker Studies in Patients With ACS and CKD
Study Study Design Population End Points Results
Wali et al94 Post hoc analysis of pooled data from 2 RCTs (CAPRICORN and COPERNICUS)
4217 patients with either post-MI left ventricular dysfunction (CAPRICORN) or severe chronic HF (COPERNICUS) randomized to carvedilol or placebo; 46% of patients were from the CAPRICORN trial. Patients categorized based on eGFR*: eGFR >60 mL/min/1.73 m2 (n=1,651), eGFR 60 (n=2,566). Among those with eGFR 60, 1,116 had an eGFR 60: 0.59 (0.430.81); eGFR 60: 0.78 (0.64-0.95). In the subgroup with eGFR 60: 0.59 (0.42-0.82); eGFR 60: 0.77 (0.620.94).
HF mortality: eGFR >60: 0.58 (0.34-0.99); eGFR 60: 0.68 (0.520.88); in the subgroup with eGFR
-
Washam et al Pharmacotherapy in CKD Patients With ACS 19
ejection fraction 2.5 mg/dL or a serum potassium >5.0 mEq/L. Serious hyperkalemia (6.0 mEq/L) occurred in 5.5% of patients receiving eplerenone com-pared with 3.9% in the placebo group (P=0.002). For patients with CrCl 2.5 mg/dL in men and >2.0 mg/dL in women) or hyperkale-mia (serum potassium >5.0 mEq/L) coexists.87
A post hoc analysis of the EPHESUS trial evaluated serial changes in eGFR related to eplerenone use in patients after ACS. In this analysis, Rossignol et al125 found that 5792 patients assigned to eplerenone 25 to 50 mg/d had a significant decline in their eGFR, with a mean adjusted difference of 1.40.3 mLmin11.73 m2 compared with placebo (P3 mg/dL.
Shlipak et al, 2001122
Observational, retrospective analysis of the CCP database
20 902 Medicare beneficiaries admitted for MI with LVEF
-
20 Circulation March 24, 2015
a 1.15-fold increased odds of experiencing a >20% decline in eGFR within the first month compared with placebo (P=0.017).125 However, an eGFR 60 mLmin11.73 m2 was not associated with early worsening renal function, and there was no interaction between worsening renal function and the favorable effects of eplerenone on cardiovascular death or hospitalization (P=0.77 for interaction) and hospitalization for heart failure (P=0.82 for interaction).125StatinsA large body of literature supports of the use of statins after an ACS to reduce the risk of death or vascular events. Current guidelines recommend statins regardless of baseline low-den-sity lipoprotein level in all ACS patients in the absence of con-traindications.26,27 With regard to CKD patients, those receiving chronic dialysis in particular, the use of statins has been more controversial. No randomized controlled trials have assessed the safety and efficacy of statins in patients with ACS and
CKD. Furthermore, patients with SCr >2 mg/dL were excluded from the original ACS randomized trials of early initiation of statins.126,127 However, in primary prevention, randomized tri-als of statin therapy in patients with CKD have yielded mixed results.128131 Early studies found no benefit of statin therapy among patients with CKD (mostly dialysis dependent),129131 which led to speculation that in ESRD, there may be a more advanced atherosclerotic state that leads to more sudden deaths caused by arrhythmias than among patients without ESRD. However, more recently, the largest of these studies, the Study of Heart and Renal Protection (SHARP), included patients with CKD both on dialysis and not on dialysis and showed a benefit of simvastatin plus ezetimibe therapy on the risk of the primary composite end point of first major atherosclerotic event (RR, 0.83; 95% CI, 0.740.94; P=0.0021), although no statistically significant difference was observed for the risk of vascular death (RR, 0.93; 95% CI, 0.801.07).128 Although
Table 10. Summary of Statin Studies in Patients With ACS and CKD
Study Study Design Population End Points Results
Lim et al132 Observational, retrospective analysis of KAMIR cohort
12 865 AMI patients; 3256 patients with AMI and renal insufficiency (eGFR
-
Washam et al Pharmacotherapy in CKD Patients With ACS 21
statin trials in ACS have largely excluded patients with CKD, observational studies have evaluated the safety and efficacy of statins in these patients.32,132134 The data on the use of statins in ACS patients with CKD are summarized in Table 10. The Korea Acute Myocardial Infarction Registry (KAMIR) study was observational and evaluated 12 865 patients with MI, 3256 of whom had renal dysfunction (defined as eGFR
-
22 Circulation March 24, 2015
Disclosures
Writing Group Disclosures
Writing Group Member Employment Research Grant
Other Research Support
Speakers Bureau/
HonorariaExpert
WitnessOwnership
InterestConsultant/Advisory
Board Other
Jeffrey B. Washam
Duke Heart Center None None None None None None None
L. Kristin Newby
Duke University Medical Center
Amylin*; Bristol Myers- Squibb*; Duke; Eli Lilly & Co*;
GlaxoSmithKline; Johnson & Johnson*; Merck & Co; NIH; Regado Biosciences*
None None None None Amgen; AstraZeneca*; Cubist*; Daiichi
Sankyo*; Genentech*;
GlaxoSmithKline*; Novartis*
American Heart Journal*; Society of Chest Pain Centers*;
JAHA*
Amber L. Beitelshees
University of Maryland None None None None None None None
Mauricio G. Cohen
University of Miami Miller School of Medicine
None None None None None Daiichi-Sankyo; AstraZeneca; The Medicines
Company*
None
Timothy D. Henry
Cedars-Sinai Heart Institute
None None None None None Daiichi Sankyo*; Eli Lilly*; The
Medicines Company*
None
Charles A. Herzog
Hennepin Healthcare System, Inc
AHRQ DEcIDE Network; NIH/NIDDK; NHLBI
Affymax*; Amgen; Gilead; Johnson &
Johnson
CardioRenal Society of
America & NKF of Arizona*; Greenfield
Health System*; Keryx*
None Boston Scientific*; Cambridge
Heart*; Johnson & Johnson*;
Merck*
Abbott*; Affymax*; Amgen;
CorMedix*; FibroGen*;
Fresenius*; Keryx*; GlaxoSmithKline*;
AbbVie*
None
Navin K. Kapur Tufts Medical Center None None None None None None None
Jessica L. Mega
Brigham & Womens Hospital
Daiichi Sankyo; AstraZeneca
None None None None Bayer*; Janssen*; Portola*
None
Venu Menon Cleveland Clinic AstraZeneca None None None None None None
Robert L. Page II
University of Colorado School of Pharmacy
None None None None None None None
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be significant if (a) the person receives $10 000 or more during any 12-month period, or 5% or more of the persons gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be modest if it is less than significant under the preceding definition.
*Modest.Significant.
by guest on March 22, 2015http://circ.ahajournals.org/Downloaded from
-
Washam et al Pharmacotherapy in CKD Patients With ACS 23
References 1. Fox CS, Muntner P, Chen AY, Alexander KP, Roe MT, Cannon CP, Saucedo
JF, Kontos MC, Wiviott SD; Acute Coronary Treatment and Intervention Outcomes Network Registry. Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and nonST-segment elevation myocardial infarction in patients with chronic kidney disease: a report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation. 2010;121:357365. doi: 10.1161/CIRCULATIONAHA.109.865352.
2. Wright RS, Reeder GS, Herzog CA, Albright RC, Williams BA, Dvorak DL, Miller WL, Murphy JG, Kopecky SL, Jaffe AS. Acute myocardial infarction and renal dysfunction: a high-risk combination. Ann Intern Med. 2002;137:563570.
3. Shlipak MG, Heidenreich PA, Noguchi H, Chertow GM, Browner WS, McClellan MB. Association of renal insufficiency with treatment and outcomes after myocardial infarction in elderly patients. Ann Intern Med. 2002;137:555562.
4. Moscucci M, Fox KA, Cannon CP, Klein W, Lpez-Sendn J, Montalescot G, White K, Goldberg RJ. Predictors of major bleeding in acute coronary syndromes: the Global Registry of Acute Coronary Events (GRACE). Eur Heart J. 2003;24:18151823.
5. Coca SG, Krumholz HM, Garg AX, Parikh CR. Underrepresentation of renal disease in randomized controlled trials of cardiovascular disease. JAMA. 2006;296:13771384. doi: 10.1001/jama.296.11.1377.
6. Charytan D, Kuntz RE. The exclusion of patients with chronic kid-ney disease from clinical trials in coronary artery disease. Kidney Int. 2006;70:20212030. doi: 10.1038/sj.ki.5001934.
7. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39:S1S266.
8. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:S1S150.
9. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:12961305. doi: 10.1056/NEJMoa041031.
10. Tonelli M, Muntner P, Lloyd A, Manns BJ, Klarenbach S, Pannu N, James MT, Hemmelgarn BR; Alberta Kidney Disease Network. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: a population-level cohort study. Lancet. 2012;380:807814. doi: 10.1016/S0140-6736(12)60572-8.
11. Herzog CA, Littrell K, Arko C, Frederick PD, Blaney M. Clinical char-acteristics of dialysis patients with acute myocardial infarction in the United States: a collaborative project of the United States Renal Data System and the National Registry of Myocardial Infarction. Circulation. 2007;116:14651472. doi: 10.1161/CIRCULATIONAHA.107.696765.
12. Sosnov J, Lessard D, Goldberg RJ, Yarzebski J, Gore JM. Differential symptoms of acute myocardial infarction in patients with kidney disease: a community-wide perspective. Am J Kidney Dis. 2006;47:378384. doi: 10.1053/j.ajkd.2005.11.017.
13. Szummer K, Lundman P, Jacobson SH, Schn S, Lindbck J, Stenestrand U, Wallentin L, Jernberg T; SWEDEHEART. Influence of renal func-tion on the effects of early revascularization in nonST-elevation myo-cardial infarction: data from the Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies (SWEDEHEART). Circulation. 2009;120:851858. doi: 10.1161/CIRCULATIONAHA.108.838169.
14. Shroff GR, Frederick PD, Herzog CA. Renal failure and acute myocardial infarction: clinical characteristics in patients with advanced chronic kid-ney disease, on dialysis, and without chronic kidney disease: a collabora-tive project of the United States Renal Data System/National Institutes of Health and the National Registry of Myocardial Infarction. Am Heart J. 2012;163:399406. doi: 10.1016/j.ahj.2011.12.002.
15. Szummer K, Lundman P, Jacobson SH, Schn S, Lindbck J, Stenestrand U, Wallentin L, Jernberg T; SWEDEHEART. Relation between renal function, presentation, use of therapies and in-hospital complications in acute coronary syndrome: data from the SWEDEHEART register. J Intern Med. 2010;268:4049. doi: 10.1111/j.1365-2796.2009.02204.x.
16. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD; Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myo-cardial infarction. Circulation. 2012;126:20202035. doi: 10.1161/CIR.0b013e31826e1058.
17. Wu AHB, Jaffe AS, Apple FS, Jesse RL, Francis GL, Morrow DA, Newby LK, Ravkilde J, Tang WHW, Christenson RH, Cannon CP, Storrow AB. National Academy of Clinical Biochemistry laboratory medicine prac-tice guidelines: use of cardiac troponin and B-type natriuretic peptide or N-terminal proB-type natriuretic peptide for etiologies other than acute coronary syndromes and heart failure. Clin Chem. 2007;53:20862096.
18. Newby LK, Jesse RL, Babb JD, Christenson RH, De Fer TM, Diamond GA, Fesmire FM, Geraci SA, Gersh BJ, Larsen GC, Kaul S, McKay CR, Philippides GJ, Weintraub WS. ACCF 2012 expert consensus docu-ment on practical clinical considerations in the interpretation of troponin elevations: a report of the American College of Cardiology Foundation task force on Clinical Expert Consensus Documents. J Am Coll Cardiol. 2012;60:24272463. doi: 10.1016/j.jacc.2012.08.969.
19. Berger AK, Duval S, Krumholz HM. Aspirin, beta-blocker, and angio-tensin-converting enzyme inhibitor therapy in patients with end-stage renal disease and an acute myocardial infarction. J Am Coll Cardiol. 2003;42:201208.
20. Beattie JN, Soman SS, Sandberg KR, Yee J, Borzak S, Garg M, McCullough PA. Determinants of mortality after myocardial infarction in patients with
Reviewer Disclosures
Reviewer Employment Research GrantOther Research
SupportSpeakers Bureau/
Honoraria Expert WitnessOwnership
InterestConsultant/
Advisory Board Other
Sripal Bangalore New York University NHLBI (PI of the ISCHEMIA CKD
trial)
None None None None None None
Gregory Barsness Mayo Clinic None None None None None None None
David Charytan Brigham and Womens Hospital
NIH Medtronic None Fresenius None Keryx*; Medtronic*
None
Peter McCullough Baylor University Medical Center, Baylor Heart and Vascular Institute, Baylor Jack and Jane Hamilton
Heart and Vascular Hospital, Dallas, TX, The Heart Hospital, Plano, TX
None None None None None None None
This table represents the relationships of reviewers that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all reviewers are required to complete and submit. A relationship is considered to be significant if (a) the person receives $10 000 or more during any 12-month period, or 5% or more of the persons gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be modest if it is less than significant under the preceding definition.
*Modest.Significant.
by guest on March 22, 2015http://circ.ahajournals.org/Downloaded from
-
24 Circulation March 24, 2015
advanced renal dysfunction. Am J Kidney Dis. 2001;37:11911200. doi: 10.1053/ajkd.2001.24522.
21. McCullough PA, Sandberg KR, Borzak S, Hudson MP, Garg M, Manley HJ. Benefits of aspirin and beta-blockade after myocardial infarction in patients with chronic kidney disease. Am Heart J. 2002;144:226232.
22. Nyman HA, Dowling TC, Hudson JQ, Peter WL, Joy MS, Nolin TD. Comparative evaluation of the Cockcroft-Gault Equation and the Modification of Diet in Renal Disease (MDRD) study equation for drug dosing: an opinion of the Nephrology Practice and Research Network of the American College of Clinical Pharmacy. Pharmacotherapy. 2011;31:11301144. doi: 10.1592/phco.31.11.1130.
23. Melloni C, Peterson ED, Chen AY, Szczech LA, Newby LK, Harrington RA, Gibler WB, Ohman EM, Spinler SA, Roe MT, Alexander KP. Cockcroft-Gault versus modification of diet in renal disease: importance of glomerular filtration rate formula for classification of chronic kidney dis-ease in patients with non-ST-segment elevation acute coronary syndromes. J Am Coll Cardiol. 2008;51:991996. doi: 10.1016/j.jacc.2007.11.045.
24. Wargo KA, Eiland EH 3rd, Hamm W, English TM, Phillippe HM. Comparison of the modification of diet in renal disease and Cockcroft-Gault equations for antimicrobial dosage adjustments. Ann Pharmacother. 2006;40:12481253. doi: 10.1345/aph.1G635.
25. Golik MV, Lawrence KR. Comparison of dosing recommendations for antimicrobial drugs based on two methods for assessing kidney func-tion: Cockcroft-Gault and Modification of Diet in Renal Disease. Pharmacotherapy. 2008;28:11251132. doi: 10.1592/phco.28.9.1125.
26. OGara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX, Anderson JL, Jacobs AK, Halperin JL, Albert NM, Brindis RG, Creager MA, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Kushner FG, Ohman EM, Stevenson WG, Yancy CW; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362e425. doi: 10.1161/CIR.0b013e3182742cf6.
27. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, Chavey WE 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC Jr. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 guide-lines for the management of patients with unstable angina/non-ST-eleva-tion myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;123:e426e579. doi: 10.1161/CIR.0b013e318212bb8b.
28. Angiomax (bivalirudin) injection [package insert]. Parsippany, NJ: The Medicines Co; 2013.
29. Melloni C, Roe MT, Chen AY, Wang TY, Wiviott SD, Ho PM, Peterson ED, Alexander KP. Use of early clopidogrel by reperfusion strategy among patients presenting with ST-segment elevation myocardial infarc-tion. Circ Cardiovasc Qual Outcomes. 2011;4:603609. doi: 10.1161/CIRCOUTCOMES.111.961045.
30. Gibson CM, Pinto DS, Murphy SA, Morrow DA, Hobbach HP, Wiviott SD, Giugliano RP, Cannon CP, Antman EM, Braunwald E; TIMI Study Group. Association of creatinine and creatinine clearance on presenta-tion in acute myocardial infarction with subsequent mortality. J Am Coll Cardiol. 2003;42:15351543.
31. Hobbach HP, Gibson CM, Giugliano RP, Hundertmark J, Schaeffer C, Tscherleniak W, Schuster P. The prognostic value of serum creatinine on admission in fibrinolytic-eligible patients with acute myocardial infarction. J Thromb Thrombolysis. 2003;16:167174. doi: 10.1023/B: THRO.0000024055.13207.50.
32. Keough-Ryan TM, Kiberd BA, Dipchand CS, Cox JL, Rose CL, Thompson KJ, Clase CM. Outcomes of acute coronary syndrome in a large Canadian cohort: impact of chronic renal insufficiency, cardiac interventions, and ane-mia. Am J Kidney Dis. 2005;46:845855. doi: 10.1053/j.ajkd.2005.07.043.
33. Medi C, Montalescot G, Budaj A, Fox KA, Lpez-Sendn J, FitzGerald G, Brieger DB; GRACE Investigators. Reperfusion in patients with renal dysfunction after presentation with ST-segment elevation or left bundle branch block: GRACE (Global Registry of Acute Coronary Events). JACC Cardiovasc Interv. 2009;2:2633. doi: 10.1016/j.jcin.2008.09.010.
34. Dragu R, Behar S, Sandach A, Boyko V, Kapeliovich M, Rispler S, Hammerman H. Should primary percutaneous coronary intervention be the preferred method of reperfusion therapy for patients with renal
failure and ST-elevation acute myocardial infarction? Am J Cardiol. 2006;97:11421145. doi: 10.1016/j.amjcard.2005.11.028.
35. Brass LM, Lichtman JH, Wang Y, Gurwitz JH, Radford MJ, Krumholz HM. Intracranial hemorrhage associated with thrombolytic therapy for elderly patients with acute myocardial infarction: results from the Cooperative Cardiovascular Project. Stroke. 2000;31:18021811.
36. Simoons ML, Maggioni AP, Knatterud G, Leimberger JD, de Jaegere P, van Domburg R, Boersma E, Franzosi MG, Califf R, Schrder R. Individual risk assessment for intracranial haemorrhage during thrombo-lytic therapy. Lancet. 1993;342:15231528.
37. Antithrombotic Trialists Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myo-cardial infarction, and stroke in high risk patients [published correction appears in BMJ. 2002;324:141]. BMJ. 2002;324:7186.
38. Yan AT, Yan RT, Tan M, Constance C, Lauzon C, Zaltzman J, Wald R, Fitchett D, Langer A, Goodman SG; Canadian Acute Coronary Syndromes (ACS) Registry Investigators. Treatment and one-year outcome of patients with renal dysfunction across the broad spectrum of acute coronary syn-dromes. Can J Cardiol. 2006;22:115120.
39. Sciahbasi A, Arcieri R, Quarto M, Pendenza G, Lanzillo C, Summaria F, Romagnoli E, Commisso C, Penco M, Lioy E. Impact of chronic aspi-rin and statin therapy on presentation of patients with acute myocardial infarction and impaired renal function. Prev Cardiol. 2010;13:1822. doi: 10.1111/j.1751-7141.2009.00050.x.
40. Baigent C, Landray M, Leaper C, Altmann P, Armitage J, Baxter A, Cairns HS, Collins R, Foley RN, Frighi V, Kourellias K, Ratcliffe PJ, Rogerson M, Scoble JE, Tomson CR, Warwick G, Wheeler DC. First United Kingdom Heart and Renal Protection (UK-HARP-I) study: biochemical efficacy and safety of simvastatin and safety of low-dose aspirin in chronic kidney dis-ease. Am J Kidney Dis. 2005;45:473484. doi: 10.1053/j.ajkd.2004.11.015.
41. Ethier J, Bragg-Gresham JL, Piera L, Akizawa T, Asano Y, Mason N, Gillespie BW, Young EW. Aspirin prescription and outcomes in hemodial-ysis patients: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2007;50:602611. doi: 10.1053/j.ajkd.2007.07.007.
42. Jneid H, Anderson JL, Wright RS, Adams CD, Bridges CR, Casey DE Jr, Ettinger SM, Fesmire FM, Ganiats TG, Lincoff AM, Peterson ED, Philippides GJ, Theroux P, Wenger NK, Zidar JP. 2012 ACCF/AHA focused update of the Guideline for the Management of Patients With Unstable Angina/NonST-Elevation Myocardial Infarction (updating the 2007 guideline and replacing the 2011 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2012;126:875910. doi: 10.1161/CIR.0b013e318256f1e0.
43. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK; Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345:494502. doi: 10.1056/NEJMoa010746.
44. Keltai M, Tonelli M, Mann JF, Sitkei E, Lewis BS, Hawken S, Mehta SR, Yusuf S; CURE Trial Investigators. Renal function and outcomes in acute coronary syndrome: impact of clopidogrel. Eur J Cardiovasc Prev Rehabil. 2007;14:312318. doi: 10.1097/01.hjr.0000220582.19516.a6.
45. Steinhubl SR, Berger PB, Mann JT 3rd, Fry ET, DeLago A, Wilmer C, Topol EJ; CREDO Investigators: Clopidogrel for the Reduction of Events During Observation. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial [published correction appears in JAMA. 2003;289:987]. JAMA. 2002;288:24112420.
46. Best PJ, Steinhubl SR, Berger PB, Dasgupta A, Brennan DM, Szczech LA, Califf RM, Topol EJ; CREDO Investigators. The efficacy and safety of short- and long-term dual antiplatelet therapy in patients with mild or moderate chronic kidney disease: results from the Clopidogrel for the Reduction of Events During Observation (CREDO) trial. Am Heart J. 2008;155:687693. doi: 10.1016/j.ahj.2007.10.046.
47. Sabatine MS, Cannon CP, Gibson CM, Lpez-Sendn JL, Montalescot G, Theroux P, Claeys MJ, Cools F, Hill KA, Skene AM, McCabe CH, Braunwald E; CLARITY-TIMI 28 Investigators. Addition of clopido-grel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation. N Engl J Med. 2005;352:11791189. doi: 10.1056/NEJMoa050522.
48. Ahmed S, Michael Gibson C, Cannon CP, Murphy SA, Sabatine MS. Impact of reduced glomerular filtration rate on outcomes in patients with ST-segment elevation myocardial infarction undergoing fibrinolysis: a CLARITY-TIMI 28 analysis. J Thromb Thrombolysis. 2011;31:493500. doi: 10.1007/s11239-011-0566-9.
by guest on March 22, 2015http://circ.ahajournals.org/Downloaded from
-
Washam et al Pharmacotherapy in CKD Patients With ACS 25
49. Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, Neumann FJ, Ardissino D, De Servi S, Murphy SA, Riesmeyer J, Weerakkody G, Gibson CM, Antman EM; TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357:20012015. doi: 10.1056/NEJMoa0706482.
50. Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, Horrow J, Husted S, James S, Katus H, Mahaffey KW, Scirica BM, Skene A, Steg PG, Storey RF, Harrington RA, Freij A, Thorsn M; PLATO Investigators. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361:10451057. doi: 10.1056/NEJMoa0904327.
51. James S, Budaj A, Aylward P, Buck KK, Cannon CP, Cornel JH, Harrington RA, Horrow J, Katus H, Keltai M, Lewis BS, Parikh K, Storey RF, Szummer K, Wojdyla D, Wallentin L. Ticagrelor versus clopidogrel in acute coronary syndromes in relation to renal function: results from the Platelet Inhibition and Patient Outcomes (PLATO) trial. Circulation. 2010;122:10561067. doi: 10.1161/CIRCULATIONAHA.109.933796.
52. Bhatt DL, Fox KA, Hacke W, Berger PB, Black HR, Boden WE, Cacoub P, Cohen EA, Creager MA, Easton JD, Flather MD, Haffner SM, Hamm CW, Hankey GJ, Johnston SC, Mak KH, Mas JL, Montalescot G, Pearson TA, Steg PG, Steinhubl SR, Weber MA, Brennan DM, Fabry-Ribaudo L, Booth J, Topol EJ; CHARISMA Investigators. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354:17061717. doi: 10.1056/NEJMoa060989.
53. Dasgupta A, Steinhubl SR, Bhatt DL, Berger PB, Shao M, Mak KH, Fox KA, Montalescot G, Weber MA, Haffner SM, Dimas AP, Steg PG, Topol EJ; CHARISMA Investigators. Clinical outcomes of patients with diabetic nephropathy randomized to clopidogrel plus aspirin versus aspirin alone (a post hoc analysis of the clopidogrel for high atherothrombotic risk and ischemic stabilization, management, and avoidance [CHARISMA] trial). Am J Cardiol. 2009;103:13591363. doi: 10.1016/j.amjcard.2009.01.342.
54. Integrilin (eptifibatide) injection [product information]. Whitehouse Station, NJ: Merck & Co, Inc; 2014.
55. Aggrastat (tirofiban) injection [product information]. Somerset, NJ: Medicure Pharma, Inc; 2014.
56. Januzzi JL Jr, Snapinn SM, DiBattiste PM, Jang IK, Theroux P. Benefits and safety of tirofiban among acute coronary syndrome patients with mild to moderate renal insufficiency: results from the Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) trial. Circulation. 2002;105:23612366.
57. Best PJ, Lennon R, Gersh BJ, Ting HH, Rihal CS, Bell MR, Herzog CA, Holmes DR Jr, Berger PB. Safety of abciximab in patients with chronic renal insufficiency who are undergoing percutaneous coro-nary interventions. Am Heart J. 2003;146:345350. doi: 10.1016/S0002-8703(03)00231-X.
58. Reddan DN, OShea JC, Sarembock IJ, Williams KA, Pieper KS, Santoian E, Owen WF, Kitt MM, Tcheng JE. Treatment effects of eptifibatide in planned coronary stent implantation in patients with chronic kidney dis-ease (ESPRIT Trial). Am J Cardiol. 2003;91:1721.
59. Freeman RV, Mehta RH, Al Badr W, Cooper JV, Kline-Rogers E, Eagle KA. Influence of concurrent renal dysfunction on outcomes of patients with acute coronary syndromes and implications of the use of glycopro-tein IIb/IIIa inhibitors. J Am Coll Cardiol. 2003;41:718724.
60. Frilling B, Zahn R, Fraiture B, Mark B, Dnges K, Becker T, Siegler KE, Seidl K, Rustige J, Senges J. Comparison of efficacy and complication rates after percutaneous coronary interventions in patients with and without renal insufficiency treated with abciximab. Am J Cardiol. 2002;89:450452.
61. Berger PB, Best PJ, Topol EJ, White J, DiBattiste PM, Chan AW, Kristensen SD, Herrmann HC, Moliterno DJ. The relation of renal function to ischemic and bleeding outcomes with 2 different glycoprotein IIb/IIIa inhibitors: the do Tirofiban and ReoPro Give Similar Efficacy Outcome (TARGET) trial. Am Heart J. 2005;149:869875. doi: 10.1016/j.ahj.2004.12.002.
62. Melloni C, James SK, White JA, Giugliano RP, Harrington RA, Huber K, Tricoci P, Armstrong PW, Van de Werf F, Montalescot G, Califf RM, Newby LK. Safety and efficacy of adjusted-dose eptifibatide in patients with acute coronary syndromes and reduced renal function. Am Heart J. 2011;162:884892.e1. doi: 10.1016/j.ahj.2011.08.020.
63. Oler A, Whooley MA, Oler J, Grady D. Adding heparin to aspirin reduces the incidence of myocardial infarction and death in patients with unstable angina: a meta-analysis. JAMA. 1996;276:811815.
64. Hirsh J, Bauer KA, Donati MB, Gould M, Samama MM, Weitz JI; American College of Chest Physicians. Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl):141S159S. doi: 10.1378/chest.08-0689.
65. Spinler SA, Inverso SM, Cohen M, Goodman SG, Stringer KA, Antman EM; ESSENCE and TIMI 11B Investigators. Safety and efficacy of unfraction-ated heparin versus enoxaparin in patients who are obese and patients with severe renal impairment: analysis from the ESSENCE and TIMI 11B stud-ies. Am Heart J. 2003;146:3341. doi: 10.1016/S0002-8703(03)00121-2.
66. Collet JP, Montalescot G, Agnelli G, Van de Werf F, Gurfinkel EP, Lpez-Sendn J, Laufenberg CV, Klutman M, Gowda N, Gulba D; GRACE Investigators. Non-ST-segment elevation acute coronary syndrome in patients with renal dysfunction: benefit of low-molecular-weight heparin alone or with glycoprotein IIb/IIIa inhibitors on outcomes: the Global Registry of Acute Coronary Events. Eur Heart J. 2005;26:22852293. doi: 10.1093/eurheartj/ehi337.
67. Fox KA, Antman EM, Montalescot G, Agewall S, SomaRaju B, Verheugt FW, Lopez-Sendon J, Hod H, Murphy SA, Braunwald E. The impact of renal dysfunction on outcomes in the ExTRACT-TIMI 25 trial. J Am Coll Cardiol. 2007;49:22492255. doi: 10.1016/j.jacc.2006.12.049.
68. Spinler SA, Mahaffey KW, Gallup D, Levine GN, Ferguson JJ 3rd, Rao SV, Gallo R, Ducas J, Goodman SG, Antman E, White HD, Biasucci L, Becker RC, Col JJ, Cohen M, Harrington RA, Califf RM; SYNERGY Trial Investigators. Relationship between renal function and outcomes in high-risk patients with non-ST-segment elevation acute coronary syn-dromes: results from SYNERGY. Int J Cardiol. 2010;144:3641. doi: 10.1016/j.ijcard.2009.03.119.
69. Fox KA, Bassand JP, Mehta SR, Wallentin L, Theroux P, Piegas LS, Valentin V, Moccetti T, Chrolavicius S, Afzal R, Yusuf S; OASIS 5 Investigators. Influence of renal function on the efficacy and safety of fondaparinux relative to enoxaparin in non ST-segment elevation acute coronary syndromes. Ann Intern Med. 2007;147:304310.
70. Becker RC, Spencer FA, Gibson M, Rush JE, Sanderink G, Murphy SA, Ball SP, Antman EM; TIMI 11A Investigators. Influence of patient charac-teristics and renal function on factor Xa inhibition pharmacokinetics and pharmacodynamics after enoxaparin administration in non-ST-segment elevation acute coronary syndromes. Am Heart J. 2002;143:753759.
71. Lim W, Dentali F, Eikelboom JW, Crowther MA. Meta-analysis: low-molecular-weight heparin and bleeding in patients with severe renal insuf-ficiency. Ann Intern Med. 2006;144:673684.
72. LaPointe NM, Chen AY, Alexander KP, Roe MT, Pollack CV Jr, Lytle BL, Ohman ME, Gibler BW, Peterson ED. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non ST-segment ele-vation acute coronary syndromes. Arch Intern Med. 2007;167:15391544. doi: 10.1001/archinte.167.14.1539.
73. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, Chavey WE 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS. ACC/AHA 2007 guidelines for the management of patients with unstable angina/nonST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/NonST-Elevation Myocardial Infarction). Circulation. 2007;116:e148304.
74. Samama MM, Gerotziafas GT. Evaluation of the pharmacological proper-ties and clinical results of the synthetic pentasaccharide (fondaparinux). Thromb Res. 2003;109:111.
75. Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators, Yusuf S, Mehta SR, Chrolavicius S, Afzal R, Pogue J, Granger CB, Budaj A, Peters RJG, Bassand J-P, Wallentin L, Joyner C, Fox KAA. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med. 2006;354:14641476.
76. Lui HK. Dosage, pharmacological effects and clinical outcomes for bivalirudin in percutaneous coronary intervention. J Invasive Cardiol. 2000;(suppl F):41F52F.
77. Robson RA. The influence of dose, gender and kidney function on bivali-rudin pharmacokinetics and pharmacodynamics in patients undergoing percutaneous transluminal angioplasty [abstract]. Cambridge, MA; The Medicines Company; 2000. Data on file.
78. Scica D. A pharmacokinetic and pharmacodynamic study of BG8967 in subjects with renal insufficiency: Study C93-313. Cambridge, MA; The Medicines Company; 2000. Data on file.
79. Chew DP, Bhatt DL, Kimball W, Henry TD, Berger P, McCullough PA, Feit F, Bittl JA, Lincoff AM. Bivalirudin provides increasing benefit with decreasing renal function: a meta-analysis of randomized trials. Am J Cardiol. 2003;92:919923.
80. Chew DP, Lincoff AM, Gurm H, Wolski K, Cohen DJ, Henry T, Feit F, Topol EJ; REPLACE-2 Investigators. Bivalirudin versus heparin and glyco-protein IIb/IIIa inhibition among patients with renal impairment undergoing
by guest on March 22, 2015http://circ.ahajournals.org/Downloaded from
-
26 Circulation March 24, 2015
percutaneous coronary intervention (a subanalysis of the REPLACE-2 trial). Am J Cardiol. 2005;95:581585. doi: 10.1016/j.amjcard.2004.11.003.
81. Delhaye C, Maluenda G, Wakabayashi K, Ben-Dor I, Collins SD, Syed AI, Gonzalez MA, Gaglia MA, Torguson R, Xue Z, Suddath WO, Satler LF, Kent KM, Lindsay J, Pichard AD, Waksman R. Safety and in-hospital outcomes of bivalirudin use in dialysis patients undergoing percutaneous coronary interven-tion. Am J Cardiol. 2010;105:297301. doi: 10.1016/j.amjcard.2009.09.030.
82. Mehran R, Nikolsky E, Lansky AJ, Kirtane AJ, Kim YH, Feit F, Manoukian S, Moses JW, Ebrahimi R, Ohman EM, White HD, Pocock SJ, Dangas GD, Stone GW. Impact of chronic kidney disease on early (30-day) and late (1-year) outcomes of patients with acute coronary syndromes treated with alternative antithrombotic treatment strategies: an ACUITY (Acute Catheterization and Urgent Intervention Triage strategY) substudy. JACC Cardiovasc Interv. 2009;2:748757. doi: 10.1016/j.jcin.2009.05.018.
83. Saltzman AJ, Stone GW, Claessen BE, Narula A, Leon-Reyes S, Weisz G, Brodie B, Witzenbichler B, Guagliumi G, Kornowski R, Dudek D, Metzger DC, Lansky AJ, Nikolsky E, Dangas GD, Mehran R. Long-term impact of chronic kidney disease in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coro-nary intervention: the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) trial. JACC Cardiovasc Interv. 2011;4:10111019. doi: 10.1016/j.jcin.2011.06.012.
84. Stone GW, Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, Kornowski R, Hartmann F, Gersh BJ, Pocock SJ, Dangas G, Wong SC, Kirtane AJ, Parise H, Mehran R; HORIZONS-AMI Trial Investigators. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med. 2008;358:22182230. doi: 10.1056/NEJMoa0708191.
85. Antman EM, Morrow DA, McCabe CH, Murphy SA, Ruda M, Sadowski Z, Budaj A, Lpez-Sendn JL, Guneri S, Jiang F, White HD, Fox KA, Braunwald E; ExTRACT-TIMI 25 Investigators. Enoxaparin ver-sus unfractionated heparin with fibrinolysis for ST-elevation myocar-dial infarction. N Engl J Med. 2006;354:14771488. doi: 10.1056/NEJMoa060898.
86. Wright RS,Anderson JL, Adams CD, Bridges CR, Casey DE Jr, Ettinger SM, Fesmire FM, Ganiats TG, Jneid H, Lincoff AM, Peterson ED, Philippides GJ, Theroux P, Wenger NK,Zidar JP. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocar-dial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;57:e215e367. doi: 10.1016/j.jacc.2011.02.011.
87. Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, Hochman JS, Krumholz HM, Lamas GA, Mullany CJ, Pearle DL, Sloan MA, Smith SC Jr. 2007 Focused update of the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction) [pub-lished correction appears in J Am Coll Cardiol. 2008;51:977]. J Am Coll Cardiol. 2008;51:210247. doi: 10.1016/j.jacc.2007.10.001.
88. First International Study of Infarct Survival Collaborative Group. Randomised trial of intravenous atenolol among 16 027 cases of suspected acute myocardial infarction: ISIS-1. Lancet. 1986;2:5766.
89. The MIAMI Trial Research Group. Metoprolol in acute myocardial infarc-tion (MIAMI): a randomised placebo-controlled international trial. Eur Heart J. 1985;6:199226.
90. Chen ZM, Pan HC, Chen YP, Peto R, Collins R, Jiang LX, Xie JX, Liu LS; COMMIT (ClOpidogrel and Metoprolol in Myocardial Infarction Trial) Collaborative Group. Early intravenous then oral metopro-lol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005;366:16221632. doi: 10.1016/S0140-6736(05)67661-1.
91. Propranolol in acute myocardial infarction: a multicentre trial. Lancet. 1966;2:14351438.
92. Dargie HJ. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet. 2001;357:13851390.
93. Tenormin oral tablets, atenolol oral tablets [product information]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2012.
94. Wali RK, Iyengar M, Beck GJ, Chartyan DM, Chonchol M, Lukas MA, Cooper C, Himmelfarb J, Weir MR, Berl T, Henrich WL, Cheung AK. Efficacy and safety of carvedilol in treatment of heart failure with chronic kidney disease: a meta-analysis of randomized trials. Circ Heart Fail. 2011;4:1826. doi: 10.1161/CIRCHEARTFAILURE.109.932558.
95. Bae EH, Lim SY, Cho KH, Choi JS, Kim CS, Park JW, Ma SK, Jeong MH, Kim SW. GFR and cardiovascular outcomes after acute myocardial infarction: results from the Korea Acute Myocardial Infarction Registry. Am J Kidney Dis. 2012;59:795802. doi: 10.1053/j.ajkd.2012.01.016.
96. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. Lancet. 1995;345:669685.
97. Gruppo Italiano per lo Studio della Sopravvivenza nellinfarto Miocardico. GISSI-3: effects of lisinopril and transdermal glyceryl trini-trate singly and together on 6-week mortality and ventricular function after acute myocardial infarction. Lancet. 1994;343:11151122.
98. Morrison LJ, Verbeek PR, McDonald AC, Sawadsky BV, Cook DJ. Mortality and prehospital thrombolysis for acute myocardial infarction: a meta-analysis. JAMA. 2000;283:26862692.
99. Dickstein K, Kjekshus J; OPTIMAAL Steering Committee of the OPTIMAAL Study Group. Effects of losartan and captopril on mortality and morbidity in high-risk patients after acute myocardial infarction: the OPTIMAAL randomised trial. Optimal Trial in Myocardial Infarction with Angiotensin II Antagonist Losartan. Lancet. 2002;360:752760.
100. Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Kber L, Maggioni AP, Solomon SD, Swedberg K, Van de Werf F, White H, Leimberger JD, Henis M, Edwards S, Zelenkofske S, Sellers MA, Califf RM; Valsartan in Acute Myocardial Infarction Trial Investigators. Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both. N Engl J Med. 2003;349:18931906. doi: 10.1056/NEJMoa032292.
101. Krumholz HM, Anderson JL, Bachelder BL, Fesmire FM, Fihn SD, Foody JM, Ho PM, Kosiborod MN, Masoudi FA, Nallamothu BK. ACC/AHA 2008 performance measures for adults with ST-elevation and non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Performance Measures for ST-Elevation and Non-ST-Elevation Myocardial Infarction). Circulation. 2008;118:25962648. doi: 10.1161/CIRCULATIONAHA.108.1911099.
102. Han JH, Chandra A, Mulgund J, Roe MT, Peterson ED, Szczech LA, Patel U, Ohman EM, Lindsell CJ, Gibler WB. Chronic kidney disease in patients with non-ST-segment elevation acute coronary syndromes. Am J Med. 2006;119:248254. doi: 10.1016/j.amjmed.2005.08.057.
103. Reddan DN, Szczech L, Bhapkar MV, Moliterno DJ, Califf RM, Ohman EM, Berger PB, Hochman JS, Van de Werf F, Harrington RA, Newby LK. Renal function, concomitant medication use and outcomes follow-ing acute coronary syndromes. Nephrol Dial Transplant. 2005;20:21052112. doi: 10.1093/ndt/gfh981.
104. Roy P, Bouchard J, Amyot R, Madore F. Prescription patterns of pharma-cological agents for left ventricular systolic dysfunction among hemo-dialysis patients. Am J Kidney Dis. 2006;48:645651. doi: 10.1053/j.ajkd.2006.06.006.
105. El-Menyar A, Zubaid M, Sulaiman K, Singh R, Al Thani H, Akbar M, Bulbanat B, Al-Hamdan R, Almahmmed W, Al Suwaidi J. In-hospital major clinical outcomes in patients with chronic renal insufficiency presenting with acute coronary syndrome: data from a registry of 8176 patients. Mayo Clin Proc. 2010;85:332340. doi: 10.4065/mcp.2009.0513.
106. Winkelmayer WC, Levin R, Setoguchi S. Associations of kidney func-tion with cardiovascular medication use after myocardial infarction. Clin J Am Soc Nephrol. 2008;3:14151422. doi: 10.2215/CJN.02010408.
107. Winkelmayer WC, Charytan DM, Brookhart MA, Levin R, Solomon DH, Avorn J. Kidney function and use of recommended medications after myocardial infarction in elderly patients. Clin J Am Soc Nephrol. 2006;1:796801. doi: 10.2215/CJN.00150106.
108. Ahmed A, Centor RM, Weaver MT, Perry GJ. A propensity score analysis of the impact of angiotensin-converting enzyme inhibitors on long-term survival of older adults with heart failure and perceived contraindications. Am Heart J. 2005;149:737743. doi: 10.1016/j.ahj.2004.06.030.
109. Ponikowski P, Ronco C, Anker SD. Cardiorenal syndromes: recom-mendations from clinical practice guidelines: the cardiologists view. Contrib Nephrol. 2010;165:145152. doi: 10.1159/000313753.
110. Ronco C, McCullough P, Anker SD, Anand I, Aspromonte N, Bagshaw SM, Bellomo R, Berl T, Bobek I, Cruz DN, Daliento L, Davenport A, Haapio M, Hillege H, House AA, Katz N, Maisel A, Mankad S, Zanco P, Mebazaa A, Palazzuoli A, Ronco F, Shaw A, Sheinfeld G, Soni S, Vescovo G, Zamperetti N, Ponikowski P; Acute Dialysis Quality Initiative (ADQI) Consensus Group. Cardio-renal syndromes: report
by guest on March 22, 2015http://circ.ahajournals.org/Downloaded from
-
Washam et al Pharmacotherapy in CKD Patients With ACS 27
from the Consensus Conference of the Acute Dialysis Quality Initiative. Eur Heart J. 2010;31:703711. doi: 10.1093/eurheartj/ehp507.
111. Bakris GL, Weir MR. Angiotensin-converting enzyme inhibitor- associated elevations in serum creatinine: is this a cause for concern? Arch Intern Med. 2000;160:685693.
112. Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal syndrome. J Am Coll Cardiol. 2008;52:15271539. doi: 10.1016/j.jacc.2008.07.051.
113. Garthwaite E, Bhandari S. The effects of angiotensin converting enzyme inhibitors on potassium homeostasis in dialysis patients with and without residual renal function. Artif Organs. 2009;33:641647. doi: 10.1111/j.1525-1594.2009.00790.x.
114. Knoll GA, Sahgal A, Nair RC, Graham J, van Walraven C, Burns KD. Renin-angiotensin system blockade and the risk of hyperkalemia in chronic hemodialysis patients. Am J Med. 2002;112:110114.
115. Han SW, Won YW, Yi JH, Kim HJ. No impact of hyperkalaemia with renin-angiotensin system blockades in maintenance haemodialysis patients. Nephrol Dial Transplant. 2007;22:11501155. doi: 10.1093/ndt/gfl752.
116. Zannad F, Kessler M, Lehert P, Grnfeld JP, Thuilliez C, Leizorovicz A, Lechat P. Prevention of cardiovascular events in end-stage renal disease: results of a randomized trial of fosinopril and implications for future studies. Kidney Int. 2006;70:13181324. doi: 10.1038/sj.ki.5001657.
117. Berger WG, Erly WK, Krupinski EA, Standen JR, Stern RG. The soli-tary pulmonary nodule on chest radiography: can we really tell if the nodule is calcified? AJR Am J Roentgenol. 2001;176:201204. doi: 10.2214/ajr.176.1.1760201.
118. Frances CD, Noguchi H, Massie BM, Browner WS, McClellan M. Are we inhibited? Renal insufficiency should not preclude the use of ACE inhibitors for patients with myocardial infarction and depressed left ven-tricular function. Arch Intern Med. 2000;160:26452650.
119. Hillege HL, van Gilst WH, van Veldhuisen DJ, Navis G, Grobbee DE, de Graeff PA, de Zeeuw D; CATS Randomized Trial. Accelerated decline and prognostic impact of renal function after myocardial infarction and the benefits of ACE inhibition: the CATS randomized trial. Eur Heart J. 2003;24:412420.
120. Krause MW, Massing M, Kshirsagar A, Rosamond W, Simpson RJ Jr. Combination therapy improves survival after acute myocardial infarction in the elderly with chronic kidney disease. Ren Fail. 2004;26:715725.
121. Tokmakova MP, Skali H, Kenchaiah S, Braunwald E, Rouleau JL, Packer M, Chertow GM, Moy LA, Pfeffer MA, Solomon SD. Chronic kidney disease, cardiovascular risk, and response to angiotensin-con-verting enzyme inhibition after myocardial infarction: the Survival And Ventricular Enlargement (SAVE) study. Circulation. 2004;110:36673673. doi: 10.1161/01.CIR.0000149806.01354.BF.
122. Shlipak MG, Browner WS, Noguchi H, Massie B, Frances CD, McClellan M. Comparison of the effects of angiotensin converting-enzyme inhibitors and beta blockers on survival in elderly patients with reduced left ventricular function after myocardial infarction. Am J Med. 2001;110:425433.
123. Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, Bittman R, Hurley S, Kleiman J, Gatlin M; Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348:13091321. doi: 10.1056/NEJMoa030207.
124. Juurlink DN, Mamdani MM, Lee DS, Kopp A, Austin PC, Laupacis A, Redelmeier DA. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004;351:543551. doi: 10.1056/NEJMoa040135.
125. Rossignol P, Cleland JG, Bhandari S, Tala S, Gustafsson F, Fay R, Lamiral Z, Dobre D, Pitt B, Zannad F. Determinants and conse-quences of renal function variations with aldosterone blocker therapy in heart failure patients after myocardial infarction: insights from the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study. Circulation. 2012;125:271279. doi: 10.1161/CIRCULATIONAHA.111.028282.
126. Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV, Hill KA, Pfeffer MA, Skene AM; Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 Investigators. Intensive versus moderate lipid
lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:14951504. doi: 10.1056/NEJMoa040583.
127. de Lemos JA, Blazing MA, Wiviott SD, Lewis EF, Fox KA, White HD, Rouleau JL, Pedersen TR, Gardner LH, Mukherjee R, Ramsey KE, Palmisano J, Bilheimer DW, Pfeffer MA, Califf RM, Braunwald E; for the A to Z Investigators. Early intensive vs a delayed conserva-tive simvastatin strategy in patients with acute coronary syndromes: phase Z of the A to Z trial. JAMA. 2004;292:13071316. doi: 10.1001/jama.292.11.1307.
128. Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano M, Kasiske B, Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U, Ophascharoensuk V, Fellstrm B, Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Grnhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham M, Majoni W, Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, Simpson D, Sleight P, Young A, Collins R; SHARP Investigators. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet. 2011;377:21812192. doi: 10.1016/S0140-6736(11)60739-3.
129. Fellstrm BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, Chae DW, Chevaile A, Cobbe SM, Grnhagen-Riska C, De Lima JJ, Lins R, Mayer G, McMahon AW, Parving HH, Remuzzi G, Samuelsson O, Sonkodi S, Sci D, Sleymanlar G, Tsakiris D, Tesar V, Todorov V, Wiecek A, Wthrich RP, Gottlow M, Johnsson E, Zannad F; AURORA Study Group. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med. 2009;360:13951407. doi: 10.1056/NEJMoa0810177.
130. Holdaas H, Fellstrm B, Jardine AG, Holme I, Nyberg G, Fauchald P, Grnhagen-Riska C, Madsen S, Neumayer HH, Cole E, Maes B, Ambhl P, Olsson AG, Hartmann A, Solbu DO, Pedersen TR; Assessment of LEscol in Renal Transplantation (ALERT) Study Investigators. Effect of fluvastatin on cardiac outcomes in renal transplant recipients: a mul-ticentre, randomised, placebo-controlled trial. Lancet. 2003;361:20242031. doi: 10.1016/S0140-6736(03)13638-0.
131. Wanner C, Krane V, Mrz W, Olschewski M, Mann JF, Ruf G, Ritz E; German Diabetes and Dialysis Study Investigators. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N Engl J Med. 2005;353:238248. doi: 10.1056/NEJMoa043545.
132. Lim SY, Bae EH, Choi JS, Kim CS, Park JW, Ma SK, Jeong MH, Kim SW; Korea Acute Myocardial Infarction Registry Investigators. Effect on short- and long-term major adverse cardiac events of statin treatment in patients with acute myocardial infarction and renal dysfunction. Am J Cardiol. 2012;109:14251430. doi: 10.1016/j.amjcard.2012.01.351.
133. Szummer K, Lundman P, Jacobson SH, Schn S, Lindbck J, Stenestrand U, Wallentin L, Jernberg T. Association between statin treatment and outcome in relation to renal function in survivors of myocardial infarc-tion. Kidney Int. 2011;79:9971004. doi: 10.1038/ki.2010.524.
134. Shibui T, Nakagomi A, Kusama Y, Atarashi H, Mizuno K. Impact of statin therapy on renal function and long-term prognosis in acute coronary syndrome patients with chronic kidney disease. Int Heart J. 2010;51:312318.
135. Tonelli M, Moy L, Sacks FM, Kiberd B, Curhan G; Cholesterol and Recurrent Events (CARE) Trial Investigators. Pravastatin for secondary prevention of cardiovascular events in persons with mild chronic renal insufficiency. Ann Intern Med. 2003;138:98104.
136. McClure DL, Valuck RJ, Glanz M, Murphy JR, Hokanson JE. Statin and statin-fibrate use was significantly associated with increased myositis risk in a managed care population. J Clin Epidemiol. 2007;60:812818. doi: 10.1016/j.jclinepi.2006.11.006.
137. US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER). Guidance for industry: pharmacokinetics in patients with impaired renal function: study design, data analysis, and impact on dosing and label-ing. Silver Spring, MD: US Department of Health and Human Services; March 2010. http://www.fda.gov/downloads/Drugs/Guidances/UCM204959.pdf. Accessed December 5, 2014.
KEY WORDS: AHA Scientific Statements acute coronary syndrome chronic kidney disease kidney disease pharmacotherapy
by guest on March 22, 2015http://circ.ahajournals.org/Downloaded from
-
Henry, Navin K. Kapur, Jessica L. Mega, Venu Menon, Robert L. Page II and L. Kristin NewbyJeffrey B. Washam, Charles A. Herzog, Amber L. Beitelshees, Mauricio G. Cohen, Timothy D.
Syndrome: A Scientific Statement From the American Heart AssociationPharmacotherapy in Chronic Kidney Disease Patients Presenting With Acute Coronary
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online February 23, 2015;Circulation.
http://circ.ahajournals.org/content/early/2015/02/23/CIR.0000000000000183.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in theclick Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on March 22, 2015http://circ.ahajournals.org/Downloaded from