CKD presentation
33
CKD for GPs Dr Toni Munno GP King Street Surgery, Kempston
Transcript of CKD presentation

CKD for GPs
Dr Toni Munno
GP King Street Surgery, Kempston

What does the ‘K’
stand for ??
Kardiovascular risk!


100
90
80
70
60
50
40
30
20
10
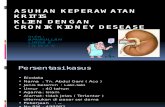
30-59 = CKD 3
15-29 = CKD 4
<15 or RRT = CKD 5
60-90 & abnormality = CKD 2
>90 & abnormality = CKD 1
eGFR & CKD

How measure (e)GFR
Clever lab things etc
Formula = MDRD
creatinine, age, sex, race (black or other)
tables
Online calcFrom lab




100
90
80
70
60
50
40
30
20
10
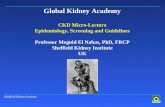
30-59 = CKD 3
15-29 = CKD 4
<15 or RRT = CKD 5
60-90 & abnormality = CKD 2
>90 & abnormality = CKD 1
prevalence
3.3%
3.0%
4.3%
0.2%
0.2%

Prevalence 2006/7
CKDNational prev 2.24%
Local prev 1.51%
Highest in Bedford4.75%
lowest in Bedford0.07%
x67
Eg list size 6000= 285 CKD pts
Eg list size 6000= 4 CKD pts
Work v. points!

Why bother?
x30 – 60 higher all cause mortality x20 more likely to die from CVD than
progress to ESRF
10,000 pts
500 have CKD 3-5(20 = stage 410 = stage 5)
90% have BP
30% have DM
40% have Vasc dis

http://www.rcplondon.ac.uk/pubs/books/CKD/CKDfullGuide.pdf


Step 1. Find them

Screen..contd

Step 2. Make the diagnosis
2 readings three months apart Use the right READ Codes

Step 3. sort them out!
Who do I need to refer?
Need to know: at least
- Blood tests- Urine examination- BP

Referal on basis eGFR
5
4
3
1, 2
4, 5 ref
3 +/-ref

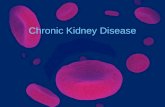
Referal for other reasons…

Urine examination+ve for blood or protein MSU
Exclude infection
+ve for protein(more than a trace)
+ve for blood
Do PCR
>100
45-100
Ref Renal clinic
mAcro mIcromIcro
& protein
Urology2WR
mIcro NO protein
>50 <50
Neg? if egfr<60

Step 4. review medication

Step 5. sort out BP
TargetsWith protein 120/75
(threshold to start Rx is 130/80 if PCR >100, 140/90 otherwise)
Without protein 130/80QOF 140/85 !
Refer if >150/90 and on 3 antiBP rx
Remember 90% will have hypertension

Step 6. should they be on ACEi ?
Yes – if proteinuria Yes – if no protein, as part combination Rx to
get to target Yes – if DM and microalbuminura
No – if no protein and already have good BP control in which case remember Read codes:
8I64 – ACE not indicated
8I6C - A2RB not indicated
BUT don’t exempt them from whole CKD domain!!


Monitoring ACEi
Check creatinine (eGFR) and K Before start medcn 2 weeks after starting 2 weeks after any dose change
Watch for creatinine increase >20%, eGFR decrease >15%If so: ‘repeat creatinine, check K, and refer for
specialist opinion on whether to stop rx or to investigate for renal artery stenosis.’

Step 7. minimize cardiovascular risk
Lifestyle: smoke, wt, excse, alc, salt BP etc
‘If 10 yr CVD risk >20% consider’: Aspirin if BP < 150/90 Lipid lowering drug therapy

Step 8. follow-up
Rem. flu & pneumo jabs
Stage 3 chronic disease model Check eGFR 6mthly
(12mthly if stable, ie < 2ml/min change over 6m) Annual check Hb, K, Ca, phosp BP
Stage 4,5 ?shared care Check eGFR 3mthly
(6mthly if stable CKD4) ? 3mthly bloods,



QOF issues
Prevalence! Role of ACEi Appropriate use exemption codes
‘unsuitable/dissent’ , max tol, drugs
Prevalence of co-existing hypertension ?likely changes next year


Resources:
everything you need to know about CKD, eGFR , treatment and referral pathways can be found online:
www.renal.org
There is a very good recent update (April 2007) about CKD and QOF from NHS Employers and the BMA
FAQs for Chronic Kidney Disease (CKD). This document can be accessed at: -
www.pcc.nhs.uk/77.php