CKD & HYPERTENSION Qs & As David Makanjuola Renal Unit St. Helier.
86
CKD & HYPERTENSION Qs & As David Makanjuola Renal Unit St. Helier
-
Upload
adam-bishop -
Category
Documents
-
view
219 -
download
1
Transcript of CKD & HYPERTENSION Qs & As David Makanjuola Renal Unit St. Helier.

CKD & HYPERTENSIONQs & As
David MakanjuolaRenal UnitSt. Helier

COMMON CONCEPTIONS OF RENAL MEDICINE
• Renal disease is RARE
• Renal disease is COMPLEX
• Nephrologists are...

All generalisations are dangerous.
Even this one.
Alexandre Dumas

Generalisations, even this one…..
Dangerous they are.

SCENARIO 1• 1 – 62 year old caucasian male with CKD stage 3.
Blood pressure is 160/95mmHg on 24 hour ABPM. The urine total protein to creatinine ratio is 8.3mg/mmol (normal range <15).
• What antihypertensive agent would you prescribe and what target blood pressure would you aim for?
Anti-hypertensive agent• ACE inhibitor• Calcium channel blocker• Diuretic• Alpha blocker• Beta blocker
TARGET BP• 140/90• 130/80• 125/75

SCENARIO 1• 1 – 62 year old caucasian male with CKD stage 3.
Blood pressure is 160/95mmHg on 24 hour ABPM. The urine total protein to creatinine ratio is 8.3mg/mmol (normal range <15).
• What antihypertensive agent would you prescribe?
Anti-hypertensive agent• ACE inhibitor• Calcium channel blocker• Diuretic• Alpha blocker• Beta blocker


SCENARIO 1• 1 – 62 year old caucasian male with CKD stage 3.
Blood pressure is 160/95mmHg on 24 hour ABPM. The urine total protein to creatinine ratio is 8.3mg/mmol (normal range <15).
• What target blood pressure would you aim for?
TARGET BP• 140/90• 130/80• 125/75

SCENARIO 1• What target blood pressure would you aim for?
For most patients a target of ≤ 140 mm Hg systolicblood pressure and ≤ 85 mm Hg diastolic bloodpressure is recommended. For patients with diabetes, renal impairment or established cardiovascular disease a lower target of ≤ 130/80 mm Hg isrecommended.

SCENARIO 1• 1 – 62 year old caucasian male with CKD stage 3.
Blood pressure is 160/95mmHg on 24 hour ABPM. The urine total protein to creatinine ratio is 8.3mg/mmol (normal range <15).
• What antihypertensive agent would you prescribe and what target blood pressure would you aim for?
• ACE inhibitor• Calcium channel blocker• Diuretic• Alpha blocker• Beta blocker
• 140/90• 130/80• 125/75

SCENARIO 2• A 62 year old man, originally from Jamaica
presents on the acute take with chest pain.
• There is no history of cardiovascular disease. He has type 2 diabetes mellitus and takes Metformin 1g bd as well as Gliclazide 80mg bd.
• His HbA1c is 8.4%. The ECG is normal, Troponin T is not elevated and his BP is 168/90mmHg.

SCENARIO 2
• When seen at the GP practice, his BP remains elevated at 170/95mmHg.
• It is 165/90mmHg when checked 10 minutes later, but he says it is always elevated when it is checked.

SCENARIO 2
• He is on no anti-hypertensive treatment.• What treatment would you initiate and why?
• ACEi• ACEi and angiotensin 2 receptor blocker• ACEi and calcium channel blocker• Thiazide

HOPE study (2000) inclusion criteria
• At least 55 years old • PLUS• history of coronary artery disease, • stroke, • peripheral vascular disease, • or diabetes plus at least one other cardiovascular
risk factor (hypertension, elevated total cholesterol levels, low high-density lipoprotein cholesterol levels, cigarette smoking, or documented microalbuminuria).

HOPE study

HOPE study - conclusion
• Ramipril reduces the rates of:– death– myocardial infarction– Stroke– revascularization– cardiac arrest– heart failure– complications related to diabetes– and new cases of diabetes in a broad spectrum of high-risk
patients.

HOPE study - conclusion
• Treating 1000 patients with Ramipril for four years prevents about 150 events in approximately 70 patients.

SCENARIO 2
• A 62 year old man, originally from Jamaica presents on the acute take with chest pain.

AASK trial (2002)• African American Study of Kidney Disease and
Hypertension
• Objective:• To compare the effects of 2 levels of blood
pressure (BP) control and 3 antihypertensive drug classes on glomerular filtration rate (GFR) decline in hypertension.
n = 1,094 black Americans

Blood pressure goal intervention
Drug intervention
Usual BPMAP 102-107 (141/85)
Low BPMAP < 92 (128/78)
Ramipril Metoprolol Amlodipine

AASK trial
BP goal intervention Drug interventionLower Usual Ramipril Metoprolol Amlodipine
AGE 54.5 54.7 54.4 54.5 54.9GFR 46 45.3 45.4 45.8 45.8

AASK trial• Change in Proteinuria• Proteinuria increased by 7% in the usual BP group and
decreased by 17% in the lower BP group during the first 6 months.
• Proteinuria increased by 58% for the Amlodipine group and declined by 14% in the Metoprolol group between baseline and 6 months (P.001).
• Follow-up proteinuria was slightly lower in the Ramipril than the Metoprolol group but not significantly (P=.06 for the comparison of total change over 4 years).

AASK trial
Effect on ESRD/ declining GFR – blood pressure arm
• There were no significant differences between the BP groups in:– the combined kidney end points of a declining GFR event or ESRD
– the combined hard clinical end points of ESRD or death
– or ESRD alone.

AASK trial
Effect on ESRD/ declining GFR – medication arm
• Significant benefits of Ramipril vs Metoprolol and Amlodipine on the main clinical composite outcome and the results of other secondary analyses suggest that:
Ramipril slows hypertensive kidney disease progression compared with the other 2 regimens.

AASK trial
• “…angiotensin- converting enzyme inhibitors should be considered as first line therapy over beta-blockers and dihydropyridine calcium channel blockers in these patients.”
• Moreover, beta-blockers may be more effective than dihydropyridine calcium channel blockers in slowing progression among patients with proteinuria.

AASK trial
• Treatment of study participants to a lower than usual mean BP of 128/78 mmHg did not significantly reduce either the mean rate of GFR decline or the risk of the clinical composite outcome compared with usual BP goal with a mean achieved BP of 141/85.

AASK TRIAL
BP goal intervention Drug interventionLower Usual Ramipril Metoprolol Amlodipine
AGE 54.5 54.7 54.4 54.5 54.9GFR 46 45.3 45.4 45.8 45.8
Diabetics excluded

SCENARIO 2
• He is on no anti-hypertensive treatment.• What treatment would you initiate and why?
• ACEi• ACEi and angiotensin 2 receptor blocker• ACEi and calcium channel blocker• Thiazide

SCENARIO 3
• 3 – 58 year old caucasian female with T2DM, CKD 3b and proteinuria of 2g/day.
• BP is 160/90, she is on an ACEi and a beta blocker. She has gout, and so had to come off diuretics. She also developed significant ankle swelling with calcium channel blockers.
• Would you add in an angiotensin receptor blocker?

ARBs in diabetics with renal disease

Benefit of Angiotensin Receptor Blockers in Diabetes:Important Findings of 3 Major Clinical Trials
• RENAAL (2001)– The angiotensin receptor blocker losartan compared to placebo
reduced the risk of diabetic nephropathy developing to renal failure
• IRMA II (2001)– Higher doses of the angiotensin receptor blocker irbesartan
reduced the risk of progression of renal insufficiency • IDNT (2001)
– The angiotensin receptor blocker irbesartan compared to the calcium channel blocker amlodipine provided better renal protection in hypertensive type 2 diabetics, reducing the chance of diabetic nephropathy developing to renal failure

Benefit of Angiotensin Receptor Blockers in Diabetes:Important Findings of 3 Major Clinical Trials
• RENAAL (2001)– The angiotensin receptor blocker losartan compared to placebo
reduced the risk of diabetic nephropathy developing to renal failure
• IRMA II (2001)– Higher doses of the angiotensin receptor blocker irbesartan
reduced the risk of progression of renal insufficiency • IDNT (2001)
– The angiotensin receptor blocker irbesartan compared to the calcium channel blocker amlodipine provided better renal protection in hypertensive type 2 diabetics, reducing the chance of diabetic nephropathy developing to renal failure

Benefit of Angiotensin Receptor Blockers in Diabetes:Important Findings of 3 Major Clinical Trials
• RENAAL (2001)– The angiotensin receptor blocker losartan compared to placebo
reduced the risk of diabetic nephropathy developing to renal failure
• IRMA II (2001)– Higher doses of the angiotensin receptor blocker irbesartan
reduced the risk of progression of renal insufficiency • IDNT (2001)
– The angiotensin receptor blocker irbesartan compared to the calcium channel blocker amlodipine provided better renal protection in hypertensive type 2 diabetics, reducing the chance of diabetic nephropathy developing to renal failure

Dual blockade

CHARM Added: Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity - Added
Purpose
To determine whether addition of the angiotensin II receptor blocker candesartan is beneficial in patients with chronic heart failure (CHF) who are taking angiotensin converting enzyme (ACE) inhibitors
ReferenceMcMurray JJV, Östergren J, Swedberg K, et al. for the CHARM Investigators and Committees. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trial. Lancet 2003;362:767–71.

CHARM Added: Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity - Added
- SUMMARY -
In patients with symptomatic CHF who were taking ACE inhibitors, candesartan reduced:
• Cardiovascular death and hospitalization for CHF• Secondary outcomes that combined these with MI, stroke and
coronary revascularization procedures
Benefit was independent of concurrent beta-blocker therapy and ACE inhibitor dose

CO-OPERATE TRIAL - 2003LOSARTAN
+PLACEBO
TRANDOLAPRIL+
PLACEBO
LOSARTAN+
TRANDOLAPRIL
LOSARTAN TRANDOLAPRIL COMBINATIONAGE 44.8 45.9 45.2CREATININE 265 267 271GFR 38.4 37.9 37.524h urine protein(g)
2.4 2.5 2.5
Systolic BP 130 129 130Diastolic BP 74 75 75
End points – Doubling of serum creatinine or end-stage renal disease

CO-OPERATE TRIAL
Significant reduction of proteinuria in combination therapy group, in spite of similar blood pressures.

CO-OPERATE TRIAL
LT
C
Fewer patients in combination therapy arm reached end-stage renal failure.

CO-OPERATE TRIAL – the aftermath• ACE Inhibition versus Angiotensin Receptor
Blockade: Which Is Better for Renal and Cardiovascular Protection?
• Actually, in most patients, achieving maximal renal and cardiovascular protection requires a multidrug regimen, usually including several antihypertensives.
• Within this approach, full dose titration of either RAS blocker followed by add-on with the second drug is more important than the choice of the initial drug.
J Am Soc Nephrol 15: S64–S70, 2004

CO-OPERATE TRIAL – the aftermath
• Lancet retracts COOPERATE trial of dual RAS inhibition and spanks lead author for serious misconduct.

CO-OPERATE TRIAL – the aftermath
• After an initial letter of concern, the Lancet has retracted the paper after the results of an academic investigation indicated serious concerns surrounding this publication.
• These include that:• the trial had not been approved by the hospital ethics committee• proper consent from patients had not been obtained• the involvement of a statistician could not be verified• the trial was not a double-blind study• and based on a sample of the medical records the authenticity of
the data could not be proved.

Adverse Effects of Combination Angiotensin IIReceptor Blockers Plus Angiotensin-Converting
Enzyme Inhibitors for Left Ventricular DysfunctionA Quantitative Review of Data From Randomized Clinical Trials
Arch Intern Med. 2007;167(18):1930-1936
• When applied to an analysis of benefit vs risks of adverse effects of combination ARB plus ACE inhibitor therapy, our findings suggest that per 1000 patients,
– 25 will discontinue this medication due to adverse effects
– 17 will experience renal dysfunction
– 8 will develop hyperkalemia
– 36 will experience symptomatic hypotension.

ONTARGET STUDY - 2008
Telmisartan, Ramipril, or Both in Patients at High Risk for Vascular Events

ONTARGET STUDYRAMIPRIL
+PLACEBO
TELMISARTAN+
PLACEBO
RAMIPRIL+
TELMISARTAN
RAMIPRIL TELMISARTAN COMBINATION
Age 66.4 66.4 66.5
Creatinine 93.5 93.8 93.8
Microalbuminuria (%) 13.1 13.2 13.3
Systolic BP 142 142 142
Diastolic BP 68 68 68
End points – Death from cardiovascular causes, MI, CVA or hospitalisation for heart failure

ONTARGET STUDY
• Surprisingly, despite a reduction in systolic blood pressure of 2 to 3 mm Hg in the combination-therapy group, as compared with the Ramipril group
— a decrease that should have translated into a risk reduction of 4 to 5% —
no significant benefit was seen in the primary outcome among patients receiving the two-drug therapy.

ONTARGET STUDY
• However, combination therapy significantly increased the risk of:– hypotension– syncope– renal dysfunction– and hyperkalaemia– with a trend toward an increased risk of renal dysfunction requiring
dialysis.

ONTARGET STUDY
• Therefore, even though combination therapy had a larger biologic effect (as suggested by greater blood-pressure lowering and changes in potassium), dual blockade did not produce any additional clinical benefit in this population.

ONTARGET STUDY• In conclusion, our data show that in patients who
have vascular disease or high-risk diabetes but do not have heart failure, Telmisartan is an equally effective alternative to Ramipril and is less likely to cause angioedema.

ONTARGET STUDY• There is no additional advantage (and there is some
harm) from the combination of Telmisartan and Ramipril used in full doses in this population, as compared with Ramipril alone.

RAAS
What exactly does the AT2 receptor mediate?

RAASAT2 receptorThe AT2 receptor shares only about 32% amino acid sequence homology with the AT1 receptor.
It is highly expressed in fetal kidney and intestine.
In adults, it is highly expressed in the myometrium with lower levels in adrenal gland and fallopian tube.

RAAS•The AT2 receptor remains enigmatic and controversial.
•Activation of AT2 receptors causes vasodilatation by generation of nitric oxide.
•Other effects mediated by the AT2 receptor are suggested to include:
•inhibition of cell growth •foetal tissue development •modulation of extracellular matrix •neuronal regeneration •Apoptosis•cellular differentiation

RAAS
Ying-Yang hypothesis proposed in which ATI and AT2 have opposite
functions.
But is everything mediated by the AT2 receptor indeed beneficial?

ACE-ARB and NEOPLASIAAngiotensin-receptor blockade and risk of cancer: meta-analysis of randomised controlled trialsLancet Oncol 2010; 11: 627–36
• This meta-analysis of randomised controlled trials suggests that ARBs are associated with a modestly increased risk of new cancer diagnosis.
• Given the limited data, it is not possible to draw conclusions about the exact risk of cancer associated with each particular drug.
• These findings warrant further investigation.

RAASThe mechanism for the possible increase in the occurrence of new cancer cases associated with ARBs is uncertain.
Experimental studies using cancer cell lines and mouse models have implicated the renin-angiotensin system in the regulation of cell proliferation, tumour growth, angiogenesis, and metastasis.

RAASEvidence shows that both AT1R blockade with an ARB (which is associated with unopposed AT2R stimulation) and direct stimulation of AT2R are capable of stimulating tumour angiogenesis in vivo.
However, the relevance of these observations in human malignancy is largely unknown.

RAASAT3 and AT4
Other poorly characterized subtypes include the AT3 and AT4 receptors.
The AT4 receptor is activated by the angiotensin II metabolite angiotensin IV, and may play a role in regulation of the CNS extracellular matrix.

SCENARIO 3So, would you add in an angiotensin receptor
blocker?DO YOU FEEL LUCKY?

Angiotensin Receptor Blockers and the Risk of Cancer Statement from the British Hypertension Society
July 2010
Our recommendation is that until more comprehensive analyses have been completed, this single study alone is not sufficient to warrant any change in current clinical recommendations of practice regarding the use of ARBs.

SCENARIO 4• An 88 year old woman presented with a blood pressure of
200/80mmHg, minor proteinuria and a history of falls.
• Her BP control has improved somewhat on an ACE inhibitor, a calcium channel blocker and a diuretic, and is now 160/65 on average.
• She was also on Doxazosin, but her stress incontinence worsened significantly, so Doxazosin was discontinued.
• What would you do with regard to further management of her hypertension?

The Systolic Hypertension in the Elderly Program, 1991

SHEP trial
The objective of the stepped-care treatment program was to use the minimal amount of medication to maintain SBP at or below the
goal.

SHEP trial
• For individuals with SBPs greater than 180 mmHg, the goal was a reduction to less than 160 mm Hg.
• For those with SBPs between 160 and 179 mm Hg, the goal was a reduction of at least 20 mm Hg.

SHEP trial designStep 1 –
Chlorthalidone 12.5 mg/d, or placebo.
Target BP attained?
Double the drug or placebo dose
Yes No
Continue
Target BP attained?
Yes No
Continue Go to step 2

SHEP trial designStep 1 –
Chlorthalidone 12.5 mg/d, or placebo.
Step 2 – Atenolol 25 mg/d, or placebo.
(When atenolol was contraindicated, reserpine, 0.05 mg/d, or placebo could be substituted).
Target BP attained?
Double the drug or placebo dose
Yes No
Continue
Target BP attained?
Yes No
Continue Go to step 2
Target BP attained?
Yes No
Continue
Target BP attained?
Yes No
Continue Continue
Double the drug or placebo dose

Bloo
d pr
essu
re (m
mH
g)
0 12 36 60Months of follow-up
SHEPAverage Blood Pressure During Follow-up
24 4850
65
80
95
110
125
140
155
170
185
200
SHEP=Systolic Hypertension in the Elderly Program SHEP Research Group. JAMA. 1991;265:3255-3264.Copyright ©1991, American Medical Association.

0123456789
10
Cum
ulati
ve s
trok
e ra
te
per 1
00 p
erso
ns
0 12 36 60Months of follow-up
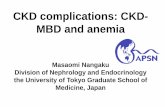
SHEPCumulative Stroke Rate
24 48 72
P=0.0003
Placebo(n=2,371)
Active Rx (n=2,365)
SHEP=Systolic Hypertension in the Elderly Program SHEP Research Group. JAMA. 1991;265:3255-3264.Copyright ©1991, American Medical Association.

SHEPConclusions
SHEP was the first clinical trial to demonstrate that reduction of blood pressure in patients with isolated systolic hypertension reduced cardiovascular (CV) mortality
The relative risk of stroke was reduced by 36% with therapy compared to placebo (P=0.0003)
The 5-year absolute benefits were a reduction in 30 strokes and 55 major CV disease events per 1,000 persons
SHEP Research Group. JAMA. 1991;265:3255-3264.
SHEP=Systolic Hypertension in the Elderly Program

SHEP demographics
CHARACTERISTIC ACTIVE TREATMENT
GROUP
PLACEBO GROUP
AVERAGE AGE (SD)
71.6 (6.7) 71.5 (6.7)
% Aged 60-69 years
41.1 41.8
% Aged 70-79 years
44.9 44.7
% Aged > 80 years
14 13.4

SCENARIO 4• What would you do with regard to further
management of her hypertension?

SCENARIO 4• What would you do with regard to further
management of her hypertension?
• I would accept the current level of improved blood pressure, because with the increased risk of falls, I might need to have the orthopaedic team on speed dial.

The problem with translating clinical trials into practice.

When a poet’s work is translated to another language, poetry is what is
lost in the translation.
Jorge Luis Borges

When a clinical trial is translated into practice, the reproducibility of the trial results is what is lost in the
translation.

THANK YOU

Syst-Eur Conclusions
• Older men and women (average age 70 yrs) with isolated systolic hypertension who received active treatment with a dihydropyridine calcium channel blocker experienced fewer strokes and cardiovascular disease (CVD) events than those receiving placebo.
• Treatment of 1,000 patients for 5 years with this type of regimen could prevent 29 strokes or 53 major CVD endpoints.
Staessen JA, et al. Lancet. 1997;350:757-764.
Syst-Eur=Systolic Hypertension in Europe Trial

0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
Rela
tive
risk
(95%
CI)
Stroke CHD
Active Therapy vs. Placebo
CHF Death
0.630.63
0.460.46
0.680.68
0.870.87
CVD
0.750.75
SHEPCardiovascular Disease Endpoints
SHEP Research Group. JAMA. 1991;265:3255-3264.
SHEP=Systolic Hypertension in the Elderly Program
CHD=coronary heart disease; CHF=congestive heart failure; CVD=cardiovascular disease

CHARM Added: Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity - Added
- TRIAL DESIGN -
DesignMulticenter, multinational, randomized, double-blind, placebo-controlled
Patients2548 patients aged >18 years with symptomatic CHF (NYHA class II–IV), who had left ventricular ejection fraction <40% and were receiving ACE inhibitors
Follow up and primary endpointPrimary endpoint: cardiovascular death or hospital admission for CHF. Median 41 months follow up.
TreatmentPlacebo or candesartan titrated to 32 mg once daily

CHARM Added: Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity - Added
- TRIAL DESIGN continued-
Age (years)a
Male
NYHA class:
Systolic BP (mmHg)a
Heart failure cause:
IschemicIdiopathicHypertensive
IIIIIIV
History
MIDiabetes mellitusHypertension
Medications
ACE inhibitorDiureticBeta-blockerSpironolactoneAspirin
Baseline characteristics (%)
64.1
125.6
79
24734
63266
Placebo(n=1272)
64.0
124.7
79
24733
62277
Candesartan(n=1276)
a Mean
553049
10090561752
Placebo(n=1272)
563048
10090551751
Candesartan(n=1276)
McMurray et al. Lancet 2003;362:767–71.

CHARM Added: Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity - Added
- RESULTS -
• Primary outcome of cardiovascular death or hospital admission for CHF significantly reduced in candesartan group compared with placebo (37.9 vs. 42.3%, hazard ratio 0.85, 95% CI 0.75–0.96, P=0.011): each component was reduced significantly
• Secondary outcomes – composites of primary outcome and MI, nonfatal stroke and coronary revascularization – also significantly reduced
• All-cause mortality not significantly reduced (30 vs. 32%, hazard ratio 0.89, 95% CI 0.77–1.02, P=0.086)
• Benefits similar in patients taking beta-blockers and those who were not (P=0.14 for treatment interaction), and regardless of whether recommended dose of ACE inhibitor achieved (P=0.26)
• Permanent discontinuation due to adverse event or laboratory abnormality more frequent with candesartan (24.2 vs. 18.3%, P=0.0003)

CHARM Added: Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity - Added
- RESULTS continued -
P
Cardiovascular death orhospital admission for CHF
0.85 (0.75–0.96) 0.011
Primary and secondary outcomes
483
No.
(37.9)
(%)
Candesartan(n=1276)
538
No.
(42.3)
Cardiovascular death 0.84 (0.72–0.98) 0.029302 (23.7)347 (27.3)Hospital admission for CHF 0.83 (0.71–0.96) 0.014309 (24.2)356 (28.0)
Cardiovascular death, hospitaladmission for CHF, or MI
0.85 (0.76–0.96) 0.010495 (38.8)550 (43.2)
Cardiovascular death, hospitaladmission for CHF, MI,or stroke
0.87 (0.77–0.98) 0.020512 (40.1)559 (43.9)
Cardiovascular death, hospitaladmission for CHF, MI, stroke,or coronary revascularization
0.87 (0.77–0.97) 0.015548 (42.9)596 (46.9)
(%)
Placebo(n=1272) Hazard ratio
(95% CI)
McMurray et al. Lancet 2003;362:767–71.

CHARM Added: Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity - Added
- RESULTS continued -
Cardiovascular death or hospital admission for CHF in relation toconcomitant treatment at baseline
CandesartanNo. of
events/n
Candesartanbetter
Placebobetter
PlaceboNo. of
events/n
β-blocker
YesNo
Recommended doseof ACE inhibitor
YesNo
All patients
223/702260/574
232/643251/633
483/1276
P fortreatmentinteraction
0.14
0.26
274/711264/561
275/648263/624
538/1272
McMurray et al. Lancet 2003;362:767–71.
0.80.6 1.0 1.2

AASK trial
• We do not interpret the apparent lack of an effect of the lower BP goal to slow decline in GFR (and reduce risk for clinical end points) to illustrate that BP lowering is not important for preserving kidney function.
• Our study did not test the hypothesis that treatment vs no treatment of hypertension preserves kidney function.
• Nevertheless, our data suggest that once BP is lowered to a given level, additional risk factors are important in patients with chronic kidney disease resulting from hypertension.

AASK trial
• The AASK is the first outcome trial to demonstrate a renoprotective effect of angiotensin- converting enzyme inhibitor in an African American population.
• We conclude that although BP reduction to levels below current guidelines for cardiovascular risk reduction are achievable, our results do not support additional reduction as a strategy to prevent progression of hypertensive nephrosclerosis.