CKD and risk management : NICE guideline 2008 …...CKD and risk management : NICE guideline...
38
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist [email protected] s ahmed, 2014
Transcript of CKD and risk management : NICE guideline 2008 …...CKD and risk management : NICE guideline...

CKD and risk management : NICE guideline
2008-2014
Shahed Ahmed
Consultant Nephrologist
s ahmed, 2014

Key points :
• Changing parameters of CKD and NICE guidance
• CKD and age related change of GFR
• Nice guidance on lipid management with CKD
• CKD Vs AKI
• Community AKI project
s ahmed, 2014

Defining CKD
• CKD is present when either:
The MDRD-derived estimated glomerular filtration rate (eGFR) is less than 60ml/min on at least two occasions over a period of no less than 90 days
Or,
The urine ACR is >30mg/mmol
(or, PCR is > 50mg/mmol)
s ahmed, 2014

Classification of CKD, based on NICE 2008
Stage of CKD Estimated GFR KIDNEY FUNCTION
Stage 1 >90ml/min with urine abnormality or abnormal renal anatomy
Normal
Stage 2 60-89ml/min with urine abnormality or abnormal renal anatomy
Mild Reduced
Stage 3a 45-59ml/min Mild to moderate reduced
Stage 3b 30-44ml/min Moderate reduced
Stage 2 15-29ml/min Severe reduced
Stage 5 <15ml/min or dialysis dependant Kidney failure
s ahmed, 2014

s ahmed, 2014
WHY CKD is a high risk disease ? CV disease mortality : General Population vs. ESRD Dialysis Patients
Foley RN, et al. Am J Kidney Dis.
1998;32:S112-S119.
0.001
0.01
0.1
1
10
100
25-34 35-44 45-54 55-64 66-74 75-84 >85
GP Male
GP Female
GP Black
GP White
Dialysis Male
Dialysis Female
Dialysis Black
Dialysis White
Age (years)
An
nu
al C
VD
Mo
rtality
(%
)

Prevalence of Chronic Kidney Disease (CKD) Stages by Age Group in NHANES 1988-1994 and 1999-2004
s ahmed, 2014

s ahmed, 2014
CV
events
N Engl J Med. 2004 Sep 23;351(13):1296-305, Go et al, Kaiser Permanente
Northern California

s ahmed, 2014
CKD- However,
The majority of patients with CKD 1-3 do not progress to ESRF.
Their risk of cardiovascular death is higher than their risk of progression.

s ahmed, 2014
Patients with CKD are more likely to die than go onto dialysis
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
No DM /
CKD
DM No
CKD
CKD No
DM
DM and
CKD
Dialysis
Death
ESRD/D
Event Free
Adapted from Collins, Adv Studies in Med, (3C) 2003, Medicare Cohort 1998-99
25% 30% 40%
15% 9%

s ahmed, 2014
In CKD – early identification is essential !
NICE: Chronic kidney disease Early identification and management of chronic kidney
disease in adults in primary and secondary care – Issue date: September 2008
The Challenges: • However, because of a lack of specific symptoms, CKD are often not diagnosed,
or diagnosed late. • 30% of people with advanced CKD disease are referred late, causing increased
mortality and morbidity.
s ahmed, 2014
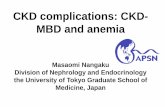
CKD – How we diagnose ? Serum Cr Vs GFR

s ahmed, 2014
eGFR: Practical Implementation Issues
• Apply only to age > 18
(MDRD ages: 18-70)
• Not Validated - AKI
Transplant
Pregnancy
• Ease of use . Good fit with data at lower GFR

s ahmed, 2014
GFR = 170 x [Pcr]-0.999 x [Age]-0.176 x [0.762 female] x [1.180 black race] x [SUN]-0.170 x [Alb]+0.318
Modified Equation 7:
GFR = 186 x [Pcr]-1. 154 x [Age]-0.203 x [0.742 female] x [1.212 black race]
Estimate GFR from Serum
Creatinine:, AS. Levey, et al;
Ann Intern Med.
1999;130:461-470.

s ahmed, 2014
Age & GFR • Functional changes
–Renal plasma flow 10%/decade
– Longitudinal study,
mean reduction CCL 0.75ml/min/yr (92 out 0f 254 no reduction)
• Lindeman, R. D., Tobin, J., and Shock, N. W.
(1985). Longitudinal studies on the rate of decline in renal function with age.Journal of the American Geriatrics Society

NICE CKD 2008: Did we overkill CKD diagnosis ?
s ahmed, 2014
Group in NHANES 1988-1994 and 1999-2004

WHATS NEW NICE CKD 2014
The new and updated areas include:
Classification of CKD and identification of people at risk of CKD complications and progression
The relationship between acute kidney injury and CKD
Self-management of CKD
Pharmacotherapy for CKD.
s ahmed, 2014

Classification of chronic kidney disease
• Classify CKD using a combination of GFR and ACR categories and be aware that:
a. Increased ACR is associated with increased risk of progression
b. Decreased GFR is associated with increased risk of progression
c. Increased ACR and decreased GFR in combination multiply the risk of progression.
s ahmed, 2014

s ahmed, 2014

Identification and investigation of people who have or are at risk of developing CKD
• Consider using eGFR cystatin C to confirm the diagnosis of CKD in people with :an eGFR creatinine of 45–59 ml/min/1.73 m2, sustained for at least 90 days and no proteinuria (albumin:creatinine ratio)ACR less than 3mg/mmol)
s ahmed, 2014
s ahmed, 2014
CKD : aim of Rx
CV risk reduction:
Target BP control Rx of hyperlipidaemia
Control of proteinuria Target primary disease: ex.- good control of diabetes
Specific Rx for CKD

s ahmed, 2014
Blood pressure and progression of CKD
Jafar et al, Ann Intern Med 2003;139:244-252
Ad
just
ed
re
lati
ve r
isk
of
pro
gre
ssio
n t
o C
KD
(9
5%
CI)
Meta-analysis of 11 randomised controlled trials with or without ACEi
1860 patients with non-diabetic kidney disease
Systolic BP (mmHg)
0
0.5
1
1.5
2
2.5
3
3.5
<110 110-119 120-129 130-139 140-159 160+
MEDLINE Database
3.14
2.08
1.83
1.23
1.00
2.48

s ahmed, 2014

s ahmed, 2014
Blood pressure targets
NICE CKD Guidance
• If CKD, blood pressure target: • <140 mmHg SBP (130-139) • < 90 mmHg DBP (80-89)
•If diabetes and CKD or ACR ≥ 70 mg/mmol, blood
pressure target: • < 130 mmHg SBP • < 80 mmHg DBP
NICE Management of CKD: NICE 2008
NICE CKD 2014
Overview: management of CKD in primary care
• Identify those at risk by eGFR and proteinuria measurement
• Explain to people they have the condition and encourage self-management
• Control blood pressure
• manage cardiovascular risk
• Medicine management
s ahmed, 2014

Cont..
Do not offer a combination of renin-angiotensin system antagonists to people with CKD
And do not offer a renin-angiotensin system antagonist to people if pretreatment serum potassium is >5.0mmol/litre
s ahmed, 2014

Key priority:
Promoting self-management of CKD
• BP control: Explain that reducing raised BP is a
key factor in preventing the progression of CKD
• BP monitoring: Advise people to monitor their own BP at home
• Smoking cessation
• Blood sugar control (if they have diabetes) • Diet: To avoid processed, high-salt and high-fat
foods
s ahmed, 2014

Key priority: Assess & control
cardio-vascular risk
• Statins: • Use statins for primary prevention of cardiovascular
disease in same way as in people without CKD • Offer statins for secondary prevention of CVD
irrespective of lipid values
• Offer antiplatelet drugs to people with CKD for
the secondary prevention of CVD (but the risks of bleeding may be increased with multiple antiplatelet drugs)
s ahmed, 2014

NICE guideline: Lipid modification Feb 2014
• prevention of CVD in primary care, use a systematic strategy to identify people aged 40-74 who are likely to be at high risk
• Use the QRISK2 risk assessment tool to assess CVD risk for the primary prevention of CVD (more than 10% , 10 year CVD risk on assessment)
• Offer statin treatment for the primary prevention of CVD with atorvastatin 20 mg.
• Start statin treatment in people with established CVD, type 1 diabetes or type 2 diabetes with atorvastatin 80 mg. s ahmed, 2014

NICE guideline: Lipid modification Feb 2014
63. In people with stage 1 or stage 2 CKD treat as primary prevention and initiate treatment with atorvastatin 20 mg if there is no evidence of CVD and more than 10% CVD risk on assessment with QRISK2. [new 2014] 64. In people with stage 1 or stage 2 CKD and evidence of CVD, start treatment with atorvastatin 20 mg and increase dose if a greater than 40% reduction in non-HDL cholesterol is not achieved. [new 2014] 65. In people with stage 3 CKD start high-intensity statin treatment with atorvastatin 20 mg. Increase the dose if a reduction in non-HDL cholesterol of greater than 40% is not achieved. [new 2014] 66. In people with CKD stage 4 or greater start treatment with atorvastatin 20 mg and agree the use of higher doses with a renal specialist. [new 2014]
s ahmed, 2014

Case
• 32 Year old lady , generally feeling unwell. H/O- HTN, depression
• On Lisinopril 20 mg, Furosemide 40 mg
• INV- S Cr 250/ eGFR 29
• Urine dip – NAD
• BP, HR , RR – normal limit
• Rx:
1. Urgent Renal O/P ref for CKD 4
2. Stop ACEI / repeat U&E , then consider referral
3. Urgent hospital Referral for AKI
s ahmed, 2014

AKI : Background
• Up to 18% of all hospital admissions have AKI
• Inpatient AKI-related mortality is between 25 and 30%
• Between 20 and 30% of cases of AKI are preventable.
Prevention could save up to 12,000 lives each year
• NHS costs related to AKI are between £434 and £620 million per year
s ahmed, 2014

Cost of AKI 23 June 2011 Health Service Journal supplement 1
s ahmed, 2014

e-AKI alert: Early Diagnosis of AKI
s ahmed, 2014

e-AKI alert

Community Acute Kidney Injury (AKI) Guideline
→
→
.
**Discuss with AKI team / on call renal Registrar if required and appropriate
AKI stage 1 AKI stage 3
New Diagnosis of AKI (Stage 1 / Stage 2/ Stage 3)
(Electronic AKI alert)
- Treat underlying probles
(dehydration, sepsis,
medication review etc.)
-To arrange Hospital
admission in appropriate
cases3**
- Repeat U & Es – 24 hours if
treated in community5
-
-Treat underlying problems (dehydration, infection, medication
review etc.)
- Repeat U & Es in 24- 48 hours
- Hospital admission if
progressive /in appropriate cases3
AKI stage 2
Patient Details:
Date:
Baseline Cr/ date:
Latest Creatinine (Cr):
Urine dip test:
To arrange patient review (To exclude CKD) and medication review
To repeat U & E within 24-48 hours (i.e, as per AKI stages as below)
-Treat underlying problems (dehydration, infection,
medication review etc.)
- Consider Hospital admission in
appropriate cases3**
- Repeat U & Es in 24 hours if
treated in community5
s ahmed, 2014

Referral Nephrology:
Discuss AKI management with a nephrologist/paediatric nephrologist as
soon as possible (and within 24 hours) if one of the following is present:
Potential diagnosis requiring
specialist treatment (for example,
vasculitis or glomerulonephritis)
AKI with no clear
cause
Inadequate treatment
response
Complications associated with AKI Stage 3 AKI
eGFR is less than < 30
ml/min/1.73 m2 after
AKI episode
Patients with renal transplant and
AKI
CKD stage 4 or 5
Renal replacement therapy:
Refer adults, children and young people immediately for RRT if any of the
following are not responding to medical management:
Hyperkalaemia Metabolic
acidosis
Symptoms or complications
of uraemia such as
pericarditis or
encephalopathy
Fluid overload
+/- pulmonary
oedema
s ahmed, 2014

Summary 1: CKD - aim of Rx First, Identify CKD
CV risk reduction:
Target BP control / Rx of hyperlipidaemia
Control of proteinuria – ACEI/ARB Target primary disease: ex.- good control of diabetes Specific Rx for CKD – anaemia / bone disease CKD vs. AKI
s ahmed, 2014

Thank you
Any Question ?
s ahmed, 2014