Cirorhosis Hepatis (Indy File)
44
CIRRHOSIS OF THE LIVER Defenition Cirrhosis of the liver is a chronic diffuse process with fibrosis and nodule formation anatomically. It was followed hepatocelluler necrosis. Although the causes are many, the end result and two mayor event, failure of liver function and portal hypertension. Etiology 1. The caused was known : Hepatitis virus type B and C. Alcoholic Metabolic, inherited and drug related Imunologic disturbance. Malnutrition. Cardiac Biliary 2. Unknown Case Presentation 1
-
Upload
cheche-novelia -
Category
Documents
-
view
128 -
download
6
Transcript of Cirorhosis Hepatis (Indy File)

CIRRHOSIS OF THE LIVER
Defenition
Cirrhosis of the liver is a chronic diffuse process with fibrosis and
nodule formation anatomically. It was followed hepatocelluler necrosis.
Although the causes are many, the end result and two mayor event, failure
of liver function and portal hypertension.
Etiology
1. The caused was known :
Hepatitis virus type B and C.
Alcoholic
Metabolic, inherited and drug related
Imunologic disturbance.
Malnutrition.
Cardiac
Biliary
2. Unknown
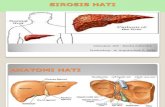
Pathogenesis
The response of the liver to necrosisasstricly limited, the most
important are collapse of hepati lobules, formation of diffuse fibrous
septum and nodular regrowth of liver ell. Thus, irrespective of etiology, the
ultimate histological picture of the liver is similar.
Case Presentation1

When the liver cell became necrotic, the reticulinframe workcollapsis with
approxiamation of portal and central zones. Some cell grow to from
nodules of various size. The nodules distort the hepatic tree so that portal
flow is impanden and portal hypertention results.
Sinusoid persist at periphery of the site of the portal central bridges.
Portal blood is diverted past functioning liver tissue leading to vasculer
insufficiency at the centre of the nodules. Basement membranes from in
the perisinosoidal from the sinusoids and the liver cells.
Clinical feature
In patient with cirrhosis of known etiology in whom there is progression
to a post necrotic stage. The clinical feature an extension of those
resulting from the initial desease process. Ussually clinical symptom are
related to portal hypertension and the sequale such as ascites,
splenomegally, hipersplenisme and bleeding esophageal varicess. The
hematology and hiperfunction abnormalities resemble those seen with
other types of cirrhosis hepatis
A. Compensated Cirrhosis
There is no complain from the patient, no specially complain such as
not healthy, exhausted powerlss, decreased in appatite, felt swollen,
weight loss and fatique. There is no defferences symptoms with chroni
hepatitis without cirrhosis depend on the liver necrosis.
B. Decompensated Cirrhosis
We can diagnosed the patient with the clinical examination,
laboratorium finding and another suggest examination. Esspecially appear
Case Presentation2

liver failure and portal hypertension complain with manifestation like
palmar erytema, vascular spiders, colateral vein, jaundice, oedema of the
feet and ascites.
Examination
Liver enlargement at earlier cirrhosis. The consistence is elastic
firm, blunt edge, pain pressure.
Splein, the parameter to known the enlargement is with scuffner
line ( I-VII).
Collateral vessels and ascites.
Spider teleangiectacia and palmaris erythema.
Dullnes percussion is very late sign of fluid under tension.
Ascitic fluid and paracentesis abdominis. Diagnosis
paracentesis is always performed. The terapeutic paracentesis
is very rarely necessary unless the patients is in severe
discomfort. Protein consentration rarely excess 10-20 g/l
Urine, the urine volume is diminished and it is deeply
pegmented and of high osmolarity. The daily out put of sodium
is greatly reduced.
Diagnosis
Post necrotic cirrhosis hepatis must be suspected in patient with
sign and sympton of cirrhosis or portal hypertension. Needle or
operativeliver biopsy confirm the diagnosis, also non uniformity of
patologic process my result in sampling errors.
Case Presentation3

Cirrhosis hepatic decompensated stage diagnosed by Suharyono
Subandri that 5 from 7 sign below can asume as it, the sign are:
Ascites
Splenomegaly
Varicess esophageal bleeding
Low albumin
Spider naevi
Palmaris Erytema
Collateral
Treatment
Management is ussually limited to treatment of the complication of
portal hypertension, including control of ascites, avoidence of drugs or
excessive protein intake that my include hepatic coma and prompt
treatment of infection, in patient in whom post necrotic cirrhosis hepatic
has developed as a result of treatable condition. Therapy directed at the
primary disorders may limit further progression.
Complication
Portal hypertension
Varicess esophageal
Ascites
Splenomegaly.
Case Presentation4

CASE REPORT
A 40 years old man was admitted to Internal Medicine Department
of General Hospital Dr. Ahmad Moechtar Bukittinggi on August 15 th 2002
with :
Chief complain : Have a right stomachache since 3 days ago.
Present Illness History :
Have a right stomachache since 3 days ago.
The patient feel weakness since 20 days ago.
The patient feel discomfort in his abdoment since 20 days ago.
Urine was like a strong of tea since 7 days ago.
Diarrhea with mucous since 3 days ago.
Febris since 3 days ago.
Headache since 3 days ago.
Nausea (+), vomite (-).
Previous Illness History :
No history of yellow disease, hypertension, diabetes melitus.
Family Illness History :
None of the family members had suffered the disease like this
Habitually History :
Never drinks alcohol
Physical Examination :
Vital sign :
General appearance : moderately ill
Case Presentation5

Consciousness : composmentis cooperatif
Blood pressure : 120/70 mmHg
Pulse rate : 92 x/min
Respiratory rate : 23 x /min
Body temperature : 37,50 C
Skin : icteric
Lymph node : no enlergment
Head : Eye : conjunctiva was anemic
Sclera was icteric
Ears, mouth and nose : normal
Neck :
JVP : 5 – 2 cm H2O
Regional lymph node : no enlargement
Thyroid gland : no enlargement
Chest : normochest, spider naevi (+)
Lung :
Inspection : simetric movement left and right
Palpation : fremitus was the same on the right and left side
Percusion : sonor both of lung
Auscultation : vesicular normal, ronchi (–), wheezing (–)
Heart :
Inspection : ictus was not visible
Palpation : ictus was palpable at 1 finger medial LMCS ICS V
Percusion : left border : 1 finger medial LMCS ICS V
Case Presentation6

right border : right sternalis line
upper border : ICS II
Auscultation : pure, regular rhythm, M1 > M2, P2 < A 2, murmur (–)
Abdomen :
Inspection : swollen abdomen (+), collateral (+)
Palpation : liver was palpable at 3 fingers under arcus costae, 3
fingers under processus xipoideus, difus, elastic, dull
and pain pressure (+)
Spleen was palpable (Schuffner 1) .
Percusion : tympany, shifting dullness (+)
Auscultation : peristaltic sound was normal
Back : pressure pain (–), knock pain (–).
Extremities :Right Left
Physiological reflex + +
Pathological reflex – –
Smooth sensibility + +
Rough sensibility + +
Edem - -
Palmar erythema : (–)
Laboratory findings :
Blood :
Hb : 5,6 g% Leucocyte : 9300/mm3
DC : 0 / 2 / 2 / 61/ 29/ 6 BSR : 30 mm/hour
Eritrocyte : 2 million ul Reticulocyte : 15 %
Case Presentation7

HbsAg :(+) Anti Hbs : (–)
SGOT :46 u/I SGPT :36 u/I
Protein total : 5,19 gr%
Albumin : 3,05 gr%
Globulin : 2,14 gr%
Total bilirubin: 1,2 gr%
Direct bilirubin: 0,28 gr%
Indirect bilirubin: 0,92 gr%
Ureum : 28
Creatinin : 0,7
Pheriperal Blood Appearance : Anisositosis, polikromasi, micrositic
hipochrom anemia.
Urin :
Bilirubin : (-) Protein : (–)
Urobilin : (+) Reduction : (–)
Sediment : eritrocyte : 0–1/ wf
Leucocyte : 1-2 / wf
Cylinder : (–)
Epitel : squamous (+)
Crystal : (–)
Feces :
Colour : Yellow Consistance : mole
Blood : (-) Bacterial : (-)
Ancylostoma sp: (+)
Case Presentation8

Working diagnosis :
- Cirrhosis hepatis post necrotic decompensated stage
- Micrositic hypocrhome anemic ec Ancylostomiasis
Differential diagnosis :
- Hepatoma
- Hepatitis B
Treatment :
Unagen 2x1
Aspar K 3x1
Spironolacton 2x1
Miniseronal 3x1
Suggested examination :
USG abdominal
Liver physiologic
Endoscopy
Follow up
August 15th 2002
A : Stomachache (+), weakness of the body (+), Fever (+).
Urine was like a strong of tea
PE :
GA Consc BP PR RR TModerate cmc 120/70 82x/i 24x/i 36,50C
Eye : conjungtiva was anemic
Sclera was icteric
Case Presentation9

Abdomen : same as before
WD/ : same as before
Treatment : continue
Follow up
August 16th 2002
A : Stomachache (-), weakness of the body (+), Fever (-).
Urine was like a light tea
PE :
GA Consc BP PR RR TModerate cmc 100/70 80x/i 20x/i 370C
Eye : conjungtiva was anemic
Sclera was icteric
Abdomen : same as before
WD/ : same as before
Treatment : continue
Follow up
August 17th 2002
A : Stomachache (+), weakness of the body (+), Fever (-).
Urine was yellow
Bowel (-), appetite (+)
PE :
GA Consc BP PR RR TModerate cmc 110/70 85x/i 20x/i 370C
Eye : conjungtiva was anemic
Sclera was icteric
Abdomen : same as before
WD/ : same as before
Treatment : continue
Case Presentation10

Follow up
August 19th 2002
A : Stomachache (+), weakness of the body (+), Fever (-).
Urine was yellow and irreguler mixturation.
Bowel (+), appetite decreased
PE :
GA Consc BP PR RR TModerate cmc 110/70 83x/i 20x/i 370C
Eye : conjungtiva was anemic
Sclera was icteric
Abdomen : same as before
WD/ : same as before
Treatment : continue + Spironolacton 3x1
Follow up
August 20th 2002
A : Distanded stomache (+), weakness of the body (+), Fever (-).
Urine was yellow and regular.
Bowel (+), appetite (+)
PE :
GA Consc BP PR RR TModerate cmc 110/70 83x/i 20x/i 370C
Eye : conjungtiva was anemic
Sclera was icteric
Abdomen : same as before
WD/ : same as before
Treatment : continue + Furosemid 1x1+Mebendazol 1x500 mg
Follow up
August 22nd 2002
A : Distanded stomache (+), weakness of the body (+), Fever (-).
Case Presentation11

Urine was yellow and regular.
Bowel (+), appetite (+)
PE :
GA Consc BP PR RR TModerate cmc 110/70 83x/i 20x/i 370C
Eye : conjungtiva was anemic
Sclera was icteric
Abdomen : Ascites decreased
WD/ : same as before
Treatment : continue
Follow up
August 29th 2002
A : Stomachache (+), weakness of the body (+), Fever (-).
Urine was yellow and regular.
Bowel (+), appetite (+)
PE :
GA Consc BP PR RR TModerate cmc 110/70 68x/i 20x/i 360C
Eye : conjungtiva was anemic
Sclera was icteric
Abdomen : Ascites decreased
Lab : Hb : 8 mg%
WD/ : same as before
Treatment : continue + blood transfusion
Case Presentation12

DISCUSSION
The diagnosis on this case made based on anamnesa, physical
examination, and laboratory finding. From anamnesis was found right
stomachache, discomfort of stomache, urine was like strong of tea.
From physical exemination found that conjunctiva was anemic,
sclera was icteric, spider naevi (+), liver was palpable 3 fingers under
arcus costae, 3 fingers under processus xipoideus, difus, elastic, dull and
pain pressure (+), spleen was palpable (Schuffner 1), collateral (+).
From laboratory finding we found Hb 5,6 g%, Pheriperal blood
appearance anisositosis, polikromation, micrositic hypocrhom anemic,
HbsAg (+), SGOT increased, SGPT increased, total protein decreased,
Case Presentation13

Albumin decreased.Total bilirubin increased, indirect bilirubin
increased.From the feces : ancylostoma sp (+).
Based on these data we can diagnose this patient with cirrhosis
hepatis post necrotic decompensated stage and micrositic hypocrhom
anemic ec ancylostomiasis.
CASE REPORT
A 51 years old man was admitted to Internal Medicine Department
of General Hospital Dr. Ahmad Moechtar Bukittinggi on May 31 th 2002
with :
Chief complain : Vomitus wich contain stomach liquid with a black colour
of blood since 5 days ago.
Present Illness History :
Vomitus wich contain stomach liquid with a black colour of blood
since 5 days ago ± 6 times aday aproximately ± 1 glass.
Feeling weakness, fatique, tired since 6 months go.
Case Presentation14

Loose of apatite since 6 months ago.
Have a not persistent febris since 2 months ago.
Icterics eye s followed by all of bodies since 1 month ago.
Pruritus was positif all of body since 1 month ago.
Miksi was like a tea colour since 1 month ago.
Get stomach pain and feel puffed up since 1 month ago.
Bowel was have black colour like an aspal since 15 days ago.
Oedem at both of foot since 5 days ago.
Previous Illness History :
No history of yellow disease
Family Illness History :
None of the family members had suffered the disease like this
Habitually History :
Never drinks alcohol
Physical Examination :
Vital sign :
General appearance : moderately ill
Consciousness : composmentis cooperatif
Blood pressure : 110/70 mmHg
Pulse rate : 84 x/min
Respiratory rate : 20 x /min
Body temperature : 360 C
Body height : 160 cm
Body weight : 45 Kg
Case Presentation15

Skin : icteric (+)
Lymph node : no enlergment
Head : Eye : conjunctiva was anemic
Sclera was icteric
Ears, mouth and nose : normal
Neck :
JVP : 5 – 2 cm H2O
Regional lymph node : no enlargement
Thyroid gland : no enlargement
Chest : normochest
Lung :
Inspection : simetric movement left and right
Palpation : fremitus was the same on the right and left side
Percusion : sonor both of lung
Auscultation : vesicular normal, ronchi (–), wheezing (–)
Heart :
Inspection : ictus was not visible
Palpation : ictus was palpable at 1 finger medial LMCS ICS V
Percusion : left border : 1 finger medial LMCS ICS V
right border : right sternalis line
upper border : ICS II
Auscultation : pure, regular rhythm, M1 > M2, P2 < A 2, murmur (–)
Abdomen :
Case Presentation16

Inspection : distended abdomen (+), collateral (–)
Palpation : liver was palpable at 2 fingers below of arcus costae,
difus, elastic, dull and pain pressure (+)
Spleen could not palpable.
Percusion : shifting dullness (+)
Auscultation : peristaltic sound was normal
Back : pressure pain (–), knock pain (–).
Extremities :Right Left
Physiological reflex + +
Pathological reflex – –
Smooth sensibility + +
Rough sensibility + +
Edem + +
Palmar erythema : (–)
Laboratory findings :
Blood :
Hb : 7 g% Ureum : 101,3 mg %
Leucocyte : 13600/mm3 Creatinin : 2,9 mg %
DC : 0 / 2 / 3 / 61/ 30/ 4 SGOT : 130 uL
BSR : 20 mm/hour SGPT : 100 uL
Eritrocyte : 2.3 million ul Total bilirubin : 10,9 mg %
Reticulocyte : 2,5 % Bilirubin indirect : 5,13 mg %
HbsAg : (–) Bilirubin direct : 4,96 mg %
Anti Hbs : (–) Protein total : 3,59 g %
Case Presentation17

ALP : 361 Albumin : 1,87 g %
Globulin : 1,72 g %
Urin :
Bilirubin : (+) Protein : (–)
Urobilin : (+) Reduction : (–)
Sediment : eritrocyte : 0–1
Leucocyte : (+)
Cylinder : (–)
Epitel : squamous (–)
Crystal : (–)
Working diagnosis :
Cirrhosis hepatis billiary decompensated stage
Differential diagnosis :
Cirrhosis hepatis post necrotic decompensated stage
Treatment :
Bad rest untill icteric, acites, and febris was recovery.
Diet low protein and low salt ( DH I )
Furosemid 1x1 tab
KCL 1x1 tab
Tramadol 2x1 tab
Miniproterenol 3x1 tab
Case Presentation18

Curcuma 3x1 tab
Suggested examination :
Routine blood, urine, feces test HbsAg USG
abdominal
Liver physiologic Endoscopy Liver biopsi
Cholangiography
Follow up
June 3th 2002
A : Fatique, weakness, lose of apatite,
Feces was brown, urine was like a tea
Stomach pain
PE :
GA Consc BP PR RR TModerate cmc 120/70 88x/i 20x/i 36,50C
Eye : conjungtiva was anemic
Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
WD/ : Cirrhosis hepatis billiary decompensated stage
Treatment : continue
June 5th 2002
A/ : frigoris
Nausea (+), vomitus (+).
Fatique
Stomach pain
PE:
Case Presentation19

GA Consc BP PR RR TModerate cmc 120/70 88x/i 20x/i 36,50C
Eye : conjungtiva was anemic
Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
Laboratory finding:
Hb : 13,1 gr %
Leucocyte : 16200/mm3
Treatment : continue
June 6th 2002
A : Frigoris, Fatique, Diarhoe
PE :
GA Consc BP PR RR TModerate cmc 120/70 70x/i 22x/i 36,50C
Eye : conjungtiva was not anemic
Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
Treatment : continue
June 8th 2002
A : Fatique
Distended abdome
Nausea (+)
Feces was yellow 5–6 x/ day
PE :
GA Consc BP PR RR TModerate cmc 120/70 85x/i 19x/i 36,50C
Eye : conjungtiva was not anemic
Case Presentation20

Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
Treatment : continue
June 10th 2002
A : febris (+), burn stomach
Distended abdomenfeces was gray
Mixturiatio was like a tea
PE :
GA Consc BP PR RR TModerate cmc 120/70 80x/i 20x/i 38,10C
Eye : conjungtiva was not anemic
Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
Laboratory finding:
HbsAg : (–) Total bilirubin : 10,9 mg %
Anti Hbs : (–) Bilirubin indirect: 5,13 mg %
SGOT : 130 uL Bilirubin direct: 4,96 mg %
SGPT : 100 uL
Treatment: continue
June 12th 2002
A : febris (+), burn stomach
Distended abdomenfeces was gray
Mixturiatio was like a tea
PE :
GA Consc BP PR RR TModerate cmc 120/70 84x/i 20x/i 37,50C
Case Presentation21

Eye : conjungtiva was not anemic
Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
Laboratory finding:
Feces : Macroscopic: yelow, solid
Urine : Eritrocyte : 1–2
Leucocyte : +
Bactery : +
Bilirubin : +
Urobilin : +
Treatment: continue
June 19th 2002
A : Fatique, weakness, lose of apatite,
Stomach pain
PE :
GA Consc BP PR RR TModerate cmc 120/70 82x/i 21x/i 36,70C
Eye : conjungtiva was not anemic
Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
Laboratory finding:
Total bilirubin : 7,79 mg % SGOT : 77 uL
Bilirubin indirect: 4,84 mg % SGPT : 98 uL
Bilirubin direct: 2,95 mg %
Case Presentation22

Treatment: continue
June 20th 2002
A : Fatique, weakness
Urine was like a tea
PE :
GA Consc BP PR RR TModerate cmc 120/70 85x/i 20x/i 36,50C
Eye : conjungtiva was anemic
Sclera was icteric
Skin : icteric
Extremity : Edema of foot : +/+
Treatment : continue
Case Presentation23

DISCUSSION
The diagnosis on this case made based on anamnesa, physical
examination, and laboratory finding. From anamnesis was found stomach
swelling since five months ago, the patients felt his stomach quikly full if
eaten some food since five months ago, and the patient also had history
alcohol consumption when his young, not all the times.
From physical exemination found that liver was palpable 5 fingers
below processus xipoideus, and 3 finger below arcus costae, blunt edge,
hard, surface was not flat, pressure pain negative. Spleen was palpable
until S4 and kidney was not palpable. in percussion of the abdoment is
tympany, but on the mass is dullnes. On the extremitas we found that
palmaris eritema in the patient hand.
From laboratory finding we found SGOT/ SGPT was increase, ratio
albumin and globulin inverse which albumin is decrease and globulin is
increase. Alkali fosfatase is normal. Concentration of ureum, kreatinin, and
uric acid is normal. Based on this data we can diagnosed this patient with
hepatoma.
Case Presentation24

CASE REPORT
A 52 years old man was admitted to Internal Medicine Department
of General Hospital Dr. Ahmad Moechtar Bukittinggi on August 30 th 2002
with :
Chief complain : Vomitus wich contain stomach liquid with a black colour
of blood since 1 day ago.
Present Illness History :
Vomitus wich contain stomach liquid with a black colour of blood
since 1 day ago, 1 x, aproximately ± 1 glass,nausea (-).
Febris since 1 day ago.
Headache since 1 day ago
Urine was like a tea colour since 3 days ago.
Bowel was have black colour since 3 days ago.
Edema (-)
Previous Illness History :
No history of yellow disease
Consumed traditional drug for rheumatic disease since three
years ago
Family Illness History :
None of the family members had suffered the disease like this
Case Presentation25

Habitually History :
Consumed traditional drug for rheumatic disease since three years
ago
Never drinks alcohol
Physical Examination :
Vital sign :
General appearance : moderately ill
Consciousness : composmentis cooperatif
Blood pressure : 120/80 mmHg
Pulse rate : 80 x/min
Respiratory rate : 28 x /min
Body temperature : 360 C
Skin : no icteric
Lymph node : no enlergment
Head : Eye : conjunctiva was anemic
Sclera was not icteric
Ears, mouth and nose : normal
Neck :
JVP : 5 – 2 cm H2O
Regional lymph node : no enlargement
Thyroid gland : no enlargement
Chest : normochest, spider naevi (+)
Case Presentation26

Lung :
Inspection : simetric movement left and right
Palpation : fremitus was the same on the right and left side
Percusion : sonor both of lung
Auscultation : vesicular normal, ronchi (–), wheezing (–)
Heart :
Inspection : ictus was not visible
Palpation : ictus was palpable at 1 finger medial LMCS ICS V
Percusion : left border : 1 finger medial LMCS ICS V
right border : right sternalis line
upper border : ICS II
Auscultation : pure, regular rhythm, M1 > M2, P2 < A 2, murmur (–)
Abdomen :
Inspection : distended abdomen (-), collateral (–)
Palpation : liver was palpable at 1 finger under arcus costae, 3
fingers under processus xipoideus, difus, elastic, dull
and pain pressure (-)
Spleen was palpable (Schuffner 1) .
Percusion : tympany, shifting dullness (-)
Auscultation : peristaltic sound was normal
Back : pressure pain (–), knock pain (–).
Extremities :Right Left
Physiological reflex + +
Case Presentation27

Pathological reflex – –
Smooth sensibility + +
Rough sensibility + +
Edem - -
Palmar erythema : (–)
Laboratory findings :
Blood :
Hb : 4,6 g% Leucocyte : 5200/mm3
DC : 0 / 2 / 3 / 59/ 30/ 6 BSR : 8 mm/hour
Eritrocyte : 1,6 million ul Reticulocyte : 3,2 %
Anti Hbs : (–)
Pheriperal Blood Appearance : Anisositosis, polikromasi, micrositic
hipocrhom anemia.
Urin :
Bilirubin : (-) Protein : (–)
Urobilin : (+) Reduction : (–)
Sediment : eritrocyte : 0–1/ wf
Leucocyte : 2-3 / wf
Cylinder : (–)
Epitel : squamous (–)
Crystal : (–)
Feces :
Colour : Black Consistance : mole
Blood : (-) Bacterial : (-)
Case Presentation28

Working diagnosis :
- Hematemesis Melena ec varices esophageal bleeding
ec Cirrhosis hepatis post necrotic decompensated stage
- Micrositic hypocrhome anemic ec bleeding
Differential diagnosis :
Hematemesis Melena ec varices esophageal bleeding ec Cirrhosis
hepatis decompensated stage ec traditional drug.
Treatment :
Bed rest, fast 24 – 48 hours after bleeding (-)
Diet low protein and low salt ( DH I )
NaCl inj 20 gtt/ minute
Transamin inj 3x1 amp
Vit K inj 3x1 amp
Suggested examination :
USG abdominal
Liver physiologic
Endoscopy
Follow up
August 31th 2002
A : Vomite (-), Fever (-), Headeache (-)
Feces was black, urine was like a tea
PE :
GA Consc BP PR RR T
Case Presentation29

Moderate cmc 120/70 81x/i 26x/i 36,50C
Eye : conjungtiva was anemic
Sclera was not icteric
Abdomen : same as before
WD/ :
- Hematemesis Melena ec varices esophageal bleeding ec Cirrhosis
hepatis post necrotic decompensated stage
- Micrositic hypocrhome anemic ec bleeding
Treatment : continue
Case Presentation30

DISCUSSION
The diagnosis on this case made based on anamnesa, physical
examination, and laboratory finding. From anamnesis was found Vomitus
wich contain stomach liquid with a black colour of blood, febris, headache,
urine was like a tea colour, bowel was have black colour, and the patient
also had history drug traditional for rheumatic consumption since three
years ago.
From physical exemination found that Conjunctiva was anemic,
spider naevi (+), liver was palpable 1 finger under arcus costae, 3 fingers
under processus xipoideus, difus, elastic, dull and pain pressure (-),
spleen was palpable (Schuffner 1) .
From laboratory finding we found Hb 4,6 g%, Pheriperal blood
appearance anisositosis, polikromation, micrositic hypocrhom anemic,
HbsAg (+),
From the feces : colour was black. Based on this data we can diagnosed
this patient with hematemesis melena ec varices esophageal bleeding
ec cirrhosis hepatis post necrotic decompensated stage and micrositic
hypocrhom anemic ec bleeding
Case Presentation31

Case Presentation32