Chronic Venous Insufficiency: Diagnosis &...
43
Chronic Venous Insufficiency: Diagnosis & Management Jennifer M. Thomas, M.D. AnMed Vascular Medicine February 28, 2015
Transcript of Chronic Venous Insufficiency: Diagnosis &...

Chronic Venous Insufficiency:
Diagnosis & Management
Jennifer M. Thomas, M.D.AnMed Vascular Medicine
February 28, 2015
Presenter
Presentation Notes
Thank you for allowing me to present today, very relevant topics we all see in practice daily…

Background• Chronic Venous Insufficiency (CVI) affects 25 to 30%
of women and 15% of men in US
• Varicose veins are the most recognized manifestation of CVI, affecting 1 out of 5 adults
• Number of studies have estimated that 1% of the adult population will be affected by venous ulceration at some point
• Direct medical cost of CVI in US estimated to be up to $1 billion/year

Prevalence of Venous Insufficiency
0. 6.25 12.5 18.75 25.
Venous Reflux Disease
Coronary Heart Disease
Peripheral Arterial Disease
Congestive Heart Failure
Stroke
Cardiac Arrhythmias
Heart Valve Disease
Annual U.S. IncidenceU.S. Prevalence
Millions
Venous reflux disease is 2x more prevalent than coronary artery disease (CAD) and 5x more prevalent than peripheral arterial disease (PAD)1
Presenter
Presentation Notes
- Also important to keep in mind many of these patients are younger than PAD, lose more days out of work

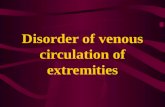
Anatomic Considerations• Lower extremity venous system
is unique in its constant need to overcome gravity while returning blood to the heart
• Normally, the calf pump and vein valve system accomplish this task
• With CVI, the valves become disrupted by a thrombotic event (secondary), can be congenitally absent/atretic, or can become dysfunctional over time (primary)
Deep femoral v.
Femoral v.
Popliteal v.
Small saphenous v.
Great saphenous v.
Perforating v.
Perforating v.
Presenter
Presentation Notes
have 3 kind of veins: superficial (lie close to the skin), deep (within groups of muscles), and perforators (connect the 2) valves are one-way flaps entire process of sending blood back to the heart is called the venous pump

Pathophysiology
• Multiple theories, all involve increased venous pressure and damage to the microcirculation
• Increases in capillary hydrostatic pressure are normally offset by the postural vasoconstriction reflex and the functional calf muscle pump
• Both are impaired in severe CVI, and perforator vein valves are often incompetent
Presenter
Presentation Notes
- under supine conditions, capillary hydrostatic pressure is 25 mmHg, then quadruples upon standing; if no compensatory mechanisms, fluid filtration increases and edema rapidly develops - when you sit/stand for long periods of time, blood in leg veins pool and increase venous pressure, damages vein valves

Pathophysiology• In calf pump muscle failure, blood from the deep
venous systems transmits pressure to the superficial system, causing increases in filtration pressure and edema
• CVI in obese patients is further exacerbated by lymphatic overload
• Bottom line: saphenofemoral or saphenopopliteal reflux occurs in 85% of patients with varicose veins as result of valvular incompetence
Presenter
Presentation Notes
-these incompetent superficial veins are important targets for management of CVI

Pathophysiology of Venous Insufficiency

Signs & Symptoms• SIGNS:
Varicose veins, telangiectasias, edema, hyperpigmentation,
eczema, lipodermatosclerosis
• SYMPTOMS:
Leg pain (especially after prolonged standing), itching, paresthesias, cellulitis, leg ulcers, restless legs, variceal bleeding, superficial thrombophebitis
• Compared to arterial disease, symptoms usually improve with leg elevation

Risk factorsAge
Female gender
Pregnancy
Obesity
Occupation
Previous DVT
Genetics
Sedentary lifestyle
Previous injury or surgery

Physical Examination
• Should examine patients standing, noting telangiectasis (dilated venules <1mm), reticular veins (nonpalpable subdermal veins <3mm), and varicose veins (>3mm)
• Also note edema, skin pigmentary changes, ulcers

Diagnostic Testing• Venous duplex supplements physical exam
• Safe, non-invasive, cost-effective method of determining reflux in the superficial, deep, and perforating veins
• Definition of reflux: retrograde flow lasting >0.5 seconds
• Can also identify thrombophlebitis and venous obstruction from previous thrombosis
Presenter
Presentation Notes
- very important to have good quality duplex, must make sure deep system is patent prior to ablation of superficial system

GSV reflux on duplex imaging
Presenter
Presentation Notes
- duplex performed with pt in standing position reflux elicited by squeezing calf (proximal veins) or foot (calf veins); compression with release (augmentation) distal to the point of insonation reliable method of detecting reflux compression abruptly removed, and presence and duration of reflux are observed with compression, vein flow initially increased as blood is pushed in normal direction of flow; once compression released, blood flow reverses momentarily

CEAP Classification• Clinical
C0: No visible or palpable signs of venous diseaseC1: telangiectases or reticular veinsC2: varicose veinsC3: edemaC4: skin changes ascribed to venous disease
a. pigmentation or eczemab. lipodermatosclerosis
C5: healed venous ulcerC6: active venous ulcer
Etiologic: congenital, primary, secondary or noneAnatomic: superficial, perforator, deepor nonePathophysiologic: reflux, obstruction, both or none

Examples of Advanced CVI
• C3 (edema): C4a (hyperpigmentation): C4b (lipodermatosclerosis):

Examples of Advanced CVI
C5 (healed ulcer): C6 (active ulcer):

Natural History
• Varicose veins constitute a progressive disease that steadily becomes worse
• Most frequent complications include superficial thrombophlebitis, bleeding, and ulcerations
• Treatment is tailored to patient’s age, comorbidities, and severity of symptoms

Conservative Management
• Bandaging has been mode of treatment since time of Hippocrates
• Graduated compression stockings combined with exercise regimen have been shown to control reflux and improve calf muscle pump function
• Compliance with stockings is significant clinical limitation
Presenter
Presentation Notes
-many pts have difficulty wearing or tolerating compression garments

Compression TherapyCLASS PRESSURE LEVEL OF
SUPPORTINDICATION CEAP
OTC <15 mmHg Minimal Asymptomatic,comfort only.
0, 1
I 15-20 mmHg Mild Minor varicosities, tired aching legs, minor swelling.
1, 2, 3
II 20-30 mmHg Moderate Moderate to severe varicosities, moderate swelling,phlebitis, following ablation.
3, 4
III 30-40 mmHg Firm Severe varicosities, swelling, management of ulcerations, following DVT, post surgery.
4, 5, 6
IV >40 mmHg Extra firm Lymphedema. NA

Conservative Management• Aside from compression, need to elevate legs to
level of heart 30 minutes 3-4 times/day
• Daily walking and simple ankle flexion exercises
• Losing weight
• Taking NSAIDs as needed for inflammation
• Appropriately lubricating with emollients, can use topical steroids for stasis dermatitis

Pneumatic Compression Therapy
Presenter
Presentation Notes
- Insurance will usually only approve for treatment of refractory lymphedema, though some studies clearly show improvement in ulcer healing times and decreased rate of recurrence

Medical Therapy• Diuretics – very overprescribed, should typically only
be used when other conditions such as CHF or CKD are contributing to swelling
• ASA – seems to accelerate healing of stasis ulcers
• Pentoxifylline – competitive nonselective phosphodiesterase inhibitor may also accelerate healing, can be adjunct to wound care and compression
• Horseshoe chestnut – placebo-controlled RCTs suggest decrease in lower leg volume and reduction in leg circumference at calf and ankle
Presenter
Presentation Notes
- Insurance will usually only approve for treatment of refractory lymphedema, though some studies clearly show improvement in ulcer healing times and decreased rate of recurrence

Conservative Management• Compression stockings do not address cosmetic
concerns
• REACTIV trial
• 1,009 CVI subjects
• Prospectively demonstrated significant improvement in health care-related QOL when managed with surgery or sclerotherapy compared to conservative management

Conservative vs Invasive Therapy
• ESCHAR (Effect of Surgery and Compression on Healing and Recurrence) trial
• C5, C6 patients randomized to medical therapy (elevation, compression, exercise) or surgical tx of superficial reflux
• No difference in rates of healing, but dramatic reduction in ulcer recurrence (12 vs 28% at 12 months)

Conservative vs Invasive Therapy
• Another recent RCT (Michaels et al) showed patients randomized to surgery had significant improvement in QOL and symptomatic relief
• These RCTs provide a grade A recommendation for surgery in addition to conservative tx in patients with VV caused by GSV reflux

Surgical Techniques
• High ligation of the Greater Saphenous Vein (GSV), +/- stripping
• Endovenous thermal ablation (EVA)
• Ambulatory Phlebectomy
Presenter
Presentation Notes
high ligation has theoretical advantage of preserving GSV for lateral use as conduit for CABG or LE bypass unfortunately HL without stripping fails to eliminate axial reflux in most pts and is commonly associated with VV recurrence EVA has been used since 1999

GSV ligation & stripping
• Possible complications include persistent lymphatic leak, prolonged wound healing, wound infection
• May require up to 4 weeks of convalescence
• Neovascularization of SFJ common, and varicose veins may recur in 20 to 60% of patients within 10 years, up to 70% after 10 years

Comparison of EVA vs L&S
• In multiple trials, EVA (using both laser and RFA techniques) found to be equally effective in eliminating reflux, with less pain and shortened time to return to normal activities compared to L&S
• Two types of energy available:
• Radiofrequency (RFA)
• Laser

Radiofrequency Ablation (RFA)
• Catheter has 7cm bipolar electrode on its distal end, can perform segmental ablation
• Mechanism involves electrode making direct contact with the vein wall to deliver RFA
• Contact with the wall results in destruction of the endothelium, occlusion by contraction of the vein wall collagen, and thrombus formation

VNUS Closure® Procedure using the ClosureFAST™ Catheter

Radiofrequency Ablation• Can be used to close GSV or SSV
• Contraindication include SVT, DVT, venous aneurysm, and abnormal ABIs
• Can be performed in outpatient office setting, depends on local resources
• Pts wear compression for at least one week afterwards, and have a follow-up duplex to rule out DVT

VNUS Closure® Visual Results
Pre-treatment One week post-treatment*
*Individual results may vary

Endovenous Laser Ablation (ELA)
• Similar to RFA, primary difference is mechanism
• Uses laser energy to form steam bubbles within vein lumen, destroying the endothelial lining
• This causes inflammatory reaction resulting in thrombotic occlusion

Laser Ablation
• Pts also wear compression for at least a week, and have a follow-up venous duplex to assess treated veins and rule out DVT
• Complications for both procedures include vessel perforation, DVT (1-2%), phlebitis, hematoma, infection, skin pigmentation, paresthesias, skin burns

Endovenous Ablation• General technique similar for either RFA or laser
• Ultrasound guidance used to access GSV or SSV
• Tip of catheter positioned 1 cm from SFJ or SPJ
• Tumescent anesthesia fluid dispensed along with course of the target vein
• Energy source activated, catheter pulled back along vein to be closed
• Does not have to be performed in hospital setting
Presenter
Presentation Notes
tumescent provides pain relief and reduces risk of thermal injury also contributes to vein spasm, which helps eliminate blood flow within treated vein and create better catheter-vein apposition

Laser vs Radiofrequency
• Efficacy seems to be equivalent in latest RCT
• Laser seems to be associated with more post-procedure pain
• No real difference in cost, often dictated by local resources

Perforators• Has been source of controversy over when to treat perforators
• Grade 2B evidence to support treatment of “pathologic perforators” in patients with advanced CVI (class C5-6) in the absence of deep venous obstruction
• large (>3.5 mm)
• high-volume
• incompetent (reflux >0.5 seconds)
• located in affected area of the limb

Perforators• Treatment options include subfascial endoscopic
perforator surgery (SEPS), thermal ablation, sclerotherapy, or US-guided ligation
• RFA catheter now has FDA-approval
• Sclerotherapy works well for smaller veins that do not immediately empty into the deep system
• If perforator too superficial for ablation or too close to the deep system for sclerotherapy, US-guided ligation very useful

Sclerotherapy• Most commonly used for smaller varicosities
• Defined as introduction of chemical into lumen of a vein to induce endothelial damage that results in thrombosis and fibrosis
• Different agents can be used, compression also important post-procedure
• Complications can include hyperpigmentation, matting, cutaneous necrosis, SVT, anaphylaxis, DVT/PE, and inadvertent arterial injection

Sclerotherapy
• Up to 65% of patients treated may develop recurrent VV within 5 years, especially if saphenous reflux left untreated
• Often requires multiple treatments
• Meta-analysis of trials with long-term follow-up suggest greater long-term benefit with surgery

Recurrence of Varicose Veins
• Need to examine for recanalized veins following ablation, or neovascularization of SFJ
• May need ablation of SSV
• May also have developed accessory saphenous veins or pathologic perforators
• Recurrence more common in patients with postthrombitic syndrome, may need venography +/-IVUS to evaluate for proximal occlusive disease that may need PTA/stenting

Summary• CVI is extremely common, with a high morbidity and
cost burden to our healthcare system
• Newer technologies offer less invasive treatment options
• Goal is to improve symptoms and prevent ulcerations, unfortunately no cure
• Remember that venous duplex helps guide treatment decisions, many patients will be best treated with conservative measures

RememberDon’t let these….. Become this…..

References• Michaels et al, Health Technol Assess. 2006; 10: 1-196.
• Osinbowale et al, Review of CVI, Endo Today, 2009, 26-32.
• Heller, Treatment of CVI, Endo Today, 2011, 12-15.
• Gloviczki et al, Clinical Practice Guidelines of SVS and American Venous Forum, J Vasc Surg 2011; 53:2S-48S.
• Barwell et al, Comparison of surgery and compression with compression alone in CVI, Lancet 2004; 363: 1854-9.
• Gohel et al, Long-term results of ESCHAR, BMJ 2007; 335:83.
• Gale et al, RCT of EVLT and ClosurePlus RFA, J Vasc Surg 2010; 52: 645-50.