Chronic Obstructive Pulmonary Disease. Why COPD is Important ? COPD is the only chronic disease that...
23
Chronic Obstructive Pulmonary Disease
-
Upload
cameron-gardner -
Category
Documents
-
view
222 -
download
0
Transcript of Chronic Obstructive Pulmonary Disease. Why COPD is Important ? COPD is the only chronic disease that...

Chronic Obstructive Pulmonary Disease
Why COPD is Important ?
COPD is the only chronic disease that is showing progressive upward trend in both mortality and morbidityIt is expected to be the third leading cause of death by 2020Approximately 14 million Indians are currently suffering form COPD*Currently there are 94 million smokers in India10 lacs Indians die in a year due to smoking related diseases
*The Indian J Chest Dis & Allied Sciences 2001; 43:139-47

Disease Trajectory of a Patients with COPD
Symptoms
Exacerbations
Exacerbations
ExacerbationsDeterioration
End of Life

“Despite this burden, COPD is a “Cindrella” conditions that receives limited recognition from both patients and physicians”
Respiratory Medicine 2002; 96: S1-S31

Obstructive Airway Disease
Asthma
Explosion in
research
Revolution in
therapy
COPD
Little research
(? neglect)
Few advances in
therapy
New DefinitionChronic obstructive pulmonary disease (COPD) is a preventable and treatable disease state characterised by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and is associated with an abnormal inflammatory response of the lungs to noxious particles or gases, primarily caused by cigarette smoking.Although COPD affects the lungs, it also produces significant systemic consequences.
ATS/ERS 2004

Risk FactorsSmoke from home cooking and heating fuelOccupational dust and chemicalsGender: More common in men. M:F ratio is 5%:2.7% (in India)Increasing ageOthers: Infection, nutrition and deficiency of 1 antitrypsin

Pathophysiology of COPD
Increased mucus production and reduced mucociliary clearance - cough and sputum productionLoss of elastic recoil - airway collapseIncrease smooth muscle tonePulmonary hyperinflationGas exchange abnormalities - hypoxemia and/or hypercapnia

Key Indicators for COPD DiagnosisChronic cough Present intermittently or every
day often present throughout the day; seldom only nocturnal
Chronic sputum production Present for many years, worst in winters. Initially mucoid – becomes purulent with exacerbation
Dyspnoea that is Progressive (worsens over time)Persistent (present every day)Worse on exerciseWorse during respiratory infections
Acute bronchitis Repeated episodes
History of exposure to risk factors
Tobacco smoke (including beedi) occupational dusts and chemical smoke from home cooking and heating fuel
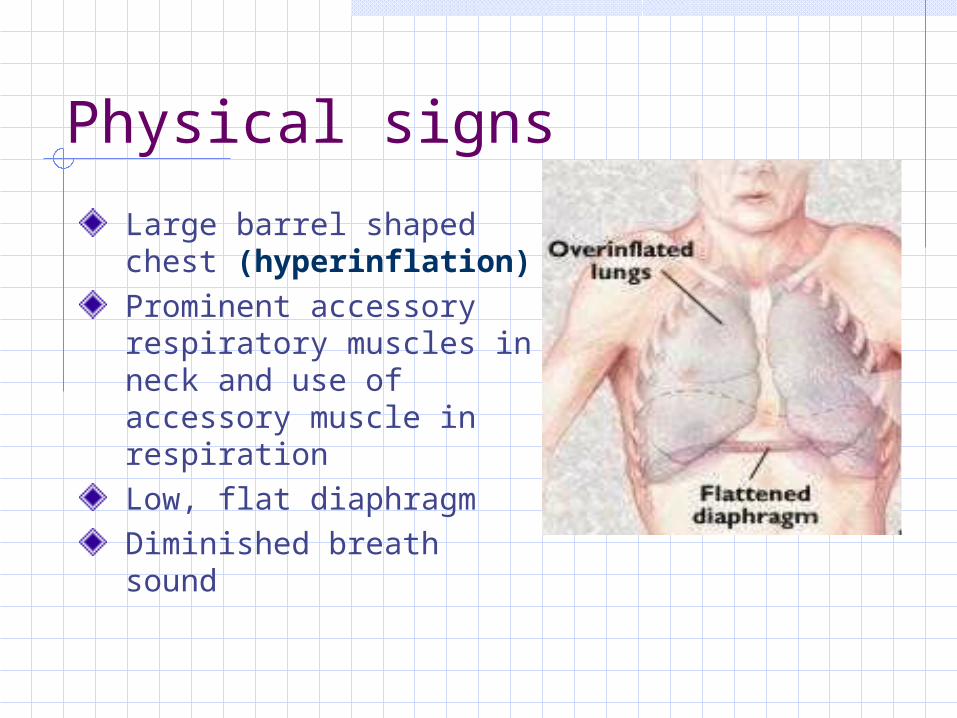
Physical signs
Large barrel shaped chest (hyperinflation)Prominent accessory respiratory muscles in neck and use of accessory muscle in respirationLow, flat diaphragmDiminished breath sound

Spirometry
Diagnosis
Assessing
severity
Assessing
prognosis
Monitoring
progression

Spirometry
FEV1 – Forced expired volume in the first secondFVC – Total volume of air that can be exhaled from maximal inhalation to maximal exhalationFEV1/FVC% - The ratio of FEV1 to FVC, expressed as a percentage.

COPD classification based on spirometry GOLD 2003
SPIROMETRY is not to substitute for clinical judgment in the evaluation of the severity of disease in individual patients.
Severity Postbronchodilator FEV1/FVC
Postbronchodilator FEV1% predicted
At risk >0.7 >80
Mild COPD <0.7 >80
Moderate COPD
<0.7 50-80
Severe COPD <0.7 30-50
Very severe COPD
<0.7 <30

Pharmacotherapy for Stable COPD
BronchodilatorsShort-acting 2-agonist – Salbutamol
Long-acting 2-agonist - Salmeterol and Formoterol
Anticholinergics – Ipratropium, Tiiotropium
Methylxanthines - Theophylline
SteroidsOral – Prednisolone
Inhaled - Fluticasone, Budesonide

Post-bronchodilator
FEV1(% predicted)
Management based on GOLD

“Bronchodilator medications are central to the symptomatic
management of COPD”
GOLD Report 2003

How Do Bronchodilators Work?
Reverse the increased bronchomotor tone
Relax the smooth muscle
Reduce the hyperinflation
Improve breathlessness

“All guidelines recommend inhaled bronchodilator as first line therapy. The ATS suggest initial therapy with an anticholinergic drug if regular therapy is needed”
Chest 2000; 117: 23S-28S

Mode of Action
Cholinergic tone is the only reversible component of COPDNormal airway have small degree of vagal cholinergic tone (no perceptible effect due to patent airways)

Mode of Action (Contd.)
Airways are narrowed in COPD therefore vagal cholinergic tone has greater effect on airway resistance (Resistance1/radius4)Therefore, the need for anticholinergic drugs that will act as muscarinic receptor antagonist and block the acetylcholine induced bronchoconstriction

Mode of Action (Contd.)
Anticholinergics may also reduce mucus hypersecretion
Anticholinergic have no effect on pulmonary vessels, and therefore do not cause a fall in
PaO2
Drugs of Today 2002; 38(9): 585-600

“Patients with moderate to severe symptoms of COPD require combination
of bronchodilators”
“Combining bronchodilators with different mechanisms and durations of actions may increase the degree of bronchodilation for
equivalent or lesser side effects’’
GOLD Report 2003
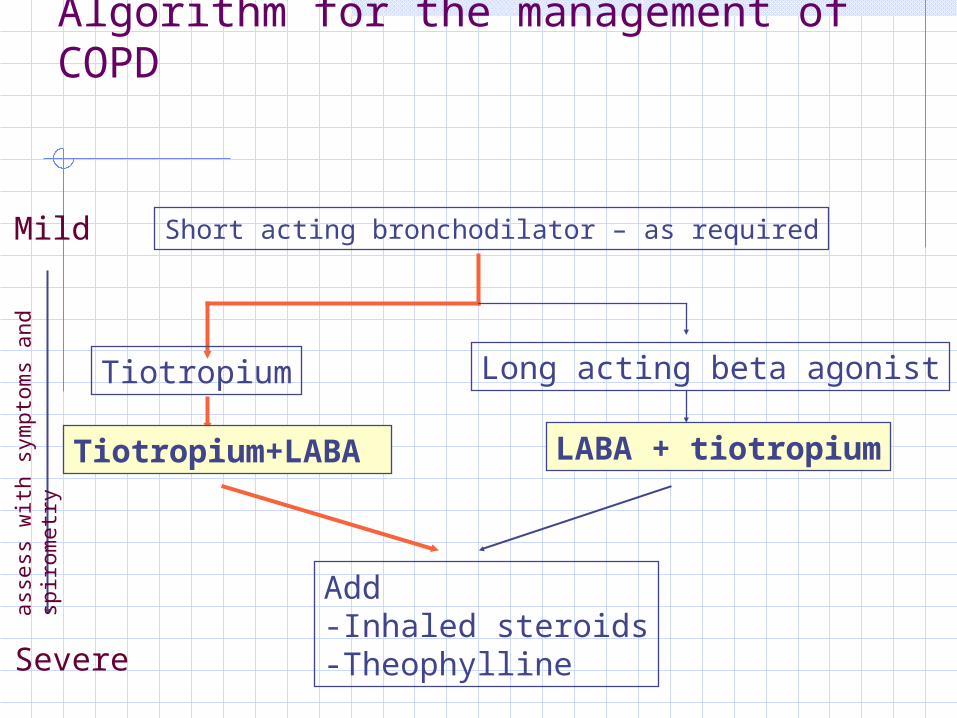
Algorithm for the management of COPD
Short acting bronchodilator – as required
Tiotropium
Tiotropium+LABA
Long acting beta agonist
LABA + tiotropium
Add-Inhaled steroids-Theophylline
Mild
Severe
ass
ess
wit
h s
ym
pto
ms
and
spir
om
etr
y










![Speleotherapy as an Effective Treatment of Chronic ... · Chronic obstructive pulmonary disease (COPD) is a chronic worldwide disease [1-4]. COPD COPD was supposed as the tenth most](https://static.fdocuments.in/doc/165x107/5cd3389988c99399578d07a7/speleotherapy-as-an-effective-treatment-of-chronic-chronic-obstructive-pulmonary.jpg)