Chronic Migraine: Observations from a Referral Headache Center President and CEO, The Carolina...
46
Chronic Migraine: Observations from a Referral Headache Center President and CEO, The Carolina Headache Foundation, Chapel Hill , NC Director, Carolina Headache Institute , Chapel Hill, NC Professor, University of North Carolina Contractor for Defense and Veteran Brain Injury Centers TNS Ft Worth 2015
-
Upload
willis-harrison -
Category
Documents
-
view
220 -
download
6
Transcript of Chronic Migraine: Observations from a Referral Headache Center President and CEO, The Carolina...

Chronic Migraine: Observations from a Referral
Headache Center
President and CEO, The Carolina Headache Foundation, Chapel Hill , NCDirector, Carolina Headache Institute , Chapel Hill, NC
Professor, University of North CarolinaContractor for Defense and Veteran Brain Injury Centers
TNS Ft Worth 2015

Disclosures
• With regards to this talk the speaker has no financial conflicts to Disclose– In the course of this talk I will mention off label
use of medications – THE ARE NO APPROVED TREATMENTS FOR MANY
OF THE HEADACHES I WILL DISCUSS

CHRONIC DAILY HEADACHE
4.1% of 13,000GeneralPublic
30%-80%Headache Clinic
Population
Scher Al et al. Headache. 1998.Sanin LC et al. Headache. 1993.

©International Headache Society 2003/5
1.5.1 Chronic migraine (ICHD-II +/- R1)New entrant to classification
A. Headache fulfilling criteria C and D for 1.1 Migraine without aura on 15 d/mo for >3 mo
B. Not attributed to another disorder

1.3 Chronic migraine (ICHD-3 beta)A. Headache (TTH-like and/or migraine-like) on ≥15 d/mo for >3
mo and fulfilling criteria B and C
B. In a patient who has had ≥5 attacks fulfilling criteria B-D for 1.1 Migraine without aura and/or criteria B and C for 1.2 Migraine with aura
C. On ≥8 d/mo for >3 mo fulfilling any of the following:1. criteria C and D for 1.1 Migraine without aura2. criteria B and C for 1.2 Migraine with aura3. believed by the patient to be migraine at onset and relieved by a triptan or ergot derivative
D. Not better accounted for by another ICHD-3 diagnosis

Which of which is Chronic Migraine?
0
5
10
Never goes away
0
5
10
Never goes away Comes and Goes

Is it a matter of scale?

Or Factors?Modifiable Non-modifiable (?)
Triggers (?) Gender/Age
Medication use (?overuse) Mood states/comorbidities
BMI (?) Trauma including abuse/neglect and PTSD
Sleep (snoring) (?) Concurrent illness – immune/inflammatory
Neck Pain (?) Comorbidites
? ?

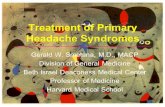
Distinguish Primary from Secondary Headache Disorders
Atypical Features
Investigations
Diagnosis
Headache
Secondary Headache
YesNoRed Flags
Primary Headache

History and examination
Systemic symptoms (fever, weight loss) or Secondary risk factors (HIV, cancer)Neurologic symptoms or signs Onset: abrupt, peak <1 minOlder: >50 (GCA; glaucoma)Previous headache history (new or change) Postural, positionalPrecipitated by Valsalva, exertion, etcPapilledema
Screen for red flags SNOOP4
Assess for worrisome signs and symptoms Look for atypical features
Step 1: Exclude Secondary HeadacheStep 1: Exclude Secondary Headache
Yes Evaluate for secondary headache

5-minute Examination of Headache Patient
• Vitals - every patient needs them (BP, temp, BMI)• Head and neck
– Palpate (skull base, TMJs, temporal arteries, upper cervical facets, pericranial muscles, paranasal sinuses)
– Listen (auscultate the head, orbits, and neck)• Focused neurological examination
– Talk to patient (mental status), watch them walk– Cranial nerves (fundi, visual fields, ocular motility, facial
symmetry, palate/tongue)– Upper motor neuron exam (arm extensor and leg flexor
strength, DTRs, plantar responses)

Diagnostic Criteria for Migraine vs. Tension-type Headache
Migraine Tension-type
Frequency Variable Variable
Duration 4-72 H 30 min – 7 days
Location Unilateral (40% bilateral) Bilateral
Description Pulsating (50% non-pulsating)
Pressing/tightening (nonpulsating)
Intensity Moderate-severe Mild-moderate
Effect of routine physical activity
Aggravated by or cause avoidance of
Not aggravated by
Nausea or vomiting Yes No
Photophobia or phonophobia
One or both No more than one
Attributable Not attributable to another disorder
Not attributable to another disorder
Headache Classification Subcommittee of the IHS. ICHD-III (beta). Cephalalgia. 2013; March.

Step 2: Identifying Primary Headache Syndrome
Episodic short duration headache <4 hours or
multiple discrete episodes
Episodic short duration headache <4 hours or
multiple discrete episodes
Episodic long duration headache
lasting >4 hours
Episodic long duration headache
lasting >4 hours
Episodic headache frequency <15 days/month
(eg, migraine)
Episodic headache frequency <15 days/month
(eg, migraine)
Identify primary headache syndrome
Identify primary headache syndrome
Chronic headachefrequency
≥15 days/month
Chronic headachefrequency
≥15 days/month
Tension-typeTension-typeMigraineMigraine

Progressive Headache
• When episodic migraine progresses, chronic migraine is the most likely diagnosis– Evolution of EM to CM
2.5% per year in general population• When is diagnostic testing necessary in progressive
headache?– Not always…Consider a therapeutic trial
• What is considered an adequate workup?– Neuroimaging?– Lumbar puncture?– Laboratory testing?

Comfort Signs that a Chronic Headache Condition is NOT Secondary Headache
• Long duration of illness• Typical clinical features• Family history of similar primary headache• Typical treatment response• Normal neurological examination• Menstrual exacerbations• Evolution of EM to CM with medication overuse

Differential Diagnosis of Primary Chronic Headache of Long Duration
Hemicrania Continua
New Daily Persistent HA
Chronic Tension Type
Chronic Migraine
Frequency ≥15 day/month ≥15 day/month ≥15 day/month ≥15 day/month
Duration Continuous Constant or intermittent
2-72 hours (H); constant or intermittent
4-72 H; constant or intermittent
PainHemicranial; steady ache; some throbbing
Like migraine or tension type headache (TTH); pressure
Like TH; tightening
Like migraine; throbbing
Associated symptoms
Ipsilateral, autonomic features
Variable NoneNausea, photophobia, Phonophobia
Treatment response Indomethacin Variable Variable Variable

Patient Characteristics Episodic Migraine Chronic MigraineHeadache frequency, days/month <15 ≥15
Report Severe headache pain (%) 78.1 92.4*
Duration of headache pain without medication (mean h)
38.8 65.1*
Duration of headache pain with medication (mean h)
12.8 24.1*
Patient Characteristics of EM vs CM
Headache: The Journal of Head and Face Pain pages 103-122, 6 FEB 2015 DOI: 10.1111/head.12505_2

Sociodemographic characteristics
EM CM
Race (% white) 87.3 90.7Women, % 80.0 78.6
Low household income (% < $22,500/year) 24.9 29.9*
Comorbidities Depression, % 17.2 30.2*Anxiety, % 18.8 30.2*Obesity, % 21.0 25.5*Cutaneous allodynia, % 63.2 68.3*
Headache: The Journal of Head and Face Pain pages 103-122, 6 FEB 2015 DOI: 10.1111/head.12505_2

TREATMENT: FDA Approved
Acute Management of Migraine Prevention of EM Prevention of CM
Triptans (oral, nasal, injectable, transdermal): almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan, zolmitriptan
Propranolol (tablets, liquid) OnabotulinumtoxinA injections
Timolol (tablets)
Divalproex sodium ERSodium valproate
Topiramate
Dihydroergotamine mesylate (tablets, nasal sprays)
Diclofenac potassium oral solutionTranscutaneous Supraorbital NeuroStimulation (tSNS) headband
Headache: The Journal of Head and Face Pain pages 103-122, 6 FEB 2015 DOI: 10.1111/head.12505_2

Current treatments• Neurotoxins• Medications
– Episodic migraine prevention for chronic migraine?
• Procedures– The worst of the worst?
• Multidisciplinary• Neil Raskin
– “You are intractable”

21
Acute Medication Overuse• A diagnosis of “Medication-
overuse Headache” (MOH) is NOT synonymous with medication overuse
• Acute medication overuse is a behavior, defined by days of medication talking
• MOH is headache attributed to the overuse of medications
Frequent Attacks
Acutetherapy
“Rebound”/ medication-overuse
headache
Treatment of suspected MOH involves the discontinuation of the overused medication(s) and initiation of preventive therapy

Figure Rates and odds ratios of transition from EM to CM by treatment efficacy category in the fully adjusted model (model 3)CI = confidence interval; CM = chronic migraine; EM = episodic
migraine; OR = odds ratio.
Richard B. Lipton et al. Neurology 2015;84:688-695
© 2015 American Academy of Neurology

Complete history and examinationComplete history and examination
Evaluate for secondary headache
Screen for red flags SNOOP
Screen for red flags SNOOP
Yes
Assess headache signs and symptoms & look for atypical features
Ste
p 1
: E
xclu
de
seco
nd
ary
hea
dac
he
Chronic headache of long duration
frequency ≥15 d/mheadache lasting >4
hours
Chronic headache of long duration
frequency ≥15 d/mheadache lasting >4
hours
Episodic headache of long duration
frequency <15 d/m >4 hours
Episodic headache of long duration
frequency <15 d/m >4 hours
YesIf headache frequency & severity
are progressing, watch for and warn against risks for chronic migraine
Identify primary headache syndromeIdentify primary headache syndrome
No
Assess for acutemedication overuse
Assess for acutemedication overuse
Ste
p 2
: Id
enti
fy p
rim
ary
hea
dac
he
syn
dro
me
MigraineMigrainous
Tension-type
MigraineMigrainous
Tension-type
Chronic migraineChronic tension-type
NDPHHemicrania continua
Chronic migraineChronic tension-type
NDPHHemicrania continua
Ste
p 3
: D
iag
no
se s
pec
ific
h
ead
ach
e d
iso
rder

Refractory Headache
• Continuous Headache• New Daily Persistent Headache• Side Locked Headache• Focal Headache
– With migraine features– Without migraine features
• Stress and Distress

Headache Index
In the last 28 days I had (write a best guess number in each blank below):
_______ Days where my worst headache was severe+_______ Days where my worst headache was moderate+_______ Days where my worst headache was mild +_______ Days with absolutely no headache, neck discomfort,
facial/ jaw discomfort whatsoever?TOTAL= ________ (total should equal 28)

Pain Diagrams
FRONT BACK
SIDE

Continuous Headache
• Is it really?• Is it severe?• Is it Migraine?
– If not……………………– What?
• Is it a headache?

New Daily Persistent Headache
• Is it really new?– Prior history of headache– How should we ask?
• Leading the witness• Following the leads
• Does it have to be continuous?• Is it a primary headache disorder?

THE 50% RULE?
If in many of your patient’s with NDPH you find SOMETHING
Then: Is NDPH an Other Primary Headache?

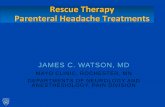
Comorbidities and Predictive Factors in NDPH
Infection39%
Trauma25%
Rheumatologic8%
Surgery3%
Vaccine3%
None22%
Preceding Event
Hindiyeh, N et al, Presented at the 56th Annual Scientific Meeting of the AHS, 27JUN2014
n = 3678% HAD SOMETHING

Side Locked Headache
• Location– Surface area– Radiation– Associations
• Duration– TAC?
• Interictal headache
– HC w &w/o features

Side Locked Headache
• Severity• Examination findings
– Hyperesthesia– Hypalgesia– TMD/TMJ– Cervicogenic
• Primary• Secondary

Side Locked Headache• Cervicogenic (11.2.1)
– Primary– Secondary
OR
• Is it 11.2.3 (Headache Attributed to Craniocervical Dystonia– Inclinometry

Focal Headache
• Without migraine features– Nummular headache– Neuralgiform pain
• With migraine features– Peripheral v central sensitization– Phantom head pain

Stress and Distress
• Diseases and drugs– If nothing works– Then do we know what we are treating?
• Don’t ask….Don’t tell• Testing for distress
– P_SD?– Aphysiology
• What to do when there is no on else to care!

What To Do?
• Examine the history– I have notes – quality?– If available look at headache calendars (some
actually keep them on their own)• Examine the treatments
– Drugs that did work• What if daily triptans render them headache free?
– Drugs that didn’t work• Dosing, etc.
– Drugs that might work– Drugs that don’t work !!!

What Do I Do?- Biopsychosocial Models• Examine the patient
– The neurologic examination is GROSS– Test, touch and move
• The sensory examination of the head– Named nerves
» GON/LON, Supraauricular/Superficial Temporal/SON– Inject if necessary
• TM Joints?• Cervical ROM
– Inclinometry?

Biopsychosocial ModelsUse validated instruments - Adapt as necessary
• Lot’s of neurologic stuff: Neurobehavioral Symptom Index (NSI)
• PTSD = Post Traumatic Checklist – Civilian (PCL-C)
• Mood/Behavioral– Patient Catastrophizing Scale (PSC)– BAI, BDI

Current treatments• Neurotoxins• Medications
– Episodic migraine prevention for chronic migraine?
• Procedures– The worst of the worst?
• Multidisciplinary• Neil Raskin
– “You are intractable”

The Goal• Validate the Model
– Is the patient credible?• The best evidence still exists for N= 1• 1 is the loneliest #
– Are there confounds?• Medical
– ?MOH
• Behavioral– “Intractability”– Is the HEADACHE credible?*******************
• AND THEN

What Do I Do?Biopsychosocial Models
• Examine the history– Phenomenology: What would it be if it could be?
• Examine the patient– Include the mind: What would it do if it could do?
• Examine myself– “we were people before we were clinicians”
• Defaults• Heuristics

What Do I Do?Biopsychosocial Models
• Examine the patient – Psycho Social– I was not trained to look into people’s souls
• Use validated instruments• Adapt as necessary

What Do I Do?Biopsychosocial Models
• Examine myself– “we were people before we were clinicians”
• Heuristics• Defaults
– MOH– Psychology and the soul

Conclusions – What should we ALL do?
• Chronic migraine is the same no matter where I see it
• Manage people– Not drugs
• Include your biases - Intractability– Cathexis
• Treat what you think/know
– Counter – transference• Not what you feel

Conclusions
• The refractory headache patient is:– Challenging– Exciting– Frustrating
• And
– Satisfying

Thank you for your attention
President and CEO, The Carolina Headache Foundation, Chapel Hill , NCDirector, Carolina Headache Institute , Chapel Hill, NC
Professor, University of North CarolinaContractor, Defense and Veteran Brain Injury Center
TNS 2015