Chronic Kidney Disease: Chronic Kidney Disease (CKD) · Hypervolemia Hypovolemia 34 Principles of...
8
Robert N. Sladen, MBChB, FCCM Allen Hyman Professor of Critical Care Anesthesiology Executive Vice-Chair Chief, Division of Critical Care Director, CTICU and SICU Department of Anesthesiology Columbia University Medical Center New York, NY Chronic Kidney Disease: The Silent Killer? No Disclosures 1 What is Chronic Kidney Disease? 2 Chronic Kidney Disease (CKD) • Functional or structural kidney damage - eGFR < 60 mL / min /1.73 m 2 x 3 months • United States: > 20 m affected (7%) - 47% of individuals > 70 yrs - End-stage renal disease (RRT): > 500 k • Risk factors: diabetes; hypertension (90%) - Risk of dying of CV disease in older patients with CKD is greater than risk of needing RRT! Drawz P et al. Ann Intern Med 2009;150:ITC2-1-15 3 Modification of Diet in Renal Disease (MDRD) http://www.nkdep.nih.gov eGFR = 186 x (S cr ) -1.154 x (Age) -0.203 x 0.742 (if female); x 1.212 (if African-American) National Kidney Disease Education Program Estimated GFR (eGFR) 4 For example: 64 yr-old woman, baseline SCr 1.9 mg/dL eGFR = 186 x (1.9) -1.154 x (64) -0.203 x (0.742) Estimated GFR (MDRD) eGFR = 26.6 mL / min /1.73m 2 http://www.mdcalc.com/mdrd-gfr-equation/ How severe is her CKD? 5 National Kidney Foundation (NKF) Kidney Disease Outcomes QI Classification CKD Stage eGFR (mL/min/1.73M 2 ) Description 1 > 90 Kidney damage with NL GFR 2 60 - 89 Mildly decreased GFR 3a 45 - 59 Moderately decreased GFR 3b 30 - 44 Moderately severe decrease 4 15 - 29 Severely decreased GFR 5 < 15 (or RRT) End-stage kidney disease Levey AS et al. Ann Intern Med 2003; 139: 137-47 6 National Kidney Foundation (NKF) Kidney Disease Outcomes QI Classification CKD Stage eGFR (mL/min/1.73M 2 ) Description 1 > 90 Kidney damage with NL GFR 2 60 - 89 Mildly decreased GFR 3 < 60 Moderately decreased GFR 4 < 30 Severely decreased GFR 5 < 15 Kidney failure Levey AS et al. Ann Intern Med 2003; 139: 137-47 7 For example: 64 yr-old woman, baseline SCr 1.9 mg/dL eGFR = 186 x (1.9) -1.154 x (64) -0.203 x (0.742) Estimated GFR (MDRD) eGFR = 26.6 mL / min /1.73m 2 http://www.mdcalc.com/mdrd-gfr-equation/ She has Stage 4 CKD … 8 Go AS et al. N Engl J Med 2004; 351:1296-1305 1.12 m adults without dialysis or transplantation Risk of CKD CV Events 1, 2 3a 3b 4 5 Hospitalization Death 9 CKD CRASH 2-16 - January 24, 2016 Sladen, Robert, MBChB, FCCM Chronic Kidney Disease
Transcript of Chronic Kidney Disease: Chronic Kidney Disease (CKD) · Hypervolemia Hypovolemia 34 Principles of...

Robert N. Sladen, MBChB, FCCM
Allen Hyman Professor of Critical Care Anesthesiology
Executive Vice-ChairChief, Division of Critical Care
Director, CTICU and SICUDepartment of Anesthesiology
Columbia University Medical CenterNew York, NY
Chronic Kidney Disease:The Silent Killer?
No Disclosures
1
What is Chronic Kidney Disease?
2
Chronic Kidney Disease (CKD)
• Functional or structural kidney damage
- eGFR < 60 mL / min /1.73 m2 x 3 months
• United States: > 20 m affected (7%)
- 47% of individuals > 70 yrs
- End-stage renal disease (RRT): > 500 k
• Risk factors: diabetes; hypertension (90%)
- Risk of dying of CV disease in older patients with CKD is greater than risk of needing RRT!
Drawz P et al. Ann Intern Med 2009;150:ITC2-1-15
3
Modification of Diet in Renal Disease (MDRD)
http://www.nkdep.nih.gov
eGFR = 186 x (Scr)-1.154 x (Age)-0.203
x 0.742 (if female); x 1.212 (if African-American)
National Kidney Disease Education Program
Estimated GFR (eGFR)
4
For example: 64 yr-old woman, baseline SCr 1.9 mg/dL
eGFR = 186 x (1.9)-1.154 x (64)-0.203 x (0.742)
Estimated GFR (MDRD)
eGFR = 26.6 mL / min /1.73m2
http://www.mdcalc.com/mdrd-gfr-equation/
How severe is her CKD?
5
National Kidney Foundation (NKF)
Kidney Disease Outcomes QI Classification
CKDStage
eGFR (mL/min/1.73M2)
Description
1 > 90 Kidney damage with NL GFR
2 60 - 89 Mildly decreased GFR
3a 45 - 59 Moderately decreased GFR
3b 30 - 44 Moderately severe decrease
4 15 - 29 Severely decreased GFR
5 < 15 (or RRT) End-stage kidney disease
Levey AS et al. Ann Intern Med 2003; 139: 137-47
6
National Kidney Foundation (NKF) Kidney Disease Outcomes QI Classification
CKDStage
eGFR (mL/min/1.73M2) Description
1 > 90 Kidney damage with NL GFR
2 60 - 89 Mildly decreased GFR
3 < 60 Moderately decreased GFR
4 < 30 Severely decreased GFR
5 < 15 Kidney failure
Levey AS et al. Ann Intern Med 2003; 139: 137-47
7
For example: 64 yr-old woman, baseline SCr 1.9 mg/dL
eGFR = 186 x (1.9)-1.154 x (64)-0.203 x (0.742)
Estimated GFR (MDRD)
eGFR = 26.6 mL / min /1.73m2
http://www.mdcalc.com/mdrd-gfr-equation/
She has Stage 4 CKD …
8
Go AS et al. N Engl J Med 2004; 351:1296-1305
1.12 m adults without dialysis or transplantation
Risk of CKDCV Events
1, 23a
3b
4
5
HospitalizationDeath
9CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease
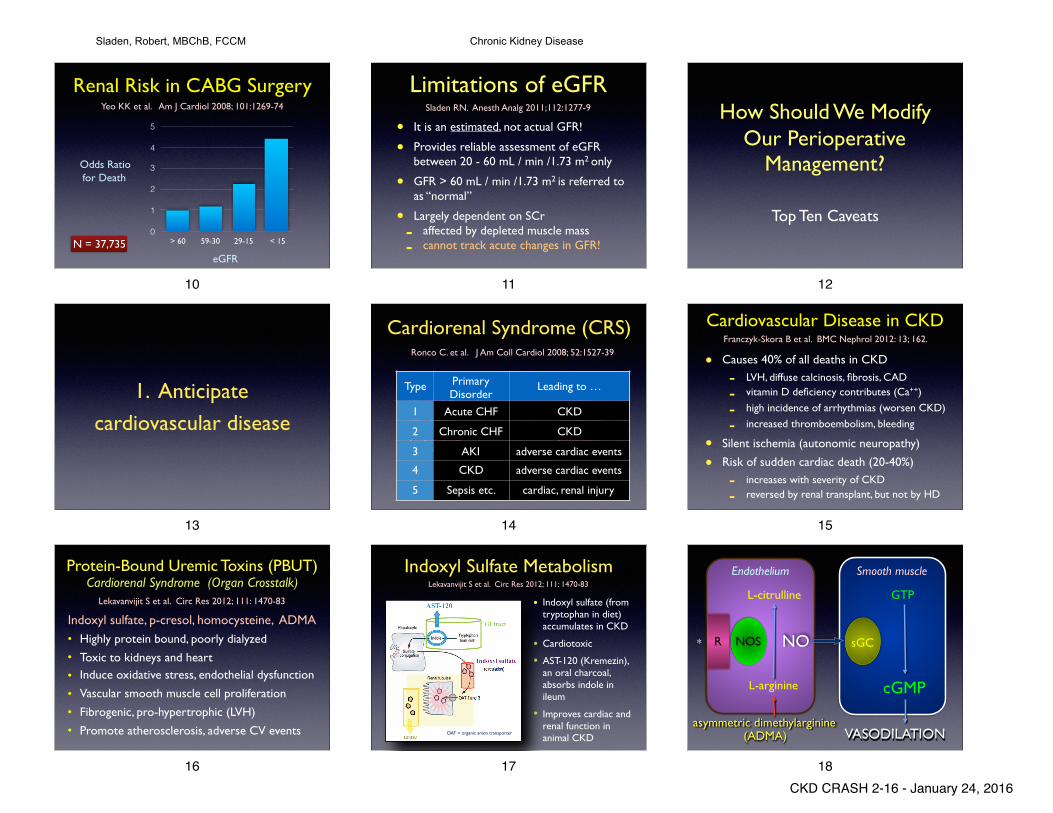
Renal Risk in CABG SurgeryYeo KK et al. Am J Cardiol 2008; 101:1269-74
N = 37,7350
1
2
3
4
5
> 60 59-30 29-15 < 15
Odds Ratiofor Death
eGFR
10
Limitations of eGFR
• It is an estimated, not actual GFR!
• Provides reliable assessment of eGFR between 20 - 60 mL / min /1.73 m2 only
• GFR > 60 mL / min /1.73 m2 is referred to as “normal”
• Largely dependent on SCr
- affected by depleted muscle mass
- cannot track acute changes in GFR!
Sladen RN. Anesth Analg 2011;112:1277-9
11
How Should We Modify Our Perioperative
Management?
Top Ten Caveats
12
1. Anticipate
cardiovascular disease
13
Cardiorenal Syndrome (CRS)Ronco C. et al. J Am Coll Cardiol 2008; 52:1527-39
Type Primary Disorder
Leading to …
1 Acute CHF CKD
2 Chronic CHF CKD
3 AKI adverse cardiac events
4 CKD adverse cardiac events
5 Sepsis etc. cardiac, renal injury
14
Cardiovascular Disease in CKD
• Causes 40% of all deaths in CKD
- LVH, diffuse calcinosis, fibrosis, CAD
- vitamin D deficiency contributes (Ca++)
- high incidence of arrhythmias (worsen CKD)
- increased thromboembolism, bleeding
• Silent ischemia (autonomic neuropathy)
• Risk of sudden cardiac death (20-40%)
- increases with severity of CKD
- reversed by renal transplant, but not by HD
Franczyk-Skora B et al. BMC Nephrol 2012: 13; 162.
15
• Highly protein bound, poorly dialyzed
• Toxic to kidneys and heart
• Induce oxidative stress, endothelial dysfunction
• Vascular smooth muscle cell proliferation
• Fibrogenic, pro-hypertrophic (LVH)
• Promote atherosclerosis, adverse CV events
Lekavanvijit S et al. Circ Res 2012; 111: 1470-83
Protein-Bound Uremic Toxins (PBUT) Cardiorenal Syndrome (Organ Crosstalk)
Indoxyl sulfate, p-cresol, homocysteine, ADMA
16
Indoxyl Sulfate Metabolism
• Indoxyl sulfate (from tryptophan in diet) accumulates in CKD
• Cardiotoxic
• AST-120 (Kremezin), an oral charcoal, absorbs indole in ileum
• Improves cardiac and renal function in animal CKD
Lekavanvijit S et al. Circ Res 2012; 111: 1470-83
OAT = organic anion transporter
17
O
Endothelium Smooth muscle
R NOS
L-arginine
L-citrulline
sGC
GTP
cGMP
NO
VASODILATION
*
asymmetric dimethylarginine(ADMA)
18CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease

Diastolic Dysfunction in CKD
• Common in CKD especially with HTN
- LVH, diffuse calcinosis, fibrosis, CAD
- increases with grade of CKD (85% stage 4-5)
• LV ejection fraction > 50%
- impaired diastolic relaxation
- evaluated by transthoracic echocardiogram
- requires higher filling pressure, slower HR
• Increased risk of cardiac mortality
Farshid A et al. BMC Nephrol 2013: 14; 280.
19
Sudden Cardiac Death (SCD)
• SV, V arrhythmias - 80-90% of patients on HD
- cardiac fibrosis, sympathetic hyperactivity
• Exacerbated during HD and hours afterwards- 50% of all deaths in HD patients
• Prolonged QT - iron overload and deposition
- Torsades des pointes, VF, asystole
- electrolyte shifts - hypokalemia, hypomagnesemia
- catecholamine bursts (hypovolemia, HD)
- drugs: antidepressants, droperidol, ciprofloxacin
Franczyk-Skora B et al. BMC Nephrol 2012: 13; 162.
20
Torsades de Pointes“Twisting of the Points”
Yap YG, Cam AJ. Heart 2003; 89: 1363-72
Multifocal ventricular tachycardia
• Prolonged QT
• Low K, Mg
• Catecholamines
• Drugs
- haloperidol
- droperidol
21
SCD: Prophylaxis
•Beta blockade
•Statins
•RAAS blockade
•AICD
Whitman IR et al. JASN 2012 23; 1929-39
22
Do A Cardiac Workup!
• Careful history (DM, HTN, CAD, arrhythmias)
• Look for anemia (EPO, iron, folate, GIB)
• ECG (QT, conduction problems, arrhythmias)
• TTE (LVH, diastolic dysfunction, CHF)
• Perioperative beta blockade
• Cardioprotective anesthetic, emergence
23
2. Anticipate autonomic neuropathy
24
Autonomic Neuropathy in CKD
• Delayed gastric emptying (aspiration risk)
• Silent myocardial ischemia
• Orthostatic hypotension
Accompanies peripheral neuropathy
25
3. Anticipate Acidosis and Hyperkalemia
26
Metabolic Acidosis in CKD
• Early: hyperchloremic acidosis- tubular HCO3 wasting
• Late: anion gap acidosis- sulfate, phosphate accumulation
• Acute on chronic acidosis- hypercarbia, shock, diarrhea, stress
27CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease

Acid-Base Management
• Check preoperative HCO3 and Cl
- hyperchloremic vs. anion gap acidosis
• Support ventilatory compensation
- increase minute ventilation in OR
- consider postoperative ventilation
• Recognize relationship to potassium
28
Potassium Balance
∆ pH 0.1 ➜ ∆ K+ 0.5 mEq/L
K+ [160] K+ [4]Na ATPase
H+
K+
β-agonists
insulin
29
Perioperative Acidosis35 yr old diabetic, cadaveric renal transplant
PaCO2 pH HCO3 K+
Preop 32 7.32 17 5
OR 40 7.25 18 5.3
PACU 44 7.21 19 5.6
PACU 48 7.18 19 5.9
30
Acute Hyperkalemia in CKD• Acute acidosis• Catabolic stress• Major trauma, surgery, sepsis• Drugs
- NSAIDs, ACE inhibitors- K - sparing diuretics- β-blockers- Cyclosporin A, tacrolimus
31
Hyperkalemia Protocol
Calcium chloride 1-2 g central IV
NaHCO3 50 - 100 mEq
Hyperventilate 0.1 pH = 0.5 K+
Insulin + glucose 5u + 25g (50 mL 50%)
Kayexalate enema 0.5 g/kg
Emergency dialysis If K+ > 6.0 mEq/L
32
4. Anticipate Acute Fluid Overload and Pulmonary Edema
33
Depleted Fluid Reserve
• Anuria- excess Na: edema, HTN- excess H2O: hyponatremia
• Nonoliguric, polyuric- unable to concentrate urine
Hypervolemia Hypovolemia
34
Principles of Fluid Management
• Correct fluid deficits
• Restrict maintenance fluid
• Monitor appropriately
• Be careful post-operatively!- withdrawal of positive pressure - reversal of sympathetic block
35
5. Anticipate Anemia and Bleeding
36CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease

Hematologic Impact of CKD
• Chronic anemia
- erythropoietin deficiency
- chronic blood loss (HD, GIB)
- iron, folate deficiency
• Uremic thrombocytopathy
- platelet dysfunction (normal count)
- care with regional, axial anesthesia
37
Erythropoietin and CKD
• CKD-induced cardiac dysfunction
- pro-inflammatory cytokines
- anti-erythrocytic circulating factors
• Erythropoietin therapy
- anti-inflammatory, anti-oxidative
- decreased LVH, fibrosis, BNP
- excess: CVA, MI, thrombosis, ESRD, death
Arcasoy M. Br J Haematol 2008; 141:14-31
38
Uremic Thrombocytopathy
vWF
VIII
vWF VIII
platelets
Urea−
endothelium
Acquired von Willebrand’s Disease
39
Uremic Thrombocytopathy
vWF
VIII
vWF VIII
platelets
Urea−
endothelium
Acquired von Willebrand’s Disease
PressorAmines
+
40
Desmopressin (DDAVP)
• Derivative of arginine vasopressin (AVP)
- vasodilator, long-acting
• 0.3 µg/kg IV over 15-20 min (hypotension)
• Improves platelet function for 1-12 hr
• Releases vWF-VIII from endothelium
- tachyphylaxis with repeat doses
- not effective with ongoing pressor therapy
8-deamino D-arginine vasopressin
41
Cryoprecipitate• Patients exposed to amines
- NE, EPI, AVP
• Recent administration of DDAVP
• Contains VWF, Factor VIII
- also fibrinogen, Factor XIII
42
6. Anticipate renal osteodystrophy
43
Vitamin D Deficiency and CKDChonchol M et al. Ann Med 2011; 43:273-82
Vitamin D3 - cholecalciferol
• Decreased intake of dairy products
- phosphate restriction
• Decreased sunlight exposure
• Vitamin D loss with proteinuria
• Vitamin D loss in dialysate
25-OH D < 30 ng/mL
44
Vitamin D Deficiency and CKD
25-OH D 1,25-OH2 D
1-alpha hydroxylase(kidney)
anti-inflammatory innate immunity
healthy bones & joints
Chonchol M et al. Ann Med 2011; 43:273-82
less active more active
CVDinfection
osteoporosis
Vitamin D3 - cholecalciferol
X45
CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease
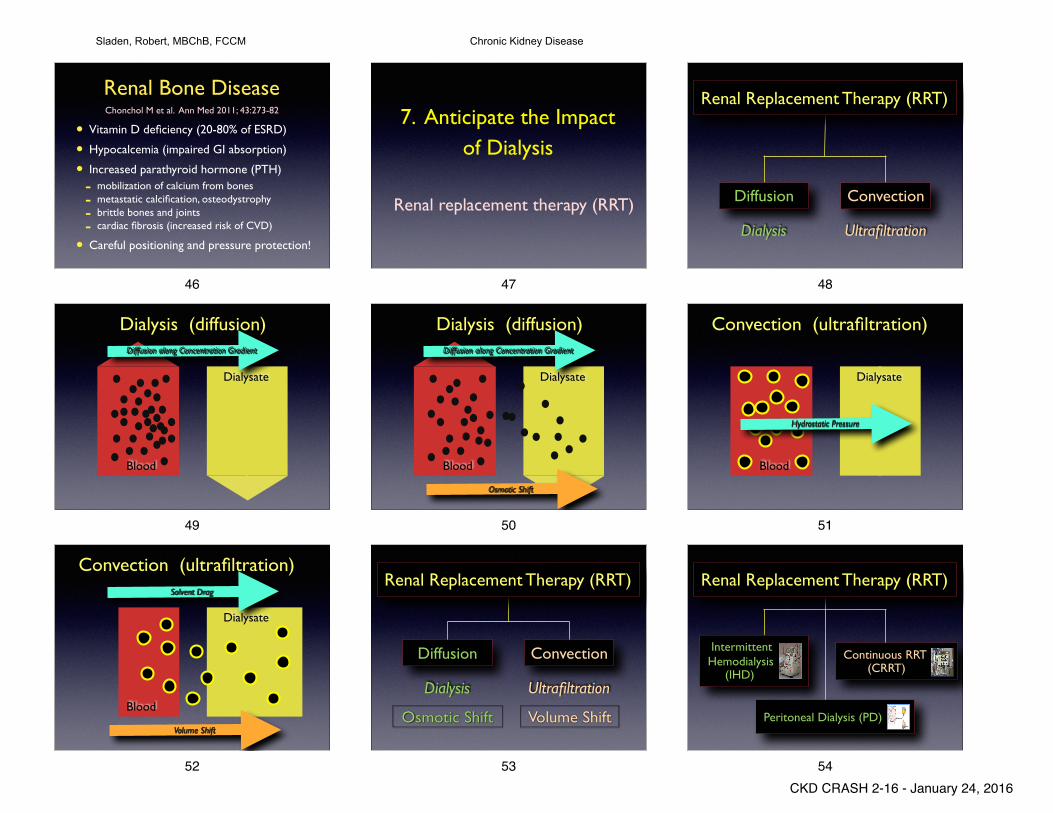
Renal Bone Disease
• Vitamin D deficiency (20-80% of ESRD)
• Hypocalcemia (impaired GI absorption)
• Increased parathyroid hormone (PTH)
- mobilization of calcium from bones- metastatic calcification, osteodystrophy- brittle bones and joints- cardiac fibrosis (increased risk of CVD)
• Careful positioning and pressure protection!
Chonchol M et al. Ann Med 2011; 43:273-82
46
7. Anticipate the Impact of Dialysis
Renal replacement therapy (RRT)
47
Diffusion Convection
Dialysis Ultrafiltration
Renal Replacement Therapy (RRT)
48
Dialysis (diffusion)
Blood
Dialysate
Diffusion along Concentration Gradient
49
Dialysis (diffusion)
Blood
Dialysate
Diffusion along Concentration Gradient
Osmotic Shift
50
Convection (ultrafiltration)
Blood
Dialysate
Hydrostatic Pressure
51
Blood
Dialysate
Solvent Drag
Volume Shift
Convection (ultrafiltration)
52
Diffusion Convection
Dialysis Ultrafiltration
Renal Replacement Therapy (RRT)
Osmotic Shift Volume Shift
53
Renal Replacement Therapy (RRT)
Peritoneal Dialysis (PD)
Continuous RRT (CRRT)
Intermittent Hemodialysis (IHD)
54CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease

What Dialysis Does Well
• Pulmonary edema
• Hyperkalemia, acidosis
• Acute uremia:- encephalopathy- enteropathy- serositis- thrombocytopathy
Controls manifestations of acute uremia
55
• Cardiovascular complications (SCD)• Anemia• Renal osteodystrophy• Peripheral neuropathy• Impaired resistance to sepsis• Poor wound healing
What Dialysis Does PoorlyControls manifestations of chronic uremia
56
Timing of Preoperative Dialysis• Ideal: afternoon, the day before surgery!
• Adverse effects of dialysis:
- AV shunt (low SVR)
- hypovolemia, hypotension, SCD
- electrolyte imbalance (K, Mg, Pi)
- myocardial ischemia, arrhythmias
- dysequilibrium syndrome
- residual anticoagulation
57
8. Anticipate delayed emergence and persistent neuromuscular blockade
58
Renal Drug Disposition• Few drugs are totally renal dependent
- aminoglycosides, digoxin
• Many drugs are partially renal dependent (decrease maintenance doses)
- metformin, cimetidine, penicillin, milrinone
- pancuronium, vecuronium, rocuronium
- atropine, glycopyrrolate, neostigmine
• Some drugs have active metabolites- morphine, meperidine, vecuronium
59
Rocuronium
• Elimination is independent of renal function
• Pharmacodynamic data are conflicting
- no difference, prolonged action, variable
• Immediately inactivated by sugammadex
- complex is excreted by kidneys
Robertson EN et al. Eur J Anaesthesiol 2005; 22: 929-32Robertson EN et al. Eur J Anaesthesiol 2005; 22: 4-10
60
Morphine
Morphine-3-G
80%
antianalgesic
Morphine-6-G
10%
analgesic (40 x potency)
excreted in urine
John Sear, Oxford
Normorphine
neuroexcitatory
61
Drugs Cleared in the Blood
Drug Mechanism
succinylcholine PChE
esmolol RBC esterase
cisatracurium Hoffman
remifentanil esterase
clevidipine esterase
62
9. Anticipate nausea, vomiting, aspiration
and perioperative GI bleeding
63CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease
Gastrointestinal Disease and CKD
• Delayed gastric emptying (aspiration risk)
- autonomic neuropathy
• GI Bleeding (increased risk and mortality):
- peptic ulcer disease (25%)
- erosive esophagitis, gastritis, duodenitis
- ischemic colitis (IHD)
- thrombocytopathy (normal count)
• Risk increases with stage of CKD
Thomas R et al. Ren Fail 2012, Oct 18 (ePub)
64
10. Anticipate Postoperative
Complications
65
Postop Complications• Acute kidney injury (AKI on CKD)
• Myocardial ischemia, arrhythmias
• Postoperative pneumonia
• Inability to tolerate hemodialysis
• Poor wound healing and wound infection
• Prolonged ICU length of stay
66
CKDis a multisystem disease - and can be a silent killer!
Be careful out there!
The Bottom Line
67
Good Luck !!
68
69
CKD CRASH 2-16 - January 24, 2016
Sladen, Robert, MBChB, FCCM Chronic Kidney Disease