
Chronic hepatitis and management of chronic hepatitis b and
45
CHRONIC HEPATITIS AND MANAGEMENT OF CHRONIC HEPATITIS-B AND C DR ANSUMAN DASH GUIDE – DR. S. K. SETHI
-
Upload
ansuman-dash -
Category
Health & Medicine
-
view
126 -
download
2
Transcript of Chronic hepatitis and management of chronic hepatitis b and

CHRONIC HEPATITIS AND
MANAGEMENT OF CHRONIC
HEPATITIS-B AND C
DR ANSUMAN DASH
GUIDE – DR. S. K. SETHI

INTRODUCTION
• Chronic hepatitis represents a series of liver disordersof varying causes and severity in which hepaticinflammation and necrosis continue for at least 6months.
• Milder forms are non-progressive or only slowlyprogressive, while more severe forms may beassociated with scarring and architecturalreorganization, which, when advanced, leadultimately to cirrhosis.

CLASSIFICATION
OLD CLASSIFICATION
CHRONIC PERSISTENT HEPATITIS
CHRONIC LOBULAR HEPATITIS
CHRONIC ACTIVE HEPATITIS
It was based on histopathological distinction
NEW CLASSIFICATION
CAUSE
GRADE
STAGE

CLASSIFICATION BY CAUSE :-
TYPE OF HEPATITIS DIAGNOSTIC TEST
Chronic hepatitis B HBsAg, IgG Anti-HBc, HBeAg,HBV DNA
Chronic hepatitis C Anti-HCV, HCV RNA
Chronic hepatitis D Anti-HDV, HDV RNA, HBsAg, IgG Anti-HBc
Autoimmune hepatitis ANA , Anti-LKM1, Hyperglobulinemia
Drug induced hepatitis
Cryptogenic hepatitis All tests negative

CLASSIFICATION BY STAGE
PATHOGENESIS
Direct injury
Immune mediated injury to hepatocyte or biliary epithelium
Promotion of fibrosis


COMMON CLINICAL FEATURES
Hepatitis B
Infection of liver parenchymal cells caused by HBV.
Also known as Serum hepatitis.
Incubation period is long (30 – 180 days).
WHO estimates that 400 million people worldwide are chronicHBV carriers.
India has about 40 million HBV infected patients according toILBS.
Transmission may be horizontal i.e. by exposure to infected bloodor blood products, by needle sharing, sexual transmission or byoccupational exposure.
Vertical or Perinatal transmission.

Slide 4
1. WHO. Hepatitis B. 2002. 2. Custer B, et al. J ClinGastroenterol. 2004;38(10 suppl):S158. 3. WHO/WPRO data.
HBsAg Prevalence (%)1
High
Intermediate < Low
Country HBsAg+ (%)
China 5.3-122
South Korea 2.6-5.12
India 2.4-4.72
Taiwan 10-13.82
Vietnam 5.7-102
Japan 4.4-133
Africa 5-192
Russia 1.4-82
US/Europe 0.3-122
Geographic Distribution of Chronic HBV Infection
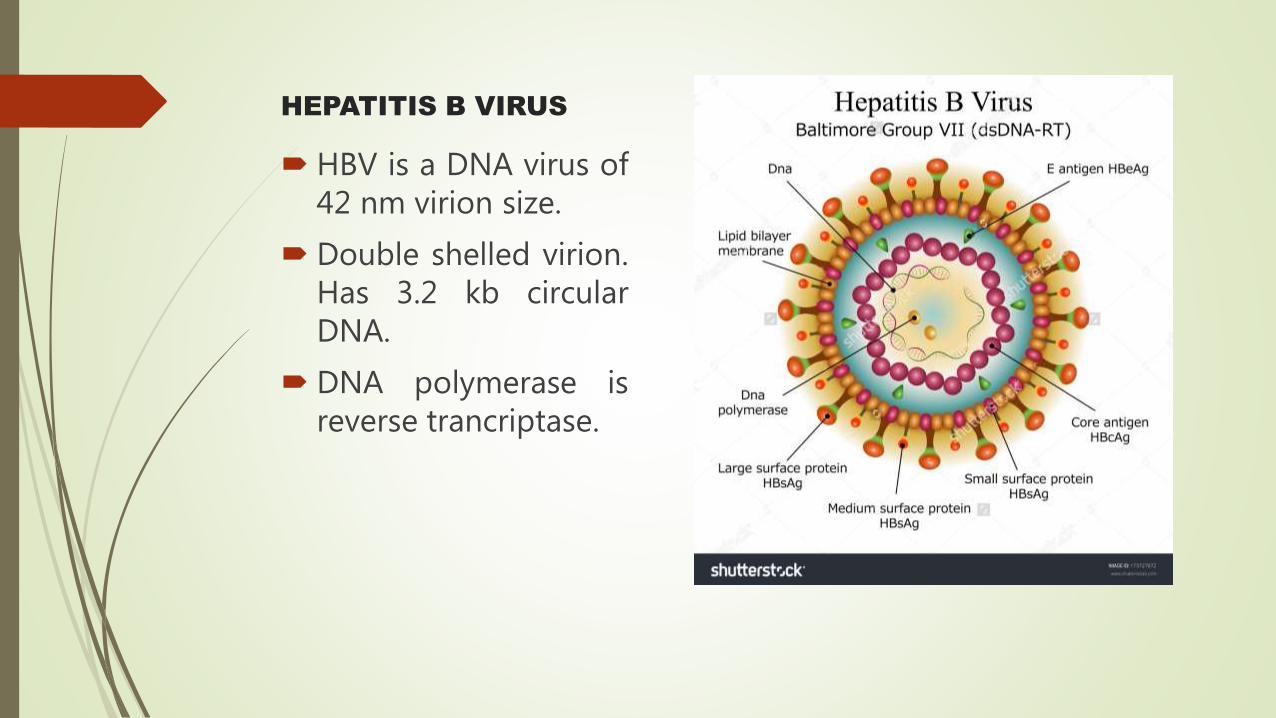
HEPATITIS B VIRUS
HBV is a DNA virus of42 nm virion size.
Double shelled virion.Has 3.2 kb circularDNA.
DNA polymerase isreverse trancriptase.

RISK FACTORS
Horizontal transmission in mainly low endemic areas by exposure to infected blood or other body fluids(sexual route), needle sharing among IV drug abusers, occupational exposure to infected blood or blood products, persons receiving transfusion of infected blood, hemodialysis patients
Vertical transmission mainly in high endemic areas by perinatal transmission from HBsAg +vemothers.

PATHOGENESIS OF HBV
Infection occurs in liver where necrosis probably results from cytotoxic T-cell response,
direct cytopathic effect of HBcAg and high level of HBsAg expression.

PHASES OF HEPATITIS B
INFECTION

WORK UP
Liver function test- ALT & AST usually around 1000 U/L at the onset of jaundice.
CBC
Hepatitis B serology i.e. HBsAg, Anti HBs, HBeAg, Anti Hbe, Anti HBc
Liver Biopsy rarely indicated
USG – to document reduction in liver size ar detect any mass.
Fibroscan (Transient elastography)

Acute HBV Typical serological course

Significance of serological markers

Clinical course of HBV
Acute hepatitis B infection
Chronic HBV infection
3-5% of adult-acquired infections
95% of infant-acquired infections
Cirrhosis
Chronic hepatitis
12-25% in 5 years
Liver failureHepatocellular carcinoma
6-15% in 5 years 20-23% in 5 years

TREATMENT
Main goal of treatment of Chronic Hepatitis B is to prevent progression to cirrhosis , hepatic failure and HCC.
7 drugs have been approved to date
Injectable Interferon α,
Pegylated Interferon(PEG)
Lamivudine,
Adefovir,
Entecavir,
Telbivudine,
Tenofovir.

INTERFERONS
Antiviral, antiproliferative and immunomodulatory effects.
IFN-α and -β bind to the same receptor and havepredominantly antiviral effects.
Pegylation reduces rate of absorption,renal clearance,decreases immunogenecity and increases half life.
The recommended dose is 180 μg weekly for 48 weeks.
PegIFN-α2a monotherapy was superior to lamivudinemonotherapy in inducing HBeAg seroconversion.
a/e include initial flu like illness, fever, chills, headache,malaise, myalgia, emotional liability.
The strongest predictor of response in HBeAg+ patients ispretreatment ALT level. other being histologic activity, lowHBV DNA level.
LAMIVUDINE
Nucleoside analogue.
Effective in suppressing HBV replication.
Recommended dose for adults with normal renal function (creatinine clearance >50 mL/min) and no HIV infection is 100 mg daily PO
ADEFOVIR DIPIVOXIL
Inhibit reverse transcriptase Effective in lamivudine-resistant HBV 10 mg daily PO
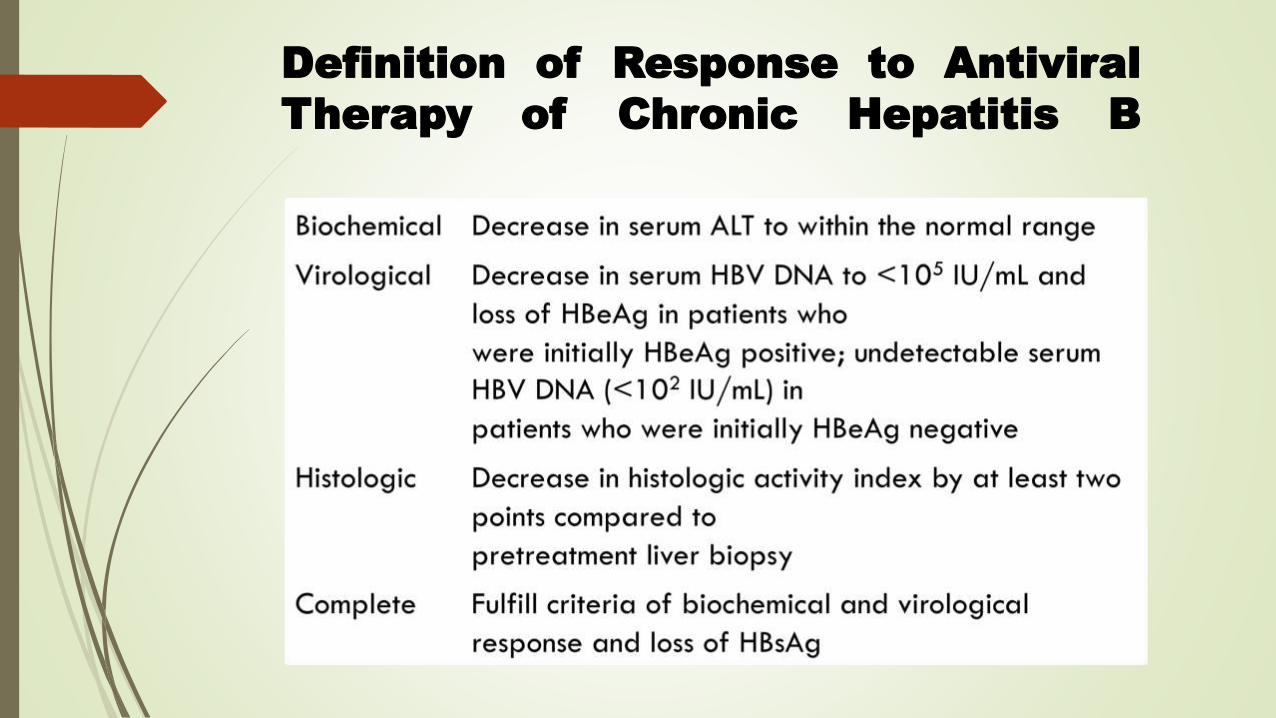
Definition of Response to Antiviral
Therapy of Chronic Hepatitis B

Chronic Hepatitis C
Infection of liver parenchyma caused by Hepatitis C virus (ssRNA Flavivirus).
Also known as Transfusion related non-A , non – B hepatitis.
Incubation period is average 6 weeks.
HCV infects more than 185 million individuals worldwide.
Global studies estimate that there are 8.7 million people living with chronic HCV in India.
Shows slight male predominance with highest prevalence in 30 – 49 yr age group.

RISK FACTORS OF HCV INFECTION

Natural history
Clinical Presentation
Most patients with chronic hepatitis have asymptomatic elevations of serum aminotransferase levels and do not have physical signs of liver disease.
Some have symptomatic liver disease.
Fatigue is the most common symptom.
Dull right upper quadrant pain.
Less common-anorexia, nausea, pruritus, arthralgia, myalgia.

WORK UP
LFT – ALT levels elevated. Unreliable because it fluctuates. Billirubin may be five times normal.
Anti HCV antibody. It takes 6 wks to 12 months to develop HCV Ab. ELISA is the test for HCV Ab. False –ve occur in immune compromised, HIV, renal failure patients. False +ve in autoimmune hepatitis.
HCV RNA detection by qualitative and quantitative PCR. It is used to confirm viremia and to assess response to treatment.
Viral genotyping. It is useful in choosing therapy.
WBC, ESR, PT are usually normal.

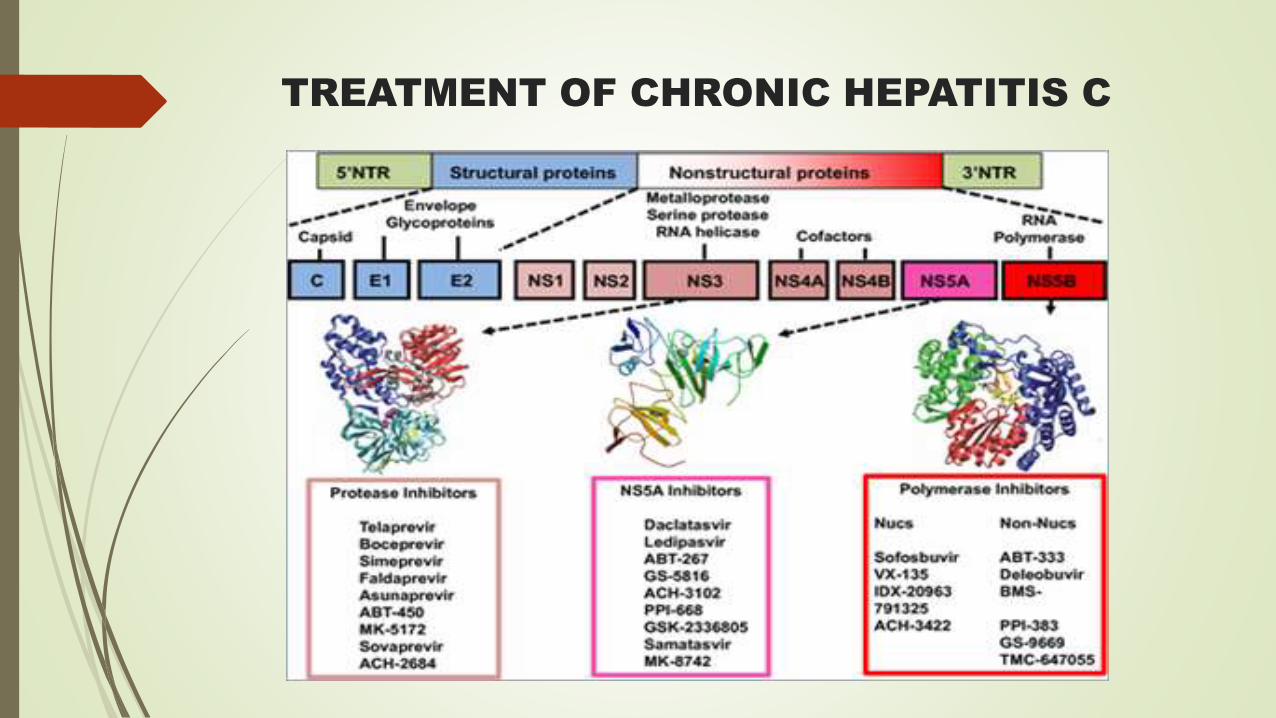
TREATMENT OF CHRONIC HEPATITIS C


RESPONSE TO TREATMENT
Autoimmune Hepatitis(AIH)
It is a chronic inflammatory condition of liver characterized by elevated serum globulin (IgG) levels, presence of circulating autoantibodies , interface hepatitis on histology and plasma cell rich infiltrate.
Also known as Plasma cell hepatitis.
Two types – Type 1 AIH most common type. Positive for ANA and Anti-SM antibody with specific HLA haplotypes B8, DR3, DR4
Type 2 is less common and primarily affects children. Anti LKM1 antibody or Anti liver cytosol 1 antibody. HLA DQB1 and DRB1 association.
Female predominance

PATHOGENESIS
Both cell mediated and humoral mechanisms appear to play a role in pathogenesis.
Some studies suggest that CD4 lymphocytes become sensitized to hepatocyte membrane protein.
Molecular mimicry by cross reacting antigens may play a role.
Arthralgia, arthritis, vasculitis and glomerulonephritis occurring in autoimmune hepatitis appear to be mediated by deposition of circulating immune complexes.

CLINICAL FEATURES
Mostly asymptomatic
Fatigue, malaise, anorexia, arthralgia, acne, jaundice are common.
Occasionally arthritis, maculopapular rash, erythema nodosum, sicca syndrome, pleurisy and pericarditis occur.
Some patients present with complications of cirrhosis such as ascites and edema.
Lab findings may include presence of Rheumatoid factor, ANA, Hypergammaglobulinemia, moderate serum bilirubin elevation, near normal ALP and increased ALT levels.

DIAGNOSIS
Exclusion of other chronic diseases
Viral hepatitis (HBV and HCV)
Alcoholic liver disease and NAFLD
Drug-induced hepatotoxicity
Wilson disease
Hereditary hemochromatosis
Alpha-1-antitrypsin deficiency
Primary biliary cirrhosis
Primary sclerosing cholangitis

Indications for treatment
Absolute RelativeSerum AST 10-fold or more greater than the upper limit of normal
Symptoms (eg, fatigue, arthralgia, jaundice)
Serum AST 5-fold or more greater than the upper limit of normal and gamma-globulin level 2-fold or more greater than normal
Serum AST and/or gamma-globulin less than absolute criteria
Bridging necrosis or multiacinar necrosis on histologic examination
Interface hepatitis

Goals of Treatment
Induce remission
Prevent disease progression
Minimize relapse of disease
Improve survival
Minimize medication side effects


Non Alcoholic Fatty Liver
Disease(NAFLD)
NAFLD was first described in the 1950s when fatty liver was characterized in a group of obese patients.
In 1980, Ludwig and colleagues at the Mayo Clinic described 20 obese, diabetic, nonalcoholic patients who had similar findings on liver biopsy to patients with alcoholic liver disease, and the term nonalcoholic steatohepatitis was introduced


PATHOGENESIS

Clinical features
Asymptomatic in majority of cases
Fatigue
Right upper quardant pain or discomfort
Hepatomegaly (50%)
Obesity
Hypertension

DIAGNOSIS
NAFLD is a diagnosis of exclusion.
Ultrasonography- helps in detecting the fatty infiltration of the liver and helps in determining the size of the liver.
Liver Biopsy - Gold standard for both diagnosis and prognosis. Shows characteristic macrovesicular steatosis with occasional vesicular fat.

Management of NAFLD


















