Chromosomal Anomalies in Prostatic Intraepithelial Neoplasia … › content › canres › 55 ›...
7
ICANCER RESEARCH55, 5408-5414, November 15, 19951 ABSTRACT The pathogenetic relationship between high-grade prostatic intraepi thelial neoplasia (PIN), prostatic carcinoma, and metastases is poorly understood. We used fluorescence in situ hybridization (FISH) with cen tromere-specific probes for chromosomes 7, 8, 10, 12, and Y to evaluate numeric chromosomal anomalies in PIN (68 foci), localized prostatic carcinoma (78 foci), and lymph node metastases (8 foci)in 40 whole-mount radical prostatectomy and pelvic lymphadenectomy specimens. Chrome somal anomalies were found in 50, 51, and 100% of the foci of PIN, carcinoma, and metastases, respectively. The mean numbers of abnormal chromosomes per focus were 0.66 in PIN, 1.09 in carcinoma, and 3.75 in metastases. The most frequent anomaly in PIN was a gain of chromosome 8 (32% of foci), followed by gains of chromosomes 10 (13%), 7 (10%), 12 (4%), and Y (4%). The most frequent anomalies in foci ofcarcinoma were gains of chromosomes 7 and 8 (28% and 30% of foci, respectively), followed by gains of chromosomes 10 (23%), 12 (9%), and Y (9%). There was a positive correlation of the gain of chromosome 8 with the patho logical stage and Gleason score (both P < 0.05). Usually, carcinoma foci contained more anomalies than paired PIN foci, but five prostates con tamed one or more foci of PIN with more anomalies than carcinoma. Among the cases with metastases, usually one or more foci of the primary tumor shared chromosomal anomalies with the matched metastases. Our results indicate that PIN and prostatic carcinoma foci have similar proportions of chromosomal anomalies, but foci of carcinoma usually have more alterations. This observation supports the hypothesis that PIN is often a precursor of carcinoma, although there are somecarcinoma foci that have few or no apparent chromosomal alterations, whereas concur rent PIN foci have multiple alterations. A gain of chromosome 8 was the most common numerical alteration and was associated with increasing cancer stage and grade, suggesting that it may play a role in the initiation and progression of prostatic carcinoma. Usually, one or more foci of the primary tumor shared chromosomal anomalies with associated lymph node metastases, suggesting that, often, just a single focus of carcinoma gives rise to metastases. INTRODUCTION Prostate cancer is the most common malignancy and the second leading cause of cancer death in men in the United States. An understanding of the genetic events that accompany the progression of precursor lesions to prostatic adenocarcinoma and the subsequent development of metastases may be useful for prevention, early detec tion, and treatment. High-grade PIN3 represents the most likely precursor of prostatic adenocarcinoma (1—6).Previous studies have provided limited infor mation concerning genetic changes in PIN (7—9), and the relationship Received 6/26/95; accepted 9/i i/95. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. I This work was supported by a P20 Grant from the NIH (CA 58225); (J. 0., D. G. B., S. T., M. M. L., R. B. J.) and a grant from Vysis, Inc. (Downers Grove, IL; J. Q., R. B. J.). 2 To whom requests for reprints should be addressed, at Cytogenetic Laboratory, Mayo Clinic, 200 First Street, SW., Rochester, MN 55905. Phone: (507) 284-4696; Fax: (507) 284-0043. 3 The abbreviations used are: PIN, prostatic intraepithelial neoplasia; FISH, fluores cence in situ hybridization; BPH, benign prostatic hyperplasia; SG, SpectrumGreen; SO, SpectrumOrange; TSG, tumor suppressor gene. of such changes with primary and metastatic carcinoma is poorly understood (8, 10, 11). FISH analysis of interphase cells with centromere-specific probes is useful for the detection of numerical chromosomal anomalies in solid tumors, including prostatic carcinoma, which is often difficult for conventional cytogenetic analysis (9, 12, 13). Furthermore, when applied to histological sections, this method allows the study of multiple foci of normal epithelium, PIN, and carcinoma within a single prostate specimen. We studied numerical chromosomal anomalies in multiple foci of PIN and carcinoma in 40 whole-mount radical prostatectomy speci mens and 8 matched lymph node metastases. Our objectives were: (a) to determine whether there is a genetic linkage between PIN and adenocarcinoma, which would support the role of PIN as a precursor lesion; (b) to evaluate the genetic heterogeneity of individual foci of PIN and carcinoma, recognizing that these are often multicentric; and (c) to evaluate the relationship between multiple primary foci of carcinoma and lymph node metastases. MATERIALS AND METHODS Patient Selection and Histopathological Evaluation. Forty cases were selectedfromthesurgicalpathologyfilesattheMayoClinicfrompatientswho had undergone radical retropubic prostatectomy and bilateral pelvic lympha denectomy between 1991 and 1994. All patients had clinically localized prostate cancer, and none had received preoperative hormone or radiation therapy. All prostate specimens were formalin fixed, totally embedded, whole mounted, and serially sliced at 5-mm intervals perpendicular to the posterior surface of the gland. For each case, a single 5-gm section was prepared from each slice and examined by two pathologists (J. 0., D. G. B.). All foci of PIN and carcinoma were then mapped directly on each slide. Foci of PIN were considered separate when they were 2 mm or more apart, as described previously (14). In addition, each slice from the entire specimen was evaluated histologically to ensure that the mapped foci of PIN were separate and distinct in deeper sections through the prostate. Carcinoma foci were considered separate by the same histological criteria. The volume of each PIN and carcinoma focus was calculated by the grid-counting method to determine the dominant (largest) lesion (14). For each case, one representative slice was selected for FISH analysis using the criteria that the slice contain at least one focus of PIN and carcinoma. Six serial 5-p@msections were prepared from this slice, and the first and sixth sections were stained by routine hematoxylin and eosin and examined by the two pathologists. Areas with benign epithelium, PIN, and carcinoma were outlined on the remaining four unstained sections for FISH analysis. A Gleason score was determined for each focus of cancer, and the pathological stage for each case was assigned using the ThM system (1992 revision; Ref. 15). In 10 cases, paraffin blocks containing lymph node metastases were also available. However, for two cases the amount of metastatic carcinoma was insufficient for serial sectioning. Ten additional specimens containing BPH were selected for concurrent FISH normal value studies. FISH with Chromosome Enumeration Probes. Tissue sections were deparaffinized with Histo-clear (National Diagnostics, Atlanta, GA), dehy drated in 100% ethanol, incubated in 2X SSC (300 mM sodium chloride and 30 m@i sodium citrate) at 75°C for 15 mm, digested in pepsin solution [Sigma Chemical Co., St. Louis, MO; 4 mg/ml in 0.9% NaCI (pH 1.5)] for 15 mm at 5408 Chromosomal Anomalies in Prostatic Intraepithelial Neoplasia and Carcinoma Detected by Fluorescence in Situ Hybridization1 Junqi Qian, David G Bostwick, Satoru Takahashi, Thomas J. Borell, John F Herath, Michael M. Lieber, and Robert B Jenkins2 Departments ofLaboratory Medicine and Pathology If. Q.. D. G. B., T. J. B., J. F. H., R. B. J.] and Urology [S. T.. M. M. U, Mayo Clinic, Rochester, Minnesota 55905
Transcript of Chromosomal Anomalies in Prostatic Intraepithelial Neoplasia … › content › canres › 55 ›...

ICANCER RESEARCH55, 5408-5414, November 15, 19951
ABSTRACT
The pathogenetic relationship between high-grade prostatic intraepithelial neoplasia (PIN), prostatic carcinoma, and metastases is poorlyunderstood. We used fluorescence in situ hybridization (FISH) with centromere-specific probes for chromosomes 7, 8, 10, 12, and Y to evaluatenumeric chromosomal anomalies in PIN (68 foci), localized prostaticcarcinoma (78 foci), and lymph node metastases (8 foci)in 40 whole-mountradical prostatectomy and pelvic lymphadenectomy specimens. Chromesomal anomalies were found in 50, 51, and 100% of the foci of PIN,carcinoma, and metastases, respectively. The mean numbers of abnormalchromosomes per focus were 0.66 in PIN, 1.09 in carcinoma, and 3.75 inmetastases. The most frequent anomaly in PIN was a gain of chromosome8 (32% of foci), followed by gains of chromosomes 10 (13%), 7 (10%), 12(4%), and Y (4%). The most frequent anomalies in foci ofcarcinoma were
gains of chromosomes 7 and 8 (28% and 30% of foci, respectively),followed by gains of chromosomes 10 (23%), 12 (9%), and Y (9%). Therewas a positive correlation of the gain of chromosome 8 with the pathological stage and Gleason score (both P < 0.05). Usually, carcinoma focicontained more anomalies than paired PIN foci, but five prostates contamed one or more foci of PIN with more anomalies than carcinoma.
Among the cases with metastases, usually one or more foci of the primarytumor shared chromosomal anomalies with the matched metastases.
Our results indicate that PIN and prostatic carcinoma foci have similarproportions of chromosomal anomalies, but foci of carcinoma usuallyhave more alterations. This observation supports the hypothesis that PINis oftena precursor of carcinoma,although there are somecarcinomafocithat have few or no apparent chromosomal alterations, whereas concurrent PIN foci have multiple alterations. A gain of chromosome 8 was themost common numerical alteration and was associated with increasingcancer stage and grade, suggesting that it may play a role in the initiation
and progression of prostatic carcinoma. Usually, one or more foci of theprimary tumor shared chromosomal anomalies with associated lymphnode metastases, suggesting that, often, just a single focus of carcinomagives rise to metastases.
INTRODUCTION
Prostate cancer is the most common malignancy and the secondleading cause of cancer death in men in the United States. Anunderstanding of the genetic events that accompany the progression ofprecursor lesions to prostatic adenocarcinoma and the subsequentdevelopment of metastases may be useful for prevention, early detection, and treatment.
High-grade PIN3 represents the most likely precursor of prostaticadenocarcinoma (1—6).Previous studies have provided limited information concerning genetic changes in PIN (7—9),and the relationship
Received 6/26/95; accepted 9/i i/95.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
I This work was supported by a P20 Grant from the NIH (CA 58225); (J. 0., D. G. B.,
S. T., M. M. L., R. B. J.) and a grant from Vysis, Inc. (Downers Grove, IL; J. Q., R. B. J.).2 To whom requests for reprints should be addressed, at Cytogenetic Laboratory, Mayo
Clinic, 200 First Street, SW., Rochester, MN 55905. Phone: (507) 284-4696; Fax: (507)284-0043.
3 The abbreviations used are: PIN, prostatic intraepithelial neoplasia; FISH, fluores
cence in situ hybridization; BPH, benign prostatic hyperplasia; SG, SpectrumGreen; SO,SpectrumOrange; TSG, tumor suppressor gene.
of such changes with primary and metastatic carcinoma is poorlyunderstood (8, 10, 11).
FISH analysis of interphase cells with centromere-specific probes isuseful for the detection of numerical chromosomal anomalies in solidtumors, including prostatic carcinoma, which is often difficult forconventional cytogenetic analysis (9, 12, 13). Furthermore, whenapplied to histological sections, this method allows the study ofmultiple foci of normal epithelium, PIN, and carcinoma within asingle prostate specimen.
We studied numerical chromosomal anomalies in multiple foci ofPIN and carcinoma in 40 whole-mount radical prostatectomy specimens and 8 matched lymph node metastases. Our objectives were: (a)to determine whether there is a genetic linkage between PIN andadenocarcinoma, which would support the role of PIN as a precursorlesion; (b) to evaluate the genetic heterogeneity of individual foci ofPIN and carcinoma, recognizing that these are often multicentric; and(c) to evaluate the relationship between multiple primary foci of
carcinoma and lymph node metastases.
MATERIALS AND METHODS
Patient Selection and Histopathological Evaluation. Forty cases wereselectedfromthesurgicalpathologyfilesat theMayoClinicfrompatientswhohad undergone radical retropubic prostatectomy and bilateral pelvic lympha
denectomy between 1991 and 1994. All patients had clinically localizedprostate cancer, and none had received preoperative hormone or radiationtherapy.
All prostate specimens were formalin fixed, totally embedded, wholemounted, and serially sliced at 5-mm intervals perpendicular to the posteriorsurface of the gland. For each case, a single 5-gm section was prepared fromeach slice and examined by two pathologists (J. 0., D. G. B.). All foci of PINand carcinoma were then mapped directly on each slide. Foci of PIN wereconsidered separate when they were 2 mm or more apart, as described
previously (14). In addition, each slice from the entire specimen was evaluatedhistologically to ensure that the mapped foci of PIN were separate and distinctin deeper sections through the prostate. Carcinoma foci were considered
separate by the same histological criteria. The volume of each PIN and
carcinoma focus was calculated by the grid-counting method to determine thedominant (largest) lesion (14).
For each case, one representative slice was selected for FISH analysis usingthe criteria that the slice contain at least one focus of PIN and carcinoma. Six
serial 5-p@msections were prepared from this slice, and the first and sixthsections were stained by routine hematoxylin and eosin and examined by thetwo pathologists. Areas with benign epithelium, PIN, and carcinoma wereoutlined on the remaining four unstained sections for FISH analysis. A Gleasonscore was determined for each focus of cancer, and the pathological stage for
each case was assigned using the ThM system (1992 revision; Ref. 15). In 10
cases, paraffin blocks containing lymph node metastases were also available.
However, for two cases the amount of metastatic carcinoma was insufficientfor serial sectioning.
Ten additional specimens containing BPH were selected for concurrentFISH normal value studies.
FISH with Chromosome Enumeration Probes. Tissue sections weredeparaffinized with Histo-clear (National Diagnostics, Atlanta, GA), dehydrated in 100% ethanol, incubated in 2X SSC (300 mM sodium chloride and
30 m@i sodium citrate) at 75°C for 15 mm, digested in pepsin solution [Sigma
Chemical Co., St. Louis, MO; 4 mg/ml in 0.9% NaCI (pH 1.5)] for 15 mm at
5408
Chromosomal Anomalies in Prostatic Intraepithelial Neoplasia and CarcinomaDetected by Fluorescence in Situ Hybridization1
Junqi Qian, David G Bostwick,Satoru Takahashi, Thomas J. Borell, John F Herath, Michael M. Lieber, andRobert B Jenkins2
Departments ofLaboratory Medicine and Pathology If. Q.. D. G. B., T. J. B., J. F. H., R. B. J.] and Urology [S. T.. M. M. U, Mayo Clinic, Rochester, Minnesota 55905

FISH IN PIN, PROSTATE CANCER, AND METASTASES
37°C,rinsed in 2X SSC at room temperature for S mm, and air dried. Becauseprevious work showed a high frequency of anomalies for chromosomes 7, 8,10, 12, X, and Y in prostatic carcinoma (9, 13, 16, 17), directly labeled
fluorescent DNA probes (VYSIS, Framingham, MA) for the centromere regions of chromosomes 7, 8, 10, 12, and X, and for the middistal Yq (Yq12)
region were chosen for study. Dual-probe hybridization was performed on theserial 5-,.@m sections using a SG-labeled probe for chromosome 8 together with
a SO-labeled probe for chromosome 7, a SG-labeled probe for chromosome 12
with a SO-labeled probe for chromosome 10, and a SG-labeled probe for
chromosome X with a SO-labeled probe for chromosome Y. Probes and target
DNA were denatured simultaneously in an 80°Coven for S mm, and each slidewas incubated at 50°Cfor 60 mm. Posthybridization washes were performedin 2X SSC and 0.6% Nonidet P-40 at 45°C for 1 mm and in 2X SSC at room
temperature for 30 s. Nuclei were counterstained with 4,6-diamidino-2-
phenylindole and antifade compound p-phenylenediamine.
Analysis of Interphase FISH. The number of centromere signals wascounted with a Zeiss Axioplan microscope equipped with a triple-pass filter(102—104—1010;Imagenoptics, Naperville, IL). For each probe, 300—500nonoverlapping interphase nuclei from foci of benign epithelium, PIN, andadenocarcinoma were counted. Nuclei from stromal elements were not enu
merated. The number of epithelial nuclei containing zero, one, two, three, four,
and five or more signals was recorded for each probe. Chromosome X was
used as an internal control for chromosome Y to determine whether any
A
apparent loss of chromosome Y was due to inefficient probe hybridization. Thechromosome X signals were not enumerated.
Statistical Analysis. The frequency and distribution of FISH anomalies
among different lesions were analyzed using the Pearson x@test and Student's
t test. The relationship of FISH results among various pathological factors was
evaluated by the Pearson@ test. The significance level was P = 0.05.
RESULTS
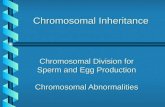
Patients ranged in age from 52 to 75 years (mean, 65.9 years).Pathological tumor stages included T2NOMO(17 cases), T3NOMIJ(13cases), and T5N1MIJ (10 cases). Seventy-eight foci of prostatic carcinoma (mean, 2.0 foci/case), and 68 foci of PIN (mean, 1.7 foci/case)were identified among the 40 cases. Multicentricity (two or morefoci/case) of PIN and carcinoma on the one slice used for FISHanalysis was noted in 55 and 50% of cases, respectively. The Gleasonscores of carcinoma foci were 4—6(33 foci), 7 (26 foci), and 8—10(19foci). Fig. 1 illustrates typical FISH results for several foci observedfor a whole-mount prostate containing stage T3bN1MO cancer. Because thin 5-p@msections were subjected to FISH analysis, manynuclei in each section were truncated. Because of nuclear truncation,
‘ S
B
p
/-fr@,
C DFig. 1. FISH with centromere probes for chromosomes 7 (orange), 8 (green), Y (orange), and X (green) in representative fields of a whole-mount section of the prostate of case
35 (stage T3bN,Me).A, tWOnormal epithelial nuclei (arrows) with two signals for chromosomes 7 and 8. B, PIN focus with several epithelial nuclei (arrows) demonstrating three signalsfor chromosomes 7 and 8. C, carcinoma focus with several nuclei (arrows) demonstrating three signals for chromosomes 7 and 8. D, lymph node metastasis with nuclei (arrows)demonstrating two signals for chromosome Y. As a result of tissue sectioning and nuclear truncation, many nuclei in A—Dhave fewer than two autosome-specific signals and fewerthan one sex chromosome-specific signal (see text). CEP, centromere-specific probe.
5409

Table 1 Normal centromere copy numbers and 3 SDfor epithelial nuclei within 5 pmsections of BPH specimensand normal regionsof 40whole-mountprostatesCentromere
copyNo.―2345>3b0.5
±2.172.8 ±15.968.2 ±15.674.9 ±12.974.6 ±10.20
1.5 ±2.4i.4 ±1.81.4 ±2.41.6 ±2.40
0.2 ±0.60.2 ±0.60.2 ±0.90.2 ±0.90
00000.5
±21d1.6 ±3.01.6 ±2.11.6 ±3.01.8 ±2.40.8
±3.066.0 ±19.267.3 ±22.871.1 ±18.069.7 ±17.10
1.1 ±2.41.1 ±1.80.8 ±2.10.7 ±2.10
0.2 ±0.90.2 ±0.9
0.09 ±0.60.05 ±0.90
0.005 ±0.090000.8
±3.0'@1.3 ±2.71.2 ±2.10.9 ±2.10.7 ±2.1
Specimen
BPHC
Table 2 Distribution of chromosomal anomalies among various foci of 40 whole.mountprostates%
Foci with anomalies for indicatedchromosomes7
8 10 12YAbnormalAbnormalFocusnGainLoss
Gain Loss Gain Loss Gain Loss GainLossfoci (%)cases(%)PIN68102
32 0 13 0 4 3405060Carcinoma7828130 2 23 0 9 49351n72Metastases863087 0 75 0 63 [email protected]
0.004 0.37 0.0003 0.0001 0.40.00010.050.020.07aComparingINversus carcinomaversus metastases. Except for gain of chromosome 7 (P = 0.007), other paired comparisons betweenPIN andcarcinoma are not significant(allP> 0.05).
Normal'
FISH IN PIN, PROSTATE CANCER, AND METASTASES
Chromosome 0 1
Y 9.7 ±9.0 89.7 ±8.77 2.5 ±3.9 23.0 ±13.28 2.8 ±5.4 27.4 ±14.7
10 2.0±2.7 21.5± 12.612 1.6±1.2 22.1±9.0
Y 19.8 ±18.3 79.4 ±18.07 4.6±8.4 28.1± 15.98 4.4 ±8.4 27.2 ±20.4
10 3.6 ±5.7 24.5 ±15.912 4.2±8.1 25.4±12.6aPercentageof300—500epithelialnucleiwithindicatedcentromerecopynumber.
b The sum of 3 + 4 + S or more signals.
C Ten BPH specimens were analyzed.
d The sum of 2 + 3 + 4 or more signals.
e Forty normal regions of whole-mount prostate were analyzed.
multiple nuclei illustrated in Fig. 1 have fewer than one and two sexchromosome- and autosome-specific signals, respectively (e.g., lessthan the expected normal complements of these chromosomes). Suchnuclear truncation may obscure a true monosomy (or nullisomy forthe Y chromosome). In addition, there are clearly nuclei in the PINfocus and the carcinoma focus that have two or more chromosomespecific signals (or two or more Y chromosomal signals). Cells withthree or more signals could be due to a true chromosomal gain or dueto nuclear overlap. Thus, to ascertain true aneusomies accurately, weundertook a detailed normal value study.
Normal Value Study. The mean ±3 SD of the number of copiesfor each chromosome among 10 cases of benign prostatic hyperplasiaand results of apparently normal epithelia of 40 whole-mount prostates are summarized in Table 1. The mean percentage of epithelialnuclei with two signals for chromosomes 7, 8, 10, and 12 ranged from66 to 75%. The ranges of mean percentages of epithelial nuclei withzero and one, three, and three or more signals were 23—33%,0.7—1.6%, and 0.7—1.8%,respectively.
The mean percentage of epithelial nuclei with one signal for chromosome Y ranged from 79—90%.The ranges of mean percentages ofnuclei with zero, two, and two or more signals were 9.7—19.8%,0.5—0.8%,and 0.5—0.8%,respectively.
For all chromosomes, the mean + 3 SD percentage of nuclei withzero and one signal (zero for the Y) was <55%, and the mean + 3 SDpercentage with three or more signals (two or more for the Y) was<5%.
Criteria for FISH Anomalies. Based on the normal value studyand an inspection of the distribution of FISH signals among thecarcinoma foci, we developed the following conservative criteria forFISH anomalies: (a) abnormal autosomal gain required 7% epithehal nuclei with three signals and 8% nuclei with three or moresignals; (b) abnormal autosomal loss required 55% nuclei with zeroor one signal; (c) abnormal Y chromosome gain and loss usedidentical criteria for nuclei with two signals, two or more signals, andzero signal, respectively; (d) tetraploidy was suspected when the
percentage of nuclei with three and four signals (or two for the Ychromosome) was similar for both chromosomes 7 and 8. No BPHspecimens or apparently normal prostate epithelia contained valuesthat exceeded these criteria.
Distribution of FISH Anomalies in PIN and Carcinoma. Table2 summarizes the overall distribution of FISH anomalies observed inall the various PIN, carcinoma, and metastatic foci evaluated. Chromosomal anomalies were found in 50% of PIN foci, 51% of cancerfoci, and 100% of metastases (P = 0.02). These values increased to60%, 72%, and 100% for PIN, carcinoma, and metastases, respectively, when the data were analyzed by case. Significant differenceswere observed in the incidence of gains of chromosomes 7, 8, 10, 12,and Y comparing foci of PIN, carcinoma, and metastases (for all,P < 0.004). The most frequent anomaly in PIN was a gain ofchromosome 8 (32% of foci), followed by gains of chromosomes 10(13%), 7 (10%), 12 (4%), and Y (4%). The most frequent anomaliesin foci of carcinoma were gains of chromosomes 7 and 8 (28% and30% of foci, respectively), followed by gains of chromosomes 10(23%), 12 (9%), and Y (9%). There was no difference in the frequencyof chromosomal anomalies between PIN and carcinoma except for thepercentage of gain of chromosome 7 (10% for PIN versus 28% forcancer, respectively; P = 0.007). Metastatic foci showed a highpercentage of anomalies for all chromosomes (>63% of foci).
The mean number of abnormal chromosomes increased from 0.66in PIN to 1.09 in carcinoma and 3.75 in metastatic foci. Except for thecomparison of PIN versus carcinoma (P = 0.054), all other pairedcomparisons of the mean number of abnormal chromosomes (carcinoma versus metastasis and PIN versus metastasis) was significantlydifferent (P < 0.005).
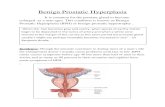
Comparison of FISH Anomalies in PIN and Carcinoma Foci.Fig. 24 illustrates representative detailed histological mapping of allPIN and carcinoma foci from a slice of whole-mount prostate case 35(stage T3bNiM@). Based on histological evaluation of the entire specimen, this slice contains four and six separate PIN and carcinoma foci,respectively. Five of the six carcinoma foci had Gleason scores of 7;
5410

FISHIN PIN, PROSTATECANCER,ANDMETASTASES
Fig. 2. Whole-mount section of the prostate ofcase 35 (stage T@bN,Ml@).A, multiple foci of carcinoma and PIN arising in the same gland (red linesoutline cancer foci; blue lines outline PIN foci). Aleft pelvic lymph node with metastasis is also illustrated. Its relative anatomical location to theprostate is indicated by its position in the figure. B,summary of chromosomes 7, 8, 10, 12, and Y FISHanomalies for the same foci. Note the heterogeneityof anomalies among multiple foci of carcinoma andPIN. A small and low-grade left-sided tumor (Can.cer 6) shares the anomalies with lymph node metastasis, whereas larger and higher-grade tumors(Cancers 1. 3. 4, and 5) show no abnormal chromosomal anomaly (N).
ICarcinoma1@I
the remaining small carcinoma focus had a Gleason score of 5. Fig. 2Bsummarizes the FISH anomalies observed in the PIN, carcinoma, andmetastatic foci. Three of the four PIN foci contained FISH anomalies:+ 10; +8,+ 10; and +8,+ 10,+Y. Two of six carcinoma foci con
tamed FISH anomalies. One Gleason score 7 carcinoma focus had+ 10. This foci surrounded the PIN focus completely with +8 and
+ 10. The smallest carcinoma focus with Gleason score 5 was ob
served to have anomalies of each chromosome evaluated. Because
7—23%of nuclei had three signals for each of the chromosomesevaluated, the possibility that this focus is near tetraploid cannot beexcluded. The metastatic focus had anomalies identical to those observed in the Gleason score 5 carcinoma focus.
Each whole-mount prostate was mapped regionally as describedabove for case 35 (data not shown but available on request). Tables 3and 4 summarize the FISH anomalies observed in all apparent PINand carcinoma foci found among the 40 whole-mount prostates. Innine cases, no apparent FISH anomalies were observed in either typeof focus. In 22 cases, FISH anomalies were observed in a minimum ofone focus of PIN and one focus of carcinoma. One or more similarFISH anomalies was shared in paired PIN and carcinoma foci in allbut 2 of these 22 cases (cases 2 and 26). Anomalies were identified in
carcinoma but not in paired PIN foci in seven cases. In general, withineach whole-mount prostate slice, the carcinoma foci contained moreanomalies than the paired PIN foci. However, in three cases, one ormore PIN foci clearly contained more anomalies than those observedin carcinoma foci (cases 3, 35, and 37; Fig. 2B). Furthermore, anomalies were identified in PIN but not in paired carcinoma foci in twocases (cases 19 and 28).
Comparison of Chromosomal Anomalies in Various PIN Foci.There was no difference in the frequency of anomalies between thedominant (largest) focus of PIN and other smaller foci of PIN for allchromosomes (P > 0.05). However, there was considerable variabilityin the frequency of anomalies among different foci of PIN for eachchromosome. In 48% of cases with multiple foci of PIN, anomalieswere observed in one or more foci of PIN, but not in other foci,indicating significant intraglandular PIN genetic heterogeneity (Fig.28 and Tables 3 and 4).
Chromosomal Anomalies in Prostatic Carcinoma. Table 5 summarizes the distribution of chromosomal anomalies in all 40 caseswith different stages of carcinoma. The percentages of primary carcinomas with chromosomal anomalies were 59, 85, and 80% in stagesT2N0MIJ, T3N@MIJ, and TXN1MO, respectively (P 0.24). A gain of
5411
[Me@s@@cI Lymph Nodes
+7,+8,+1O,+12,+Y(23%-37% fltraplold
B
[ó@rcinomaI
IPIN

Table 3 FISHfor chromosomes 7, 8, 10, 12, and Yfor ailfoci ofPIN andcarcinomaamong30 whole-mount prostates containing localized carcinoma (stageT2_3N@M0)PIN
CancerCase
Dominant focus― Other foci― Dominant focus― Otherfoci―1
+8 +8,—12 +7,+8,+10,+Y+7,+82+Y+7,+8,+103+7,+8+74+8 —7/+8,—12+7,+8,—125+7,+8,+10,+12,+Y +8 +7,+8,+10,+12,+Y
6 N― N+77NN8N+79N N-710+8 N +7,+8N11N NN12+7+713+10+7,+1014N N/N +7N15+7 N+716N NN17N +10/+10 +10+1018
+7,+819+7 NN20+8+7,+8,+10,+12,+Y21NN22
+823NN24NN25N +10N26+10 N/N+8,—1227NN28+7 NN29N N +8N30N N N-8a
Fordefinitionofdominantandotherfoci,see“MaterialsandMethods.―If“OtherFoci―column is blank, additional foci were not apparent in the gland. A slash (I)separatesthe
results for two or more additionalfoci.bN, no apparent chromosomal anomaly.
Table 4 FISHofchromosomes 7, 8, 10, 12, atic! Yfor allfoci ofPJN andcarcinoma among 10 whoIc-mount prostates associated with lymph node metastases (stageT,,N1M0)PINCancerCancer
Lymph nodemetastasesCaseDominant focus―Other foci―Dominant focus―Otherfoci―31N―+12+7,+8,+10,+12N/N/N+7,+8,+10,+12,+Y.32+8+8,+12+7,+8,+10,+12,—Y+7,+8,+12,—Y+7,+8,+10,+12,—Y33NN/NNNNAC34+8+7,+8+8NA35+10+8,+10/+8,+10,+YINN+10/+7,+8,+10,+12,+YINININ+7,+8,+10,+12,+Y36N+8+10—8/+8,+10/+8,+10/N/N/N+7,+8,+10,+1237+8,+10N+8N/N/N+838+8+8+8—l2/+7,+8,+lO,+12,+Y/N+7,+8,+10,+12,+Y39NNN+10,+Y40+8+8N+10+Y/+8,+10,+Y/N/N+8,—12,+Y
Table 5 Distribution ofchromosomal anomalies by cancer stage among 40 whole-mountprostatesCases
of carcinoma with anomalies for indicated chromosomes(%)7
8 1012YAbnormalStagenGainLoss
Gain Loss Gain Loss Gain LossGainLosscases(%)T2N@M.@
T3N@M@
T@N1M.@Pa17
13
105346
500.930
18 0 29 0 6 08 54 8 15 0 8 15
0 80 10 60 0 40 100.34 0.005 0.45 0.07 0.04 0.2712
830
0.290
010
0.2159
8580
0.24a
ComparingstageT2N0M0 versusT3N0M@ versus TXN!M.J.
FISH IN PIN, PROSTATE CANCER, AND METASTASES
creased in frequency with increasing Gleason score, but this wassignificant for only a gain of chromosome 8, a gain of chromosome10, and a loss of chromosome Y. The mean number of abnormalchromosomes increased from 0.88 in carcinoma foci with Gleasonscores 7 to 1.78 in carcinoma foci with Gleason scores 8(P = 0.016).
Intraglandular genetic heterogeneity was found in 55% of caseswith multiple foci of carcinoma. There was no apparent difference inthe frequency of chromosomal anomalies in multicentric cancersbetween the dominant (largest) focus and other small foci (data notshown; example shown in Fig. 2B).
Chromosomal Anomalies in Lymph Node Metastases. Table 4also summarizes the FISH anomalies observed within the regionalmetastatic foci of the stage T5N1M0 cancers. All metastases showedchromosomal anomalies (100%), and the percentage of anomalies washigh for all chromosomes (>63%). Except for one case (case 39), inwhich the primary tumor showed no anomalies, one or more cancerfoci found in the primary tumor usually shared anomalies with thematched metastases. In cases 31, 32, and 37, the dominant focus ofcarcinoma demonstrated the same anomalies as the metastases. Incases 35, 36, 38, and 40, similar anomalies were noted in nondomi
nant foci. For each of these seven cases, the metastatic foci werelocated on the ipsilateral side corresponding to the side of the prostatewith the matched abnormal focus of cancer (Fig. 2B and Table 4). Thedominant (largest) focus of cancer was on the same side as themetastases in 87.5% of cases.
DISCUSSION
The genetic changes in PIN (7—9)and their relationship to thegenetic changes in prostatic carcinoma are poorly understood (8, 10,11). In this study, the overall frequencies of numeric chromosomalanomalies in PIN and carcinoma foci were remarkably similar (50 and51%, respectively), suggesting that they share a similar underlyingpathogenesis (18). Because one prostate specimen can harbor morethan one focus of PIN and/or carcinoma with FISH anomalies, these
chromosome 8 was correlated significantly with pathological stage(P = 0.005). A marginal positive correlation for a gain of chromosome 12 with pathological stage (P = 0.04) was also found.
Table 6 indicates the distribution of chromosomal anomalies incarcinoma according to Gleason score. Chromosomal anomalies in
aFordefinitionofdominantandotherfoci,see“MaterialsandMethods.―If“OtherFoci―columnisblank,additionalfociwerenotapparentinthegland.Aslash(I)separatestheresults for two or more additional foci.
b N, no apparent chromosomal anomaly.CNA, not available.
5412

Table 6 Distribution of chromosomal anomalies by cancer gleason score wnong 40 whole-mountprostatesGleason
scorenFoci
of carcinoma with anomalies for indicated chromosomes(%)7
8 10 12
Gain Loss Gain Loss Gain Loss Gain LossGainYLossAbnormal foci(%)4—6
7
8—10Pa33
26
1930
0 18 0 9 0 6 623 4 27 8 23 0 4 4
32 0 53 0 47 0 21 00.52 0.36 0.03 0.13 0.007 0.1 0.556
816
0.480
011
0.0436
5768
0.06a
ComparingGleasonscores 4—6versus 7 versus 8—10.
FISH IN PIN, PROSTATE CANCER, AND METASTASES
proportions increased when the data were analyzed by case. Overall,the mean number of abnormal chromosomes increased in PIN tocarcinoma foci, and within each whole-mount prostate, the carcinomafoci contained more anomalies than the paired PIN foci. These findings suggest that PIN is a precursor of carcinoma (1—8,14, 18, 19).However, within five prostates, one or more PIN focus containedclearly more anomalies than concurrent carcinoma foci, and withintwo prostates, chromosomal anomalies in PIN and carcinoma weredifferent. These results indicate that some PIN foci may have adivergent pathogenesis or that foci of carcinoma may be occasionallyderived from other precursor lesions such as atypical adenomatoushyperplasia (20). These results also indicate that some molecular
genetic events in the malignant transformation of the prostate epithehum are not detectable by FISH with centromere-specific probes.
High-grade PIN and prostatic carcinoma are usually multicentric (2,4, 8, 14). The genetic changes among multiple foci of PIN andcarcinoma have not been well defmed (8, 18). Our observationsdemonstrate that genetic analysis of multiple foci of PIN and carcinoma in whole-mount, regionally mapped prostates is useful forunderstanding fully the alterations within these multicentric lesionsand evaluating their pathogenetic relationships. We have demonstrated that FISH anomalies can be found in one focus of PIN,whereas other multicentric PIN foci may have no apparent FISHanomalies or may have other anomalies. Similar intraglandular genetic heterogeneity was observed in multiple foci of carcinoma. Somesmall, low-grade tumor foci were aneuploid by FISH, whereas concurrent, dominant, high-grade tumor foci were apparently normal,indicating that small cancers can have significant alterations. UsingPCR, ISH, and DNA ploidy techniques, similar intraglandular heterogeneity has been reported (18, 21, 22). Thus, the size of a cancerfocus and its degree of histological dedifferentiation may not reflectthe extent of its genetic alterations.
A gain of chromosome 8 was the most frequent numeric anomalyin PIN and prostatic carcinoma. Other studies have also demonstrateda gain of the chromosome 8 centromere by FISH and a loss of portionsof the 8p arm by PCR in specimens of PIN and carcinoma (7—9,18),suggesting that alterations of this chromosome and/or a TSG on theshort arm may be important for the initiation or early progression ofprostate cancer. Supporting this hypothesis, and consistent with previous reports (9, 16, 17), the gain of chromosome 8 also correlatedwith carcinoma stage and grade. Multiplication of the 8q arm is oftenaccompanied by 8p arm allelic loss (23—27).A likely genetic mechanism underlying both the FISH and molecular genetic observations isthe presence of multiple 8q isochromosomes in tumor cells (25).
In this series, we observed that the gain of chromosome 8 was themost frequent chromosomal anomaly in metastatic foci, and the frequency was much higher than in PIN and carcinoma. Similarly,Visakorpi et a!. (26) found gains of 8q far more frequently in locallyrecurrent cancer than in the primary cancer. Amplification of 8q DNAsequences was observed in 75% of metastatic lymph node lesions(27), suggesting that the 8q arm may harbor a gene(s) with amplification and overexpression that may play a key role in the progression
and evolution of prostatic carcinoma. The cumulative findings suggestthat the gain of chromosome 8 is a marker of clinically aggressiveprostatic carcinoma.
The role of chromosome 7 in prostatic carcinoma is controversial.A positive correlation of trisomy 7 with tumor grade, stage, andprognosis has been reported (9, 13, 28). Allelic loss studies have alsosuggested a possible location for a putative TSG (29). However, someauthors have reported no association of trisomy 7 with clinical andpathological parameters (17, 21). Consistent with previous reports (9,13, 17, 28), in the current study, trisomy 7 was one of the mostfrequently observed aberrations, but it did not correlate with tumorstage and grade. However, the frequency of trisomy 7 was muchhigher in carcinoma than in PIN (P = 0.007). This indicates that again of chromosome 7 may play a role in the progression of precursorlesions to carcinoma.
A gain of chromosome 10 was found in 23% of foci of carcinoma,and this correlated with the Gleason score. Recently, allelic lossstudies have suggested that the lOq arm may also harbor a TSG (30,31). Anomalies of chromosomes 12 and Y have also been reported tobe frequent in prostate cancer (13, 21, 32), but usually in associationwith anomalies of chromosomes 7, 8, and 10.
A prior publication showed loss of several chromosomes in prostatecancer by FISH (33). The discordance of gain and loss of chromosomes in prostate cancer from different institutions is likely caused bydifferent criteria for FISH anomalies (7, 21, 28, 33). In addition,because our FISH studies were performed on tissue sections, we wereunable to establish a reference ploidy accurately. It is possible thatsome of the apparent gains we observed were actually losses relativeto tetraploidy.
The molecular basis for prostate cancer metastasis remains unclearand has been the subject of several recent investigations (10, 11, 21,31, 32). Four paired primary tumors and metastases have been observed to have similar p53 or FISH alterations (10, 11, 21, 32).Frequent allelic loss of chromosomes 8, 10, and 16 has been reportedin metastatic lesions (31, 34). None of these genetic studies usedwhole-mount, regionally mapped prostates. Sakr et a!. (8) reportedthat some lymph node metastases did not share genetic alterationswith a primary tumor, but this result may have been due toincomplete sampling of prostate tumor foci. In our study, all eightmetastatic foci showed multiple chromosomal anomalies. The percentage of chromosomal aneusomy and the average number ofabnormal chromosomes were higher than those of primary tumorand PIN foci, indicating that primary tumor cells with multiplegenetic anomalies are usually ones that metastasize and/or thatmetastatic lesions are genetically unstable (35). Interestingly, oneor more primary tumors usually shared the same FISH alterationsas the matched ipsilateral metastasis, suggesting that this tumorfocus gave rise to the metastases. These FISH data demonstratethat the size and grade of a primary tumor focus cannot be used topredict its metastatic behavior reliably in individual cases.
5413

FISH IN PIN, PROSTATE CANCER, AND METASTASES
relationship with carcinoma in 217 whole mount radical prostatectomies. Am. J. Surg.Pathol., 19: 506—518, 1995.
21. Alers, C. A., Krijtenburg, P. J., Vissers, K. J., Bosman, F. T., van der Kwast, T. H.,and Dekken, H. Interphase cytogenetics of prostatic adenocarcinoma and precursorlesions: analysis of 25 radical prostatectomies and 17 adjacent prostatic intraepithelialneoplasias. Genes Chromosomes & Cancer, 12: 241—250,1995.
22. Greene, D. R., Rogers, E., Weasels, E. C., Wheeler, T. M., Taylor, S. R., Santucci,R. A., Thompson, T. C., and Scardino, P. T. Some small prostate cancers are
nondiploid by nuclear image analysis: correlation of deoxyribonucleic acid ploidystatus and pathological features. J. Urol., 151: 1301—1307,1994.
23. Bova, G. S., Carter, B. S., Bussemakers, M. J. G., Emi, M., Fujiwara, Y., Kyprianou,N., Jacobs, S. C., Robinson, J. C., Epstein, J. I., Walsh, P. C., and Isaacs, W. B.Homozygous deletion and frequent allelic loss of chromosome 8p22 loci in humanprostate cancer. Cancer Res., 53: 3869—3873, 1993.
24. Macoska, J. A., Trybus, T. M., Sakr, W. A., Wolf, M. C., Benson, P. D., Powell, I. J.,and Pontes, J. E. Fluorescence in situ hybridization analysis of 8p allelic loss andchromosome 8 instability in human prostate cancer. Cancer Res., 54: 3824—3830,1994.
25. Cher, M. L, MacGrogan, D., Bookstein, R., Brown, J. A., Jenkins, R. B., Jensen,R. H. Comparative genomic hybridization, allelic imbalance, and fluorescence in situ
hybridization on chromosome 8 in prostate cancer. Genes Chromosomes & Cancer,11: 153—162,1994.
26. Visakorpi, T., Kallioniemi, A. H., Syvanen, A. C., Hyytinen, E. R., Karhu, R.,Tammela, T., Isola, J. J., and Kallioniemi, 0. P. Genetic changes in primary andrecurrent prostate cancer by comparative genomic hybridization. Cancer Res., 55:342—347, 1995.
27. Van Den Berg, C., Guan, X. Y., Von Hoff, D., Jenkins, R. B., Bitter, M., Griffin, C.,Kallioniemi, 0., Visakorpi, T., McGill, J., Herath, J. F., Epstein, J. I., Scarosdy, M.,Meltzer, P., and Trent, J. DNA sequence amplification in human prostate canceridentified by chromosome microdissection: potential prognostic implications. Chin.Cancer Res., 1: 11—18,1995.
28. Bandyk, M. G., Thao, L., Troncoso, P., Pisters, L. L., Palmer, J. L, von Eschenbach,A. C., Chung, L. W. K., and Liang, J. C. Trisomy 7: a potential cytogenetic marker
of human prostate cancer progression. Genes Chromosomes & Cancer, 9: 19—27,1994.
29. Zenklusen, J. C., Thompson, J. C., Troncoso, P., Kagan, J., and Conti, C. J. Loss ofheterozygosity in human primary prostate carcinoma: a possible tumor suppressorgene at 7q31.1. Cancer Rca., 54: 6370—6373, 1994.
30. Eagle, L R., Yin, X., Brothman, A. R., Williams, B. J., Atkin, N. B., and Prochownik,E. V. Mutation of the MXIJ gene in prostate cancer. Nature Genet., 9: 249—255, 1995.
31. Bergerheim, U. S. R., Kunimi, K., Collins, V. P., and Ekman, P. Deletion ofchromosomes 8, 10, and 16 in human prostatic carcinoma. Genes Chromosomes &Cancer, 3: 215—220,1991.
32. Steilen, H., Ketter, R., Romanakis, K., Zwergel, T., Unteregger, G., Bonkhoff, H.,Seitz, G., Ziegler, M., Zang, K. D., and Wullich, B. DNA aneuploidy in prostaticcarcinoma: a frequent event as shown by fluorescence in situ DNA hybridization.Hum. Pathol., 25: 1306—1313, 1994.
33. Baretton, G. B., Valina, C., Vogt, T., Schneiderbanger, K., Diebold, J., and Lohrs, U.Interphase cytogenetic analysis of prostatic carcinoma by use of nonisotopic in situhybridization. Cancer Res., 54: 4472—4480, 1994.
34. Isaacs, W. B., Bova, G. S., Morton, R. A., Bussemaker, M. J., Brooks, J. D., andEwing, C. M. Molecular genetics and chromosomal alterations in prostate cancer.Cancer (Phila.), 75: 2004—2012, 1995.
35. Shackney, S. E., Smith, C. A., Miller, B. W., Burholt, D. R., Murtha, K., Giles, H. R.,Ketterer, D. M., and Police, A. A. Model for the genetic evolution of human solidtumors. Cancer Res., 49: 3344—3354, 1989.
5414
REFERENCES
1. Bostwick, D. G., and Brawer, M. K. Prostatic intra-epitheial neoplasia and earlyinvasion in prostate cancer. Cancer (Phila.), 59: 788—794, 1987.
2. McNeal, J. E., and Bostwick, D. G. Intraductal dysplasia: a premalignant lesion of theprostate. Hum. Pathol., 17: 64—71,1986.
3. McNeal, J. E., Ahoy, J., Leav, I., Redwine, E. A., Freiha, F. S., and Stamey, T. A.Immunohistochemical evidence for impaired cell differentiation in the premalignantphase of prostate carcinogenesis. Am. J. Clin. Pathol., 90: 23—32,1988.
4. Quinn, B. D., Cho, K. R., and Epstein, J. I. Relationship of severe dysplasia to stageB adenocarcinoma of prostate. Cancer (Phila), 65: 2328—2337, 1990.
5. Davidson, D., Bostwick, D. G., Qian, J., Wollan, P., Osterling, J. E., Rudders, R. A.,Siroky, M., and Stilmant, M. Prostatic intraepithelial neoplasia is predictive ofadenocarcinoma. J. Urol., 154: 1295—1299,1995.
6. Bostwick, D. G., Amin, M. B., Dundore, P., Marsh, W., and Schultz, D. S. Architectural patterns of high-grade prostatic intraepithelial neoplasia. Hum. Pathol., 24:298—310,1993.
7. Macoska, J. A., Micale, M. A., Sakr, W. A., Benson, P. D., and Wolman, S. R.
Extensive genetic alterations in prostate cancer revealed by dual PCR and FISHanalysis. Genes Chromosomes & Cancer, 8: 88-97, 1993.
8. Sake, w. A., Macoska, J. A., Benson, P. D., Grignon, D. J., Wolman, S. R., Pontes,J. E., and Crissman, J. D. Allelic loss in locally metastatic, multisampled prostatecancer. Cancer Res., 54: 3273—3279,1994.
9. Takahashi, S., Qian, J., Brown, J. A., Alcaraz, A., Bostwick, D. G., Lieber, M. M.,and Jenkins, R. B. Potential markers of prostate cancer aggressiveness detected byfluorescence in situ hybridization. Cancer Rca., 54: 3574—3579,1994.
10. Effert, P. J., Neubauer, A., Walther, P. J., and Liu, E. T. Alterations of p53 gene areassociated with the progression of a human prostate carcinoma. J. Urol., 147:789—793, 1992.
11. Macoska, J. A., Powell, I. J., Sakr, w. A, and Lane, M. Loss ofthe l7p chromosomalregion in a metastatic carcinoma of the prostate. J. Urol., 147: 1142—1146, 1992.
12. Devilee, P., Thierry, R. F., Kievits, T., Kolluri, R., Hopman, A. H. N., Willard, H. F.,Pearson, P. L., and Cornellisse, C. J. Detection of chromosome aneuploidy ininterphase nuclei from human primary breast tumors using chromosome-specificrepetitive DNA probes. Cancer Rca., 48: 5825—5830,1988.
13. Alcaraz, A., Takahashi, S., Brown, i. A., Herath, J. F., Bergstralh, E., Larson-Keller,J., Lieber, M. M., and Jenkins, R. B. Aneuploidy and aneusomy of chromosome 7detected by fluorescence in situ hybridization are markers of poor prognosis inprostate cancer. Cancer Res., 54: 3998—4002,1994.
14. Qian, J., Wollan, P., and Bostwick, D. G. The extent and multicentricity of high gradeintraepithelial neoplasia in clinically localized prostatic adenocarcinoma. Hum.Pathol., in press, 1995.
15. Schroder, F. H., Hermanek, P., Denis, L, Fair, W. R., Gospodarowicz, M., andPavone-Macaluso, M. The TNM classification of prostate cancer. Prostate, 4 (Suppl.):129—138,1992.
16. Persons, D. L, Gibney, D. J., Hatzmann, J. A., Lieber, M. M., Farrow, G. M., andJenkins, R. B. Use of fluorescence in situ hybridization for deoxyribonucleic acidploidy analysis of prostatic carcinoma. J. Urol., 150: 120—125,1993.
17. Brown, J. A., Alcaraz, A., Takahashi, S., Persons, D. L, Lieber, M. M., and Jenkins,R. B. Chromosomal aneusomies detected by fluorescence in situ hybridization analysis in clinically localized prostate carcinoma. J. Urol., 152: 1157—1162, 1994.
18. Emmert-Buck, M. R., Vocke, C. D., Pozzatti, R. 0., Duray, P. H., Jennings, S. B.,Florence, C. D., Zhuang, Z., Bostwick, D. G., Liofta, L A., and Linehan, W. LAllelic loss on chromosome 8pl2—2lin microdissected prostatic intraepithelial neoplasia (PIN). Cancer Res. 55: 2959—2962, 1995.
19. Bostwick, D. G. High grade prostatic intraepithelial neoplasia: the most likelyprecursor of prostate cancer. Cancer (Phila.), 75: 1823—1836,1995.
20. Bostwick, D. G., and Qian, J. Atypical adenomatous hyperplasia of the prostate: