Christopher R. Graber, MD Salina Women’s Clinic September 27, 2011 (revised from Mar 2010)
22
Christopher R. Graber, MD Salina Women’s Clinic September 27, 2011 (revised from Mar 2010) Pre-Term Labor
-
Upload
joanna-emma-skinner -
Category
Documents
-
view
215 -
download
0
Transcript of Christopher R. Graber, MD Salina Women’s Clinic September 27, 2011 (revised from Mar 2010)

Christopher R. Graber, MD
Salina Women’s Clinic
September 27, 2011
(revised from Mar 2010)
Pre-Term Labor

DefinitionsRandom FactsRisk Factors for PTLTocolytics
Gr. tokos: childbirth, lytic: capable of dissolvingIdentifying patients at high riskPreterm contractions aloneRecommendationsReferences
Introduction

Term: 37-42 wgaPreterm: between 20 and 37 wgaLabor: contractions causing cervical changeInsufficient cervix: painless cervical dilation,
usually before 20 weeksTocolytic: any medicine given to inhibit
myometrial contractionsEtOH, MgSO4, CCA, betamimetics, NSAIDs
Definitions

Preterm birth is a leading cause of neonatal morbidity and mortality
In the US, 11.5% of all births are preterm35% of health care $$ for infants75% of neonatal mortality50% of long-term neurologic impairments
The incidence of preterm birth is essentially the same as 40 years ago
Random Facts

Multiple gestationsPrior preterm birthPreterm premature ROMBacterial vaginosis (unclear if Rx helps)Genitial infectionsPeriodontal diseaseEnvironmental factors
Smoking, drug useLong periods of standing – 1 study
Risk Factors for PTL

Etoh – mid 20th centuryMgSO4 – most commonly used, controversialCalcium Channel Blockers – newer
Nifedipine (Procardia)Betamimetics – most common outpatient
Ritodrine, turbutalineOxytocin antagonists – experimental
Atosiban
Tocolytics


May prolong gestation for 2-7 daysAllow for steroids and/or transport
Betamethasone 12mg IM q24h x 2 doses
No clear “first-line” drugSide effects are common, adverse events are
rare but seriousDo NOT combine tocolytics
Tocolytics

Controversy for MgSO4

2005: 192 patients, 24 to 33.6 wga, randomized to MgSO4 or Nifedipine
Primary outcome: arrest of preterm labor – prevention of delivery for 48 hours with uterine quiesence
Primary outcome – MgSO4 87% vs. Nifedipine (72%)
No differences – del within 48h, gestational age at del, birth prior to 37 or 32 weeks.
MgSO4 newborns spent more time in NICUMild and severe adverse effects more
common in MgSO4 group
MgSO4 vs. Nifedipine

ACOG Committee Opinion 455, March 2010Observational studies in ‘90’s showed fewer
neurologic complications if MgSO4 exposure for preterm del
Led to several large studiesMeta-analysis suggests that MgSO4
decreases risk for cerebral palsy (RR 0.71, 95% confidence 0.55-0.91)
No effect on fetal/infant deathSerious maternal complications not more
common
MgSO4 for Neuroprotection

MgSO4 for Neuroprotection

Who to treat?Probability of progressive labor, gestational
age, risks of treatmentRegular uterine activity that does not decrease
with bed rest and hydrationContraindications
Severe preeclampsia, active vaginal bleeding (abruption), chorio, lethal abnormalities, advanced dilation, fetal indications
High Risk?

Document cervical dilation (?change)Consider fetal fibronectin
NPV 99%, PPV 50% for delivery in 2 weeksNo bleeding, cvx <3cm, NPV for 24h
Consider cervical sonoTransvaginal most accurate
Identify High Risk Patients


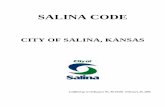
Cervical Length (mm)
Fetal Fibronectin + (%)
Fetal Fibronectin – (%)
25 65 25
26-35 45 14
>35 25 7
Prior Preterm Birth
Fetal fibronectin and cervical length (transvaginal) assessed at 24wga. From: Iams JD, et al. The Preterm Prediction Study: recurrence risk of spontaneous preterm birth. Am Journal of Obstetrics and Gynecology. 1998; 178: 1035-1040.
Recurrence risk of spontaneous preterm birth at <35wga in women with a prior preterm birth

Preterm contractions do not reliably predict cervical changeStudy: 760 women presenting with symptoms
18% delivered before 37wga3% delivered within 2 weeks of first presentation
Bed rest, pelvic rest, hydrationUncertain benefits, never provenPossible side effects: DVT, no income
Preterm Contractions

Women with multiple gestations are at high risk for PTL but are also at high risk for pulmonary edema with MgSO4 or turbutaline.
Repeated courses of tocolysis?Limited benefits for initial courseOnly for transportMgSO4 for neuroprotection?
Consider amniocentesis for FLM
Other random facts

No clear “first-line” tocolytic drugsAntibiotics do not appear to prolong gestation
Reserve for GBS prophylaxisNeither maintenance treatment with
tocolytics nor repeated acute tocolysis improve perinatal outcomes
Recommendations – Level A

Tocolytics may prolong pregnancy 2-7 days to allow for transport and ANCS (the most beneficial intervention for true PTL)
There are no current data to support the use of salivary estriol, Home Uterine Activity Monitoring (HUAM), or BV screening as strategies to identify or prevent PTL
Recommendations – Level A

Cervical ultrasound and/or fetal fibronectin have good negative predictive value and may be useful in determining women at high risk
Amniocentesis for FLM may be used during preterm labor episodes
Bed rest, hydration, and pelvic rest do not appear to improve the rate of preterm birth
Recommendations – Level B

ACOG Practice Bulletin. Assessment of Risk Factors for Preterm Birth. Number 31, October 2001, reaffirmed 2008.
ACOG Practice Bulletin. Management of Preterm Labor. Number 43, May 2003, reaffirmed 2008.
ACOG Committee Opinion . Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection. Number 455, March 2010.
Elliott, JP, et al. In Defense of Magnesium Sulfate. Obstetrics & Gynecology. 113(6):1341-1348, June 2009.
Grimes, DA, et al. Magnesium Sulfate Tocolysis: Time to Quit . Obstetrics & Gynecology. 108(4):986-989, October 2006.
Iams JD, et al. The Preterm Prediction Study: recurrence risk of spontaneous preterm birth. Am erican Journal of Obstetrics and Gynecology. 1998; 178: 1035-1040.
Lyell DJ. Magnesium sulfate compared with nifedipine for acute tocolysis of preterm labor: a randomized controlled trial. Obstetrics & Gynecology July 2007; 110(1): 61-7.
References