
Christine Schutz - ANZONAanzona.net/conf2013/A3_ChristineSchutz.pdf · Christine Schutz Research...
37
A systematic review of the effect of Tranexamic acid in knee and hip arthroplasty Christine Schutz Research Coordinator Wakefield Orthopaedic Clinic.
Transcript of Christine Schutz - ANZONAanzona.net/conf2013/A3_ChristineSchutz.pdf · Christine Schutz Research...
A systematic review of the effect of Tranexamic acid in knee and hip arthroplasty Christine Schutz Research Coordinator Wakefield Orthopaedic Clinic.

Overview
Background to how TX works
The studies of TX acid in Orthopaedics
Results of retrospective study at WOC
Blood management in elective THR and TKR surgery.
Conclusions re dose of tranexamic acid.
Where to from here?
Disclosures No conflict of interest
Thank you to ANZONA
Thank you to Surgeons at WOC
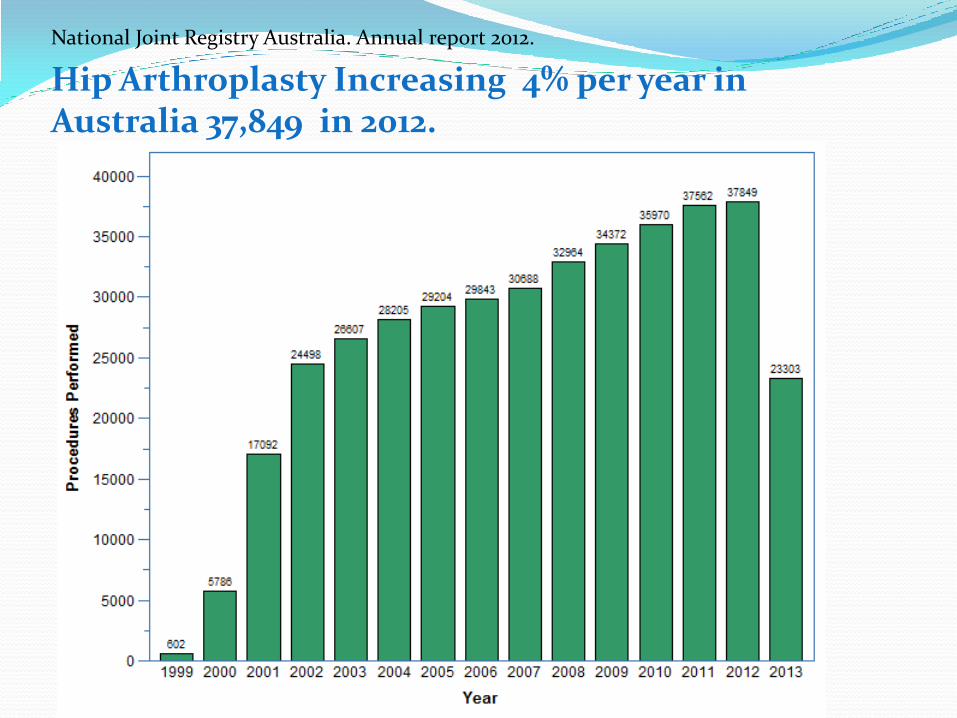
National Joint Registry Australia. Annual report 2012.
Hip Arthroplasty Increasing 4% per year in Australia 37,849 in 2012.
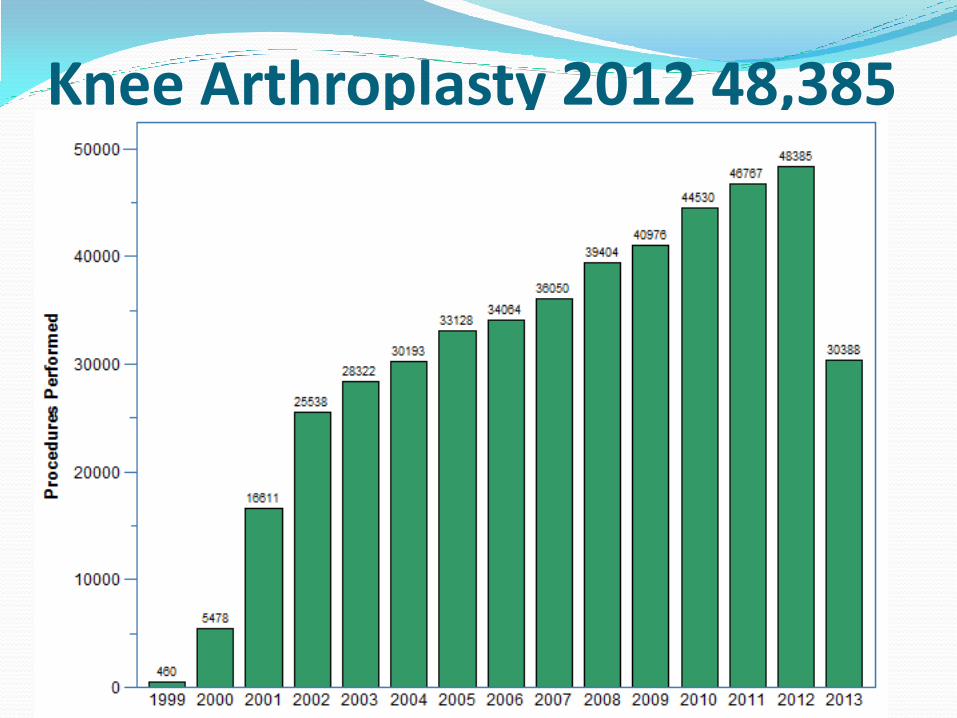
Knee Arthroplasty 2012 48,385
Indications for Joint replacement Pain : severity at rest, distance walking commonly due to
Osteoarthritis.
Function : Need for a cane, Climbing stairs, Daily living
Examination: ROM, Joint stability, other.
Radiographic. Joint space limited.

Tranexamic Acid Inhibits fibrinolysis by
blocking lysine-binding site of plasminogen to fibrin
Reduces blood loss and need for Blood transfusions

TX ACID Mechanism of Action. Tranexamic acid also know as CYKLOKAPRON in Aust. Given as IV , intra articular, oral, spray., Topical
Found to reduce blood loss in trauma and elective surgery reducing transfusion rates by a third.
Is a synthetic lysine derivative that stops the breakdown of fibrin by inhibiting activation of plasminogen.
Has a 2 hour half life. Excreted mainly via kidneys.
.

Contraindications for TX use Previous History of DVT Sensitivity to Tranexamic acid Visual problems colour disturbances Poor renal function. ____________________________________ COMMON SIDE EFFECTS: Nausea Vomiting and Diarrhoea Dizziness Hypotension Rash (allergic reaction) Over dosage rare.
CRASH 2 trial (Trauma) Largest trial published
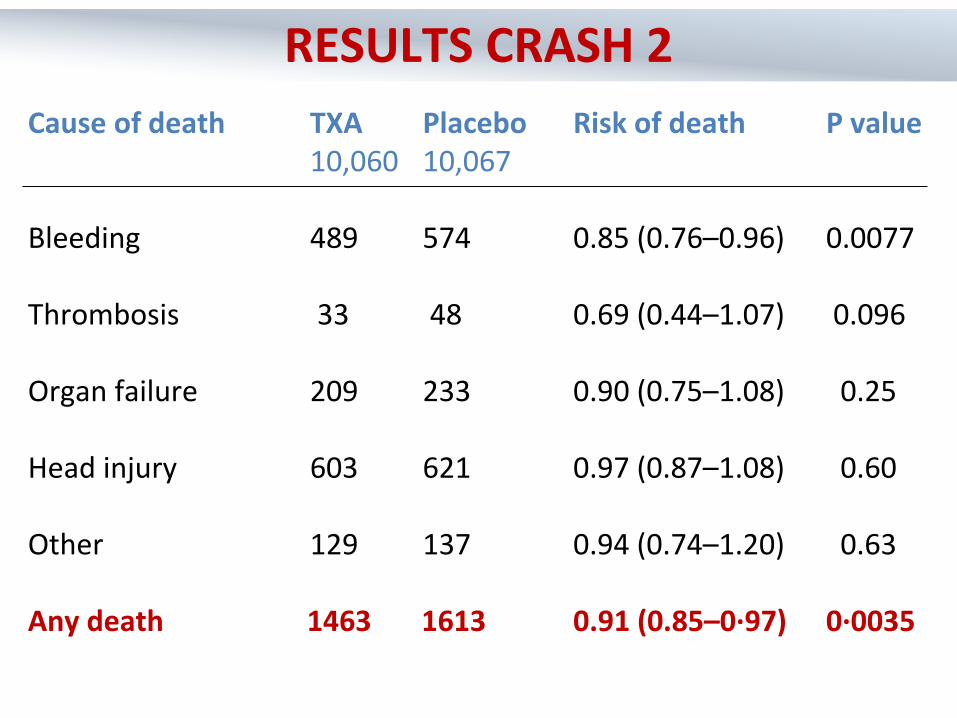
Cause of death TXA Placebo Risk of death P value 10,060 10,067 Bleeding 489 574 0.85 (0.76–0.96) 0.0077 Thrombosis 33 48 0.69 (0.44–1.07) 0.096 Organ failure 209 233 0.90 (0.75–1.08) 0.25 Head injury 603 621 0.97 (0.87–1.08) 0.60 Other 129 137 0.94 (0.74–1.20) 0.63 Any death 1463 1613 0.91 (0.85–0·97) 0·0035
RESULTS CRASH 2

Risk ratio (95% CI)
TXA worse TXA better
TXA
allocated
(10,060)
Placebo
allocated
(10,067)
Any 168 (1.63%) 201 (1.95%)
.6 .7 .8 .9 1 1.1 1.2
Stroke 57 (0.56%) 66 (0.65%)
DVT 40 (0.40%) 41 (0.41%)
PE 72 (0.69%) 71 (0.70%)
MI 35 (0.35%) 55 (0.52%)
There was no increase in thrombosis

Tranexamic acid dose Same for hips and knees.
15mg/kg initial dose IV
Follow 6 – 8 hrs post surgery

CYKLOKAPRON Solution for Injection IV
500mg ampoules in 5ml Water
1000mg ampoules in 10ml Water
Tablets available in 500mg (bottle of 100 tabs)

Use in Total Knee Arthroplasty meta analysis 16 randomised placebo controlled studies
11 = efficacy (reduced blood loss)
Mean age = 65-77 years
N= 365 tranx patients
N= 390 controls
Cemented and non cemented prosthesis used.
Post LMWH
Overall dose 10- 30mg/kg efficacy shown
Knee arthroplasty
Topical v Intra articular for TKA
• Antapur et al Bone and joint (2012)
• Study Number= 99 pts
• Randomized to 3 sub groups
• Doses 1.5, placebo and 3gm.
• Results:
• No difference in rate of transfusion between the 1.5g group and placebo
• The TX group of 3 g = 0 transfusion.
• 2 out of 99 pts had PE in the 1.5 g group.

Meta analysis of TKA trials Cochrane Bone, joint and Trauma J Bone Joint Surg Br 2011 Dec 93 (12 )
1577 - 85
Reduction in allogenic blood transfusion 16% (95% CI : )9-0.26
Total blood loss 460 mls
19 Randomized controlled trials.
Concluded that TX was effective and safe for use in TKA and reduced blood loss.
Tx does not increase prevalence of DVT or PE.

Timing of Administration of TXA 10 - 15 minutes before tourniquet released, repeat q 6 - 8
hrs for first day
Nielsen, Ugeskr Laeger 2002
One injection pre-op, one on release of tourniquet
Tanaka, JBJS (Br) 2001
Just prior to tourniquet release and 3 hrs later
Good, BJA 2003
Oral TX study Repat (50TKA) 25 acid/25 placebo in progress
Dose studies Andreau study (71 TKA )
Looked at 2 dose schedules. IV
Dose 1. Given IV in theatre 15mg/kg.
Dose 2 Given 3 hours post surgery 15mg/kg.
Group 1
Showed no Transfusion required in TX group.
Group 2 (control)
37 % requiring Transfusion in non TX group.(autologous blood)
Tourniquet times 86-92 mins

• Arthroplasty Hip and Knee with DVT prophylaxis.
• Review presented by Blake et al July 2012
• Low risk of Thromboembolic Complications
• N = 2246 primary THA and TKA
• Dose TX = 1 g IV beginning and at closure.
• Results: rate of DVT similar across groups
• p = 0.61
• Aspirin alone
• Warfarin
• LMWH
Dose studies some concerns Lack of information
regarding DVT prophylaxis and use of TX acid.
Variable dose regimes
Multiple confounding variables
1st Dose of commencement of injectable LMWH post operatively unclear.

• Imai et al J of Arthroplasty V 27 2012
• BLOOD LOSS FOCUS.
• HIP________________________________
• N= 107 patients.
• Randomized to 5 groups (Dose and Timing)
• Found most effective dose for reduction of blood loss for hip arthroplasty
• 1g TXA given prior to surgery and 6 hrs post.
• Limited data on risks of DVT
TX in hip arthroplasty Limited dose selected studies
6 studies included in meta analysis
No studies that used the dose of 60mg/kg.
Same dosing is used as for knees.
Should be given as slow intravenous infusion
Loading dose 50mg/min
1g in 100ml can give at 5ml/min
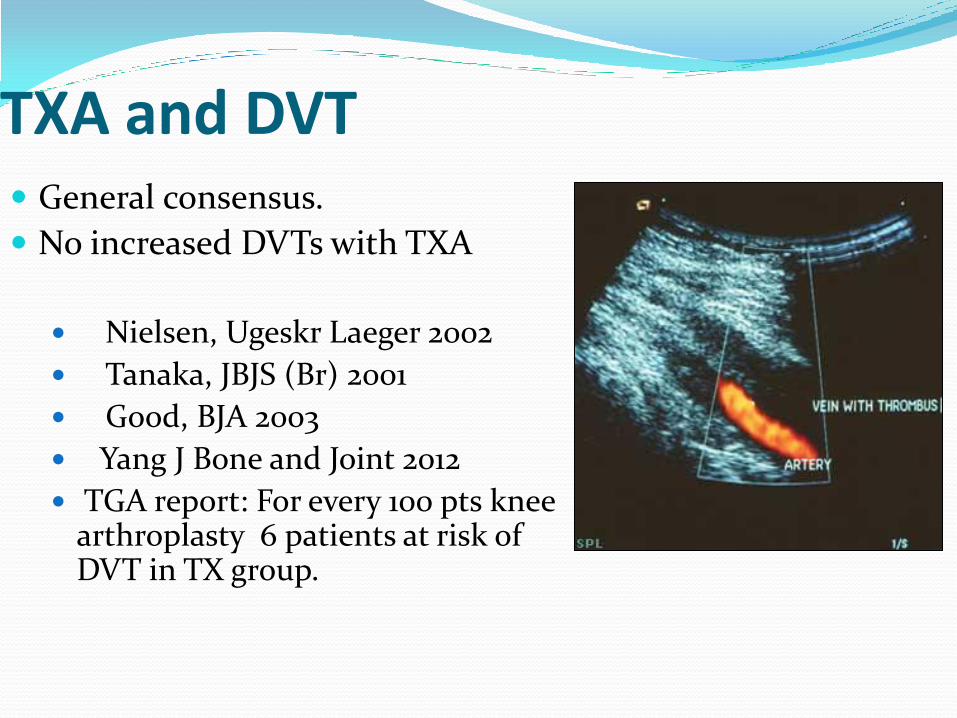
TXA and DVT General consensus.
No increased DVTs with TXA
Nielsen, Ugeskr Laeger 2002
Tanaka, JBJS (Br) 2001
Good, BJA 2003
Yang J Bone and Joint 2012
TGA report: For every 100 pts knee arthroplasty 6 patients at risk of DVT in TX group.
Meta analysis re blood loss Hiipala et al
No increase in Thromboembolic events.
Transfusion risk reduced by 64%
Dutch 10 yr Study (Slappendal)
80% less transfusion
40% less infection
Decreased morbidity
Reduced hospital duration
Trend Of DVT In TX reports. Recent FDA reports. May 2013 1505 people reported side effects of TX acid.
(Gastro type effects)
31 ie (2.06% ) with DVT
Most DVT occurred in < 1 month (88.24%)
1- 6 months DVT occurred in 11.76 %

Retrospective study at WOC Review of 354 records
Hip (151)
61 m
90 f
Knee (203)
86m
117 f

RESULTS OF REVIEW WOC
88 24
27
12
HIPs
TX
Blood and TX
Transfusion
No TX no Tf
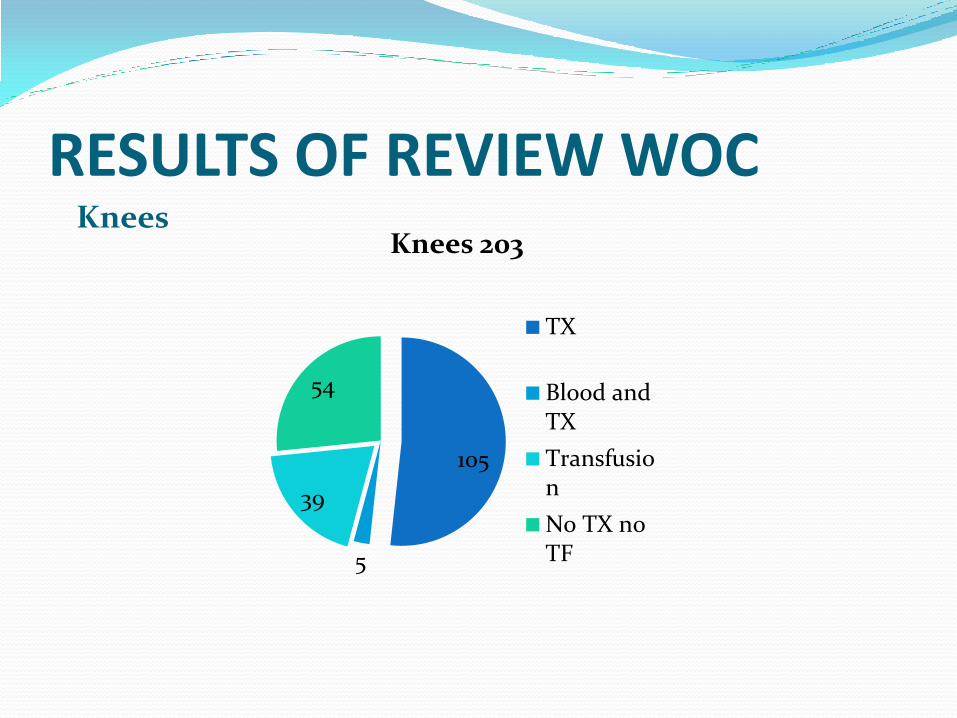
RESULTS OF REVIEW WOC Knees
105
5
39
54
Knees 203
TX
Blood andTX
Transfusion
No TX noTF

Adverse events for hip and knees
Hypotension (29 H) (17 K)
Pulmonary embolism (3 H)
Rash (6)
Confusion (5)
Clinical Perspective Blood management protocol
• Preoperative:
• Get sound history of bleeding v clotting
• Cease supplements eg fish oils etc.
• Cease NSAIDs antiplatelet meds and aspirin 7- 10 days before surgery.
• Discontinue warfarin 5 days prior check INR
• Check for preoperative anaemia.
• Consider iron therapy if <100 ug/l
Clinical Perspective Blood management protocol
• Perioperative management
• Revising the transfusion trigger to 8Hbg or below has been shown to be safe.
• Maintain normothermia
• Surgeon preference re tourniquet and drain.
• TX given by anaesthetist 15mg/kg before tourniquet release and 2nd dose surgeon pref.

Clinical Perspective Blood management protocol.
• Post operative
• Maintain normothermia
• Limb elevation
• Withhold thromboprophylaxis until surgical haemostasis (ie 6-8 hrs)
• Check Hg status transfusion trigger post 8 hr surgery.(<8Hgb)
Conclusions TX Acid reduces mortality in bleeding trauma
patients. Reduces bleeding generally by 25- 30% and leads to decreased transfusion rates.
TX acid Preoperatively in Total Knee Replacement does not increase incidence of DVT and PE Best dose : how, timing, and dose ????
Preoperative anaemia , intraoperative blood loss and post operative care can be influenced by blood management protocols.
Audit regularly TX administration. Dose studies needed

References Blake et al Clinical orthopaedic Research July 2012
Alvarez J et al Transfusion 2008 48: 519 -525
Benoni C Acta othopaedics Scand 2001 72: 442-448
Naudi Douglas Ralley Clinical Orthopaedics and related research July 2010 V 468 pg 1905
Product Information Cyklokapron p 1- 27.
Imai et al Arthroplasty 2012

Thankyou


















