Chorea
38
Case presention
Transcript of Chorea

Case presention

20 y old ethiopian female pt, presented to hospital w h/o sudden onset Of abnormal movement in lt arm and lt lower limb.Pt was well befor and has no medical disease befor.No h/o fever or headach or loc orvomitting or visual impairment.No previous h/o same complain beforNo h/o chest pain ,sob,cough or palpition.No h/o abdominal painjaundice , BHC.No h/o joint pain or skin changes befor.No h/o new drugs intak.FH:no similar complainSH:single, not work.non smoker.PMH:no previous hospitalization or drugs intake or allergy


O/EPt awake,has normal speech,follow command,w abnormal behivoure.Vitally stableCranial nerve :normalMotor: has abnormal movement in lt side,as invoulntary jerky ,rapid,
resless brief at proximal joint.rt side weakness<hypotonia ,Hyper reflexia, toe is upgoing.Sensory and coordination was normal

DD
VASCULAR as ischemic stroke involve bg either venous or arterial or hg
or AVM
Sydenham chorea
Infection as diphteria, brucella,pertussi,hsv,hiv,infectious mononuclosis,lyme.mycoplasma.measles, mumps,rubella.
Vasculitis
SLE , APLS
Metabolic as hypocalcemia ,magnesimia,natremia,hyo or hyoer glycemia,vit b12 def,hypotd.hypo ptd.wilson d..
Drugs as OCP,AED.Antipsychotic

Pt admitted as acase of chorea
Her intial investigation as cbc,u&e, lft , pt,ptt,glucos.ca, mg was normal
ESR was 105, CT brain show lt occipital and rt thalamus and IC hypodensity.
-Started on halopredol, sodium valoprate,artan, asa and zocor
Ct brain w contrast was ordered to r/o CVT as MRI techniqe not available.
Cvt was r/o
Brucella, salmonella,ANA,TFT was normal.
HIV was poitive
.



So final x is hemichorea seconrey to ischenic stroke involving BG and subthalamas.
PML in HIV pt.
Demylinated disease involve BG.
TO R/O TUMORE
FINAL DIGNOSIS

CHORA
IS sudden brief spontenouse, involuntry purpoles,continouse,irregular and unpredictable jerkson facial,truncal musculture.
CAUSES OF CHOREA IN ADULT:
Hereditary:
Huntington disease
HDL1,HDL2,HDL3
Herditery non progressive chorea
Neuroacanthoytosis
DRPLA
SCA17
Ataxia talengectasia
Wilson disease
Lesh nyhan syndrom

Secondery
Infection or immunologic
as sydenham chora, encaphalities
SLE, APLS
Drug induced as
AED as phenytoin ,antipsychotic ,levodopa,anticholonergic,ca chanel blocher
Metabolic as
chorea gravidarum,hyperthyrodism,OCP, hyperosmolar non ketotic hyerglycemia encaphalopathy
Vascular as
hemichorea, hemiballismus w subthalamic lesion.or postpump chorioathetosis after cardic surgery
Unknown as
senile chorea or essential chorea

COREA IN CHILDHOOD
Ataxia talengectasia
HD,WD,halleverdon-spatz,in born error of metabolism as
Glutaric acidemia, propionic acidemia,homocystenemia,PKU,sulfite oxidase deficiency
Mitochondria encaphalomyopathies
Pyruvate carboxylas def
Neuroacanthocytosi
Adrenal insufficiency
Anoxic encaphalopthy
Encaphalitis
GM1
Gangliosidosis
Hypocalcemia
Lesc-nyhan syndrom

SYDENHAM CHOREA
It is the most common acquired chorea in young age.
Associated w strain of gp A beta haemolytic streptococcus infection w induce antibodies that cross react w neural cytoplasmic ag in caudate and thalamus.
Also associated w imbalance arise from dopaminoergic system, intrastraited choenergic system,inhanced GABA.
Incidence:
Higher in developing countrie,in female more than male by ratio of 2;1
Age: onset 5-15
Sometime postive family history of RF &sydenham chorea
Clinical pictures:
Pt may present in delayed 6 m or more of onset of RHD.
Pt present w hypotonia, ild muscle weakness< uni or bilateral>
Mostly at rest aggrevated bystress, ceas w sleep.

20%in one side<hemichorea>
It interfer w mivement causing clumsy gait dropping, slipping,explosive dysarthia.
Inability to sustain contraction<milkmaid grip.>
Pronator sign w consist of hyperpronation of hand causing palm to face outward when arms are held over head.
Associated w personality changes, emotional liability,anxity and obssesive compulssive disorder.
Investigation:
High ASO ab titer in serum, 25% has negative evidence of infection.
Antineural ab is high in csf
MRI will show high signal intensity in t2 involve BG and cerebral white matter w localized swelling.
Functional PET show reversable straital hypermetabolism.

Treatment of sc:
AED as valopric acid or carbamezapin at dose used in tt of sz.
Dopaminergic blocker as halopridol, pimozide w start in small dose then increase gradulaay.
IVIG and PE is effective against anti neural AB.
Prophylactic pencillin for at least 10 y to prevent other RHD symptoms.
Prognosis:
Resolve spontenously in 3-6 months, rarly to last more than 1 year.
Mild chorea w out functional disability may be found up to 10 y after intial attack>

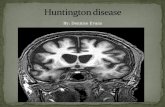
HUNTINGTON DISEASE
It is an ADD
From parenta to childeren
Involove gliosis of caudate and putman along w regional or more diffuse atrophy of 20% of brain.
Incidence:
Age of onset 30-55 and can present between 2-92
10 in each 100000 of population
Common in sctaland ,india,japan,china and venzuila
Prensent as juvenil or in adult age
Clinical fetures:
Start as clumsiness then turn to chorea.
Bradykinesia and difficulty in sustaining ongoing movement.
Cant maintain eye closed or hold mouth open or protude toung for long time

W the time progress to bradykinesia and dystonia.
Lately ot show irritability of gait , sadness sleepdisorder.depression.decrease motivation and memory and wt, bladder incotince, swallowing difficulties and speech disorder.
Laps of tone of antigavity muscle.
Walking resemble marionette, lurching, swaying, dipping and bobbing.
Tandem gait difficultythen become immpossible.
Intractable falls lead to wheelchair or bedbound.
Dysphagia and dysathia prgressivly impaire nutrition and communication.
Most pt spend last years of them life in nursung homesetting and die from pneumonia or head injury.
Demensia is subcortical include decrease attension. Motivation,judgement,insight and problem solving.
Mean survival age is 17 years.

Investigation:
Gentic testing
MRI show generalized striatal atrophy.
Somatosensory evoked potential is abnormal in 94%.
Treatment:
Trial of coenzyme 10 and antiexcitatory agent as Remacemide were disappointing.
Glutamic antagonist as Amantadine 4oomg.
Antidopaminergic as tetrabenazine.
SSRI improve irratability and aggresiveness and ocd.
Valopric acid and CMZ and olanzepin.
JHD:
aADD degenerative disease associated w progressive cognative decline.
Age: onset 35-40 sometime befor age of 4 year.

Etiology:
Genatic mutation at expanded DNA trinuclotide CAG repeat within coding region as more than 38 repeat.
10% of carrier of this gene has onset of clinical manifastion befor 20y.
70-80% inherte this gene from affected father.
1%have negative genatic test.
Clincal manifastion:
In child differnet than adult as mental retardation and rigidity apear clumsy intially then gait disturbance.
Cerebellar sign.
Seizure in 30-50% of patient and difficult to controll.
Diagnosis:
Gentaic test to find the size of gene repeat.

MRIbrain:atrophy of caudate and high signal of putman.
PET:
Marked reduction of glucose metabolism at caudate.
Treatment:
CMZ as mood stabilizer.
Respererine.
Dopaimine antagonist as L-dopa helpful for rigidity, but may be proveked hallucinaion and psychosis and excerbete chorea.
Bq hereditery chorea:
Rare familial ADD disease w onset in early childhood releated to expanded CAG repeat mutation at chromosome 14.
Clinically:
Onset of manifastion at childhood at age of beging of walking and diminsh at adolscence associated w dysarthia and athetosis and hand tremor and hypotonia w no abnormal in cognative function.

DIGNOSIS:
PET:
Decrease in straital metabolism.
Treatment:
CMZ- phenytoin.
Halopridol.
Prednson
Dopamine antagonist.
NEUROACANTHOCYTOSIS:
It is the most common hereditery after HD w mild chorea in compare to HD.
Incidence:
Age of onset in young between 20-40 y, but can be apear in age between 8-62y.
Cause:
ARD include genatic mutation at chromosome 9 q21q22 coding for chorin

Protien leading to decrease in dopaminergic receptor at stritum binding and decrease in sub p in SN.
Erythrocyt membrene lipid is alterted as increase palmitic acid and decrease stearic acid.
Clinically:
Had tics occasionally associae w sz in one third of patient and amotrophy and abscent tendon reflux.
Also has feeding dystonia,toung push food out of mouth>. Aslo linglabial dyskinesia as self multiation w lip and touge bitting.
Sometime has dystonia and parkinsonism at onset of disease.
In rare cases may have Mc lead phenotype associated chorea & sz&peripharal neuropathy&liver dysfunction and haemolysis.
Investigation:
Blood smear will show spiky erythrocyte more than 15% w normal lipoprotenemia.
MRI brain:t2 show hypermetabolism in straitum.
Treatment: AED asVA or CMZ.

WILSON DISEAS:
ARD due to mutation of chromosome 13 at wc1 gene encoding for copper transporting p- type adenosin w express in liver and kidney.
Copper will be accumalate in liver ,kidney ,cornea and brain.
Clinically:
Pt present at age of 3-50 y.50%has hepatic manifastion at intial symptomsin form of fulminate hepatic failure, cirrhosis,CAH or hepatomegally, and mostly at child age befor 10.
Untreated individual eventually develop neurological manifastion,40% in second decad of age as chorea, dysarthia, dysphagia, instability of gait and dystonia and bradykinesia,intellectual delay and psychiatric disorder as depression ,emotional liability and personality changes.
WD pt may develop haemolytic anaemia and RTA.
Slet lamp examination show kayser fischer ring w consist of copper deposition at periphery of cornea.

Investigation:
24 h urine ca exceretion show high copper in urine.
Liver biobsy to determin high copper content in liver tissue, it is the most sensitive test, but normal in 5-15% of pt.
Treatment:
Decrease copper containg diet
Decrease absorption of copper
Chealating agent
Liver transplant.
DRPLA<DENTORUBROPALLIDOLYSIAN ATROPHY:>
<Haw river syndrome>
It is an ADD,include mution in expanded CAG gene w repeat of 49-75 at chromosome 12.
Most common at young age in african amircan and japan.
Include degeneration in dentate, red nucleuse,GB,STN and white matter..pt present w chorea, ataxia, dystonia ,myoclonic sz and demensia

HUNTIGTON LIKE DISEASE:
When neuroacanthocytosis and HD was excluded by gene marker should consider less common disorder called HDL.
Has 3 typs:
HDL1:
ADD,include mutation at chromosome 20 ectopeptide repeat gene at prion protien.
HDL2:
Common in african include repeationat CAG gene and CTG gene at chromosome 16encoding for protien link between plasma mb and endoplasmic retinculum.
HDL3:
ARD expanded CAG gene, pt present at age of 3-4 y w chorea ,dystonia,ataxia,gait unstability, spastic sz, mutisim and intellectual impairment. Pt has bilateral frontal&caudate atrophy

HERDITERY NON –PROGERESSIVE CHOREA:
<Essential tremor>
ADD at childhood age.
Linked to chromosomal14 q13.1q21
Run in families
Only features is chorea
Dignose be PET w show straial hypometabolism.
SENILE CHOREA:
No family h/o.
No demensia.
Begain insidouse,mild,involuntery limb, face,buccal movement.
Slow in intensity.
DNA test ½ CAG expand.
Dx by MRI brain w show mild caudate and putman atrophy.

SLE:
APL-Ab lupus anticagulant heterogenouse gp of Ab causing thrombosis,intermittent chorea
PET :normal.
TT:antidopamine.
APLS:
Younger age.
Pt have migrane.spontenous abortion,,thickend cardic valve, livedo reticularies,raynaude phenomena,multi infarct demensia.
Prolonged PT.
High ACLA.
PET:has straital hypermetabolism.
TT:
Anticoagulant,immunosupresent,plasma exchange.

VASCULAR:
Age: middle to eldery
Sudden onset on one side.
As choretic movement in arm and leg associated w ballism more violent than chorea w larg amplitude ,uncoordinated forceful movement of proximal muscle ,present at rest suppress by involuntery. It may present w hemiplasia or hemiparesis.
Its due to destruction lesion in cl subthalamus and its connection.
Vascular lesion either hg or ischemia.
Tumor or plaque of MS in subthalamus or can followed thalamectomy.
Movement tend to diminshed w time.
DD of hemichorea or hemiballismus:
It seen also in AIDS, toxoplasma involve STN w respond to antidopaminergic medication.
Also seen in hyperosmolar non ketotic hyperglycemia releated to hypoperfusion of straitum.

Post-cardic surgery for CHD pt using pump for long time associated w deep hypothermia and circulatory arrest.
Lesch-Nyhan syndrome (LNS), also known as Nyhan’s syndrome or Kelley-Seegmiller syndrome, is a rare, inherited disorder caused by a deficiency of the enzyme hypoxanthine-guanine phosphoribosyltransferase (HGPRT), produced by mutations in the HPRT gene. The lack of HGPRT causes a build-up of uric acid in all body fluids: both hyperuricemia and hyperuricosuria, which lead to problems such as severe gout and kidney problems, poor muscle control, and moderate mental retardation. These complications usually appear in the first year of life. A striking feature of LNS is self-mutilating behaviors, characterized by lip and finger biting, that begin in the second year of life. Neurological symptoms include facial grimacing, involuntary writhing, and repetitive movements of the arms and legs similar to those seen in Huntington's disease. The direct cause of the neurological abnormalities remains unknown. Because a lack of HGPRT causes the body to poorly utilize
vitamin B12, some boys may develop megaloblastic anemia ,

LNS is an X-linked recessive disease: the gene mutation is usually carried by the mother and passed on to her son,
although one-third of all cases arise de novo (from new mutations) and do not have a family history .LNS is present at birth in baby boys.
Most but not all persons with this deficiency have severe mental and physical problems throughout life. There are a few
rare cases in the world of affected females.[2]The symptoms caused by the buildup of uric acid (gout and renal symptoms) respond well to treatment with drugs such as allopurinol that reduce the levels of uric acid in the blood.
The mental deficits and self-mutilating behavior do not respond well to treatment.
There is no cure, but many patients live to adulthood. Several new experimental treatments may alleviate symptoms. LNS is
rare, affecting about one in 380,000 live births.[3]

Signs and symptoms
LNS is characterized by three major hallmarks: neurologic dysfunction, cognitive and behavioral disturbances including self-mutilation, and uric acid overproduction (hyperuricemia). Damage to the basal ganglia causes sufferers to adopt a characteristic fencing stance due to the nature of the lesion. Some may also be afflicted with macrocytic anemia. Virtually all patients are male; males suffer delayed growth and puberty, and most develop shrunken testicles or testicular atrophy. Female carriers are at an increased risk for gouty arthritis, but are usually otherwise unaffected.
[edit ]Overproduction of uric acidOne of the first symptoms of the disease is the presence of sand-like crystals of uric acid in the diapers of the affected infant. Overproduction of uric acid may lead to the development of uric acid crystals or stones in the kidneys, ureters, or bladder. Such crystals deposited in joints later in the disease may produce gout-like arthritis, with swelling and tenderness.

The overproduction of uric acid is present at birth, but may not be recognized by routine clinical laboratory testing methods. The serum uric acid concentration is often normal, as the excess purines are promptly eliminated in the urine. The crystals usually appear as an orange grainy material, or they may coalesce to form either multiple tiny stones or distinct large stones that are difficult to pass. The stones, or calculi, usually cause hematuria (blood in the urine) and increase the risk of urinary tract infection. Some victims suffer kidney damage due to such kidney stones. Stones may be the presenting feature of the disease, but can go undetected for months or even years.
Nervous system impairmentThe periods before and surrounding birth are typically normal in individuals with LNS. The most common presenting features are abnormally decreased muscle tone (hypotonia) and developmental delay, which are evident by three to six months of age. Affected individuals are late in sitting up, while most never crawl or walk. Lack of speech is also a very common trait associated with LNS.Irritability is most often noticed along with the first signs of nervous system impairment. Within the first few years of life, extrapyramidal involvement causes abnormal involuntary muscle contractions such as loss of motor control (dystonia), writhing
motions( choreoathetosis )

arching of the spine (opisthotonus). Signs of pyramidal system involvement, including spasticity, overactive reflexes (hyperreflexia) and extensor plantar reflexes, also occur. The resemblance to athetoid cerebral palsy is apparent in the neurologic aspects of LNS. As a result, most individuals are initially diagnosed as having cerebral palsy. The motor disability is so extensive that most individuals never walk, and are confined to a wheelchair for life.
[edit ]Self-injuring behaviorPersons affected are cognitively impaired and have behavioral disturbances that emerge between two and three years of age. The uncontrollable self-injury associated with LNS also usually begins at three years of age. The self-injury begins with biting of the lips and tongue and as the disease progresses, affected individuals frequently develop finger biting and head banging. The self-injury can increase during times of stress. Self-mutilation is a distinguishing characteristic of the disease and is apparent in 85% of affected males.

The majority of individuals are cognitively impaired, which is not easy to determine because of the behavioral disturbances and motor deficits associated with the syndrome. In many ways, the behaviors may be seen as a psychological extension of the compulsion to cause self-injury: rejecting desired treats or travel, repaying kindness with coldness or rage, failing to answer test questions correctly despite study and a desire to succeed, provoking anger from caregivers when affection is desired, and so on.
Compulsive behaviors also occur, including aggressiveness, vomiting, spitting, and involuntary swearing, or coprolalia. The development of this type of behavior is sometimes seen within the first year, or in early childhood, but others may not develop it until later in life.LNS in femalesWhile carrier females are generally asymptomatic, they do experience an increase in uric acid excretion, and some may develop symptoms of hyperuricemia, and suffer from gout in their later years. Testing in this context has no clinical consequence, but it may reveal the possibility of transmitting the trait to male children. Women may also require testing if a male child develops LNS. In this instance, a negative test means the son's disease is the result of a new mutation, and the risk in siblings is not increase

In order for a female to be affected, she would need to have two copies of the mutated gene, one of which would be inherited from her father. Males affected with LNS do not usually have children due to the debilitating effects of the disease. It is possible for a female to inherit an X chromosome from her unaffected father, who carries a new mutation of the HPRT gene. Under these circumstances, a girl could be born with LNS, and though there are a few reports of this happening, it is very rare. The overwhelming majority of patients with LNS are male.DiagnosisWhen an affected individual has fully developed the three clinical elements of uric acid overproduction, neurologic dysfunction, and cognitive and behavioral disturbances, diagnosis of LNS is easily made. Difficulties of diagnosis are abundant in the early stages when the three features are not yet obvious. Suspicion often comes about when the developmental delay of the individual is associated with hyperuricemia. Otherwise, the diagnosis should be alleged when developmental delay is associated with kidney stones (nephrolithiasis) or blood in the urine (hematuria), caused by uric acid stones. For the most part, Lesch-Nyhan syndrome is
first suspected when self-inflicted injury behavior develops. .

Diagnostic approachThe urate to creatinine (breakdown product of creatine phosphate in muscle) concentration ratio in urine is elevated. This is a good indicator of acid overproduction. For children under ten years of age with Lesch-Nyhan syndrome, a urate to creatinine ratio above two is typically found. Twenty-four-hour urate excretion of more than 20 mg/kg is also typical but is not diagnostic. Hyperuricemia (serum uric acid concentration of >8 mg/dL) is often present but not reliable enough for diagnosis. Activity of the HGPRT enzyme in cells from any type of tissue (e.g., blood, cultured fibroblasts, or lymphoblasts) that is less than 1.5% of normal enzyme activity confirms the diagnosis of Lesch-Nyhan syndrome. Molecular genetic studies of the HPRT gene mutations may confirm diagnosis, and are particularly helpful for subsequent 'carrier testing' in at-risk females such as close family relatives on the female side

Treatment of chorea:
Halopridol:
Start w 0.5 mg-2mg /day
Increase gradually to satisfactory result.
SE:sedation ,akinesia,traditve kinesia,dystonia,cognative impairment.parkinsonism features.
Benzodiazepin:
As clonazepam, diazepam are used in early stage.
SE: sedation.
Na valoprate:
15-20 mg/day
Show subside of symptoms in child w 1 week.

Tetrabenazine:
Presynaptic depletor of dopamine
SE:
Traditive dyskinesia ,depression,drowsness,orthoststic hypotension,increase wt.
Dopamine antagonist:
SE: traditive kinesia
Pimozide:
0.2mg/kg/day
Should fu ECG bec it prolonged QT interval.