Choosing Appropriate Support Surfaces Betsy Willy MA, PT, CWS Pathway Health Services September 11,...
32
Choosing Appropriate Support Surfaces Betsy Willy MA, PT, CWS Pathway Health Services September 11, 2012
-
Upload
krista-ferrett -
Category
Documents
-
view
237 -
download
0
Transcript of Choosing Appropriate Support Surfaces Betsy Willy MA, PT, CWS Pathway Health Services September 11,...

Choosing Appropriate Support Surfaces
Betsy Willy MA, PT, CWS
Pathway Health Services
September 11, 2012
Lack of Standardized Testing
• Results in inability to compare products• Standardized Testing Initiative by NPUAP
– Began with standardizing terms and definitions – Established standards for testing materials– Recruiting participants to develop research to
compare products using standardized measures
• Outcome – to provide the clinician with an evidence based system to choose appropriate support surface

Definition of Support Surface (NPUAP)• “A specialized device for pressure redistribution
designed for management of tissue loads, micro-climate, and/or other therapeutic functions” – Any mattresses– Integrated bed system– Mattress replacement– Overlay– Seat cushion– Seat cushion overlay

Updated Terminology
• Static = non-powered
• Dynamic = powered
• Pressure reduction or relief = Pressure Redistribution

Elements Critical To Pressure Ulcer Prevention
• Low Moisture retention
• Reduced heat accumulation
• Shear reduction
• Friction reduction
• Pressure redistribution

Properties to Consider
• Envelopment – the ability of the support surface to conform, so to fit or mold around irregularities in the body
• Immersion - The depth of penetration (sinking into a support surface)
• Life Expectancy – the defined period of time during which a product is able to effectively fulfill its designated purpose

Components of Foam Support Surfaces• Viscoelastic Foam – (memory foam)
– a type of porous polymer material that conforms in proportion to the applied weight
• Elastic Foam – (non-memory foam used for packing boxes)
• Open cell foam – (sofa cushion)– permeable structure with no barrier between cells allowing
gases or liquids to pass through the foam
• Closed Cell Foam– Non permeable structure preventing gases or liquids from
passing through the foam
Other Components of Support Surfaces
• Air – in cells or bladder
• Gel – in combination or alone
• Water
• Solid (solid seat insert)
• Combination – foam/gel

Types of Support Surfaces
• Foam Overlay (add height to mattress)• Water mattress• Alternating Air Pressure• Low Air Loss • Air Fluidized (glass beads with air)• Zone (pressure can be controlled by zone)• Multi zoned surface• Lateral Rotation (rotates about a longitudinal axis –
degree of turn, duration and frequency)

Low Tech Support Surfaces Non Powered

High Tech – Powered Support Surfaces

Desirable Characteristics
• Prevents loads surpassing Capillary Closing of 32 mm/hg pressure
• Reduces moisture and heat accumulation• Reduces shear and friction• Is easy to use and maintain• Is economical• Allows for spontaneous movement on the
support surface

Cochrane Collaboration Podcast• Due to poor quality of
the studies to date (2011), comparison of the qualities between various products cannot be supported by current research.
• Recommendations for practice:– High risk individuals
should be provided replacement alternating air mattress rather than overlay
– Very high risk individuals should be provided high tech mattress such as low or high air loss

Support Devices (WOCN)
Performance Characteristics
Air fluidized
Low air
loss
Alternating air
Static Flotation
Foam Standard Mattress
Increased support area
Yes Yes Yes Yes Yes No
Low Moisture retention
Yes Yes No No No No
Reduced heat accumulation
Yes Yes No No No No
Shear Reduction
Yes ? Yes Yes No No
Pressure reduction
Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low

NPUAP Recommendations• “Support surfaces alone
can neither prevent nor heal pressure ulcers.” – Use as part of a total
program of prevention and treatment
• Use standardized risk assessment tool in conjunction with comprehensive assessment to determine risk level and Tissue Tolerance Tool
• When PrU deteriorates or fails to heal, consider replacing support surface with one that provides more aggressive pressure redistribution, heat and moisture reduction
• Reevaluate the whole person for root cause

Overall Goal of Support Surface
• Evenly distribute pressure over large area
• Allows person to immerse (sink into surface
• Decreases heat and moisture

Overall Recommendations

Overall Recommendations
• Do not use egg crate or foam overlays
• An individualized turning schedule should be assessed with each surface
• Turning and repositioning is required for all products
• Off load heels on any surface
• Assess products periodically for “bottoming out” and document monitoring
• The less padding between the skin and support surface, the more effective the surface can be
• Foam has a defined life expectancy – when a cushion retains the shape of the buttocks, it needs to be discarded

Shear WoundsContributing factorsContributing factors Tear Drop shaped wounds caused by
separation of tissues when skin remains stable on support surface and boney structure slides resulting in facial tissue tears
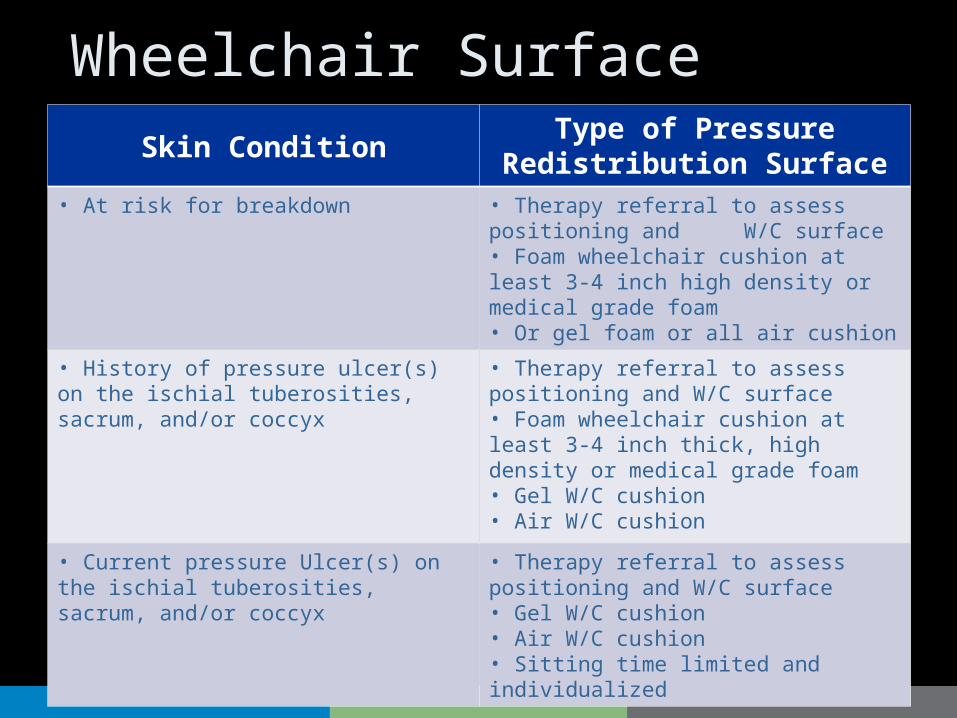
Wheelchair SurfaceSkin Condition
Type of Pressure Redistribution Surface
• At risk for breakdown • Therapy referral to assess positioning and W/C surface• Foam wheelchair cushion at least 3-4 inch high density or medical grade foam• Or gel foam or all air cushion
• History of pressure ulcer(s) on the ischial tuberosities, sacrum, and/or coccyx
• Therapy referral to assess positioning and W/C surface• Foam wheelchair cushion at least 3-4 inch thick, high density or medical grade foam• Gel W/C cushion• Air W/C cushion
• Current pressure Ulcer(s) on the ischial tuberosities, sacrum, and/or coccyx
• Therapy referral to assess positioning and W/C surface• Gel W/C cushion• Air W/C cushion• Sitting time limited and individualized

Off-loading Heels and Feet• Side lying: Lateral
aspect of foot must be off-loaded – Pillow under lateral calf of
lower leg in side lying– Pillow between knees– Ensure feet are not
touching support surface on any product
• Ambulatory – Non-weight bearing on
ulcerated foot
• Supine – Pillow under calf suspending heels– Ensure feet are not
touching support surface– Body pillow or pillows
under fitted sheet is harder to displace
• Sitting – Use heel free device– Foam boots do not
redistribute pressure
Motorized Scooter and Bedside Recliner
• 3-4 inch foam cushion places the center of gravity of the individual too high for fall prevention
• Use one inch gel cushion
• Limit time on device if this intervention is not adequate to prevent non-blanching red areas or to promote healing of pressure ulcer

Maintenance and Replacement• Follow manufacturers
directions for pressure settings
• Alarm lights on low air loss mattresses – Look first for air leaks with
stethoscope
– Check air hose connections
– Check pump function
• Monitor and document that device is functioning
• Check all air devices for adequate inflation– Place flat hand under device
– Push up into air
– Should be able to displace air to within 2 inches of body part
– If you can touch the boney prominence, increase air pressure
Wheelchair cushions
• Open the cover and check components of cushion – Check for wear or deterioration of foam and
gel– Ensure proper inflation if air cushion– Research supports – the more
interconnecting air cells, the more aggressive the pressure redistribution will be through immersion
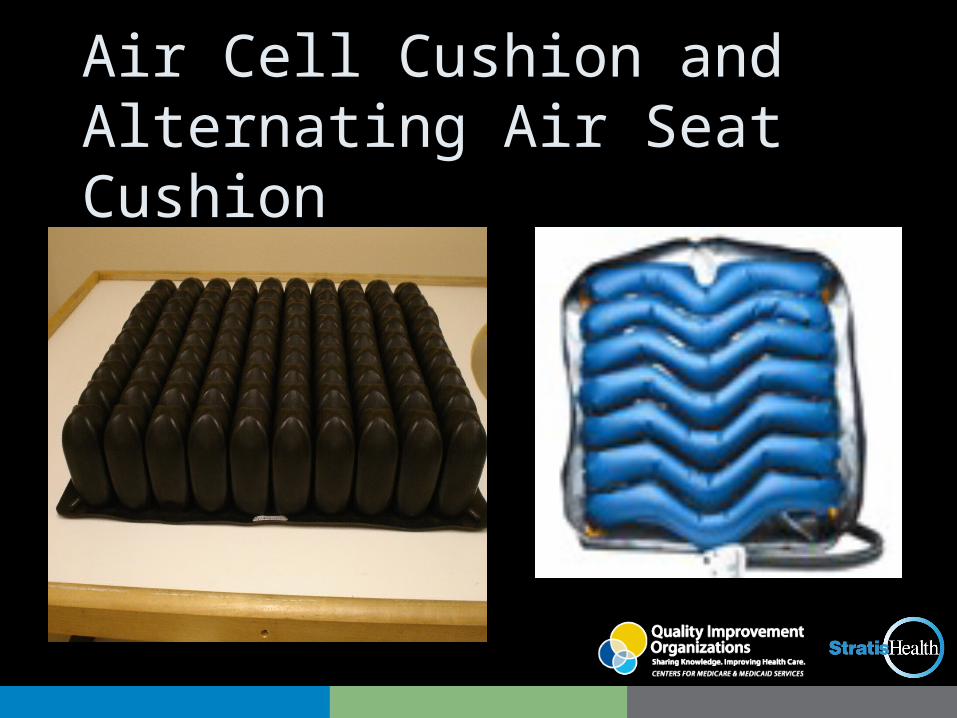
Air Cell Cushion and Alternating Air Seat Cushion
Geri Chair vs Tilt in Space • Severely contracted
individuals– Require complex
positioning in bed – refer to therapy for assistance
– Seating • Tilt in space chairs
accommodate contractures better than Geri Chair
• If geri chairs are used, add gel overlay and limit time exposed to pressure
• Constant movement– Huntington’s Disease
• Wider bed• Reduce friction• Padded wall and floor
• Sliding into sacral sitting– Prevent shear and friction
• “Dump” seat or use Gravity assisted Seating by changing the wheel position to lower the back of the chair seat

Kyphotic Back• Spinous processes at
high risk – Choose wheelchair back
that will conform to the individual’s back
• Keyhole – Keen
• Jay Personal back – Jay
• Deep Incrediback or moldable incrediback by Comfort Care
– Increase seat depth to decrease pressure per square inch
– Drop back of seat to prevent sliding
Sacral Sitting• If due to high extension
tone as in Parkinson’s Disease– To decrease tone and
stabilize pelvis try anti-thrust cushion with gel under coccyx and ischial tuberoscities with pelvic belt to stabilize
– Belt is not a restraint if person is dependent
– Lower seat back if needed

Sacral Sliding
• Avoid use of wedge cushion by dropping back of seat– Put back wheel in
highest axel position – Front caster in lowest
axel position – If this raises the knees to
high to allow feet flat for self propelling, start with a lower chair frame (hemi or super hemi)

Resources• National Pressure Ulcer Advisory
Panel Support Surface Standards Initiative; Terms and Definitions Related to Support Surfaces 01/29/2007
• Pressure Ulcer Prevention and Treatment; Quick Reference Guide 2009 EPUAP and NPUAP (www.npuap.org)
• Wound Care; A Collaborative Practice Manual for Health Professionals, 3rd edition; Carrie Sussman, Barbara Bates-Jensen; 2007 Lippincot, Williams and Wilkins
• Wound Resource Manual; Long Term Care 4th edition, Pathway Health Services (www.pathwayhealth.com)
• Cochran Collaboration PodCast 6/2011; Jill Hetherington; Efficacy of use of pressure relieving support surfaces in prevention of pressure ulcers
• Wound, Ostomy, and Continence Nurses Society (WOCN). Guideline for prevention and management of pressure ulcers.
Stratis Health is a nonprofit organization that leads collaboration and innovation in health care quality and safety, and serves as a trusted expert in facilitating improvement for people and communities.
This material was prepared by Stratis Health, the Minnesota Medicare Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The materials do not necessarily reflect CMS policy. 10SOW-MN-C7-12-116 083112