Cholera
15
Cholera 1 Cholera Cholera Classification and external resources Scanning electron microscope image of Vibrio cholerae ICD-10 A00 [1] ICD-9 001 [2] DiseasesDB 29089 [3] MedlinePlus 000303 [4] eMedicine med/351 [5] MeSH D002771 [6] Cholera is an infection of the small intestine caused by the bacterium Vibrio cholerae. The main symptoms are watery diarrhea and vomiting. Transmission occurs primarily by drinking water or eating food that has been contaminated by the feces (waste product) of an infected person, including one with no apparent symptoms. Severe cholera, requiring hospitalization, results from the accumulation of about a million bacterial cells within the body. [medical citation needed] The severity of the diarrhea and vomiting can lead to rapid dehydration and electrolyte imbalance, and death in some cases. The primary treatment is oral rehydration therapy, typically with oral rehydration solution, to replace water and electrolytes. If this is not tolerated or does not provide improvement fast enough, intravenous fluids can also be used. Antibacterial drugs are beneficial in those with severe disease to shorten its duration and severity. Worldwide, it affects 3–5 million people and causes 100,000–130,000 deaths a year as of 2010[7]. Cholera was one of the earliest infections to be studied by epidemiological methods. Signs and symptoms The primary symptoms of cholera are profuse diarrhea and vomiting of clear fluid. These symptoms usually start suddenly, half a day to five days after ingestion of the bacteria. The diarrhea is frequently described as "rice water" in nature and may have a fishy odor. An untreated person with cholera may produce 10 to 20 litres (3 to 5 US gal) of diarrhea a day. Severe cholera kills about half of affected individuals. Estimates of the ratio of asymptomatic to symptomatic infections have ranged from 3 to 100. Cholera has been nicknamed the "blue death" because a victim's skin turns bluish-gray from extreme loss of fluids. [8]
-
Upload
jorge-cano-nistal -
Category
Documents
-
view
16 -
download
2
Transcript of Cholera

Cholera 1
Cholera
CholeraClassification and external resources
Scanning electron microscope image of Vibrio cholerae
ICD-10 A00 [1]
ICD-9 001 [2]
DiseasesDB 29089 [3]
MedlinePlus 000303 [4]
eMedicine med/351 [5]
MeSH D002771 [6]
Cholera is an infection of the small intestine caused by the bacterium Vibrio cholerae.The main symptoms are watery diarrhea and vomiting. Transmission occurs primarily by drinking water or eatingfood that has been contaminated by the feces (waste product) of an infected person, including one with no apparentsymptoms. Severe cholera, requiring hospitalization, results from the accumulation of about a million bacterial cellswithin the body.[medical citation needed]
The severity of the diarrhea and vomiting can lead to rapid dehydration and electrolyte imbalance, and death in somecases. The primary treatment is oral rehydration therapy, typically with oral rehydration solution, to replace waterand electrolytes. If this is not tolerated or does not provide improvement fast enough, intravenous fluids can also beused. Antibacterial drugs are beneficial in those with severe disease to shorten its duration and severity.Worldwide, it affects 3–5 million people and causes 100,000–130,000 deaths a year as of 2010[7]. Cholera was oneof the earliest infections to be studied by epidemiological methods.
Signs and symptomsThe primary symptoms of cholera are profuse diarrhea and vomiting of clear fluid. These symptoms usually startsuddenly, half a day to five days after ingestion of the bacteria. The diarrhea is frequently described as "rice water"in nature and may have a fishy odor. An untreated person with cholera may produce 10 to 20 litres (3 to 5 US gal) ofdiarrhea a day. Severe cholera kills about half of affected individuals. Estimates of the ratio of asymptomatic tosymptomatic infections have ranged from 3 to 100. Cholera has been nicknamed the "blue death" because a victim'sskin turns bluish-gray from extreme loss of fluids.[8]

Cholera 2
Typical "rice water" diarrhea
If the severe diarrhea is not treated, it can result in life-threateningdehydration and electrolyte imbalances.
Fever is rare and should raise suspicion for secondary infection.Patients can be lethargic, and might have sunken eyes, dry mouth, coldclammy skin, decreased skin turgor, or wrinkled hands and feet.Kussmaul breathing, a deep and labored breathing pattern, can occurbecause of acidosis from stool bicarbonate losses and lactic acidosisassociated with poor perfusion. Blood pressure drops due todehydration, peripheral pulse is rapid and thready, and urine outputdecreases with time. Muscle cramping and weakness, alteredconsciousness, seizures, or even coma due to electrolyte losses and ionshifts are common, especially in children.
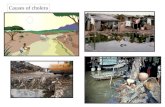
Cause
Vibrio cholerae, the bacterium that causescholera
Transmission is primarily by the fecal contamination of food and watercaused by poor sanitation. At one time it was thought that cholera wascaused by exposure to toxic gases or miasmas resulting from thefermentation of composting feces in open cesspools, as was common inall large cities before the installation of septic systems.[medical citation
needed]
Susceptibility
About 100 million bacteria must typically be ingested to cause cholerain a normal healthy adult. This dose, however, is less in those withlowered gastric acidity (for instance those using proton pumpinhibitors). Children are also more susceptible, with two- tofour-year-olds having the highest rates of infection. Individuals' susceptibility to cholera is also affected by theirblood type, with those with type O blood being the most susceptible. Persons with lowered immunity, such aspersons with AIDS or children who are malnourished, are more likely to experience a severe case if they becomeinfected.[9] Any individual, even a healthy adult in middle age, can experience a severe case, and each person's caseshould be measured by the loss of fluids, preferably in consultation with a professional health care provider.[medical
citation needed]
The cystic fibrosis genetic mutation in humans has been said to maintain a selective advantage: heterozygous carriersof the mutation (who are thus not affected by cystic fibrosis) are more resistant to V. cholerae infections. In thismodel, the genetic deficiency in the cystic fibrosis transmembrane conductance regulator channel proteins interfereswith bacteria binding to the gastrointestinal epithelium, thus reducing the effects of an infection.
TransmissionCholera is typically transmitted by either contaminated food or water. In the developed world, seafood is the usualcause, while in the developing world it is more often water. Most cholera cases in developed countries are a result oftransmission by food. This occurs when people harvest oysters in waters infected with sewage, as Vibrio choleraeaccumulates in zooplankton and the oysters eat the zooplankton. Cholera has been found in two animal populations:shellfish and plankton.

Cholera 3
People infected with cholera often have diarrhea, and if this highly liquid stool, colloquially referred to as"rice-water", contaminates water used by others, disease transmission may occur. The source of the contamination istypically other cholera sufferers when their untreated diarrheal discharge is allowed to get into waterways,groundwater or drinking water supplies. Drinking any infected water and eating any foods washed in the water, aswell as shellfish living in the affected waterway, can cause a person to contract an infection. Cholera is rarely spreaddirectly from person to person. Both toxic and nontoxic strains exist. Nontoxic strains can acquire toxicity through atemperate bacteriophage. Coastal cholera outbreaks typically follow zooplankton blooms, thus making cholera azoonotic disease.[medical citation needed]
Mechanism
Drawing of Death bringing cholera, in Le PetitJournal (1912)
When consumed, most bacteria do not survive the acidic conditions ofthe human stomach.[10] The few surviving bacteria conserve theirenergy and stored nutrients during the passage through the stomach byshutting down much protein production. When the surviving bacteriaexit the stomach and reach the small intestine, they need to propelthemselves through the thick mucus that lines the small intestine to getto the intestinal walls where they can thrive. V. cholerae bacteria startup production of the hollow cylindrical protein flagellin to makeflagella, the cork-screw helical fibers they rotate to propel themselvesthrough the mucus of the small intestine.[medical citation needed]
Once the cholera bacteria reach the intestinal wall they no longer needthe flagella to move. The bacteria stop producing the protein flagellinto conserve energy and nutrients by changing the mix of proteinswhich they express in response to the changed chemical surroundings.On reaching the intestinal wall, V. cholerae start producing the toxicproteins that give the infected person a watery diarrhea. This carriesthe multiplying new generations of V. cholerae bacteria out into thedrinking water of the next host if proper sanitation measures are not inplace.[medical citation needed]
The cholera toxin (CTX or CT) is an oligomeric complex made up of six protein subunits: a single copy of the Asubunit (part A), and five copies of the B subunit (part B), connected by a disulfide bond. The five B subunits form afive-membered ring that binds to GM1 gangliosides on the surface of the intestinal epithelium cells. The A1 portionof the A subunit is an enzyme that ADP-ribosylates G proteins, while the A2 chain fits into the central pore of the Bsubunit ring. Upon binding, the complex is taken into the cell via receptor-mediated endocytosis. Once inside thecell, the disulfide bond is reduced, and the A1 subunit is freed to bind with a human partner protein calledADP-ribosylation factor 6 (Arf6). Binding exposes its active site, allowing it to permanently ribosylate the Gs alphasubunit of the heterotrimeric G protein. This results in constitutive cAMP production, which in turn leads tosecretion of H2O, Na+, K+, Cl−, and HCO3
− into the lumen of the small intestine and rapid dehydration. The geneencoding the cholera toxin was introduced into V. cholerae by horizontal gene transfer. Virulent strains of V.cholerae carry a variant of temperate bacteriophage called CTXf or CTXφ.
Microbiologists have studied the genetic mechanisms by which the V. cholerae bacteria turn off the production of some proteins and turn on the production of other proteins as they respond to the series of chemical environments they encounter, passing through the stomach, through the mucous layer of the small intestine, and on to the intestinal wall. Of particular interest have been the genetic mechanisms by which cholera bacteria turn on the protein production of the toxins that interact with host cell mechanisms to pump chloride ions into the small intestine,

Cholera 4
creating an ionic pressure which prevents sodium ions from entering the cell. The chloride and sodium ions create asalt-water environment in the small intestines, which through osmosis can pull up to six litres of water per daythrough the intestinal cells, creating the massive amounts of diarrhea. The host can become rapidly dehydrated if anappropriate mixture of dilute salt water and sugar is not taken to replace the blood's water and salts lost in thediarrhea.[medical citation needed]
By inserting separate, successive sections of V. cholerae DNA into the DNA of other bacteria, such as E. coli thatwould not naturally produce the protein toxins, researchers have investigated the mechanisms by which V. choleraeresponds to the changing chemical environments of the stomach, mucous layers, and intestinal wall. Researchershave discovered a complex cascade of regulatory proteins controls expression of V. cholerae virulence determinants.In responding to the chemical environment at the intestinal wall, the V. cholerae bacteria produce the TcpP/TcpHproteins, which, together with the ToxR/ToxS proteins, activate the expression of the ToxT regulatory protein. ToxTthen directly activates expression of virulence genes that produce the toxins, causing diarrhea in the infected personand allowing the bacteria to colonize the intestine. Current research aims at discovering "the signal that makes thecholera bacteria stop swimming and start to colonize (that is, adhere to the cells of) the small intestine."
Genetic structureAmplified fragment length polymorphism fingerprinting of the pandemic isolates of V. cholerae has revealedvariation in the genetic structure. Two clusters have been identified: Cluster I and Cluster II. For the most part,Cluster I consists of strains from the 1960s and 1970s, while Cluster II largely contains strains from the 1980s and1990s, based on the change in the clone structure. This grouping of strains is best seen in the strains from the Africancontinent.Wikipedia:Identifying reliable sources (medicine)
DiagnosisA rapid dipstick test is available to determine the presence of V. cholerae. In those samples that test positive, furthertesting should be done to determine antibiotic resistance. In epidemic situations, a clinical diagnosis may be made bytaking a patient history and doing a brief examination. Treatment is usually started without or before confirmation bylaboratory analysis.Stool and swab samples collected in the acute stage of the disease, before antibiotics have been administered, are themost useful specimens for laboratory diagnosis. If an epidemic of cholera is suspected, the most common causativeagent is V. cholerae O1. If V. cholerae serogroup O1 is not isolated, the laboratory should test for V. cholerae O139.However, if neither of these organisms is isolated, it is necessary to send stool specimens to a reference laboratory.Infection with V. cholerae O139 should be reported and handled in the same manner as that caused by V. choleraeO1. The associated diarrheal illness should be referred to as cholera and must be reported in the United States.

Cholera 5
Prevention
Cholera hospital in Dhaka, showing typical"cholera beds"
The World Health Organization recommends focusing on prevention,preparedness, and response to combat the spread of cholera.[11] Theyalso stress the importance of an effective surveillance system.Governments can play a role in all of these areas, and in preventingcholera or indirectly facilitating its spread.
Although cholera may be life-threatening, prevention of the disease isnormally straightforward if proper sanitation practices are followed. Indeveloped countries, due to nearly universal advanced water treatmentand sanitation practices, cholera is no longer a major health threat. Thelast major outbreak of cholera in the United States occurred in1910–1911. Effective sanitation practices, if instituted and adhered toin time, are usually sufficient to stop an epidemic. There are severalpoints along the cholera transmission path at which its spread may behalted:[medical citation needed]
• Sterilization: Proper disposal and treatment of infected fecal wastewater produced by cholera victims and all contaminated materials(e.g. clothing, bedding, etc.) are essential. All materials that come incontact with cholera patients should be sanitized by washing in hot water, using chlorine bleach if possible. Handsthat touch cholera patients or their clothing, bedding, etc., should be thoroughly cleaned and disinfected withchlorinated water or other effective antimicrobial agents.
• Sewage: antibacterial treatment of general sewage by chlorine, ozone, ultraviolet light or other effective treatmentbefore it enters the waterways or underground water supplies helps prevent undiagnosed patients frominadvertently spreading the disease.
• Sources: Warnings about possible cholera contamination should be posted around contaminated water sourceswith directions on how to decontaminate the water (boiling, chlorination etc.) for possible use.
• Water purification: All water used for drinking, washing, or cooking should be sterilized by either boiling,chlorination, ozone water treatment, ultraviolet light sterilization (e.g. by solar water disinfection), orantimicrobial filtration in any area where cholera may be present. Chlorination and boiling are often the leastexpensive and most effective means of halting transmission. Cloth filters or sari filtration, though very basic, havesignificantly reduced the occurrence of cholera when used in poor villages in Bangladesh that rely on untreatedsurface water. Better antimicrobial filters, like those present in advanced individual water treatment hiking kits,are most effective. Public health education and adherence to appropriate sanitation practices are of primaryimportance to help prevent and control transmission of cholera and other diseases.
SurveillanceSurveillance and prompt reporting allow for containing cholera epidemics rapidly. Cholera exists as a seasonaldisease in many endemic countries, occurring annually mostly during rainy seasons. Surveillance systems canprovide early alerts to outbreaks, therefore leading to coordinated response and assist in preparation of preparednessplans. Efficient surveillance systems can also improve the risk assessment for potential cholera outbreaks.Understanding the seasonality and location of outbreaks provides guidance for improving cholera control activitiesfor the most vulnerable. For prevention to be effective, it is important that cases be reported to national healthauthorities.

Cholera 6
Vaccine
Preventive inoculation against cholera in 1966
A number of safe and effective oral vaccines for cholera are available.Dukoral, an orally administered, inactivated whole cell vaccine, has anoverall efficacy of about 52% during the first year after being givenand 62% in the second year, with minimal side effects. It is available inover 60 countries. However, it is not currently recommended by theCenters for Disease Control and Prevention (CDC) for most peopletraveling from the United States to endemic countries. One injectablevaccine was found to be effective for two to three years. The protectiveefficacy was 28% lower in children less than 5 years old. However, asof 2010, it has limited availability. Work is under way to investigatethe role of mass vaccination. The World Health Organization (WHO)recommends immunization of high-risk groups, such as children andpeople with HIV, in countries where this disease is endemic. If people are immunized broadly, herd immunityresults, with a decrease in the amount of contamination in the environment.
Sari filtrationAn effective and relatively cheap method to prevent the transmission of cholera is the use of a folded sari (a longcloth garment) to filter drinking water. In Bangladesh this practice was found to decrease rates of cholera by nearlyhalf. It involves folding a sari four to eight times. Between uses the cloth should be rinsed in clean water and dried inthe sun to kill any bacteria on it. A nylon cloth appears to work as well.
Treatment
Cholera patient being treated by medical staff in1992
Continued eating speeds the recovery of normal intestinal function.The World Health Organization recommends this generally for cases ofdiarrhea no matter what the underlying cause. A CDC training manualspecifically for cholera states: “Continue to breastfeed your baby if thebaby has watery diarrhea, even when traveling to get treatment. Adultsand older children should continue to eat frequently.”[12]
Fluids
The most common error in caring for patients with cholera is tounderestimate the speed and volume of fluids required.[13] In mostcases, cholera can be successfully treated with oral rehydration therapy (ORT), which is highly effective, safe, andsimple to administer. Rice-based solutions are preferred to glucose-based ones due to greater efficiency. In severecases with significant dehydration, intravenous rehydration may be necessary. Ringer's lactate is the preferredsolution, often with added potassium.[] Large volumes and continued replacement until diarrhea has subsided may beneeded. Ten percent of a person's body weight in fluid may need to be given in the first two to four hours. Thismethod was first tried on a mass scale during the Bangladesh Liberation War, and was found to have muchsuccess.[14]
If commercially produced oral rehydration solutions are too expensive or difficult to obtain, solutions can be made.One such recipe calls for 1 liter of boiled water, 1/2 teaspoon of salt, 6 teaspoons of sugar, and added mashed bananafor potassium and to improve taste.

Cholera 7
ElectrolytesAs there frequently is initially acidosis, the potassium level may be normal, even though large losses have occurred.As the dehydration is corrected, potassium levels may decrease rapidly, and thus need to be replaced. This may bedone by eating foods high in potassium like bananas or green coconut water.
AntibioticsAntibiotic treatments for one to three days shorten the course of the disease and reduce the severity of the symptoms.Use of antibiotics also reduces fluid requirements. People will recover without them, however, if sufficient hydrationis maintained. The World Health Organization only recommends antibiotics in those with severe dehydration.Doxycycline is typically used first line, although some strains of V. cholerae have shown resistance. Testing forresistance during an outbreak can help determine appropriate future choices. Other antibiotics proven to be effectiveinclude cotrimoxazole, erythromycin, tetracycline, chloramphenicol, and furazolidone. Fluoroquinolones, such asnorfloxacin, also may be used, but resistance has been reported.In many areas of the world, antibiotic resistance is increasing. In Bangladesh, for example, most cases are resistant totetracycline, trimethoprim-sulfamethoxazole, and erythromycin. Rapid diagnostic assay methods are available for theidentification of multiple drug-resistant cases. New generation antimicrobials have been discovered which areeffective against in in vitro studies.
Zinc supplementationIn Bangladesh zinc supplementation reduced the duration and severity of diarrhea in children with cholera whengiven with antibiotics and rehydration therapy as needed. It reduced the length of disease by eight hours and theamount of diarrheal stool by 10%. Supplementation appears to be also effective in both treating and preventinginfectious diarrhea due to other causes among children in the developing world.
PrognosisIf people with cholera are treated quickly and properly, the mortality rate is less than 1%; however, with untreatedcholera, the mortality rate rises to 50–60%. For certain genetic strains of cholera, such as the one present during the2010 epidemic in Haiti and the 2004 outbreak in India, death can occur within two hours of becoming ill.
Epidemiology
Hand bill from the New York City Board ofHealth, 1832—the outdated public health advice
demonstrates the lack of understanding of thedisease and its actual causative factors.
Cholera affects an estimated 3–5 million people worldwide, and causes58,000–130,000 deaths a year as of 2010. This occurs mainly in thedeveloping world. In the early 1980s, death rates are believed to havebeen greater than 3 million a year. It is difficult to calculate exactnumbers of cases, as many go unreported due to concerns that anoutbreak may have a negative impact on the tourism of a country.Cholera remains both epidemic and endemic in many areas of theworld.
Although much is known about the mechanisms behind the spread ofcholera, this has not led to a full understanding of what makes choleraoutbreaks happen some places and not others. Lack of treatment ofhuman feces and lack of treatment of drinking water greatly facilitate
its spread, but bodies of water can serve as a reservoir, and seafood shipped long distances can spread the disease. Cholera was not known in the Americas for most of the 20th century, but it reappeared towards the end of that

Cholera 8
century.
HistoryThe word cholera is from Greek: χολέρα kholera from χολή kholē "bile". Cholera likely has its origins in the IndianSubcontinent; it has been prevalent in the Ganges delta since ancient times. Choleras first origins, within the IndianSubcontinent, are believed to have occurred due to the result of poor living conditions as well as the presence ofpools of still water; both of which are ideal living conditions for cholera to thrive. The disease first spread by traderoutes (land and sea) to Russia in 1817, then, through technological advancements, to the rest of Europe, and fromEurope to North America and the rest of the world. Seven cholera pandemics have occurred in the past 200 years,with the seventh originating in Indonesia in 1961.[15]
Map of the 2008–2009 cholera outbreak insub-Saharan Africa showing the statistics as of 12
February 2009.
The first cholera pandemic occurred in the Bengal region of Indiastarting in 1817 through 1824. The disease dispersed from India toSoutheast Asia, China, Japan, the Middle East, and southern Russia.The second pandemic lasted from 1827 to 1835 and affected the UnitedStates and Europe particularly due to the result of advancements intransportation, such as trade, and increased human migration, includingsoldiers. The third pandemic erupted in 1839, persisted until 1856,extended to North Africa, and reached South America, for the first timespecifically infringing upon Brazil. Cholera hit the sub-SaharanAfrican region during the fourth pandemic from 1863 to 1875. Thefifth and sixth pandemics raged from 1881–1896 and 1899-1923.These epidemics were less fatal due to a greater understanding of thecholera bacteria. Egypt, the Arabian peninsula, Persia, India, and thePhilippines were hit hardest during these epidemics, while other areas,like Germany in 1892 and Naples from 1910–1911, experienced severeoutbreaks. The final pandemic originated in 1961 in Indonesia and ismarked by the emergence of a new strain, nicknamed El Tor, which still persists today in developing countries.[16]
From a local disease, cholera became one of the most widespread and deadly diseases of the 19th century, killing anestimated tens of millions of people.[17] In Russia alone, between 1847 and 1851, more than one million peopleperished of the disease.[18] It killed 150,000 Americans during the second pandemic. Between 1900 and 1920,perhaps eight million people died of cholera in India.[19] Cholera became the first reportable disease in the UnitedStates due to the significant effects it had on health. John Snow, in England, was the first to identify the importanceof contaminated water in its cause in 1854. Cholera is now no longer considered a pressing health threat in Europeand North America due to filtering and chlorination of water supplies, but still heavily affects populations indeveloping countries.
In the past, vessels flew a yellow quarantine flag if any crew members or passengers were suffering from cholera. Noone aboard a vessel flying a yellow flag would be allowed ashore for an extended period, typically 30 to 40 days. Inmodern sets of international maritime signal flags, the quarantine flag is yellow and black.

Cholera 9
Signal flag "Lima" called the "Yellow Jack"which when flown in harbor means ship is underquarantine. A simple yellow flag (also called the
"Yellow Jack") had historically been used tosignal quarantine (it stands for Q among signal
flags), but now indicates the opposite, as a signalof a ship free of disease that requests boarding
and inspection.
Historically many different claimed remedies have existed in folklore.In the 1854–1855 outbreak in Naples homeopathic Camphor was usedaccording to Hahnemann.[20] While T. J. Ritter's "Mother's Remedies"book lists tomato syrup as a home remedy from northern America.While elecampagne was recommended in the United Kingdomaccording to William Thomas Fernie
Cholera cases are much less frequent in developed countries wheregovernments have helped to establish water sanitation practices andeffective medical treatments.[21] The United States, for example, usedto have a severe cholera problem similar to those in some developingcountries. There were three large cholera outbreaks in the 1800s, whichcan be attributed to Vibrio cholerae's spread through interiorwaterways like the Erie Canal and routes along the Eastern Seaboard.The island of Manhattan in New York City touched the AtlanticOcean, where cholera collected just off the coast. At this time, NewYork City did not have as effective a sanitation system as it does today,so cholera was able to spread.[22]
Research
The bacterium was isolated in 1855 by Italian anatomist Filippo Pacini, but its exact nature and his results were notwidely known.
Spanish physician Jaume Ferran i Clua developed a cholera vaccine in 1885, the first to immunize humans against abacterial disease.[23]
Ukrainian bacteriologist Waldemar Haffkine developed a cholera vaccine in July 1892.[24]
One of the major contributions to fighting cholera was made by the physician and pioneer medical scientist JohnSnow (1813–1858), who in 1854 found a link between cholera and contaminated drinking water. Dr. Snow proposeda microbial origin for epidemic cholera in 1849. In his major "state of the art" review of 1855, he proposed asubstantially complete and correct model for the etiology of the disease. In two pioneering epidemiological fieldstudies, he was able to demonstrate human sewage contamination was the most probable disease vector in two majorepidemics in London in 1854.[25] His model was not immediately accepted, but it was seen to be the more plausible,as medical microbiology developed over the next 30 years or so.
Robert Koch (third from the right) on a choleraresearch expedition in Egypt in 1884, one year
after he identified V. cholerae.
Cities in developed nations made massive investment in clean watersupply and well-separated sewage treatment infrastructures betweenthe mid-1850s and the 1900s. This eliminated the threat of choleraepidemics from the major developed cities in the world. In 1883,Robert Koch identified V. cholerae with a microscope as the bacilluscausing the disease.[26]
Robert Allan Phillips, working at the US Naval Medical Research UnitTwo in Southeast Asia, evaluated the pathophysiology of the diseaseusing modern laboratory chemistry techniques and developed aprotocol for rehydration. His research led the Lasker Foundation toaward him its prize in 1967.[citation needed]

Cholera 10
Cholera has been a laboratory for the study of evolution of virulence. The province of Bengal in British India waspartitioned into West Bengal and East Pakistan in 1947. Prior to partition, both regions had cholera pathogens withsimilar characteristics. After 1947, India made more progress on public health than East Pakistan (now Bangladesh).As a consequence,Wikipedia:Please clarify the strains of the pathogen that succeeded in India had a greater incentivein the longevity of the host. They have become less virulent than the strains prevailing in Bangladesh. These drawupon the resources of the host population and rapidly kill many victims.More recently, in 2002, Alam, et al., studied stool samples from patients at the International Centre for DiarrhoealDisease in Dhaka, Bangladesh. From the various experiments they conducted, the researchers found a correlationbetween the passage of V. cholerae through the human digestive system and an increased infectivity state.Furthermore, the researchers found the bacterium creates a hyperinfected state where genes that control biosynthesisof amino acids, iron uptake systems, and formation of periplasmic nitrate reductase complexes were induced justbefore defecation. These induced characteristics allow the cholera vibrios to survive in the "rice water" stools, anenvironment of limited oxygen and iron, of patients with a cholera infection.
Society and cultureIn many developing countries, cholera still reaches its victims through contaminated water sources, and countrieswithout proper sanitation techniques have greater incidence of the disease.[27] Governments can play a role in this. In2008, for example, the Zimbabwean cholera outbreak was due partly to the government's role, according to a reportfrom the James Baker Institute. The Haitian government’s inability to provide safe drinking water after the 2010earthquake led to an increase in cholera cases as well.[28] Similarly, South Africa’s cholera outbreak was exacerbatedby the government’s policy of privatizing water programs. The wealthy elite of the country were able to afford safewater while others had to use water from cholera-infected rivers.Wikipedia:Verifiability[29]
According to Rita R. Colwell of the James Baker Institute, if cholera does begin to spread, government preparednessis crucial. A government's ability to contain the disease before it extends to other areas can prevent a high death tolland the development of an epidemic or even pandemic. Effective disease surveillance can ensure that choleraoutbreaks are recognized as soon as possible and dealt with appropriately. Oftentimes, this will allow public healthprograms to determine and control the cause of the cases, whether it is unsanitary water or seafood that haveaccumulated a lot of Vibrio cholerae specimens. Having an effective surveillance program contributes to agovernment’s ability to prevent cholera from spreading. In the year 2000 in the state of Kerala in India, the Kottayamdistrict was determined to be "cholera-affected"; this pronouncement led to task forces that concentrated oneducating citizens with 13,670 information sessions about human health.[30] These task forces promoted the boilingof water to obtain safe water, and provided chlorine and oral rehydration salts. Ultimately, this helped to control thespread of the disease to other areas and minimize deaths. On the other hand, researchers have shown that most of thecitizens infected during the 1991 cholera outbreak in Bangladesh lived in rural areas, and were not recognized by thegovernment's surveillance program. This inhibited physicians' abilities to detect cholera cases early.[31]
According to Colwell, the quality and inclusiveness of a country's health care system affects the control of cholera,as it did in the Zimbabwean cholera outbreak. While sanitation practices are important, when governments respondquickly and have readily available vaccines, the country will have a lower cholera death toll. Affordability ofvaccines can be a problem; if the governments do not provide vaccinations, only the wealthy may be able to affordthem and there will be a greater toll on the country's poor.[32] The speed with which government leaders respond tocholera outbreaks is important.Besides contributing to an effective or declining public health care system and water sanitation treatments,government can have indirect effects on cholera control and the effectiveness of a response to cholera. A country'sgovernment can impact its ability to prevent disease and control its spread. A speedy government response backedby a fully functioning health care system and financial resources can prevent cholera's spread. This limits cholera'sability to cause death, or at the very least a decline in education, as children are kept out of school to minimize the

Cholera 11
risk of infection.
Notable cases• Tchaikovsky's death has traditionally been attributed to cholera, most probably contracted through drinking
contaminated water several days earlier.[33] "Since the water was not boiled and cholera was affecting SaintPetersburg, such a connection is quite plausible ...."[34] Tchaikovsky's mother died of cholera,[35] and his fatherbecame sick with cholera at this time but made a full recovery.[36] Some scholars, however, including Englishmusicologist and Tchaikovsky authority David Brown and biographer Anthony Holden, have theorized that hisdeath was a suicide.[37]
• After the 2010 earthquake, an outbreak swept over Haiti, traced to a United Nations base. This marks the worstcholera outbreak in recent history, as well as the best documented cholera outbreak in modern public health.
Other famous people believed to have died of cholera include:• Sadi Carnot, Physicist, a founder of thermodynamics (d. 1832)[38]
• Charles X, King of France (d. 1836)[39]
• James K. Polk, eleventh president of the United States (d. 1849)• Carl von Clausewitz, Prussian soldier and German military theorist (d. 1831)[40]
References[1] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ A00[2] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=001[3] http:/ / www. diseasesdatabase. com/ ddb29089. htm[4] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000303. htm[5] http:/ / www. emedicine. com/ med/ topic351. htm[6] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2013/ MB_cgi?field=uid& term=D002771[7] http:/ / en. wikipedia. org/ w/ index. php?title=Cholera& action=edit[8][8] McElroy, Ann and Patricia K. Townsend. Medical Anthropology in Ecological Perspective. Boulder, CO: Westview, 2009, 375.[9] Prevention and control of cholera outbreaks: WHO policy and recommendations (http:/ / www. emro. who. int/ csr/ Media/ PDF/
cholera_whopolicy. pdf), World Health Organization, Regional Office for the Eastern Mediterranean, undated but citing sources from ’07, ’04,’03, ’04, and ’05.
[10] (using the turning off and turning on of gene expression to make toxin proteins in cholera bacteria as a "comprehensive example" of what isknown about the mechanisms by which bacteria change the mix of proteins they express to respond to the changing opportunities for survivingand thriving in different chemical environments).
[11] "Cholera Fact Sheet", World Health Organization. who.int (http:/ / www. who. int/ mediacentre/ factsheets/ fs107/ en/ index. html).Retrieved November 5, 2013.
[12] Community Health Worker Training Materials for Cholera Prevention and Control (http:/ / www. cdc. gov/ haiticholera/ pdf/chw_trainingmaterialsforcholera. pdf), CDC, slides at back are dated 11/17/2010. See esp pages 7-8.
[13] globalhealthcenter.umn.edu (http:/ / globalhealthcenter. umn. edu/ documents/ Cholera-Lancet-July2012. pdf)[14] The Civil War That Killed Cholera (http:/ / www. foreignpolicy. com/ articles/ 2011/ 03/ 21/ the_civil_war_that_killed_cholera),
foreignpolicy.com.[15] " Cholera's seven pandemics (http:/ / www. cbc. ca/ health/ story/ 2008/ 05/ 09/ f-cholera-outbreaks. html)". CBC News. October 22, 2010.[16] Aberth, John. Plagues in world History. Lanham, MD: Rowman & Littlefield, 2011, 102.[17] .Kelley Lee (2003) "Health impacts of globalization: towards global governance". Palgrave Macmillan. p.131. ISBN 0-333-80254-3[18] Geoffrey A. Hosking (2001). " Russia and the Russians: a history (http:/ / books. google. com/ books?id=oh-5AAmboMUC& pg=PA9&
dq& hl=en#v=onepage& q=& f=false)". Harvard University Press. p.9. ISBN 0-674-00473-6[19] J. N. Hays (2005). " Epidemics and pandemics: their impacts on human history (http:/ / books. google. com/ books?id=GyE8Qt-kS1kC&
pg=PA347& dq& hl=en#v=onepage& q=& f=false)". p.347. ISBN 1-85109-658-2[20] www.legatum.sk (http:/ / www. legatum. sk/ en:ahr:bayes-cholera-as-treated-by-dr-rubini-158-10355), The American Homoeopathic
Review Vol. 06 No. 11-12, 1866, pages 401-403[21] "Cholera", World Health Organization. who.int (http:/ / www. who. int/ topics/ cholera/ about/ en/ index. html)[22][22] Lacey, S.W. Clin. Infect. Dis 20, 409. 1995. Retrieved September 18, 2013.[23] onlinelibrary.wiley.com (http:/ / www. historyofvaccines. org/ content/ timelines/ others#EVT_101034)[24] haffkineinstitute.org (http:/ / www. haffkineinstitute. org/ waldemar. htm)[25] Dr John Snow, The mode of communication of cholera, London 1855

Cholera 12
[26] Aberth,John. Plagues in World History. Lanham, MD: Rowman & Littlefield, 2011, 101.[27][27] "Cholera vaccines. A brief summary of the March 2010 position paper" (PDF). World Health Organization. Retrieved September 19, 2013.[28][28] Walton, David. "Responding to Cholera in Post-Earthquake Haiti." The New England Journal of Medicine 364. 2011. Retrieved October 19,
2013.[29] Pauw, J. "The Politics of Underdevelopment: metered to death- how a water experiment caused riots and a cholera epidemic."
baywood.metapress.com (http:/ / baywood. metapress. com/ app/ home/ contribution. asp?referrer=parent&backto=issue,9,11;journal,40,171;linkingpublicationresults,1:300313,1), International Journal of Health Services 33. 2003. RetrievedSeptember 24, 2013.
[30][30] John, T. Jacob, K. Rajappan, and K. K. Arjunan. "Communicable diseases monitored by disease surveillance in Kottayam district, Keralastate, India." Indian Journal of Medical Research 120 (2004): 86-93.
[31] Siddique, AK. "Cholera Epidemics in Bangladesh: 1985-1991." Journal of Diarrhoeal Diseases Research Volume 10, Number 2 (1992): 79.books.google.com (http:/ / books. google. com/ books?hl=en& lr=& id=qE5qb2v8_DEC& oi=fnd& pg=PA79& dq=cholera+ government&ots=v8PY4Uron_& sig=02ZLs7qKUcbFdwgLdwrrSeHgqmY#v=onepage& q=cholera government& f=false). Retrieved November 5, 2013.
[32] DeRoeck, Denise. "Policymakers’ views regarding the introduction of new-generation vaccines against typhoid fever, shigellosis and cholerain Asia." sciencedirect.com (http:/ / www. sciencedirect. com/ science/ article/ pii/ S0264410X04008886), Vaccine, volume 23, issue 21.2005. Retrieved September 21, 2013.
[33] Brown, Man and Music, 430–32; Holden, 371; Warrack, Tchaikovsky, 269–270.[34] (summarizing various theories on what killed the composer Tchaikovsky, including his brother Modest's idea that Tchaikovsky drank
cholera-infested water the day before he became ill).[35] David Brown, Early Years, 46.[36][36] Holden, 23.[37] Brown, Man and Music, 431–35; Holden, 373–400.[38][38] Asimov, Isaac (1982), Asimov's Biographical Encyclopedia of Science and Technology (2nd rev. ed.), Doubleday[39] Susan Nagel, Marie Thérèse: Child of Terror, p. 349-350.[40] Smith, Rupert, The Utility of Force, Penguin Books, 2006, page 57
Further reading• Colwell RR (December 1996). "Global climate and infectious disease: the cholera paradigm" (http:/ / www.
sciencemag. org/ cgi/ pmidlookup?view=long& pmid=8953025). Science 274 (5295): 2025–31. doi:10.1126/science.274.5295.2025 (http:/ / dx. doi. org/ 10. 1126/ science. 274. 5295. 2025). PMID 8953025 (http:// www. ncbi. nlm. nih. gov/ pubmed/ 8953025).
• Drasar, B. S.; Forrest, Bruce D., eds. (1996). Cholera and the ecology of Vibrio cholerae (http:/ / books. google.com/ ?id=NNQtXqqnVSIC& printsec=frontcover). Springer. p. 355. ISBN 0-412-61220-8
• Echenberg, Myron (2011) Africa in the Time of Cholera. A History of Pandemics from 1817 to the Present,Cambridge University Press, New York (Paperback) ISBN 978-0-521-18820-3
• Furuque, Shah M.; Nair, G. Balakrish, eds. (2008). Vibrio Cholerae: Genomics and Molecular Biology (http:/ /books. google. com/ ?id=fP67F_eOSgQC& printsec=frontcover). Horizon Scientific Press. p. 218.ISBN 1-904455-33-6
• Gilbert, Pamela K. (2008). Cholera and Nation: Doctoring the Social Body in Victorian England (http:/ / books.google. com/ ?id=nzr71cHdiNkC& printsec=frontcover). SUNY Press. p. 231. ISBN 0-7914-7343-0
• Henze, Charlotte E. (2011) Disease, Health Care and Government in Late Imperial Russia: Life and Death on theVolga, 1823-1914. Routledge, Oxon, UK 2011. ISBN 9780415547949.
• Jermyn, William S.; O'Shea, Yvonne A.; Quirke, Anne Marie; Boyd, E. Fidelma (2006). "Genomics and theEvolution of Pathogenic Vibrio Cholerae" (http:/ / books. google. com/ ?id=SX862lszVM4C&printsec=frontcover). In Chan, Voon L.; Sherman, Philip M.; Bourke, Billy. Bacterial genomes and infectiousdiseases. Humana Press. p. 270. ISBN 1-58829-496-X
• Johnson, Steven (2006). The Ghost Map: The Story of London's Most Terrifying Epidemic--and How It ChangedScience, Cities, and the Modern World. Riverhead Hardcover. ISBN 1-59448-925-4.
• McGrew, Roderick (1985) Encyclopedia of Medical History, brief history pp. 59–64.• Mintz ED, Guerrant RL (March 2009). "A lion in our village--the unconscionable tragedy of cholera in Africa"
(http:/ / content. nejm. org/ cgi/ pmidlookup?view=short& pmid=19279337& promo=ONFLNS19). N. Engl. J. Med. 360 (11): 1060–3. doi: 10.1056/NEJMp0810559 (http:/ / dx. doi. org/ 10. 1056/ NEJMp0810559). PMID

Cholera 13
19279337 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 19279337).• Pardio Sedas, Violeta T. (2008). "Impact of Climate and Environmental Factors on the Epidemiology of Vibrio
choerae in Aquatic Ecosystems" (http:/ / books. google. com/ ?id=LYYXNnA1swcC& printsec=frontcover). InHofer, Tobias N. Marine Pollution: New Research. Nova Science publishers. p. 448. pp. 221–254.ISBN 1-60456-242-0
• Ryan, Kenneth J.; Ray, C. George, eds. (2003). Sherris medical microbiology: an introduction to infectiousdiseases (http:/ / books. google. com/ ?id=mcjQ96KsQ_EC& printsec=frontcover) (4th ed.). McGraw-HillProfessional. p. 979. ISBN 0-8385-8529-9
• Wachsmuth, Kaye; Blake, Paul A.; Olsvik, Ørjan, eds. (1994). Vibrio cholerae and cholera: molecular to globalperspectives (http:/ / books. google. com/ ?id=xBhwzHQkdkYC& printsec=frontcover). ASM Press. p. 465.ISBN 1-55581-067-5
External links• Cholera (http:/ / www. who. int/ cholera)—World Health Organization• The Attenuation of the Causal Agent of Fowl Cholera (http:/ / www. pasteurbrewing. com/ Articles/
works-of-louis-pasteur-english/ the-attenuation-of-the-causal-agent-of-fowl-cholera. html), by Louis Pasteur,1880
• What is Cholera? (http:/ / www. cdc. gov/ cholera/ index. html)—Centers for Disease Control and Prevention• Cholera Epidemic in NYC in 1832 (http:/ / www. nytimes. com/ 2008/ 04/ 15/ science/ 15chol. html?) New York
Times 15 April 2008• The Cholera Timebomb in The DRC (http:/ / www. thefirstpost. co. uk/
45971,news-comment,news-politics,in-pictures-the-cholera-time-bomb)—slideshow by The First Post

Article Sources and Contributors 14
Article Sources and ContributorsCholera Source: http://en.wikipedia.org/w/index.php?oldid=586327572 Contributors: -Midorihana-, 069952497a, 0x6D667061, 0zymandias, 1exec1, 28421u2232nfenfcenc, 2help, A2coelho,ABF, AKMask, ALS manager, Aapsan, Academic Challenger, Acroterion, Aegir101, Afkatk, Ahoerstemeier, Airborne84, Aitias, Ajaxfiore, Ajray, Akcarver, Alan Liefting, Alansohn, AldezD,Aleenf1, Alex.muller, Alex.tan, Allstarecho, Amc4536, Andres, Andrew Dalby, Andrew Ross-Parker, AndrewHowse, AndrewJD, Andrewrp, Angelfirenze, Angr, Anquillaf, Antandrus,Antiqueight, Antonio Lopez, Aqadir149, Aranea Mortem, Arcadian, Arctic Fox, Arfgab, Arman Cagle, Armeria, Ashmoo, Attys, Aumnamahashiva, Avionics1980, Avnjay, Avoided, Avriette,AxelBoldt, Azuris, Bachrach44, Baron.atreid, Beatdown, Beeblebrox, Beetstra, Beland, Ben Fredlund, Bender235, Beyond My Ken, Bgwhite, BiT, Bigbull133, Bill william compton, BillC,Billhpike, Billlion, BillyTFried, Binary TSO, Blahedo, Blanchardb, Blechnic, Bluebulb, Bluezy, Bmcln1, Bob247, Bomac, Bongwarrior, Bowmerang, BozMo, Brianga, Brim, Bruce1ee, Brycen,Bstephens393, Burner0718, Bwood, CDN99, Cactus.man, Cacycle, Callanecc, Calmer Waters, Caltas, Can't sleep, clown will eat me, CanadianLinuxUser, CanbekEsen, Canterbury Tail,Capricorn42, Caracaskid, Carlw4514, Caster23, CatherineMunro, CattleGirl, Ccady, Cdcdoc, CeilingCrash, Celestianpower, Ceranthor, Charlene.fic, Chinasaur, Chris Capoccia, Chris the speller,ChrisHamburg, Chriswaterguy, Chun-hian, Chzz, Ck4829, Closedmouth, Clueponic, ComfyKem, Common Man, CommonsDelinker, Computer18.9, Confession0791, Conversion script, CoolNerd, Corinne68, Cp7801k, Cpl Syx, Crazyboy14285714, Culturenut, Cycormier, D'lin, D. Recorder, DARTH SIDIOUS 2, DD2K, DJ Clayworth, DJP, DO11.10, DTRY, DVD R W, Dabomb87,Dan Aquinas, Dana boomer, DandyDan2007, DanielCD, Danny, Dardura108, Darkthingstab1, Darkwind, Darkzinc1998, David Newton, Davidruben, Dbachmann, Deconcoder, Den fjättradeankan, Dennisp234, DennyColt, Dgw, Dhollm, Dianaliu, Diannaa, Discospinster, Distantsuns, Dkabban-GMU, DocWatson42, Dogcow, Dogru144, Dominicanpapi82, Donmillsbridge,Dontmentionit, Doomfus, DopefishJustin, Doris west, Doseiai2, Dougher, Dougluce, Dpotter, Dr.salt, Drawn Some, Dreadstar, Driftwood87, Drphilharmonic, Drredgreen, Dthomsen8,Dungodung, Dusti, Dwm39tall, E.ThomasWood, ESkog, Ebikeofacookbook, Edgar181, Edward Vielmetti, Edward321, Eenu, Efrem7, Egmontaz, Eisnel, Elassint, Elchupachipmunk, Eleiser,EliasAlucard, EmanWilm, EmoMan13, Enlil Ninlil, Enviroboy, Eog1916, Epbr123, Eric567, Ericamick, Erick808, ErikHaugen, Everyking, Ewen, Exadrid, Excirial, Extransit, Facts707,Falcon8765, Favonian, Felidofractals, Feline1, Ferrierd, Fetchcomms, Ffirehorse, Filibustered, Finavon, Flameigloo, Fleela, Flower-gmu, Flyer22, Fowler&fowler, FrancoGG, Frankie1969,Fredil Yupigo, FreplySpang, Frymaster, Fshaikh GMU, Fungible, Funnyfarmofdoom, Fæ, GT5162, GaHeRiS, Gabbe, Gahg, Gaius Cornelius, Gak, Gandydancer, Gareth Griffith-Jones,Gberning, Gegnome, GeneralAtrocity, Giftlite, Gigemag76, Gilliam, Gillis, Glane23, Go229, Gogo Dodo, GoingBatty, Graham87, Graminophile, Gregsinclair, Guddu namaste, Gurch,Gzornenplatz, HMSSolent, HOT L Baltimore, Hadal, Halogenated, Hammer1980, Hamtechperson, Haroulitos, Hayleesmith777, Hellosparta, Herika007, Historymike, Hollis-B, Hotcrocodile,Htfiddler, Human.v2.0, Hunterhogan, Husond, Hutchy508, Hydrargyrum, I dream of horses, I'm lucas, II MusLiM HyBRiD II, IJA, Iamanorange, Iamollie, Imagine-GMU, Inhakito, Inka 888,Inwind, Isidore, Ivan Bajlo, J.delanoy, J36miles, J991, JHunterJ, JIP, JJHmngr, JMO161, JSpung, JV Smithy, Ja 62, Jabaker75, Jack Greenmaven, Jacopo Werther, Jamie C, Jantzen212003,Jaranda, Jared Preston, Jaydec, Jdcopp, Jedi Master MIK, Jeff G., Jethro B, Jh51681, Jhbuk, Jim1138, Jimjamjak, JinJian, Jjron, Jlh04002, Jmh649, Jni, JoanneB, Joaquin008, Jobaboba,Joel.labes, Joelmills, John Snow II, John Vandenberg, JohnCD, Johnbod, Jojhutton, Jomasecu, Jonathanriley, Jonkerz, Jovianeye, Jpear11, Jredmond, Jreferee, Jsjsjs1111, Julesd, Julle, Jumpingcheese, Jusdafax, KBi, KConWiki, KDS4444, KGasso, KNewman, Kafziel, Katalaveno, Kathypham, Katwmn6, Kbh3rd, Keegan, Keegsmeister, Kelovy, KenWalker, Kernow, Kerowyn, KevinMyers, Kewp, Khalid Mahmood, Khazar2, Killerlula, Kilva, Kimmyfromtexas, King of Hearts, Kingchongoo, Kingdon, Kingpin13, Kingturtle, Kirachinmoku, Kjnoel, KnowledgeOfSelf,Kntrabssi, Koavf, Kolbasz, Kpjas, Kristof vt, Kslotte, Kubanczyk, Kukini, L Kensington, LWG, Lacrimosus, Lagalag, Latcarf, Latka, Laurap414, Law, Lawrence1995, Lbeaumont, Lcamtuf,Lcarscad, LeadSongDog, Lectonar, LessHeard vanU, Letdemsay, Lexicon, Lights, Lihaas, LilHelpa, Lionslayer, Literalman, LittleT889, Lizia7, Logan, Lol832, Louprado, Lradrama,Lsaintgermain, LuisVilla, Luisfernandolozano, M-le-mot-dit, MECU, MONGO, MadGeographer, MadGuy7023, MaddiyK, Magarmach, Magioladitis, Magnus Manske, Makemi, Man1111,Mandarax, Mani1, Maniadis, MantisEars, Manuel Trujillo Berges, MarcoTolo, Marek69, Margaret52, Mark Arsten, Mark1000, MarkinBoston, MarsRover, Martarius, Masonfiftyfive, Matchups,Materialscientist, Matijap, Mattbr, MatthewDBA, Maurog, Maxis ftw, Maxlee, Mayooranathan, McCart42, McDogm, Mcwescott, Mdann52, Mdjohnson, Mdukas, Meekywiki, Megaman en m,Melissababex, Merope, Methecooldude, MichaelBillington, Midgrid, Mike Christie, Mike g5065, Mike2vil, MikeFTM, Mikeylane, Mintleaf, Miquonranger03, Missionary, MisterHand,Mjpieters, Mnyakaba-GMU, Mokgen, MonaScabra, Mononomic, Mr. Celery, MrFish, MrMoustacheMM, Mshecket, Msikma, MusikAnimal, Mxn, Mygerardromance, Myles Callum, Nabokov,Naj-GMU, Naja Haje, Nanzilla, Napalm Llama, NawlinWiki, Nburden, Neckro, Neurolysis, Neurophyre, NickGorton, Nihiltres, Nirvana888, Nitesshadow, Nk, Nneonneo, No Guru, No More MrNice Guy, Noah Salzman, Nocturnal Wanderer, Noodleki, NotWith, Nova77, Novidmarana, Nuno Tavares, Obarskyr, Ocaasi, OcciMoron, Oda Mari, Ohnoitsjamie, Omnipaedista, Onco p53,OneHappyHusky, Oneiros, Oneworld777, Optimist on the run, Osisiogu, OverlordQ, Oxymoron83, Ozan Ayyüce, PFHLai, PIL1987, Pacotaco43, Palmcluster, Parap110, Parkwells, Paul Erik,Paul W, Paul-L, Pawyilee, Pax:Vobiscum, Penrithguy, PersianPride91, Petiatil, Petri Krohn, Pfalstad, Pfistermeister, Pgk, Phaedriel, Pharaoh of the Wizards, Phil Bridger, Philip Trueman,Phyzome, Pi, Piano non troppo, Piledhigheranddeeper, Pinethicket, Pixie2000, Plugwash, Pluma, Pmsyyz, Poetaris, Polihale, Pooky07, Pozcircuitboy, Prashanthns, Prestonmcconkie, Prim Ethics,Promotinghealth, Pschemp, Pstudier, Publicus, Pvanheus, Qoou.Anonimu, Quackslikeaduck, Quale, Quebec99, Quotidinanity, Qxz, R'n'B, RFerreira, RG2, RJBL0, Radon210, RainbowOfLight,Ramsis II, RandomAct, Randommusings, Raph, RastNim, Raviaka Ruslan, Rbreen, Rdsmith4, Ready, Rearete, Reconsider the static, Red1001802, Rednblu, Redthoreau, Remember,Retzs1atcentral.edu, RexNL, Rezecib, Riana, Rich Farmbrough, Richard Arthur Norton (1958- ), RjCan, Rjensen, Rjwilmsi, Rklawton, Rl, Rob-bob7-0, Robert K S, Robert McClenon, RobertG,Rocketrod1960, Rojomoke, Ronhjones, RoyBoy, Rrburke, Ruby Murray, Russthomas15, Ryan4314, Rzafar, SDC, SMC, SMP, Sabedon, Saberclaw, Sacxpert, Safewater, Sagaciousuk,Salvadorjo, Salvio giuliano, Sam Vimes, Sam.cullen10, Sameerkale, Samster1762, Sandover, SandyGeorgia, Sango123, Sangriademuertos, Santa Sangre, Sapphic, Scetoaux, Schellack,SchfiftyThree, Scott 97, Scottyaz, Sdennis-martineau, Sean Whitton, SeanMack, Seduisant, Senor Cuete, Sergay, Serpent's Choice, Sfahey, Shanes, Shiltz, Sifaka, Skeggy ben, Skizzik,SkyMachine, Slammer111, Slodj, Sm8900, Snoyes, SoCalSuperEagle, Soap, Solace098, Some jerk on the Internet, SpaceFlight89, Spacenookie, Spandlingford, Sparky the Seventh Chaos,Spidey104, Spikeyali, Spliffy, Splodgeness, Spongefrog, Spudgun, SpuriousQ, Srikeit, Stephenb, SteveMacIntyre, Steven Luo, Stevenfruitsmaak, Storkk, Straker, Stupid girl, SuW, Suede, SunCreator, Surv1v4l1st, Susfele, Svick, Swedish fusilier, Sweeperchick8705, Swithrow2546, Syndicate, TBadger, TNTfan101, TaintedMustard, Tarnjp, TastyCakes, Tatterfly, Tazmaniacs,Tearlach, Teledildonix314, TenOfAllTrades, ThatPeskyCommoner, Thatguyflint, The Almighty dF, The Everchosen, The Land, The Ogre, The Random Editor, The Thing That Should Not Be,The editor1, TheCatalyst31, TheRanger, TheRingess, TheThreeMuskaspackers, Themfromspace, Themusicking, Thenoob123, Theplacebo, Theshazaambritania, Thine Antique Pen, Think outsidethe box, Thirdeyeopen33, Thorwald, Tiddly Tom, Tide rolls, TigerPaw2154, TigerShark, Tim!, TimVickers, Timemutt, Timvasquez, Titoxd, ToastyMallows, Tobby72, Toccata quarta, Toddst1,Tolly4bolly, Tom harrison, Tomdo08, Tomyumgoong, TorstenMandal, Touchstone42, Tpbradbury, Tremello, Tresiden, Triona, Tristanb, Troy 07, True Pagan Warrior, Twas Now, Tyler trampel,Uannis, Ufwuct, Una Smith, Uncle Dick, Updatehelper, Useight, Utcursch, V65Magna1, Vacation9, Vaccines546, Vary, Velho, VernoWhitney, Vineetcoolguy, Viriditas, WACourson,WadeSimMiser, Wavelength, Wayne Slam, Whisky drinker, Whkoh, Who wants to know, Who.was.phone, Whoop whoop pull up, Widr, WikHead, Wiki alf, Wikidye, Wikih101, Wikipelli,Wildhartlivie, Wilt, Wimt, Winkydink, Witoldzio, WizardOfKozz, Wolfkeeper, Wolfmankurd, Woohookitty, Wouterstomp, WriterHound, Wtmitchell, Wykypydya, XSSUUMMZZx, XUniverse,Xaphnir, Xb2u7Zjzc32, Xxxxxxxxxxxxl, Yamamoto Ichiro, Yekrats, Yintan, Ykraps, Youknowit123, Yurik, Zahnradzacken, Zashitnik, Zeeyanwiki, Zeimusu, Zenzoken, Zidonuke, Zusasa,Валерий Пасько, 552140 ,ساجد امجد ساجد ,דוד anonymous edits
Image Sources, Licenses and ContributorsFile:Cholera bacteria SEM.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Cholera_bacteria_SEM.jpg License: Copyrighted free use Contributors: Bff, Copydays, DO11.10,Dietzel65, Martin H., NEON ja, Oks, Romary, Shizhao, Thiotrix, Zeimusu, 2 anonymous editsImage:Cholera feces.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Cholera_feces.jpg License: Creative Commons Attribution-Sharealike 3.0,2.5,2.0,1.0 Contributors: F1jmmImage:Vibrio cholerae.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Vibrio_cholerae.jpg License: Public Domain Contributors: Tom Kirn, Ron Taylor, Louisa Howard -Dartmouth Electron Microscope FacilityImage:Cholera.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Cholera.jpg License: Public Domain Contributors: Bohème, DL5MDA, Folcrum, Kramer Associates, Monaneko,Pmx, Shyam, Wolfmann, 4 anonymous editsImage:Cholera hospital in Dhaka.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Cholera_hospital_in_Dhaka.jpg License: Creative Commons Attribution 2.0 Contributors:MindmatrixFile:It doesn't hurt, but it tickles. A U.S. Navy hospital corpsman, member of a USAID military health team, inoculates a flo - NARA - 541855.jpg Source:http://en.wikipedia.org/w/index.php?title=File:It_doesn't_hurt,_but_it_tickles._A_U.S._Navy_hospital_corpsman,_member_of_a_USAID_military_health_team,_inoculates_a_flo_-_NARA_-_541855.jpg License: Public Domain Contributors: Bestiasonica, JustSomePics, Ras67, 2 anonymous editsImage:Cholera rehydration nurses.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Cholera_rehydration_nurses.jpg License: Public domain Contributors: Centers for DiseaseControl and PreventionImage:Cholera 395.1.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Cholera_395.1.jpg License: Public Domain Contributors: Sanatory Committee, under the sanction of theMedical Counsel, in New York CityFile:Africa cholera2008b.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Africa_cholera2008b.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors:Fowler&fowler«Talk». Original uploader was Fowler&fowler at en.wikipediaImage:ICS Lima.svg Source: http://en.wikipedia.org/w/index.php?title=File:ICS_Lima.svg License: Public Domain Contributors: Bukk, Denelson83, Indolences, MattesFile:Robert Koch (Deutsche Cholera-Expedition in Ägypten 1884).jpg Source:http://en.wikipedia.org/w/index.php?title=File:Robert_Koch_(Deutsche_Cholera-Expedition_in_Ägypten_1884).jpg License: Public Domain Contributors: Unknow

License 15
LicenseCreative Commons Attribution-Share Alike 3.0//creativecommons.org/licenses/by-sa/3.0/