
choanal atresia
77
5 1
-
Upload
tariq-maka -
Category
Health & Medicine
-
view
30 -
download
0
Transcript of choanal atresia

5
1

DR TARIQUE AHMED MAKA
REGISTRAR ENT
MANAGEMENT OF BILATERAL
CHOANAL ATRESIA

MANAGEMENT OF BILATERAL CHOANAL ATRESIA
SEQUENCE OF CPC Case presentation
Literature review
Statistical data
Conclusion
3

4
CASE PRESENTATION
MANAGEMENT OF BILATERAL CHOANAL ATRESIA

PATIENT PROFILE
Name XYZ
Age Newborn
Gender Male
Residence Rawalpindi
Date of admission 25.10.12
5

PRESENTING COMPLAINTS
Difficulty in breathing
Cyanotic spells
6
since birth

HISTORY OF PRESENT ILLNES
Difficulty in breathing
Cyanotic spells
7

ANTENATAL HISTORY
25yrs
PG
Planned pregnancy
Regular antenatal visits
8
NATAL HISTORY
39 weeks pregnancy
Spontaneous labour
Vertex presentation
Emergency LSCS
Liquor clear
9

POSTNATAL HISTORY
Baby cried immediately
APGAR score 8/10 ,9/10
Admitted in NICU
10

FAMILY HISTORY
Non consanguinous
No family history of any
Neonatal death
Congenital anomalies
Chronic illness in family
11

Medical History
Surgical History
Drug History
Socio economic history
Unremarkable
12

Heart rate 150 beats/min
Respiratory rate 66/min
Weight 2.1 kg
OFC 31.4cm
PHYSICAL EXAMINATION
13
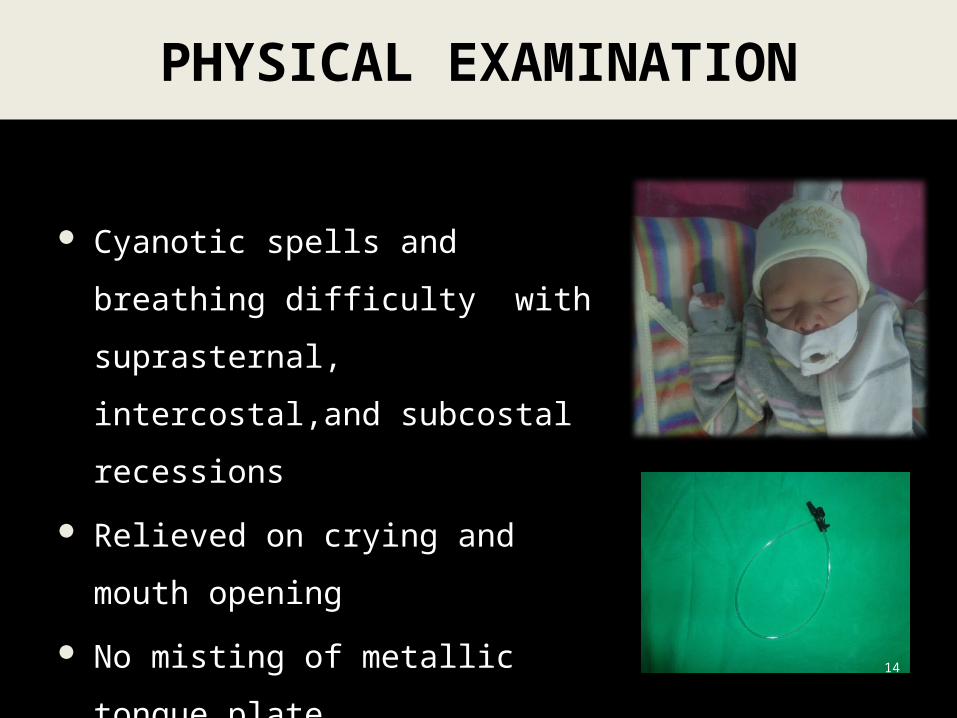
Cyanotic spells and breathing
difficulty with suprasternal,
intercostal,and subcostal recessions
Relieved on crying and mouth
opening
No misting of metallic tongue plate
Inability to pass nasal catheter
PHYSICAL EXAMINATION
14

No mass/cyst No laryngeal air way obstruction Vocal cords equally mobile
15
DIRECT LARYNGOSCOPY

GIT system
Central Nervous system
Cardiovascular System
Unremarkable
16
SYSTEMIC EXAMINATION

Bilateral choanal atresia
Laryngomalacia
Vocal cord palsy
Haemangioma
DIFFERENTIAL DIAGNOSIS
17
Subglotic stenosis

Test Result Reference range
Haemoglobin 17.4g/dL 16-20g/dL
Total Leucocyte Count 19.8x 10^9 /L 4.0-10.0x10^9 /L
HCT 0.528
MCV 101.3fl
MCH 33.4pg
MCHC 33.0g/l
Platelet Count 369 x 10 9 /L 150-400x10^9 /L
HAEMATOLOGICAL INVESTIGATION
1818
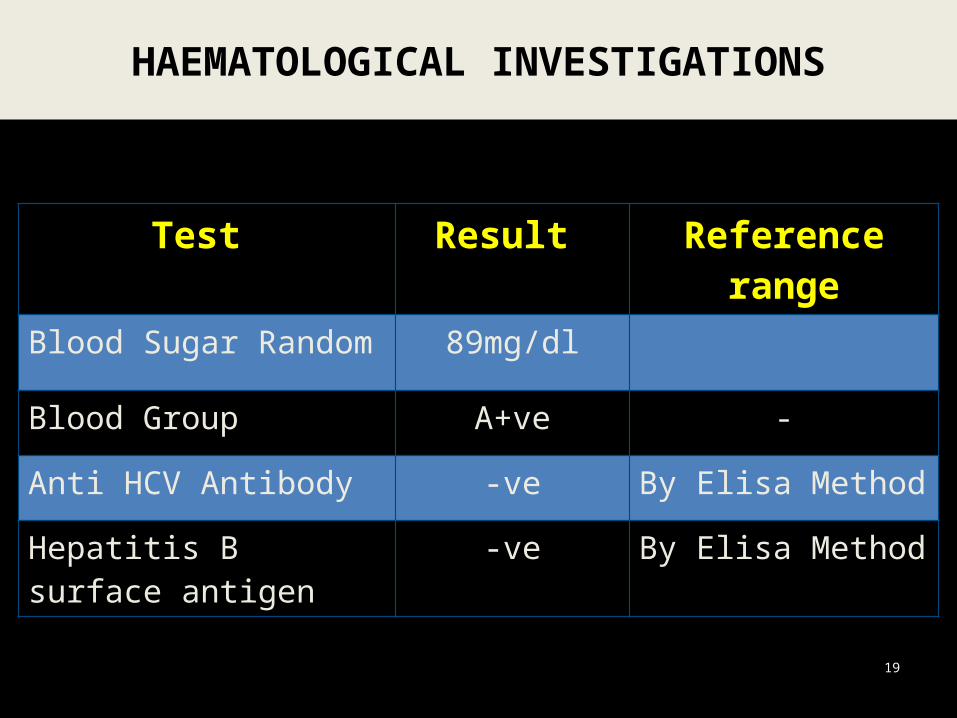
Test Result Reference range
Blood Sugar Random 89mg/dl
Blood Group A+ve -
Anti HCV Antibody -ve By Elisa Method
Hepatitis B surface antigen
-ve By Elisa Method
HAEMATOLOGICAL INVESTIGATIONS
19

TEST PATIENT CONTROL
PT 14 14
PTTK 32 32
HAEMATOLOGICAL INVESTIGATIONS
20

CT SCAN
CT scan paranasal sinus with contrast for delineation of Choanal atresia confirmed the diagnosis of bilateral choanal atresia of bony type
22

CT SCAN
23

CT SCAN
24

Case Summary
Newborn
Breathing difficulty and cyanotic spells
Relieved by crying
Inability to pass nasal catheter
Bilateral choanal atresia on CT scan
CASE SUMMARY
25

DIAGNOSIS
26
BILATERAL CHOANAL ATRESIA
Case Summary
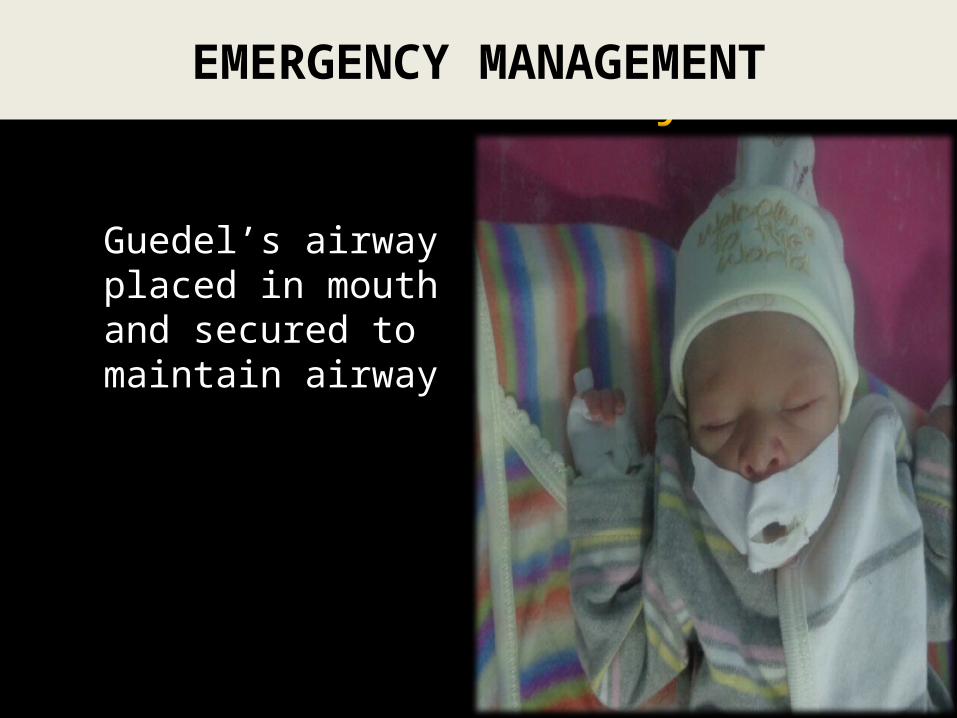
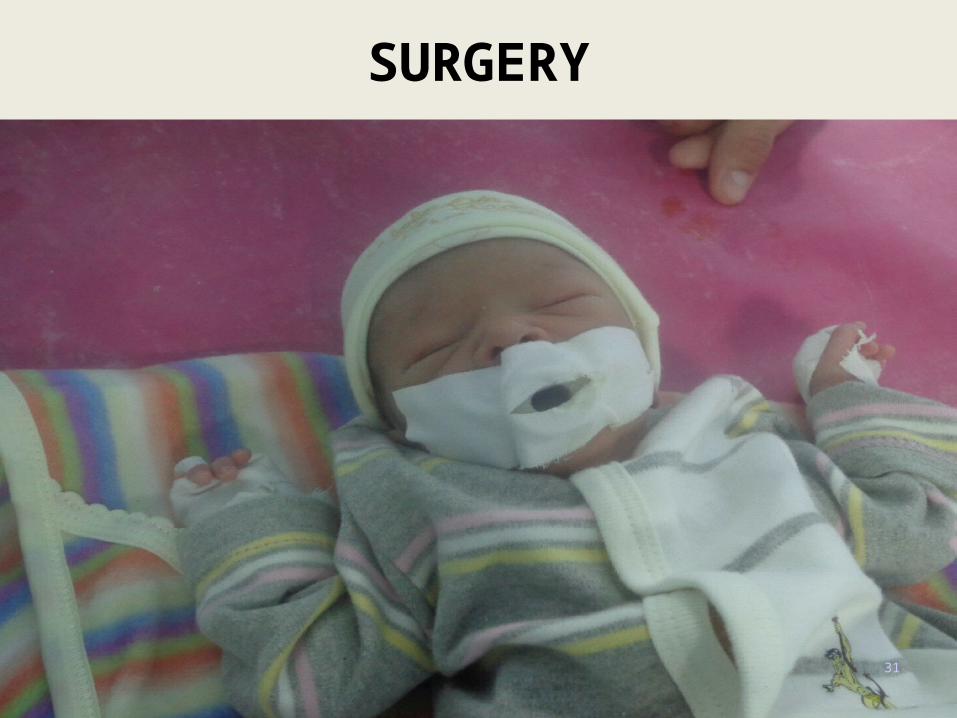
Guedel’s airway placed in mouth and secured to maintain airway
27
EMERGENCY MANAGEMENT
Case Summary
Inj vit K 1g i/m stat
Inj clefron 100mg i.v BD
inj amikin15 mg i.v BD
MANAGEMENT
28

Parents explained about the nature of condition in detail
Surgery planned through Transnasal approach
Pre-anaesthesia assessment done
Written informed consent obtained
29
SURGERY

30
OPERATIVE STEPS
31
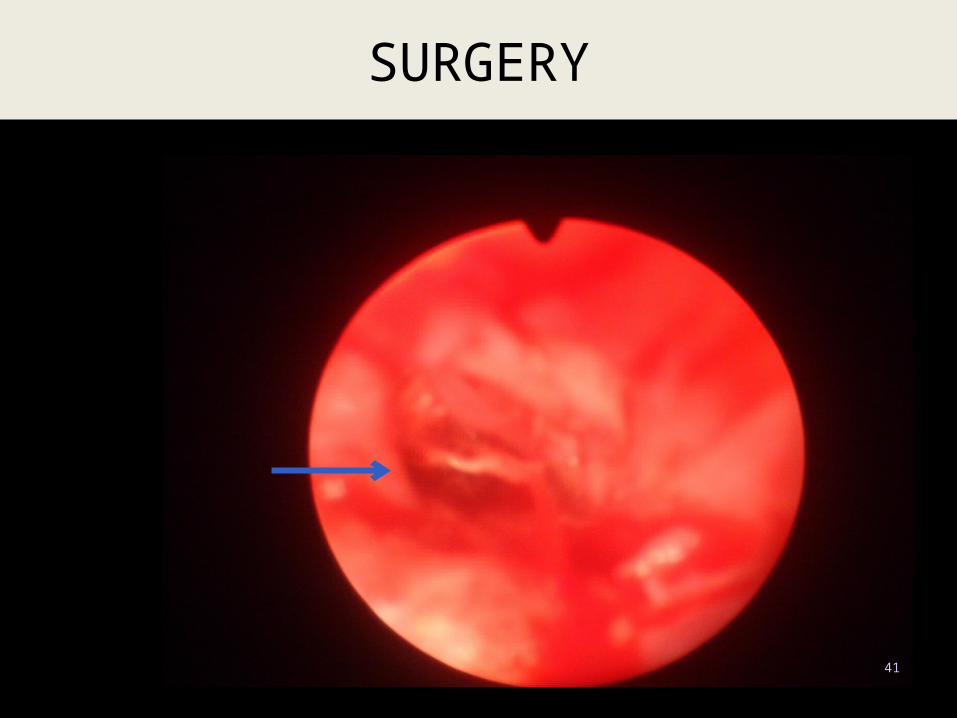
SURGERY

32
SURGERY

33
SURGERY

34
SURGERY

35
SURGERY

36
SURGERY

37
SURGERY

38
SURGERY

39
SURGERY

40
SURGERY
41
SURGERY

42
SURGERY

43
SURGERY

44
SURGERY

45
SURGERY

46
SURGERY

Nursed at neonatal ICU for 2 days Administered
Inj augmentin Inj dexamethasoneI/V fluids as advised by PediatricianRegular suction of tubes to prevent blockage
47
POST OP CARE

48
POST OP CARE

49
POST OP CARE

50
FOLLOW UP

51
PRESENT STATUS

LITERATURE REVIEW
52
PART II
LITERATURE REVIEW

1755, Roederer
18th CenturyFirst recorded case
19th CenturyFirst successful surgery
HISTORY OFCHOANAL ATRESIA
53
1854, Emmert

BRIEF ANATOMY OF CHOANAE
• Medially: Free posterior edge of vomer• Laterally: Medial pterygoid lamina• Roof : Body of sphenoid• Floor : Free posterior edge of horizontal plate
54

Choanal atresia is a rare life threatening congenital anomaly.
Persistence of nasobuccal membrane.
Unilateral or bilateral
CHOANAL ATRESIA
55
Haddad J Jr. Congenital disorders of the nose. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds.

EPIDEMIOLOGY
1 in 5,000 to 7,000 live births Females > males Atresias are bony,membranous or mixed Unilateral to bilateral cases is 2:1 Unilateral presentation predominantly affects the
right nasal aperture
56 Hengerer AS, Brickman TM, Jeyakumar A. Choanal atresia: embryologic analysis and evolution of treatment, a 30-year experience. Laryngoscope. May 2008;118(5):862-866.
ETIOLOGY
Cause is unknown Smoking Coffee consumption High zinc and B-12 intake Prenatal use of antithyroid
(methimazole, carbimazole) medications
57
Barbero P, Valdez R, Rodríguez H, et al. Choanal atresia associated with maternal hyperthyroidism treated with methimazole: a case-control study. Am J Med Genet A. Sep 15 2008;146A(18):2390-5.

PATHOGENESIS
58
Persistence of the buccopharyngeal membrane
Failure of the bucconasal membrane to rupture
Medial outgrowth of vertical and horizontal processes
of the palatine bone
Abnormal mesodermal adhesions forming in the
choanal area
Assanasen P, Metheetrairut C. Choanal atresia. J Med Assoc Thai. May 2009;92(5):699-706.

ASSOCIATED CONDITIONS
59
Coloboma Heart defects Atresia choanae Retardation of growth Genital anomalies Ear abnormalities
(CHARGE)
Asher BF et al. Airway Complications in CHARGE Association. Arch Otolaryngol Head Neck Surg. May 1990;116:594-595.

CLINICAL PRESENTATION
60
Bilateral choanal atresia is a life threatening condition:
Complete nasal obstruction Respiratory obstruction and
cyanosis is cyclic Inability to feed and breath at the
same time.
Sadek SA (January 1998). "Congenital bilateral choanal atresia" Int. J. Pediatr. Otorhinolaryngol. 42 (3): 247–56. doi:10.1016/S0165-5876(97)

CLINICAL EXAMINATION
Pashley NRT. Choanal Atresia,(Chapter33). Clinical Pediatric Otolaryngology. St. Louis, MO: C.V. Mosby Company; 1986 . 61v
Failure to pass a # 6 to 8 french plastic catheter through the nares
Placing wisps of cotton in front of the nares and absence of nasal movement of air.
Absence of fog on a mirror when placed under the nostrils

RECOMMENDED TESTS
62
CT scanEndoscopy of the noseCardiac echoRenal ultrasoundRhinogram

DIAGNOSTIC TEST
CT with intranasal contrast that shows narrowing of the posterior nasal cavity at the level of the pterygoid plate is the confirmatory test
Benjamin B. Evaluation of Choanal Atresia. Ann Otol Rhinol Laryngol. 94:429-432.63

64
MANAGEMENT OF
CHOANAL ATRESIA

MANAGEMENT
65
MANAGEMENT OF CHOANAL ATRESIA
EMERGENCY/ INITIAL
MANAGEMENT
SURGICAL MANAGEMENT

A. Airway oral airway of some sort must be
implemented very early
B. Feeding Delayed surgical correction;
orogastric tube
INITIAL MANAGEMENT
Hengerer AS et al. Choanal Atresia: A New Embryologic Theory and Its Influence on Surgical Management. Laryngoscope. August 1982;92:913-921.

A. Transnasal blind puncture
B. Transnasal endoscopic Approach
C. Transpalatal Approach
SURGICAL MANAGEMENT
67
Richardson MA and Osguthorpe JD. Choanal Atresia. Current Therapy in Otolaryngology-Head and Neck Surgery. St. Louis, MO: B.C. Decker Inc.; 1990

TECHNIQUE 120 degree endoscope placed in mouth and positioned
in nasopharynx
Atretic plate perforated
Bilateral nasal stents placed
Philtrum is protected
Stents left in situ for 6 weeks
TRANSNASAL ENDOSCOPIC APPROACH
68

Advantages: a. This approach is faster, easier, and less problematic.
b. Blood loss is minimal.
c. Excellent for children of all ages.
d. Allows for earlier repair in properly selected patients and may avoid restenosis.
e. The child can breast feed immediately post op.
f. If no additional problems then the child can be discharged on the 3rd or 4th post op day.
TRANSNASAL ENDOSCOPIC APPROACH
69

DISADVANTAGES AND COMPLICATIONS: a. Longer stenting time post op.
b. Can not be done on patients with multiple nasal and nasopharyngeal anomalies.
TRANSNASAL ENDOSCOPIC APPROACH
Josephson GD, Vickery CL, Giles WC, Gross CW. Transnasal endoscopic repair of congenital choanal atresia: long-term results. Arch Otolaryngol Head Neck Surg. May 1998;124(5):537-40.

TRANSPALATAL APPROACH In rare circumstances where the
skull base is abnormally developed (other craniofacial anomalies are present), the surgeon may need to use a transpalatal approach to access the area of choanal atresia through the roof of the mouth.
SURGICAL MANAGEMENT
Zeitouni AG, Shapiro RS. Congenital anomalies of the nose and anterior skull base. In: Tewfik TL, Der Kaloustian VM, eds. Congenital Anomalies of the Ear, Nose, and Throat. New York, NY: Oxford University Press; 1997:189-200

A. STENTING:
1. Secure them in place for a approximate period of 4-8 weeks
B. WOUND CARE:
2. The parents must be taught to maintain the stents with frequent suction and a saline-moistened pipe cleaner or cotton applicator 3 to 6 times per day.
3. Antibiotics and decongestant72
POST OPERATIVE CARE

C. FOLLOW UP:
1. Every 2 weeks or more frequently if needed while the stents are in place.
2. Once the stents are removed, the patients are seen weekly for the first 2-3 weeks.
73
POST OPERATIVE CARE

RELEVANT STATISTICAL DATA
74

RELEVANT DATA
Total Cases of CHOANAL ATRESIA = 4 Duration 1st JANUARY, 2011 to 1st JANUARY, 2013 Unilateral = 3 Bilateral = 1 75
BilateralUnilateral

RELEVANT DATA
The male female ratio was 1 : 3
76
male female0
0.5
1
1.5
2
2.5
3
3.5

Bilateral choanal atresia is a rare life threatening condition which presents with stridor and acute respiratory distress at birth
Only immediate clinical evaluation and efficient management is life saving
CONCLUSION
77

Thank You
78













![THREE NOVEL MUTATIONS OF CHD7 GENE IN TWO TURKISH … · syndrome [16]. Choanal atresia or stenosis is found in approximately half of the patients and noticed due to respiratory difficulty](https://static.fdocuments.in/doc/165x107/5f0d1c4d7e708231d438bad3/three-novel-mutations-of-chd7-gene-in-two-turkish-syndrome-16-choanal-atresia.jpg)




