
CHN NOTES.doc
78
CHN I – Definition of Terms Community- derived from a latin word “comunicas” which means a group of people. a group of people with common characteristics or interests living together within a territory or geographical boundary place where people under usual conditions are found Health – is the OLOF (Optimum Level of Functioning) Community Health – part of paramedical and medical intervention/approach which is concerned on the health of the whole population Aims: 1. health promotion 2. disease prevention 3. management of factors affecting health Nursing – both profession & a vocation. Assisting sick individuals to become healthy and healthy individuals achieve optimum wellness II – Community Health Nursing The utilization of the nursing process in the different levels of clientele-individuals, families, population groups and communities, concerned with the promotion of health, prevention of disease and disability and rehabilitation. Goal: “To raise the level of citizenry by helping communities and families to cope with the discontinuities in and threats to health in such a way as to maximize their potential for high-level wellness” MISSION OF CHN · Health Promotion · Health Protection · Health Balance
-
Upload
laniejeciel -
Category
Documents
-
view
289 -
download
4
Transcript of CHN NOTES.doc

CHNI – Definition of Terms
Community- derived from a latin word “comunicas” which means
a group of people.
a group of people with common characteristics or interests
living together within a territory or geographical boundary
place where people under usual conditions are found
Health – is the OLOF (Optimum Level of Functioning)
Community Health – part of paramedical and medical intervention/approach which is concerned on the health of the whole population
Aims:
1. health promotion
2. disease prevention
3. management of factors affecting health
Nursing – both profession & a vocation. Assisting sick individuals to become healthy and healthy individuals achieve optimum wellness
II – Community Health Nursing
The utilization of the nursing process in the different levels of clientele-individuals, families, population groups and communities, concerned with the promotion of health, prevention of disease and disability and rehabilitation.
Goal: “To raise the level of citizenry by helping communities and families to cope with the discontinuities in and threats to health in such a way as to maximize their potential for high-level wellness”
MISSION OF CHN
· Health Promotion
· Health Protection
· Health Balance
· Disease prevention
· Social Justice
PHILOSOPHY OF CHN

The philosophy of CHN is based on the worth and dignity on the worth and dignity of man.
Principles of Community Health:
1. The community is the patient in CHN, the family is the unit of care and there are four levels of clientele: individual, family, population group (those who share common characteristics, developmental stages and common exposure to health problems – e.g. children, elderly), and the community.
2. In CHN, the client is considered as an ACTIVE partner NOT PASSIVE recipient of care
3. CHN practice is affected by developments in health technology, in particular, changes in society, in general
4. The goal of CHN is achieved through multi-sectoral efforts
5. CHN is a part of health care system and the larger human services system.
Role of CH Nurse:
Clinician – who is a health care provider, taking care of the sick people at home or in the RHU
Health Advocator – speaks on behalf of the client
Advocator – act on behalf of the client
Supervisor – who monitors and supervises the performance of midwives
Facilitator – who establishes multi-sectoral linkages by referral system
Collaborator – working with other health team member
COMMON PROCEDURE IN CHN:
· HOME VISIT
· BAG TECHNIQUE
· STERILIZATION
· SPECIMEN COLLECTION
- URINE
- FECES
- SPUTUM
Levels of Client in CHN:
1. Application of Nursing Process to:
1.a Family
1.a.1 Family Coping Index

Physical Independence - ability of the family to move in & out of bed & performed activities of daily living
Therapeutic Independence - ability of the family to comply with the therapeutic regimen (diet, medication & usage of appliances)
Knowledge of Health Condition- wisdom of the family to understand the disease process
Application of General &Personal Hygiene- ability of the family to perform hygiene & maintain environment conducive for living
Emotional Competence – ability of the family to make decision maturely & appropriately (facing the reality of life)
Family Living Pattern- the relationship of the family towards each other with love, respect & trust
Utilization of Community Resources – ability of the family to know the function & existence of resources within the vicinity
Health Care Attitude – relationship of the family with the health care provider
Physical Environment – ability of the family to maintain environment conducive for living
1.a.2 Family Life Cycle
Stage I – Beginning Family (newly wed couples)
TASK: compliance with the PD 965 & acceptance of the new member of the family
Stage II – Early Child Bearing Family(0-30 months old)
TASK: emphasize the importance of pregnancy & immunization & learn the concept of parenting
Stage III –Family with Pre- school Children (3-6yrs old)
TASK: learn the concept of responsible parenthood
Stage IV – Family with School age Children (6-12yrs old)
TASK: Reinforce the concept of responsible parenthood
Stage V - Family with Teen Agers (13-25yrs old)
TASK: Parents to learn the concept of “let go system” and understands the “generation gap”
Stage VI – Launching Center (1st child will get married up to the last child)
TASK: compliance with the PD 965 & acceptance of the new member of the family
Stage VII -Family with Middle Adult parents (36-60yrs old)
TASK: provide a healthy environment, adjust with a new lifestyle and adjust with the financial aspect
Stage VIII – Aging Family (61yrs old up to death)

TASK: learn the concept of death positively
1.b Community
COMMUNITY ASSESSMENT:
Status
Structure
Process
TYPES OF COMMUNITY ASSESSMENT:
1. COMMUNITY DIAGNOSIS
A process by which the nurse collects data about the community in order to identify factors which may influence the deaths and illnesses of the population, to formulate a community health nursing diagnosis and develop and implement community health nursing interventions and strategies.
2 Types:
Comprehensive Community Diagnosis Problem-Oriented Community Diagnosis
- aims to obtain general information about the community
- type of assessment responds to a particular need
STEPS:
Preparatory Phase
1. site selection
2. preparation of the community
3. statement of the objectives
4. determine the data to be collected
5. identify methods and instruments for data collection
6. finalize sampling design and methods
7. make a timetable
Implementation Phase
1. data collection
2. data organization/collation
3. data presentation
4. data analysis

5. identification of health problems
6. priority zation of health problems
7. development of a health plan
8. validation and feedback
Evaluation Phase
BIOSTATISTICS
2.1 DEMOGRAPHY - study of population size, composition and spatial distribution as affected by births, deaths and migration.
Sources : Census – complete enumeration of the population
2 Ways of Assigning People:
1. De Jure – People were assigned to the place where assigned to the place they usually live regardless of where they are at the time of census.
2.De Facto – People were assigned to the place where they are physically present at are at the time of census regardless, of their usual place of residence.
Components:
1. Population size
2. Population composition
* Age Distribution
* Sex Ratio
* Population Pyramid
* Median age – age below which 50% of the population fall and above
which 50% of the population fall. The lower the median
age, the younger the population (high fertility, high death rates).
* Age – Dependency Ratio – used as an index of age-induced economic drain on human resources
* Other characteristics:
- occupational groups
- economic groups
- educational attainment
- ethnic group
3. Population Distribution

* Urban-Rural – shows the proportion of people living in urban compared to the rural areas
* Crowding Index – indicates the ease by which a communicable disease can be transmitted from 1 host to another susceptible host.
* Population Density – determines congestion of the place
VITAL STATISTICS
the application of statistical measures to vital events (births, deaths and common illnesses) that is utilized to gauge the levels of health, illness and health services of a community.
TYPES:
Fertility Rate
1. A. CRUDE BIRTH RATE
total # of livebirths in a given calendar year X 1000
estimated population as of July 1 of the same given year
1. B. GENERAL FERTILITY RATE
total # of livebirths in a given calendar year X 1000
Total number of reproductive age
Mortality Rate
A. CRUDE DEATH RATE
Total # of death in a given calendar year X 1000
Estimated population as of July 1 of the same calendar year
B. INFANT MORTALITY RATE
Total # of death below 1 yr in a given calendar year X 1000
Estimated population as of July 1 of the same calendar year
C. MATERNAL MORTALITY RATE
Total # of death among all maternal cases in a given calendar year X 1000
Estimated population as of July 1 of the same calendar year
Morbidity Rate
A. PREVALENCE RATE
Total # of new & old cases in a given calendar year X 100
Estimated population as of July 1 of the same calendar year
B. INCIDENCE RATE
Total # of new cases in a given calendar year X 100
Estimated population as of July 1 of the same calendar year
C. ATTACK RATE
Total # of person who are exposed to the disease X 100
Estimated population as of July 1 of the same calendar year
III – Epidemiology
The study of distribution of disease or physiologic condition among human population s and the factors affecting such distribution
the study of the occurrence and distribution of health conditions such as disease, death, deformities or disabilities on human populations
1. a. Patterns of disease occurrence
Epidemic
- a situation when there is a high incidence of new cases of a specific disease in excess of the expected.
- when the proportion of the susceptibles are high compared to the proportion of the immunes
Epidemic potential
- an area becomes vulnerable to a disease upsurge due to causal factors such as climatic changes, ecologic changes, or socio-economic changes
Endemic
- habitual presence of a disease in a given geographic location accounting for the low number of both immunes and susceptibles
e.g. Malaria is a disease endemic at Palawan.
- the causative factor of the disease is constantly available or present to the area.
Sporadic
- disease occurs every now and then affecting only a small number of people relative to the total population
- intermittent
Pandemic
- global occurrence of a disease

Steps in EPIDEMIOLOGICAL IVESTIGATION:
1. Establish fact of presence of epidemic
2. Establish time and space relationship of the disease
3. Relate to characteristics of the group in the community
4. Correlate all data obtained
1. b. Role of the Nurse
Case Finding
Health Teaching
Counseling
Follow up visit
IV. Health Situation of the Philippines
Philippine Scenario:
· In the past 20 years some infectious degenerative diseases are on the rise.
· Many Filipinos are still living in remote and hard to reach areas where it is difficult to deliver the health services they need
· The scarcity of doctors, nurses and midwives add to the poor health delivery system to the poor
VITAL HEALTH STATISTICS 2005
• PROJECTED POPULATION :
MALE – 42,874,766
FEMALE – 42,362,147
BOTH SEXES - 85,236,913
• LIFE EXPECTANCY
FEMALE - 70 yrs. old
MALE - 64 yrs. Old
LEADING CAUSES OF MORBIDITY
· Most of the top ten leading causes of morbidity are communicable disease
· These include the diarrhea, pneumonia, bronchitis, influenza, TB, malaria and varicella
· Leading non CD are heart problem, HPN, accidents and malignant neoplasm
LEADING CAUSES OF MORTALITY

· The top 10 leading causes of mortality are due to non CD
· Diseases of the heart and vascular system are the 2 most common causes of deaths.
· Pneumonia, PTB and diarrheal diseases consistently remain the 10 leading causes of deaths.
V. Health Care Delivery System
the totality of all policies, facilities, equipments, products, human resources and services which address the health needs, problems and concerns of the people. It is large, complex, multi-level and multi-disciplinary.
HEALTH SECTORS
· GOVERNMENT SECTORS
Department of Health
Vision: Health for all by year 2000 ands Health in the Hands of the People by 2020
Mission: In partnership with the people, provide equity, quality and access to health care esp. the marginalized
5 Major Functions:
1. Ensure equal access to basic health services
2. Ensure formulation of national policies for proper division of labor and proper coordination of operations among the government agency jurisdictions
3. Ensure a minimum level of implementation nationwide of services regarded as public health goods
4. Plan and establish arrangements for the public health systems to achieve economies of scale
5. maintain a medium of regulations and standards to protect consumers and guide providers
· NON GOVERNMENT SECTORS
· PRIVATE SECTORS
PRIMARY STRATEGIES TO ACHIEVE HEALTH GOALS
· Support for health goal
· Assurance of health care
· Increasing investment for PHC
· Development of National Standard
MILESTONE IN HEALTH CARE DELIVRY SYSTEM
· RA 1082 - RHU Act
· RA 1891 - Strengthen Health Services

· PD 568 - Restructuring HCDS
· RA 7160 - LGU Code
VI – National Health Plan
National Health Plan is a long-term directional plan for health; the blueprint defining the country’s health – PROBLEMS, POLICY THRUSTS STRATEGIES, THRUSTS
GOAL :
to enable the Filipino population to achieve a level of health which will allow Filipino to lead a socially and economically-productive life, with longer life expectancy, low infant mortality, low maternal mortality and less disability through measures that will guarantee access of everyone to essential health care
OBJECTIVES:
promote equity in health status among all segments of society
address specific health problems of the population
upgrade the status and transform the HCDS into a responsive, dynamic and highly efficient, and effective one in the provision of solutions to changing the health needs of the population
promote active and sustained people’s participation in health care
“ MAJOR HEALTH PLANS TOWARDS “HEALTH IN THE HANDS OF THE
PEOPLE IN THE YEAR 2020”
A. MAJOR HEALTH PLAN
· 23 IN 93
· Health for more in 94
· Think health…… Health Link
· 5 in 95
B. PRIORITY PROGRAM IN YEAR 2000
· Plan 50
· Plan 500
· Women’s health
·

Children’s health
· Healthy Lifestyle
· Prevention & Control of Infectious Disease
C. PRIORITY PROGRAM IN THE YEAR 2005
· Ligtas Buntis Campaign
· Mag healthy Lifestlye tayo
· TB Network
· Blood Donation Program (RA 7719)
· DTOMIS
· Ligtas Tigdas Campaign
· Murang Gamot
· Anti Tobacco Signature Campaign
· Doctors to the Barrios Program
· Food Fortification Program
· Sentrong Sigla Movement
D. NATIONAL HEALTH EVENTS FOR 2006
JANUARY
· National Cancer Consciousness Week – (16-22)
FEBRUARY
· Heart Month

· Dental Health Month
· Responsible Parenthood Campaign National Health Insurance Program
MARCH
· Women’s Health Month
· Rabies Awareness Month
· Burn Injury Prevention Month
· Responsible Parenthood Campaign
· Colon and Rectal Cancer Awareness Month
· World TB Day – (24)
APRIL
· Cancer in Children Awareness Month
· World Health Day – (7)
· Bright Child Week Phase I -
· Garantisadong Pambata (11-17)
MAY
· Natural Family Planning Month
· Cervical Cancer Awareness Month
· AIDS Candlelight Memorial Day – (21)
· World No Tobacco Day – (31)
JUNE
· Dengue Awareness Month
· No Smoking Month
· National Kidney Month
· Prostate Cancer Awareness Month
JULY
· Nutrition Month
· National Blood Donation Month
· National Disaster Consciousness Month
AUGUST

· National Lung Month
· National Tuberculosis Awareness Month
· Sight-Saving Month
· Family Planning Month
· Lung Cancer Awareness Month
SEPTEMBER
· Generics Awareness Month
· Liver Cancer Awareness Month
OCTOBER
· National Children’s Month
· Breast Cancer Awareness Month
· National Newborn Screening Week (3-9)
· Bright Child Week Phase II Garantisadong Pambata (10-16)
NOVEMBER
· Filariasis Awareness Month
· Cancer Pain Management Awareness Month
· Traditional and Alternative Health Care Month
· Campaign on Violence Against Women and Children
DECEMBER
· Firecracker Injury Prevention Campaign:
· “OPLAN IWAS PAPUTOK”
VII – INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESSES (IMCI)
INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESSES (IMCI)
· IMCI is an integrated approach to child health that focuses on the well-being of the whole child.
· IMCI strategy is the main intervention proposed to achieve a significant reduction in the number of deaths from communicable diseases in children under five
Goal:
· By 2010, to reduce the infant and under five mortality rate at least one third, in pursuit of the goal of reducing it by two thirds by 2015.
AIM:
· to reduce death, illness and disability, and to promote improved growth and development among children under 5 years of age.
· IMCI includes both preventive and curative elements that are implemented by families and communities as well as by health facilities.
IMCI OBJECTIVES:
· To reduce significantly global mortality and morbidity associated with the major causes of disease in children
· To contribute to the healthy growth & development of children
IMCI COMPONENTS OF STRATEGY:
· Improving case management skills of health workers
· Improving the health systems to deliver IMCI
· Improving family and community practices
**For many sick children a single diagnosis may not be apparent or appropriate
Presenting complaint:
· Cough and/or fast breathing
· Lethargy/Unconsciousness
· Measles rash
· “Very sick” young infant
Possible course/ associated condition:
· Pneumonia, Severe anemia, P. falciparum malaria
· Cerebral malaria, meningitis, severe dehydration
· Pneumonia, Diarrhea, Ear infection
· Pneumonia, Meningitis, Sepsis
Five Disease Focus of IMCI:
· Acute Respiratory Infection
· Diarrhea
· Fever
·
Malaria
· Measles
· Dengue Fever
· Ear Infection
· Malnutrition
THE IMCI CASE MANAGEMENT PROCESS
· Assess and classify
· Identify appropriate treatment
· Treat/refer
· Counsel
· Follow-up
THE INTEGRATED CASE MANAGEMENT PROCESS
Check for General Danger Signs:
· A general danger sign is present if:
- the child is not able to drink or breastfeed
- the child vomits everything
- the child has had convulsions
- the child is lethargic or unconscious
ASSESS MAIN SYMPTOMS
· Cough/DOB
· Diarrhea
· Fever
· Ear problems
ASSESS AND CLASSIFY COUGH OR DIFFICULTY OF BREATHING
- Respiratory infections can occur in any part of the respiratory tract such as the nose, throat, larynx, trachea, air passages or lungs.
Assess and classify PNEUMONIA
· cough or difficult breathing

· an infection of the lungs
· Both bacteria and viruses can cause pneumonia
· Children with bacterial pneumonia may die from hypoxia (too little oxygen) or sepsis (generalized infection).
** A child with cough or difficult breathing is assessed for:
· How long the child has had cough or difficult breathing
· Fast breathing
· Chest indrawing
· Stridor in a calm child.
REMEMBER:
** If the child is 2 months up to 12 months the child has fast breathing if you count 50 breaths per minute or more
** If the child is 12 months up to 5 years the child has fast breathing if you count 40 breaths per minute or more.
IMCI COLOR CODING
PINK(URGENT REFERRAL) YELLOW(Treatment at outpatient health facility)
GREEN(Home management)
OUTPATIENT HEALTH FACILITY
•Pre-referral treatments
•Advise parents
•Refer child
OUTPATIENT HEALTH FACILITY
•Treat local infection
•Give oral drugs
•Advise and teach caretaker
Follow-up
HOMECaretaker is counseled on:
•Home treatment/s
•Feeding and fluids
•When to return immediately
Follow-up
REFERRAL FACILITY
•Emergency Triage and Treatment ( ETAT)
•Diagnosis, Treatment
•Monitoring, follow-up
SEVERE PNEUMONIA OR VERY SEVERE DISEASE
•Give first dose of an appropriate antobiotic
•Give Vitamin A
•Treat the child to prevent low blood sugar
•Refer urgently to the

hospital
•Give paracetamol for fever > 38.5oC
•Any general danger sign or
•Chest indrawing or
•Stridor in calm child
PNEUMONIA
•Give an appropriate antibiotic for 5 days
•Soothe the throat and relieve cough with a safe remedy
•Advise mother when to return immediately
•Follow up in 2 days
•Give Paracetamol for fever > 38.5oC
Fast breathing NO PNEUMONIA : COUGH OR COLD
•If coughing more than more than 30 days, refer for assessment
•Soothe the throat and relieve the cough with a safe remedy
•Advise mother when to return immediately
Follow up in 5 days if not improving
•No signs of pneumonia or very severe disease
Assess and classify DIARRHEA
A child with diarrhoea is assessed for:
· how long the child has had diarrhoea
· blood in the stool to determine if the child has dysentery
· signs of dehydration
Classify DYSENTERY
· child with diarrhea and blood in the stool

Two of the following signs ?
Abnormally sleepy or difficult to awaken
Sunken eyes
Not able to drink or drinking poorly
Skin pinch goes back very slowly
SEVERE DEHYDRATION
•If child has no other severe classification:
- Give fluid for severe dehydration ( Plan C ) OR
If child has another severe classification :
- Refer URGENTLY to hospital with mother giving frequent sips of ORS on the way - Advise the mother to continue breastfeeding
If child is 2 years or older and there is cholera in your area, give antibiotic for cholera
Two of the following signs :
Restless, irritable
Sunken eyes
Drinks eagerly, thirsty
Skin pinch goes back slowly
SOME DEHYDRATION
•Give fluid and food for some dehydration ( Plan B )
If child also has a severe classification :
- Refer URGENTLY to hospital with mother giving frequent sips of ORS on the way - Advise mother when to return immediately
Follow up in 5 days if not improving
•Not enough signs to classify as some or severe dehydration
NO DEHYDRATION
•Home Care
Give fluid and food to treat diarrhea at home ( Plan A )
•Advise mother when to return immediately
•Follow up in 5 days if not improving
Dehydration present SEVERE PERSISTENT DIARRHEA
•Treat dehydration before referral unless the child has another severe classification

Give Vitamin a
Refer to hospital
No dehydration PERSISTENT DIARRHEA
•Advise the mother on feeding a child who has persistent diarrhea
Give Vitamin A
Follow up in 5 days
Blood in the stool DYSENTERY
•Treat for 5 days with an oral antibiotic recommended for Shigella in your area
Follow up in 2 days
Give also referral treatment
Does the child have fever?
**Decide :
- Malaria Risk
- No Malaria Risk
- Measles
- Dengue
Malaria Risk
•Any general danger sign or
Stiff neck
VERY SEVERE FEBRILE DISEASE / MALARIA
•Give first dose of quinine ( under medical supervision or if a hospital is not accessible within 4hrs )
Give first dose of an appropriate antibiotic
Treat the child to prevent low blood sugar
Give one dose of paracetamol in health center for high fever

(38.5oC) or above
Send a blood smear with the patient
Refer URGENTLY to hospital
•Blood smear ( + )
If blood smear not done:
NO runny nose, and
NO measles, and
NO other causes of fever
MALARIA
•Treat the child with an oral antimalarial
Give one dose of paracetamol in health center for high fever (38.5oC) or above
Advise mother when to return immediately
Follow up in 2 days if fever persists
If fever is present everyday for more than 7 days, refer for assessment
•Blood smear ( – ), or
Runny nose, or
Measles, or
Other causes of fever
FEVER : MALARIA UNLIKELY
•Give one dose of paracetamol in health center for high fever (38.5oC) or above
Advise mother when to return immediately
Follow up in 2 days if fever persists
If fever is present everyday for more than 7 days, refer for assessment
No Malaria Risk
•Any general danger sign or
VERY SEVERE FEBRILE DISEASE
•Give first dose of an appropriate antibiotic
Treat the child to prevent low

Stiff neck
blood sugar
Give one dose of paracetamol in health center for high fever (38.5oC) or above
Refer URGENTLY to hospital
•No signs of very severe febrile disease
FEVER : NO MALARIA
•Give one dose of paracetamol in health center for high fever (38.5oC) or above
Advise mother when to return immediately
Follow up in 2 days if fever persists
If fever is present everyday for more than 7 days, refer for assessment
Measles
•Clouding of cornea or
Deep or extensive mouth ulcers
SEVERE COMPLICATED MEASLES
•Give Vitamin A
Give first dose of an appropriate antibiotic
If clouding of the cornea or pus draining from the eye, apply tetracycline eye ointment
Refer URGENTLY to hospital
•Pus draining from the eye or
Mouth ulcers
MEASLES WITH EYE OR MOUTH COMPLICATIONS
•Give Vitamin A
If pus draining from the eye, apply tetracycline eye ointment
If mouth ulcers, teach the mother to treat with gentian

violet
•Measles now or within the last 3 months
MEASLES •Give Vitamin A
Dengue Fever
•Bleeding from nose or gums or
Bleeding in stools or vomitus or
Black stools or vomitus or
Skin petechiae or
Cold clammy extremities or
Capillary refill more than 3 seconds or
Abdominal pain or
Vomiting
Tourniquet test ( + )
SEVERE DENGUE HEMORRHAGIC FEVER
•If skin petechiae or Tourniquet test,are the only positive signs give ORS
If any other signs are positive, give fluids rapidly as in Plan C
Treat the child to prevent low blood sugar
DO NOT GIVE ASPIRIN
Refer all children Urgently to hospital
No signs of severe dengue hemorrhagic fever
FEVER: DENGUE HEMORRHAGIC UNLIKELY
•DO NOT GIVE ASPIRIN
Give one dose of paracetamol in health center for high fever (38.5oC) or above
Follow up in 2 days if fever persists or child shows signs of bleeding
Advise mother when to return immediately
Does the child have an ear problem?
•Tender swelling MASTOIDITIS •Give first dose of

behind the ear
appropriate antibiotic
Give paracetamol for pain
• Refer URGENTLY
•Pus seen draining from the ear and discharge is reported for less than 14 days or
Ear pain
ACUTE EAR INFECTION
•Give antibiotic for 5 days
Give paracetamol for pain
Dry the ear by wicking
Follow up in 5 days
•Pus seen draining from the ear and discharge is reported for less than 14 days
CHRONIC EAR INFECTION •Dry the ear by wicking
Follow up in 5 days
•No ear pain and no pus seen draining from the ear
NO EAR INFECTION •No additional
treatment
Check for Malnutrition and Anemia
Give an Appropriate Antibiotic:
1. A. For Pneumonia, Acute ear infection or Very Severe disease
2. COTRIMOXAZOLEBID FOR 5 DAYS AMOXYCILLINBID FOR 5 DAYS
Age or Weight Adulttablet Syrup Tablet Syrup
2 months up to 12 months ( 4 – < 9 kg )
1 / 2 5 ml 1 / 2 5 ml
12 months up to 5 years ( 10 – 19kg )
1 7.5 ml 1 10 ml
B. For Dysentery
COTRIMOXAZOLEBID FOR 5 DAYS AMOXYCILLINBID FOR 5 DAYS
AGE OR WEIGHT TABLET SYRUP SYRUP 250MG/5ML

2 – 4 months( 4 – < 6kg )
½ 5 ml 1.25 ml ( ¼ tsp )
4 – 12 months( 6 – < 10 kg )
½ 5 ml 2.5 ml ( ½ tsp )
1 – 5 years old( 10 – 19 kg )
1 7.5 ml ( 1 tsp )
C. For Cholera
TETRACYCLINEQID FOR 3 DAYS
COTRIMOXAZOLEBID FOR 3 DAYS
AGE OR WEIGHT Capsule 250mg Tablet Syrup
2 – 4 months( 4 – < 6kg ) ¼ 1 / 2 5ml
4 – 12 months( 6 – < 10 kg ) ½ 1 / 2 5 ml
1 – 5 years old( 10 – 19 kg 1 1 7.5m
Give an Oral Antimalarial
CHOLOROQUINEGive for 3 days
PrimaquineGive single dose in health center for P. Falciparum
PrimaquineGive daily for 14 days for P. Vivax
Sulfadoxine + PyrimethamineGive single dose
AGE TABLET ( 150MG ) TABLET( 15MG) TABLET( 15MG) TABLET( 15MG)
DAY1 DAY2 DAY3
2months –5months
½ ½ ½ ¼
5 months –12 months
½ ½ ½ 1/2

12months –3 years old
1 1 ½ ½ ¼ ¾
3 years old -5 years old
1 ½ 1 ½ 1 3/4 1/2 1
GIVE VITAMIN A
AGE VITAMIN A CAPSULES200,000 IU
6 months – 12 months 1//2
12 months – 5 years old 1
GIVE IRON
AGE or WEIGHT Iron/Folate TabletFeSo4 200mg + 250mcg Folate (60mg elemental iron)
Iron SyrupFeSo4 150 mg/5ml( 6mg elemental iron per ml )
2months-4months( 4 – <6kg ) 2.5 ml
4months – 12months( 6 – <10kg )
4 ml
12months – 3 years ( 10 – <14kg )
1/2 5 ml
3years – 5 years ( 14 – 19kg ) 1/2 7.5 ml
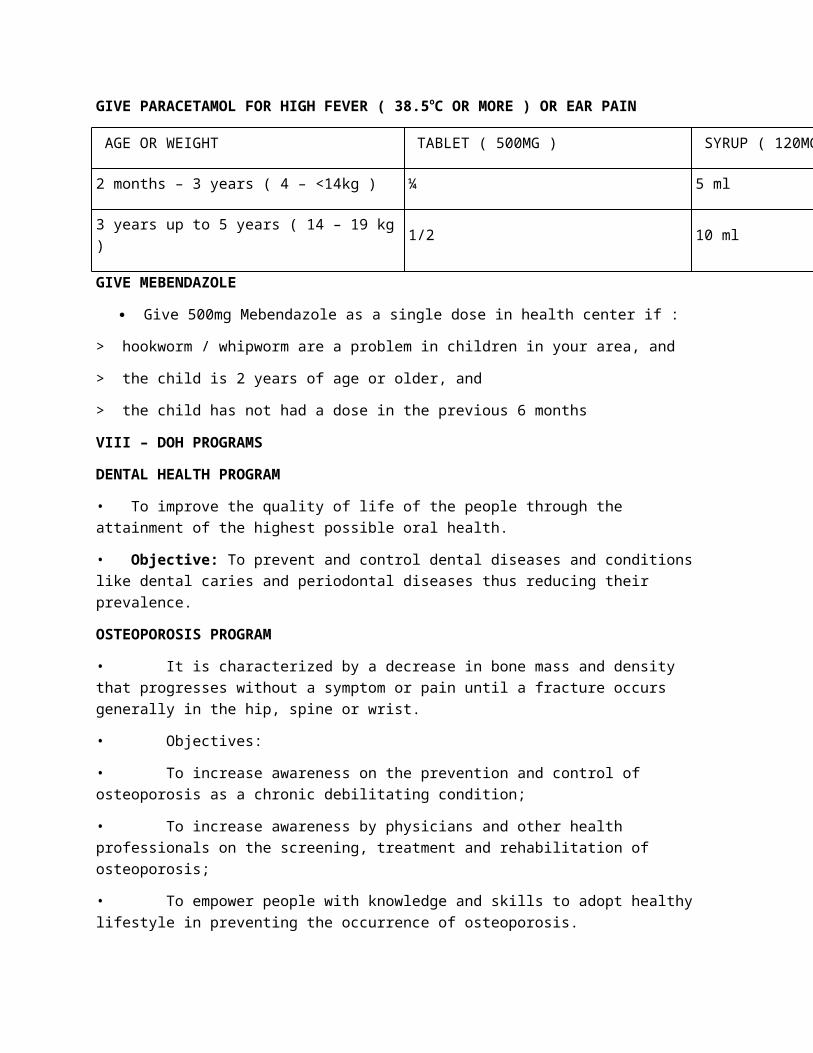
GIVE PARACETAMOL FOR HIGH FEVER ( 38.5oC OR MORE ) OR EAR PAIN
AGE OR WEIGHT TABLET ( 500MG ) SYRUP ( 120MG / 5ML )
2 months – 3 years ( 4 – <14kg ) ¼ 5 ml
3 years up to 5 years ( 14 – 19 kg ) 1/2 10 ml
GIVE MEBENDAZOLE
Give 500mg Mebendazole as a single dose in health center if :
> hookworm / whipworm are a problem in children in your area, and

> the child is 2 years of age or older, and
> the child has not had a dose in the previous 6 months
VIII – DOH PROGRAMS
DENTAL HEALTH PROGRAM
• To improve the quality of life of the people through the attainment of the highest possible oral health.
• Objective: To prevent and control dental diseases and conditions like dental caries and periodontal diseases thus reducing their prevalence.
OSTEOPOROSIS PROGRAM
• It is characterized by a decrease in bone mass and density that progresses without a symptom or pain until a fracture occurs generally in the hip, spine or wrist.
• Objectives:
• To increase awareness on the prevention and control of osteoporosis as a chronic debilitating condition;
• To increase awareness by physicians and other health professionals on the screening, treatment and rehabilitation of osteoporosis;
• To empower people with knowledge and skills to adopt healthy lifestyle in preventing the occurrence of osteoporosis.
HEALTH EDUCATION & CO
· Accepted activity at all levels of public health used as a means of improving the health of the people through techniques which may influence peoples thought motivation, judgment and action.
Three aspects of health education:
Information
Communication
Education
Sequence of steps in health education:
Creating awareness
Creating motivation
Decision making action
REPRODUCTIVE HEALTH
1. Family Planning

2. MCH & Nutrition
3. Prevention / treatment of Reproductive Tract Infection & STD
4. Prevention of abortion & its complication
5. Education & counseling on sexuality & sexual health
6. Adolescent sexual reproductive health
7. Violence against women
8. Men’s reproductive health ( Male sexual disorder )
9. Breast CA & other gyne problem
10. Prevention / treatment of infertility
OLDER PERSONS HEALTH SERVICES
· Participation in the celebration of Healthy National Elderly Week ( Oct 1-7)- Lecture on healthy lifestyle for the elderly
· Provision of drugs for the elderly( 20% discount)
GUIDELINES FOR GOOD NUTRITION
· Nutritional Guidelines are primary recommendations to promote good health through proper nutrition.
ACTIVITIES:
1.Malnutrition Rehabilitation Program
• Targeted Food Task Force Assistance Program (TFAP)
• Nutrition Rehabilitation Ward
• Akbayan sa Kalusugan sa Kabataan (ASK Project)
2.Micronutrient Supplementation Program
· “23 in ‘93”
· Fortified Vitamin Rice
· “Health for More in ‘94”
· “Buwan ng Kabataan, Pag-asa ng Bayan”
· National Focus: National Micronutrient Day or “Araw ng Sangkap Pinoy“
PROTEIN ENERGY MALNUTRITION
1. Marasmus – looks like an old worried man
- less subcutaneous fats

2. Kwashiorkor – a moon face child
- with flag sign (hair changes)
VITAMIN A DEFICIENCY
Early symptoms: Xeropthalmia (Nigtblindess)
Bitot’s spot (silvery foamy spot located @ lateral sclera)
Corneal Xerosis (eye lesion)
Conjunctival Xerosis(scar in the eyes)
Keratomalacia ( whitish to grayish sclera)
BLINDNESS
RESPIRATORY INFECTION CONTROL
• Provision of medicines
• Consultative meetings with CARI coordinators
• Monitoring of health facilities on the implementation of the program
ALTERNATIVE MEDICINE
· RA 8423
· 23 IN 93
1. A. Herbal Medicine(LUBBY SANTA)
Herbal Medicine
USES
Lagundi ( Vitex Negundo)
SHARED
Skin diseases
Headache,
Asthma,fever,cough&colds
Rheumatism
Eczema
Dysentery

Ulasimang Bato (Peperonia Pellucida) Lowers uric acid
Bawang ( Allium Sativum) HAT
Headache and Tootache
Bayabas ( Psidium Guajava) Anti septic, Anti-diarrheal
Yerba Buena (Mentha Cordifolia)Rheumatism and other body aches, analgesics
Sambong (Blumea Balsamifera) Edema, diuretics
Akapulko Fungal infection, skin diseases
Niog Niogan (Quisqualis Indica) Anti-helminthic
Tsaang Gubat (Carmona Retusa) Diarrhea
Ampalaya (Momordica Charantia) DM
MATERNAL- CHILD CARE
I – Maternal Care
A. FAMILY PLANNING
I. Spacing / Artificial Method
A. Hormonal
B. Mechanical & Barrier
C. Biologic
D. Natural
II. Permanent (surgical/irreversible)
A. Tubal Ligation
B. Vasectomy
III. Behavioral Method
B. BREASTFEEDING
II – CHILD CARE
A. UNDER FIVE CARE PROGRAM

· A package of child health-related services focused to the 0-59 months old children to assure their wellness and survival
Growth Monitoring Chart (GMC)
· A standard tool used in health centers to record vital information related to child growth and development, to assess signs of malnutrition
B. EXPANDED PROGRAM ON IMMUNIZATION
· LEGAL BASIS
· PD #996 – Compulsory basic
· PP #147 – National Immunization Day
· PP #773 – Knock out Polio Days
· PP # 1064 – polio eradication campaign
· PP #4 - Ligtas Tigdas month
MENTAL HEALTH
a state of well-being where a person can realize his or her own abilities, to cope with the normal stresses of life and work productively
Components of Mental Health Program
Stress Management and Crisis Intervention
Drugs and Alcohol Abuse Rehabilitation
Treatment and Rehabilitation of Mentally-Ill Patients
Special Project for Vulnerable Groups
SENTRONG SIGLA MOVEMENT
AIM: to promote availability of quality health services
4 pillars:
Quality assurance
Grants & technical assistance
Health promotion
Award
COMMUNITY ORGANIZING PARTICIPATORY ACTION RESEARCH
Community Organizing
· a continuous and sustained process of

· EDUCATING THE PEOPLE,
· CRITICAL AWARENESS
· MOBILIZING
Participatory Action Research
· A combination of education, research and action.
· The purpose is the EMPOWERMENT of people
4 Phases:
· Pre entry
· Entry
· Organizational Building
· Sustenance and Strengthening
Laws Affecting CHN Implementation:
RA 8749 – Clean Air Act (2000)
RA 6425 – Dangerous Drug Act: sale, administration and distribution of prohibited drugs is punishable by law
RA 9173
RA 2382 – Philippines Medical Act: define the practice of medicine in the Philippines
RA 1082 – Rural Health Act: employment of more physicians, nurses, midwives who will live in the rural areas to help raise the health condition.
RA 3573 – Reporting of Communicable Disease
RA 6675 – Generic Act: promotes, requires and ensures the production of an adequate supply, distribution, use of drugs identified by their generic names.
RA 6365
RA 6758
RA 4703
RA 7305 – Magna Carta for Public Health Workers (approved by Pres. Corazon C. Aquino): aims to promote and improve the social and economic well being of health workers, their living and conditions.
RA 7160 – Local Government Code: responsibility for the delivery of basic services of the national government
IX – CHRONIC COMMUNICABLE DISEASES
I – TUBERCULOSIS
TB is a highly infectious chronic disease that usually affects the lungs.
Causative Agent: Mycobacterium Tuberculosis
S/S:
cough
afternoon fever
weight loss
night sweat
blood stain sputum
Prevalence/Incidence:
ranks sixth in the leading causes of morbidity (with 114,221 cases) in the Philippines
sixth leading cause of mortality (with 28507 cases) in the Philippines.
Nursing and Medical Management
Ventilation systems
Ultraviolet lighting
Vaccines, such as the bacillus Calmette Guerin (BCG) vaccine
drug therapy
Preventing Tuberculosis
BCG vaccination
Adequate rest
Balanced diet
Fresh air
Adequate exercise
Good personal Hygiene
DOTS (Direct Observed Treatment Short Course)
Regimen Type of TB Patient
Regimen I
2RIPE / 4RI
New pulmonary smear (+) cases
New seriously ill pulmonary smear (-)

cases w/ extensive lung lesions
New severely ill extra-pulmo TB
Regimen II
2RIPES/
1RIPE / 5RIE
New pulmonary smear (+) case
New seriously ill pulmonary smear (-) cases w/ extensive lung lesions
New severely ill extra-pulmo TB
Regimen III
2RIP / 4RI
New smear(-) but with minimal pulmonary TB on radiography as confirmed by a medical officer
New extra-pulmo TB (not serious)
II – LEPROSY
Sometimes known as Hansen’s disease
is an infectious disease caused by , an aerobic, acid fast, rod-shaped mycobacterium
Gerhard Armauer Hansen
Historically, leprosy was an incurable and disfiguring disease
Today, leprosy is easily curable by multi-drug antibiotic therapy
Signs & Symptoms
Early stage(CLUMP) Late Stage(GMISC)
Change in skin color Gynocomastia
Loss in sensation Madarosis(loss of eyebrows)
Ulcers that do not heal Inability to close eyelids (Lagopthalmos)
Muscle weakness Sinking nosebridge
Painful nerves Clawing/contractures of fingers & nose
Prevalence Rate
Metro Manila, the prevalence rate ranged from 0.40 – 3.01 per one thousand population.
MANAGEMENT:
Dapsone, Lamprene
clofazimine and rifampin
Multi-Drug-Therapy (MDT)

six month course of tablets for the milder form of leprosy and two years for the more severe form
X – Vector Borne Communicable Disease
I – LEPTOSPIROSIS
an infectious disease that affects humans and animals, is considered the most common zoonosis in the world
Causative Agent: Leptospira interrogans
S/S:
-high fever -severe headache
-chills -muscle aches
-vomiting -may include jaundice (yellow skin and eyes)
-red eyes -abdominal pain
-diarrhea
TREATMENT:
PET - > Penicillins , Erythromycin, Tetracycline
II – MALARIA
Malaria (from Medieval Italian: mala aria – “bad air”; formerly called ague or marsh fever) is an infectious disease that is widespread in many tropical and subtropical regions.
Causative Agent: Anopheles female mosquito
Signs & Symptoms:
Chills to convulsion
Hepatomegaly
Anemia
Sweats profusely
Elevated temperature
Treatment: Chemoprophylaxis – chloroquine taken at weekly interval, starting from 1-2 weeks before entering the endemic area.
Preventive Measures: (CLEAN)
Chemically treated mosquito nets

Larvae eating fish
Environmental clean up
Anti mosquito soap/lotion
Neem trees/eucalyptus tree
III – FILIARIASIS
name for a group of tropical diseases caused by various thread-like parasitic round worms (nematodes) and their larvae
larvae transmit the disease to humans through a mosquito bite
can progress to include gross enlargement of the limbs and genitalia in a condition called elephantiasis
S/S:
Asymptomatic Stage
Characterized by the presence of microfilariae in the peripheral blood
No clinical signs and symptoms of the disease
Some remain asymptomatic for years and in some instances for life
Acute Stage
Lymphadenitis (inflammation of lymph nodes)
Lymphangitis (inflammation of lymph vessels)
In some cases the male genitalia is affected leading to orchitis (redness, painful and tender scrotum)
Chronic Stage
Hydrocoele (swelling of the scrotum)
Lyphedema (temporary swelling of the upper and lower extremities
Elephantiasis (enlargement and thickening of the skin of the lower and / or upper extremities, scrotum, breast)
MANAGEMENT:
Diethylcarbamazine
Ivermectin,
Albendazolethe
No treatment can reverse elephantiasis

VI – SCHISTOSOMIASIS
parasitic disease caused by a larvae
Causative Agent: Schistosoma intercalatum, Schistosoma japonicum, Schistosoma mansoni
Signs & Symptoms: (BALLIPS)
Bulging abdomen
Abdominal pain
Loose bowel movement
Low grade fever
Inflammation of liver & spleen
Pallor
Seizure
Treatment: Diethylcarbamazepine citrate (DEC) or Hetrazan (drug of choice)
VII – DENGUE
DENGUE is a mosquito-borne infection which in recent years has become a major international public health concern..
It is found in tropical and sub-tropical regions around the world, predominantly in urban and semi-urban areas.
S/S: (VLINOSPARD)
Vomiting
Low platelet
Nausea
Onset of fever
Severe headache
Pain of the muscle and joint
Abdominal pain
Rashes
Diarhhea
TREATMENT:
The mainstay of treatment is supportive therapy.
- intravenous fluids

- A platelet transfusion
Millenium Goals
Posted: September 17, 2011 in CHN
0
Goal 1. Eradicate extreme poverty and hunger
Target 1. Halve, between 1990 and 2015, the proportion of people whose income is less than one dollar a day
o Poorest quintile’s share in national income or consumption, per cent (WB)
o Population below $1 (PPP) per day consumption, percentage
o Population below national poverty line, rural, percentage
o Population below national poverty line, total, percentage
o Population below national poverty line, urban, percentage
o Poverty gap ratio
o Purchasing power parities (PPP) conversion factor, local currency unit to international dollar
Target 2. Halve, between 1990 and 2015, the proportion of people who suffer from Hunger
o Children under 5 moderately or severely underweight, percentage
o Children under 5 severely underweight, percentage
o Population undernourished, number of people
o Population undernourished, percentage
Goal 2. Achieve universal primary education
Target 3. Ensure that, by 2015, children everywhere, boys and girls alike, will be able to complete a full course of primary schooling
o Literacy rates of 15-24 years old, both sexes, percentage
o Literacy rates of 15-24 years old, men, percentage
o Literacy rates of 15-24 years old, women, percentage
o Net enrolment ratio in primary education, both sexes
o Net enrolment ratio in primary education, boys
o Net enrolment ratio in primary education, girls
o Percentage of pupils starting grade 1 reaching grade 5, both sexes
http://www.indexmundi.com/philippines/literacy-rates-of-15-24-years-old,-both-sexes,-percentage.html
http://www.indexmundi.com/philippines/population-below-national-poverty-line,-urban,-percentage.html
http://www.indexmundi.com/philippines/population-below-national-poverty-line,-total,-percentage.html

o Percentage of pupils starting grade 1 reaching grade 5, boys
o Percentage of pupils starting grade 1 reaching grade 5, girls
o Primary completion rate, both sexes
o Primary completion rate, boys
o Primary completion rate, girls
Goal 3. Promote gender equality and empower women
Target 4. Eliminate gender disparity in primary and secondary education, preferably by 2005, and to all levels of education no later than 2015
o Gender Parity Index in primary level enrolment
o Gender Parity Index in secondary level enrolment
o Gender Parity Index in tertiary level enrolment
o Seats held by men in national parliament
o Seats held by women in national parliament
o Seats held by women in national parliament, percentage
o Share of women in wage employment in the non-agricultural sector
o Total number of seats in national parliament
o Women to men parity index, as ratio of literacy rates, 15-24 years old
Goal 4. Reduce child mortality
Target 5. Reduce by two thirds, between 1990 and 2015, the under-five mortality rate
o Children 1 year old immunized against measles, percentage
o Children under five mortality rate per 1,000 live births
o Infant mortality rate (0-1 year) per 1,000 live births
Goal 5. Improve maternal health
Target 6. Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio
o Births attended by skilled health personnel, percentage
o Maternal mortality ratio per 100,000 live births
Goal 6. Combat HIV/AIDS, malaria and other diseases
Target 7. Have halted by 2015 and begun to reverse the spread of HIV/AIDS
o AIDS deaths

o Condom use to overall contraceptive use among currently married women 15-49 years old, percentage
o Contraceptive use among currently married women 15-49 years old, any method, percentage
o Contraceptive use among currently married women 15-49 years old, condom, percentage
o Contraceptive use among currently married women 15-49 years old, modern methods, percentage
o Men 15-24 years old, who know that a person can protect himself from HIV infection by consistent condom use, percentage
o People living with HIV, 15-49 years old, percentage
o Ratio of school attendance rate of orphans to school attendance rate of non orphans
o Women 15-24 years old, who know that a healthy-looking person can transmit HIV, percentage
o Women 15-24 years old, who know that a person can protect himself from HIV infection by consistent condom use, percentage
Target 8. Have halted by 2015 and begun to reverse the incidence of malaria and other major diseases
o Tuberculosis death rate per 100,000 population
o Tuberculosis detection rate under DOTS, percentage
o Tuberculosis prevalence rate per 100,000 population
o Tuberculosis treatment success rate under DOTS, percentage
Goal 7. Ensure environmental sustainability
Target 9. Integrate the principles of sustainable development into country policies and programmes and reverse the loss of environmental resources
o Carbon dioxide emissions (CO2), metric tons of CO2 per capita (CDIAC)
o Carbon dioxide emissions (CO2), thousand metric tons of CO2 (CDIAC)
o Consumption of all Ozone-Depleting Substances in ODP metric tons
o Consumption of ozone-depleting CFCs in ODP metric tons
o Energy use (Kg oil equivalent) per $1,000 (PPP) GDP
o Land area covered by forest, percentage
o Protected area to total surface area, percentage

o Protected areas, sq. km.
Target 10. Halve by 2015 the proportion of people without sustainable access to safe drinking water
o Proportion of the population using improved drinking water sources, rural
o Proportion of the population using improved drinking water sources, total
o Proportion of the population using improved drinking water sources, urban
o Proportion of the population using improved sanitation facilities, rural
o Proportion of the population using improved sanitation facilities, total
o Proportion of the population using improved sanitation facilities, urban
Target 11. By 2020 to have achieved a significant improvement in the lives of at least 100 million slum dwellers
o Slum population as percentage of urban, percentage
o Slum population in urban areas
Goal 8. Develop a global partnership for development
Target 15. Deal comprehensively with the debt problems of developing countries through national and international measures in order to make debt sustainable in the long term
o Debt service as percentage of exports of goods and services and net income from abroad
Target 16. In cooperation with developing countries, develop and implement strategies for decent and productive work for youth
o Ratio of youth unemployment rate to adult unemployment rate, both sexes
o Ratio of youth unemployment rate to adult unemployment rate, men
o Ratio of youth unemployment rate to adult unemployment rate, women
o Share of youth unemployed to total unemployed, both sexes
o Share of youth unemployed to total unemployed, men
o Share of youth unemployed to total unemployed, women
o Share of youth unemployed to youth population, both sexes
o Share of youth unemployed to youth population, men
o Share of youth unemployed to youth population, women
o Youth unemployment rate, aged 15-24, both sexes
http://www.indexmundi.com/philippines/share-of-youth-unemployed-to-youth-population,-both-sexes.html

o Youth unemployment rate, aged 15-24, men
o Youth unemployment rate, aged 15-24, women
Target 18. In cooperation with the private sector, make available the benefits of new technologies, especially information and communications
o Internet users
o Internet users per 100 population
o Personal computers
o Personal computers per 100 population
o Telephone lines and cellular subscribers
o Telephone lines and cellular subscribers per 100 population
Components of a Community Health Care: Components of A Community
Posted: September 17, 2011 in CHN
0
1. The CORERepresents the people that make up the community included in the community CORE are the demographic of the population as well as the values, beliefs and history of the people.
2. Eights (8) subsystems of the communitya.Housing – what type of housing facilities are there in the community, are there enough housing facilities available; are there housing laws/regulations governing the people? What are these?
b. Education – these include laws, regulations, facilities, activities affecting education, ratio of health educators to learners, distribution of educational facilities, who utilizes these, what informal educational facilities and activities exist in the community.
c. Fire and Safety – fire protection facilities and fire prevention activities, distribution of these.
d.Politics and government – political structures present in the community, decision-making process/pattern leadership style observed, etc.
e. Health – health facilities and activities: distribution, utilization, ratio of providers to clientele served; priorities in health, programs developed, etc…
f. Communication – systems, types of communication existing, forms of communication, be it formal or informal; etc..
g. Economics – occupation, types of economic activities, income, etc…
h. Recreation – recreational activities/facilities: types, consumers, appropriateness to consumers, etc…
ELEMENTS OF A HEALTH COMMUNITY1. People are partners in health care

2. People work together to attain goals.3. Physical environment promotes health, safety, order and cleanliness.4. Safe water and nutritious food.5. Families provide members with basic needs.6. Available, affordable health care.
A HEALTH COMMUNITY…
1. … prompts its members to have a high degree of awareness that “we are community”2. … uses its natural resources while taking steps to conserve them for future generations.3. … openly recognizes the existence of sub-groups and welcomes their participation in community affairs.4. … is prepared to meet crises.5. … is a problem-solving community; it identifies, analyzes & organizes organizes to meet its own needs.6. … has open channels of communication that allows information to flow among all subgroups of its citizens in all directions7. … seeks to make each of its system’s resources available to all members of the community.8. … has legitimate and effective ways to settle disputes and meet needs that arise within the community.9. … encourages maximum citizen participation in decision-making.10. … promotes a high level wellness among all its members.
CHN Complete
Posted: September 17, 2011 in CHN
0
Community Health Nursing
CHW – group of people with common chrematistics or interest within a territory or geographical boundary
Community
1. Patient/Client
2. Setting - outside curative institutions
home – family HNSg
school – SHSg
places of work – occupational HNSg
World Views:
1. Community integral part of society compose of families
Eg. – poor community
under nutrition

poor food supply
level of knowledge – poor
o intrapersonal conflict – choosing what to wear
o intrapersonal family
o intrapersonal community (interfamilial) regionalism – parochial
o intra sociedad (inter societal)
2. Conflicts/contradiction – always present in the community
Note: Should be positive in dealing with conflict.
3. Condition in the family is always changing
Health
1. Wellness – Illness continuum
Optimum – internal ————- death
Wellness - external
External
Macro system
political
economic
socio cultural – education, customs, beliefs, practices, tradition, mass media
o maintain continuum balance and purpose direction with environment
o progress toward a high level of FXU, lice to the fullest potential
o Epidemiologic model
2. High Level Wellness
3. Agent Host Environmental Model
Agent (Etiologic Facts)
1. Infections/biological factor
2. Mechanical
3. Physical
4. Carcinogenetics – pringels, tobleron (GMO’s – chemical
5. Poison – eg. MSG

6. Allergies
7. Nutritive elements
8. Psychological
Host – intrinsic factor – age, sex
exposure
response – susceptibility
- resistance
environment – extrinsic factor
4. Health Belief Model
relationship bet a person’s belief and his behavior in health
3 components
1. Susceptibility to illness
2. Seriousness of an illness
3. Benefits taking the action
AN/AIDS
Common in
1. Commercial Sex Worker – unprotactive penetrated sex
2. Sea farers
3. Religious Nums
Vaginal – male and female 1:000
Oral – male to male also common in male to female 1:200
Felacio – mouth to penis
Oral – cumaningus – mount to vagina
Aningus – mouth to amus
Preventive :
1. abstinence – sex (safe)
2. Be Faithful – Mutual/Monogamy
3. Correct continous consistent use of condom
4. Do no penetrate

5. Evolutionary Based Model
illness and death sometimes serves an evolutionary function
Elements:
life events
life style determinants
control perception
viability emotions
health out comes
o client’s won being
o health is not merely the absence of DSE illness of infirmity
o state of complete physical mental, and social wen being
6. Health Promotion Model
7. WHO – Definition 1978 – Alma Ata
Health
1. Social phenomenon – Health outcome is interplay of different societal factors
outcome with interplay of different factors and society:
biological
physical
ecologic multiple causation Theory
political (Holistic)
economic
socio-cultural
Community Health
Part of medical paramedical intrapersonal which is concerned and the heath of the whole population.
Major Concept
1-health promotion & DSE prevention
2- people participation
Individual Applied Community
Client Study As Client

- Anatomy - structure - demography
- Physio - functions - Sociology
- Patho - malfunction - epidemiology
Public Health & Longetirity (CBQ)
WINSLOW – contribution to the most effective total development and life on the
Individual and the society.
HANLON – priority the survival of the species the prevention of condition which
lead to the structure destruction or retardation of human function and
potential in early year of life.
Communication Health Nursing
- special field of nursing that combines the skills of nursing public health, and some phases of social assistance and FXUS as part of the total health project and promotion of health.
JACOBSON – is a learned practice discipline with the ultimate goal of contributing as individual and in collaboration with others, promotions of clients’ optimum level of fractioning through teaching and delivery care.
Jacobson Major Roles
1. Health Educator
2. Provider of Nursing Care
FREEMAN – aimed developing and enhancing health capability of people,
Individual, families and communities.
Community
People Organization (PO)
Agency
1. Ngo
2. GO – DOH – National – Regional – Province – Municipal – BHW
RA – 7305 – Magna Corta of PHWorker
RA – 7160 – Local Government Code
Devolution of Health Services
CHN CONCEPTS:
1. 10 Focus on CHN is an heath promotion

2. CHN practice is extended to benefit not only individual but whole & family
3. CHN are generalist in terms of their practice throughout life’s continuum – its full range of Health problems and need.
4. Contact with client may continue over a long period of time which includes all ages and types of HC
Levels
Primary HC – community
20 HC – Regimal, Provincial, Municipal & District
Tertiary – sophisticated medical center
Assessment:
Community Dx
health problems and needs
sources of solve to problem
Principle of Community Health Nursing
1. Recognize needs of individual
2. Knowledge and understanding of agency and policies facilitates goal achievement
3. The family is the unit of service
Planning
1. Prioritization
2. Goal setting
3. Objectives
4. Actions/Intervention
5. Evaluation out come:
- criteria
- standard
Health Education and Counseling
common goal – behavior change or modification
Basic Different
Health Education – dive advice
Counseling – provide all option

Implementation:
Community – family focus of /unit of care
4. Respect values, customs and beliefs of clients – as nurse we should not be judgmental
5. Health education and counseling are vital parts of CHN
6. Collaborative working relationship with the health team facilitates goals achievement.
7. Continuing staff education ensures quality client care and upgrade nursing practice.
8. Indigenous and communication resources
appropriate tech – methods and tech both scientifically sound and socially
and acceptable
9. Individual families and communities must actively participate in decision making
10. Supervising of nursing services be qualified personnel provides guidance and direction to work.
11. Accurate recording and reporting serve as bases for evaluation and guide for future actions.
12. Periodic and continuing education
board quest
how would you evaluate – objective – if both present answer this
criteria
HEALTH SITUATION
1. Health Indices
A. Basic Indicators Anemia
1. Nutrition 48% of Filipinos
2. DSE Pattern 58% of pregnant women
- morbidity
- mortality
infant mortality rate according to DOH – 18.7
life expectancy: Female 69.2
Male 63.7
HEALTH PROMOTION
Consist of activities directed towards increasing the fever of well being and actualizing the health potential of individuals families communication and societies.

Different with prevention
not desl dysixy or health problem financial
“approach “ behavior not
avoidance behavior
seeks to expand (+) potential for health
Multidimensional Nature of Health Promotion
1. Individual – lifestyle
- personal habits & practices affecting health
-lifestyle
- lifestyle responsibility
2. Family – health behavior and belief
3. Community – norms
4. Environment – harmony and bal bet human and surroundings
5. Society – basic human needs
HEALTH PROMOTION METHODS
health education
Good standard nutrition adjusted to development phases of life
Attention to personality development
Provision of adequate housing
Recreation and agreeable working condition
Genetics counseling
Periodic selective examination – self breast examination (SBE)
SCREENING METHOD
Presumptive identification of unorganized dse or defect by the application of test, examination or other procedures that can be applied rapidly and inexpensively population.
mass screening
case finding
contact tracing

multi phasic screening eg HIV antibody testing
surveillance
RA 7305 – Jon reporting of communicable dse
Tertiary Prevention
methods
Dx
Tx
Mx
Rehabilitation
Community Organizing
Awareness raising
Organizing
Mobilizing / responsible action
Key Concepts and Principles
1. Objective analysis of objective condition – scientific
2. Basic trust among people
3. By the people from the people, for the people
4. People want and can change
5. Self-willed changes will have move meaning and performance than imposed changes.
Primary Health Care
- Essential care based on scientifically – sound and socially acceptable methods and technology made universally available to individuals families and communities at the cost they can afford at any given stage development than their full participation towards self-reliance and self determination.
8 Primary Health Care
1. Health Education
2. Food Supply and Nutrition
3. Immunization
4. Hw and Basic Sanitation
5. Prevent & control of common dse
6. Tx of endemic dse
7. MCH including FP
Individual
1. Assessment
a. Data collection
2 types data – subject & objective
2 methods – interview & observation
4 Instruments
1. Nursing History (subjective)
2. Physical Examination
3. Laboratory Exam
4. Process Recording
b. Data Analysis
2. Nsg. Dx
Health Care V/E Etiology
3. Planning
a. Prioritization
b. Goal
c. Objective
d. Nsg. Intervention
e. Evaluation Outcomes - Criteria , standard
4. Implementation
- health educator
- provider of HC
- supervisor Client /Patient Advocate
- researcher
- health organizer
- CH, Monitor
8 Basic Tasks:

1. Physical Maintenance
2. Allocation of Resources
3. Division of Labor
4. Socialization of Family Members
5. Reproduction, recruitment and releases
6. Maintenance of order
7. Placement of members in larger society – production of good member
8. Maintenance of motivation and morale
Nuclear Family – Mother, Father, son & daughter
Extended – grandparent relation or daughter in law.
First Level Assessment
Health Threats
Health Deficits
Forcible Crisis/Stresspoints
Family Tasks
1. Ability to recognize the presence of the problem
2. Ability to make decisions.
3. Ability to perform nursing care to sick
4. Ability to provide home environment
5. Ability to utilize community resources
Incubation Pd- entry of Pathogen to appearance of 1st SK
IMMUNITY
Passive – quick to come/to go active – slow to come / to go
1. natural – utero, breast feeding 1. Natural – getting the dse
2. Artificial – sevum prob. Antitoxin 2. Artificial – utanus toxoid
Pregnant
TT1 – 4th month
TT2 – 8th month
Pregnancy 2

TT3 – booster 1st
Pregnancy 3
TT4 – booster 2nd
Pregnancy 4
TT5 – booster – lifelong immunization
Community Mental Health Nursing
1. A unique process which includes an integration of concepts from nursing mental health, social psychology community network.
Occupational Health Nursing
- Application of Nursing principles and procedure conserving health of the healthworkers.
School Health Nursing
Components
1. School Health Services
2. Health Instruction
a. direct – nurse doing the school teaching
b. indirect
3. Health School Living
4. School – Community Linkage
Median age of Filipinos is 20 yrs old
50 % – 20 years old
50% – above 20 years old
Vital Statistics – application of statiscal measure to vital events fertility , mortality, morbidity
RA 3753 – Civil Registry Law
Requires the registration of births and deaths to local registrars
RA 3573 – Law on reporting notifiable disease
Family Planning Program
Goal Improve material & child through:
proper timing of pregnancy
proper spacing of pregnancy

number of pregnancies
Pregnancy :
Ideal age: 30-30- yrs.
20 -18 - 30 – 35 with risk
18 – 35 – high risk
Ideal interval – 3 years
2 years – with risk
4 years – high risk
ideal No – 3
4 – with risk
4 – risk
COMMUNICABLE DISEASE NURSING COMMUNICABLE DISEASE
Posted: September 17, 2011 in CHN
0
Infectious Agent or its toxic products – AGENTDirectly or Indirectly – MODE OF TRANSMISSIONPerson, Animal or Intermediate Vector – HOSTEnvironment – ENVIRONMENTECOLOGIC TRIAD OF DISEASEAgent – element, substance, animate or inanimate that may serve as stimulus to initiate a disease processHost – organism that provides nourishment for another organismEnvironment – physical (climate), biological (plants & animals)CONTAGIOUS VS. INFECTIOUSContagiousDiseases that are easily spread directly transmitted from person to person (direct contact) through an intermediary hostInfectiousDiseases that caused by a pathogen not transmitted by ordinary contact but require a direct inoculation through a break in the skin or mucous membrane.NOTE: ALL CONTAGIOUS DISEASE ARE INFECTIOUS BUT INFECTIOUS DISEASE IS NOT ALWAYS CONTAGIOUS
What is Infection?INFECTION – “the state or condition in which the body or part of the body is invaded by a pathogenic agent ( bacteria, virus, parasites etc.) which under favorable conditions multiplies and produces effects which are injurious…”
Infectious AgentA. RESIDENT ORGANISMSdeeply seated in the epidermis, not easily removed by simple handwashing,Ex: Staphylococci
B. TRANSIENT ORGANISMrepresent recent contamination,survive for a limited period of time, acquired during contact with the infected colonized patient or environment,easily removed by good handwashing
Ex: ( Klebsiella & Pseudomonas)
Infectious AgentBacteria – heama organism, systemicVirus – nuero organism, systemicFungi – skin organism, localProtozoa – GI organism, localInfectious Agent
FACTORS THAT AFFECTS THE AGENT TO DEVELOP A DISEASEPathogenicity – ability to cause a diseaseInfective dose – no of organism to initiate infectionVirulence – ability to enter or move through tissuesSpecificity – ability of the organism to develop antigens
STAGES OF INFECTIOUS PROCESSMeans of Transmission1. CONTACT – most common means of transmitting microorganisms from one person to another.A. Direct Contact (person to person)occurs when one person touches anotherbest vehicle is the Hands especially those of the Health Care workersB. Indirect Contact (inanimate object)- occurs when a person touches an inanimate object contaminated by an infected patient2. AIRBORNE- droplet, dust, organisms in env.3. VECTOR – insects or animals4. VEHICLE- food (salmonella), water (shigellosis), blood (Hepa B), medication ( contaminated infusion)
PREVENTION OF COMMUNICABLE DISEASEHealth Education – primary role of the nurse

Specific Protection- handwashing, use of protective devicesEnvironmental Sanitation – clean and conducive for health
Definition of Prevention“Actions aimed at eradicating, eliminating, or minimizing the impact of disease and disability. The concept of prevention is best defined in the context of levels, traditionally called primary, secondary, and tertiary prevention”
Prevention of Needlestick InjuriesDispose Used Needles in Puncture Proof Needle ContainersDon’t Recap Needles (Unless using the One-handed Technique)Use Gloves When Handling Needles (Won’t Prevent Injuries but May Lessen Chance of Transmitting Diseases)
CONTROL OF C0MMUNICABLE DIESEASE1. Notification2. Epidemiological Investigation3. Case finding; early dx and prompt treatment4. Isolation and Quarantine5. Disinfection; disinfestation6. Medical Asepsisa. Handwashingb. Concurrent disinfectionc. Personal protective equipments (PPEs)d. Barrier Cards/Placarding
Objectives of CCDRestoration of health, reduce deaths and disabilityInterpretation of control measures to IFC for practice to prevent spread of CD.Promotion of health and prevention of spread of CD
Diseases that require weekly monitoring:1. Acute flaccid paralysis (AFP) polio2. Measles3. Severe acute diarrhea (SAD)4. Neonatal tetanus5. AIDS
Diseases that require reporting w/in 24 hrs1. Acute flaccid paralysis (AFP) polio2. Measles
Diseases targeted for eradication1. Acute flaccid paralysis polio2. Neonatal tetanus3. Measles4. Rabies

EpidemiologyStudy of the occurrence and distribution of diseases in the population
Patterns of occurrence of disease –frequency of disease occurrenceSporadicOn and off occurrence of the diseaseMost of the time it is not found in the communityOne or two cases that occur are not relatedEndemicPersistently present in the community all year roundEx: malaria in PalawanEpidemicAn unexpected increase in the number of cases of diseasePandemicEpidemic of a worldwide proportionsTime Related Patterns of Occurrencecyclical variationa periodic increase in the number of cases of a diseasea seasonal disease, an increase is expected or there is usual increase- dengue fever during rainy seasons are increased but it is not considered an epidemic because it is expected to rise at this particular timehot spot-a rising increase that may lead to an epidemic
Time Related Patterns of OccurrenceShort time fluctuationA change in the frequency of occurrence of a disease over a short period of timeMaybe (+) or (-)Secular variationA change in the frequency of occurrence of a diseae taking place over a long period of timeEx: a.) the change in the pattern of occurrence of polio after being eradicated in 2000, then sudden repport of cases in 2001 due to mutant restraints.b.) small pox virus-eradicated in 1979 (last case reported) and no another incidence as of todayTypes of EpidemiologyDescriptive Epidemiology – concerned with disease frequency & distributionAnalytic EpidemiologyIs a study of the factors affecting occurrence and distribution of the disease.Ex. Epidemiologic investigationTherapeutic/ClinicalStudy of the efficacy of a treatment of a particular diseaseEx. Clinical trial of a newly proposed therapeutic regimenEvaluation EpidemiologyStudy of the over-all effectiveness of a total/ comprehensive public health program.Ex. Evaluation of the under five clinic
Note: We make use of the epidemiology in CHN in order to come up a community diagnosis and also to determine the effectiveness of a particular treatmentTypes of Epidemiologic Data

Demographic dataDemography is the study of population groupsEx. Population size and distributionVital StatisticsEnvironmental dataHealth services dataEx. Ratio between nurse and the population being servedEx. Degree of utilization of health facility/ serviceEpidemiologic Investigation
1st step- Statement of the problem2nd step- Appraisal of facts – describing the epidemic in terms of time, place, person.3rd step- formulation of hypothesis4th step-Testing the hypothesis5th step- Conclusion and recommendation
TERMSDisinfection – pathogens but not spores are destroyed
Disinfectant – substance use on inanimate objects
Concurrent disinfection – ongoing practices in the care of the patient to limit or control the spread of microorganisms.
Terminal disinfection – practices to remove pathogens from the patient’s environment after his illness is no longer communicable
FACTORS AFFECTING ISOLATIONMode of TransmissionSourceStatus of the client’s defense mechanismAbility of client to implement precautionsISOLATIONEPILaunched by DOH in cooperation with WHO and UNICEF last July 1976Objective – reduce morbidity and mortality among infants and children caused by the six childhood immunizable diseasesPD No. 996 (Sept. 16, 1076) – “ Providing for compulsary basic immunization for infants and children below 8 y/oPP No. 6 (April 3, 1996) – “ Implementing a United Nations goal on Universal Child Immunization by 1990”RA 7846 (Dec. 30, 1994) – immunization hepa BPD No. 4 (July 29, 1998) – “Declaring the period of September 16 to October 14, 1998 as Ligtas Tigdas Month and launching the Phil Measles Elimination Campaign”
Legislation, Laws affecting EPI

Proclamation No. 46 – “polio eradication project”Proclamation No. 1064 – AFP surveillanceProclamation No. 1066 – National Neonatal Tetanus Elimination Campaign
EPIBCG – TBDPT – Diptheria, Pertussis, TetanuOPV – PoliomyletisHepatitis BMeaslesImmunizationContraindications-conditions that require hospitalizationFor DPT 2 and 3 – history of seizures/ convulsions within 3 days after the first immunization with DPTNursing responsibility: ask how the child reacts to the first doseFor infant BCG – clinical AIDSThe following conditions are NOT contraindications:Fever up to 38.5 ºCSimple or mild acute respiratory infectionSimple diarrhea without dehydrationMalnutrition (it is indication for immunization)
Schedule of immunizationInfant BCG0 to 11 months or 0 to 1 yearat birth0.05 ml (dose) – ID, right armSchool entrance BCGWhen the child enters Grade 1 with or without scar on the right arm then still go on with the vaccination except if he is repeating Grade 1
Schedule of immunizationDPT3 doses, 4 weeks or 1 month intervalTarget age: 1 ½ to 11 months but child is eligible up to 6 yearsIf 7 years old and above DT only not P0.5 ml, IM, vastus lateralis
Schedule of immunizationOPV3 doses, 4 weeks/1 monthTarget population: same as above, eligibility until Grade 62-3 drops, oral route*Feb 8-March 8: Oplan Polio Revival DriveNo side effect, but advise the mother to avoid feeding the child for 30 minutes after the vaccine, if vomits within the 30 minute period, repeat the vaccination

Schedule of immunizationHepa B3 doses, 4 weeksCan be given at birthTarget age 1 ½ to 11 months0.5 ml, IM, vastus lateralisPatient may experience local tendernessSchedule of immunizationMeasles9 to 11 monthsMost babies have protection because of maternal antibodies thus this vaccine is given at 9 months because the time where the maternal antibodies wear off, other virus if it still active it will kill the vaccine0.5 ml, subcutaneous, any armMeaslesFever and measles rash lasting for 1 to 3 days within 2 weeks after immunization (modified measles)
ImmunizationFully Immunized Child – when he received all the antigens that should be given in the first year of life (1 dose BCG, MV; 3 doses DPT, OPV, HB)Completely Immunized Child – All vaccines given but went beyond 0ne year of age
CHN 1
Posted: September 17, 2011 in CHN
0
History
Act No. 157- Creation of Board of Health of the Philippine (BON)
Act No. 1407- Abolish BOH to DILG
1919 Mrs. Carmen Del Rosario – 1st Filipino Nurse Supervisor
1990-1992 – Local Revolutionary Code of 1991, RA 7160 Revolution Code National to local
Definition
Health – (WHO) state of complete physical, mental and social well being, not merely the absence of disease or infirmity
Public health – (Dr. C.E. Winslow) the science and art of preventing disease, prolonging life, promoting health and efficiency through organized community effeort.
Community Health Nursing (Jacobson)- is a learned practice discipline with the ultimate goal of contributing as individual and in collaboration with others to the promotion of clients optimum level of function through teaching and delivery of care.
Factors affecting Optimum Level of Function (OLOF)

1. 1. Political
2. 2. Behavioral
3. 3. hereditary
4. 4. Health Care Delivery System
5. 5. Environmental Influences
6. 6. Socio economic Influences
Concepts
1. 1. The primary focus of community health nursing practice is on health promotion.
2. 2. Community health nurses are generalist in term of their practice through life but the whole community.
3. 3. Community health nurses are generalist in terms of their practice through life continuity in its full range of health problems and needs.
4. 4. The nature of CHN practice requires that current knowledge derived from the biological, social science, ecology, clinical nursing and community health organizations be utilized
5. 5. Contact with the client and or family may continue over a long period of time which includes all ages and all types of health care.
6. 6. The dynamic process of assessing, planning, implementing and intervening provide measurements of progress, evaluation and a continuum of the cycle until the termination of nursing is implicit in the practice of community health nursing.
Principles
1. 1. CHN is based on recognized needs of communities, families, groups and individuals.
2. 2. The community health nurse must understand fully the objectives and policies of the agency she represents.
3. 3. In CHN, the family is the Unit of services.
4. 4. CHN must be available to all regardless of race, creed and socioeconomic status
5. 5. Health teaching is a primary responsibility of the CHN.
6. 6. The community health nurse works as a member of the health team.
7. 7. There must be a provision for period’s evaluation of community health team.
8. 8. Opportunities for continuation staff education programs nurses must be provided by the CHN agency. The community health nurse also has a responsibility for his/her own professional growth.
9. 9. The community health nurse makes use of available community health resources.

10. 10. The community health nurse utilizes the already existing active organized groups in the community.
11. 11. There must be provision for educative supervision CHN
12. 12. There should be accurate recording and reporting in CHN.
Public Health Nurse
1. 1. Planner/programmer
2. 2. Provide of Nursing Care/Caregiver
3. 3. Manager/Supervisor
4. 4. Community Organizer
5. 5. Coordinator of Service
6. 6. Trainer/ Health Educator/ Counselor
7. 7. Health monitor
8. 8. Role Model
9. 9. Change Agent
10. 10. Recorder/ Reporter/ Statistician
11. 11. Researcher
Community Health Process
Assessment
Collection of data, collected from family, groups and community.
Examples: Demographic Data
Vital Health Statistics
Community Dynamics
Health Status
Education
Methods: Community Survey
Interview
Statistics
Epidemiological studies
Common indicators of health status

Ø Morbidity
Ø Mortality
Categories of Health Problems
Ø Health Deficit (HD)
Ø Health Treat (HT)
Ø Foreseeable Crisis (FC)
Ex: Active TB- HD
45 yr, old male smoke- HT
Sedimentary health style- Ht
Early pregnancy- FC
Father of family losses his job FC
Death in the family- FC
Patient is sick due to pneumonia- HD
Children who are not immunized- HT
Lack of prenatal check – up- HT
Eclampsia- HD
Working hazard- HT
Hypertensive- HD
With measles “child”- HD
Family members has liprosy (microbactria liporea)- HD
Marriage- FC
Community diagnosis
1. A. Physical Characteristics
2. B. Population Characteristics
3. C. Environmental factors
4. D. Knowledge, attitude, practices of the people
5. E. Community resources and facilities
Planning: Based on the actual and potential problems that were identified and prioritized
Goal: Declaration of purpose or intent, gives essential direction to action

Specific objectives: Made in terms of activities of daily living
Implementation:
Ø Carries out nursing procedures which are consistent with nursing with nursing care plans.
Ø Involve the patient with his/her family
Ø Utilized support system
Evaluation
Frame works
1. a. Structural elements
2. b. Process elements
3. c. Outcome elements
Nursing Procedures
Clinic Visit
1. 1. Pre-consultation conference
2. 2. Medical examination
3. 3. Nursing intervention
4. 4. Post consultation conference
Home Visit- face to face contact with the client
Principles
1. 1. A home visit should have a purpose or objective
2. 2. Planning for a home visit should use every available information about the family, and individual
3. 3. Planning should revolve around the essential needs of the individual
4. 4. Planning of a continuing care involve the individual or family
5. 5. Planning should be flexible and practical
Bag technique- Tool
Public health bag- is an indispensable equipment of the public health nurse
Principles
1. 1. Prevent the spread of infection
2. 2. Save time and effort

3. 3. should not shadow the concern for the patient
4. 4. Can be performer in a variety of ways
Zippiram solution- disinfectant


















