![[XLS]reports.mca.gov.inreports.mca.gov.in/Reports/MasterDataExcels/company... · Web view3800000 3800000 700000 530340 100000 100000 5000000 1200000 600000 509600 30000000 9377400](https://static.fdocuments.in/doc/165x107/5ad0382a7f8b9a71028d9ead/xls-view3800000-3800000-700000-530340-100000-100000-5000000-1200000-600000-509600.jpg)
CHLORID kidney conceivable, might complicated...
54
A STUDY OF THE ACTION OF AMMONIUM CHLORID AND ORGANIC MERCURY COMPOUNDS BY NORMAN M. KEITH mm MARY WH-ELAN (From the Division of Medicine, Mayo Clinic) (Received for publication May 29, 1926) The elimination of urine from the body is not the function of the kidney alone: the blood and the tissues are profoundly concerned. The blood may be considered the connecting link between the other two. The concentration in the blood of those substances which eventually appear in the urine must fluctuate with variations in the chemical state of either the tissues or the kidney or both. It is conceivable, therefore, that an absolutely, or apparently, identical chemical disturbance of the blood might result from either chemical changes in the tissues or disturbance of the excretory function of the kidneys. The general problem of the site of initiation of disease characterized by retention of urinary elements is thus complicated by the possibility that fundamentally different diseases may present the same superficial appearance. The problem became still more intricate with the demonstration that retention of urea does not parallel retention of salt and water. Edema may be accompanied by normal excretion of urea, and nor- mal urea content in the blood; urea may be retained without edema and even without serious anatomic changes in the kidneys; salt may be retained without edema being demonstrable. The effect of diuretics is similarly difficult to explain. Diuresis can be produced by those which are known to increase blood-flow and by those which cannot be shown to have any such primary effect. It is impossible, therefore, to explain diuresis in every instance on the same hypothesis. The newer diuretics, ammonium chlorid and Fellow in Chemistry, The Mayo Foundation. 149
-
Upload
hoangduong -
Category
Documents
-
view
217 -
download
2
Transcript of CHLORID kidney conceivable, might complicated...
A STUDYOF THE ACTION OF AMMONIUMCHLORIDANDORGANICMERCURYCOMPOUNDS
BY NORMANM. KEITH mmMARYWH-ELAN(From the Division of Medicine, Mayo Clinic)
(Received for publication May 29, 1926)
The elimination of urine from the body is not the function of thekidney alone: the blood and the tissues are profoundly concerned.The blood may be considered the connecting link between the othertwo. The concentration in the blood of those substances whicheventually appear in the urine must fluctuate with variations in thechemical state of either the tissues or the kidney or both. It isconceivable, therefore, that an absolutely, or apparently, identicalchemical disturbance of the blood might result from either chemicalchanges in the tissues or disturbance of the excretory function of thekidneys. The general problem of the site of initiation of diseasecharacterized by retention of urinary elements is thus complicatedby the possibility that fundamentally different diseases may presentthe same superficial appearance.
The problem became still more intricate with the demonstrationthat retention of urea does not parallel retention of salt and water.Edema may be accompanied by normal excretion of urea, and nor-mal urea content in the blood; urea may be retained without edemaand even without serious anatomic changes in the kidneys; salt maybe retained without edema being demonstrable.
The effect of diuretics is similarly difficult to explain. Diuresiscan be produced by those which are known to increase blood-flowand by those which cannot be shown to have any such primary effect.It is impossible, therefore, to explain diuresis in every instance on thesame hypothesis. The newer diuretics, ammonium chlorid and
Fellow in Chemistry, The Mayo Foundation.149
ACTION OF AMMONIUMCHLORID
novasurol,2 have been thought to act in a purely chemical way, byaffecting the threshold of excretable bodies in the blood, and the acid-base equilibrium in the blood and tissues. Study of the chemicalstate of the blood cannot be divorced from consideration of thechemical reactions in the tissues. Whether these diuretics act onthe tissues, the blood or the kidney is so important a problem thatits elucidation will probably go a long way toward settling the wholequestion of the formation of urine.
Certain of the chemical constituents of the blood, like urea, willbe excreted as soon as they appear; they have no threshold. Others,like the inorganic salts and glucose, must attain a fairly definitelevel before any escapes. This threshold varies in different indi-viduals, and in the same person at different periods, even in health;in certain diseases the threshold is profoundly altered for one ormore of them, even for those that normally have no threshold. Thisdisturbance in the threshold of urea or salts may be associated withmarked changes in the acid-base equilibrium of the blood and tissues.In acidosis the carbon dioxid combining-power of the plasma is de-creased by acid entering the blood, although the hydrogen-ion con-centration may be kept normal by the buffer system.
The effect of these newer diuretics on water retained in the inter-stices of the body is quite remarkable. Here again, if the mechanismof this action can be explained, the cause of the retention will beclear. There is some relation between the excretion of salts and theexcretion of water; edema is often associated with chemical changesin the blood. Haldane found that the ingestion of ammoniumchlorid by a normal man caused acidosis, as well as increase in urinaryexcretion, and he attributes this diuresis to the acidosis.
The object of the present study is to determine what chemicalchanges, especially in the content of salts and their ions, occurred inthe blood and urine during the reduction of ascites and edema bythe use of ammonium chlorid and novasurol, singly and in combina-tion, and to compare them with the effects produced by the samemedication in the normal.
2Novasurol and salyrgan were used in these experiments. Novasurol is adouble salt of sodium oxymercuri-o-chlorphenoxy-acetate with diethylbarbituricacid. Salyrgan is mercuric acetate-salicylallylamid-o-acetate of sodium.
150
NORMANM. KEITH AND MARYWHELAN 151
AMMONIUMCHLORID
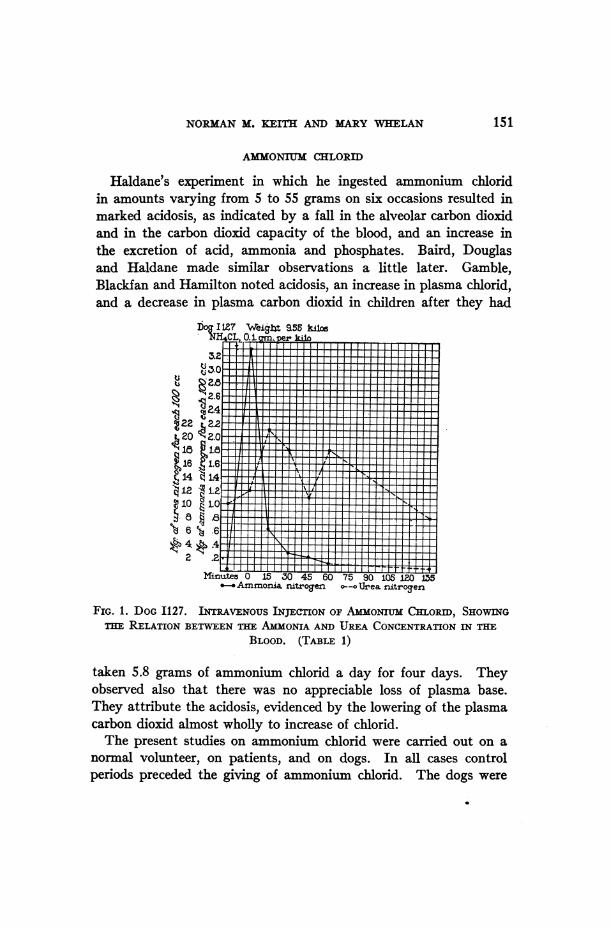
Haldane's experiment in which he ingested ammonium chloridin amounts varying from 5 to 55 grams on six occasions resulted inmarked acidosis, as indicated by a fall in the alveolar carbon dioxidand in the carbon dioxid capacity of the blood, and an increase inthe excretion of acid, ammonia and phosphates. Baird, Douglasand Haldane made similar observations a little later. Gamble,Blackfan and Hamilton noted acidosis, an increase in plasma chlorid,and a decrease in plasma carbon dioxid in children after they had
Dog I127 WeiSbt 955kilN-NH4 0L .1a,per kilo
L_1___SlL1Ll _
22 22 ---20 2.0
,14 1.4 i I '1-
10 to _A_3 - -
t4,.4 lH t ;i 0
Minu±tes 0 15 30 45 60 75 90 105 1201O5--.Ammonia. nritro9en a--. Urea nitrogen
FIG. 1. DOGI127. INTRAVENOUSINJECTION OF AmmONIUMCHLORID, SHOWINGTHE RELATION BETWEENTHE AmmONIAAND UREACONCENTRATIONIN THE
BLOOD. (TABLE 1)
taken 5.8 grams of ammonium chlorid a day for four days. Theyobserved also that there was no appreciable loss of plasma base.They attribute the acidosis, evidenced by the lowering of the plasmacarbon dioxid almost wholly to increase of chlorid.
The present studies on ammonium chlorid were carried out on anormal volunteer, on patients, and on dogs. In all cases controlperiods preceded the giving of ammonium chlorid. The dogs were
ACTION OF AMMONIUMCHLORID
iuaz lad 'satunlOA '3aMod O2uiuiqwoz'p!xo!p uoqil m
1ua3lad tuStdi ioJlqD e
1uai elad Uu 'UaOol!u 0an I-
Jutolad
-uatu luasoll!u -cluoutuwON0)
i00
152
NORMANM. KEITH AND MARYWHELAN
eq
CE)
o
N0
CE)o0Nooooeq
0
0
0
o.
o
C%
0.
CE)
N6* -
C4 c
*-4
6;
o.i doD
,-o c
IbO0
4)
'~4
0
bO
%5-4
Cd
0--
blo
V4)C.)
O
-4
0
O
.0
00
0
0
Qu
C1)4)
\0
0\
NO
.4>4-
*4)
03
00~ ~o o
O CQ
o _ _
C0
0O 0
o 0o K
°0° O
C40 00
oo0
~O O4UE)C)%OE CE E)C)CE E
°b4-0-0 0
-c~~~~~-- -~~~~~~Q% ONCI%
0 - CnC14 C1 o. . . .
O O O O
bo0
"A0u
9
I
bO0*
'-4
0
b0
C.)
5-'-4
0u
O0
-i
0
0
0
0Q
C.)
C;
u
V4)
*--
~4 ,-trN 4-'0oo
+
U)
0.
U) o
.0
_-0
U)o
4E)m- C~40 00U))
0% 0% 0000-C1 ~
4J~~~~~~~~~~~~~~~~~1U)~~~~~~~~~~~~~~~C
U)
153
ACTION OF AMMONIUMCHLORID
*tustu'Imoq qaxa uaBojl!u ealI
if)-c'-
*ttl2l limoq I') 00qoea uaRoil!u BeuoLutuV 0 00
*tu2ui 'uasoIii!u vIt'l0-
00~~
U1tUI 'UD201jTU eiUOlWuW if) %
_N O
00Hd
ZC3 'atunCIOAUf) O
C%
00 0Cjua) jad' 'sumIoA 'lamodSuTunqtuo) 'p!xoip uoqxeD
lad wBusLumoluaSao o XjoL0
s uAmsauason!u -BiuoxwwvN 0 )O O'0 ~~~~~~~~~~~~~~~~~00
0U3 0 0 d 00'OUtU'UOI~U !UWW o *o o
0) S)t S0 00 O 0) 00
;° ~ C .C0) EQe 5 bo 5 4J E
~~ q~~~ 0)~0 00 0
8u cD, U EnX fsoi,
-< c ¢° E O b,E '0
0*-iNO C-) Cd C 4
Q- --
-,
0 00o o u ) oo -o
S~~~~~~~~~~~~~- N N '. -4 U X eX
0) C CICJd)-0 -)C4
.;~04- * * Q* ~ QU * . .. .. .. ..- c- 2Q,-4 cIQ ra
U if)Oif)U)/I 1 En)0f 0 Enf.5 #)~~-4~ ~ Cf)(w Cf)
00-00%0% 0'" -41 i) i4f~~~~~~~~~~bO oo oo Cd os Cco N XX
00~000 % CMtI)
toC,)
¢4if
00
154
U)
0)
1-4
0)
0
0U)
00
U)C)
U)00
bU)
00
0)
0 .0
:3d
b iD
1U0IU)*%nU
e4-
U)
*00
'0
00
NORMANM. KEITH AND
0o 0%0% O
MARYWHELAN
0oI
Io 0 o 0 000 0000
S- I Co,)
o o00 00Uo) b b oo00
o 0 %0 0 0
C~4 00 .
1- ~ 00 000%
o 0U) I 'e$.
if) U) m U) 4
- ~~~~~00-00o 0o4
b o Io o o oo.~~~~~~~~~~~~.
bO MO bo;WO; N;
0
00 0 0
04 0 " 0
~~ ~ 4) r 4
~~*~ ~ ~ dC4 4
0 U 0 Q) 0U 00 0 0 00%0t~~0 0 000 1-ae4 0-e4 ~ ~ ' 0 00
VU)oN_1V-ole
4i
rA¢b
155
ACTION OF AMMONITUMCHLORID
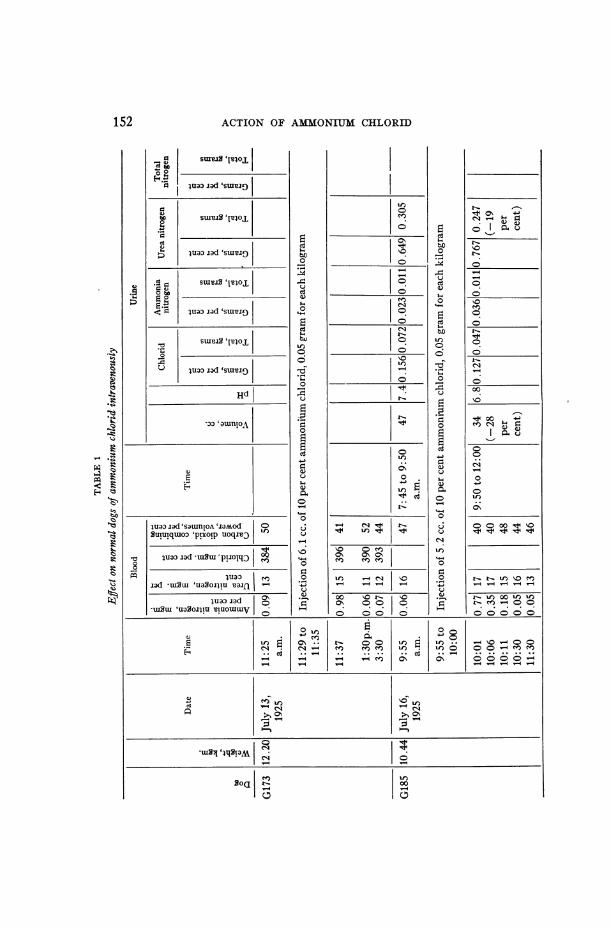
given no food during the eighteen hours preceding the experimentand until the study period was completed (usually four hours afterthe intravenous injection of 10 per cent ammonium chlorid, 0.05to 0.1 gram (for each kilogram). Human subjects were kept onweighed low-salt, low-fluid diets3 both before and during the inges-tion of ammonium chIorid. The average usual dose of ammoniumchlorid was 9 grams a day. The actual total amount ingested in onecase was 364 grams over a continuous period of forty-two days. Dur-ing both control and experimental periods studies of the blood andurine were made.
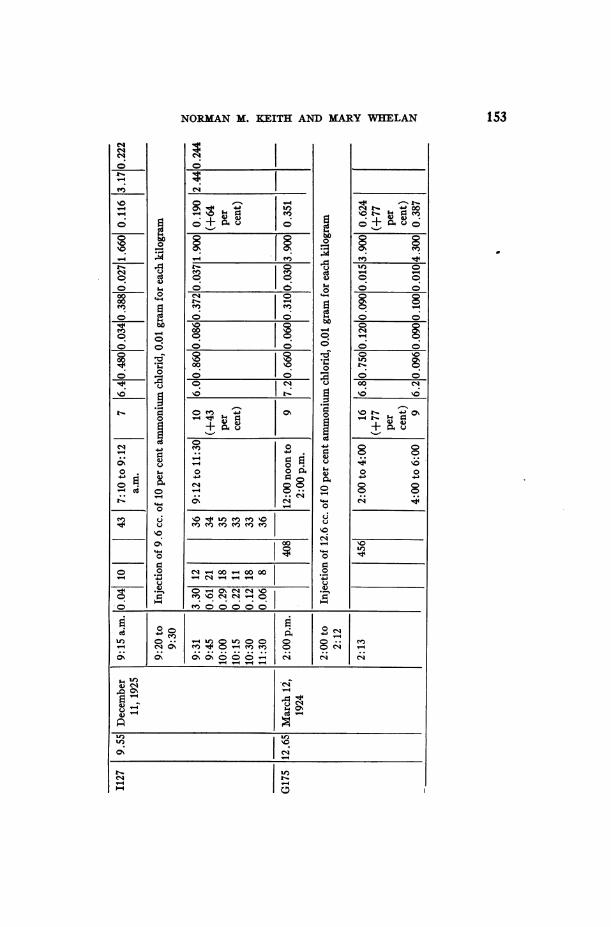
Blood. Ammonia was determined in the blood of dogs on threeoccasions, and all the findings were similar. The concentration ofammonia nitrogen in the blood rose immediately after the injection,reaching a maximum of 3.3 mgm. for each 100 cc. in two minutes,but dropped so rapidly that in fourteen minutes it was reduced to0.61 mgm. or one-fifth the maximal value. The rapid drop continuedfor from half an hour to two hours, until the concentration becamenormal. Blood-urea nitrogen did not show a marked change evenat the end of two hours in dogs G173 and G185, but with the largerinjection in dog I127 (fig. 1) it rose from 10 to 21 mgm. Plasmachlorids did not change appreciably; the carbon dioxid combining-power of the plasma showed a slight initial drop, which in some casespersisted for two hours. Urine collected at intervals of two hoursbefore and after the injection of ammonium chlorid showed an in-crease in volume in two experiments and a decrease in a third, anincrease in hydrogen-ion concentration in all, and an increase inthe concentration of chlorids in two experiments. The ammoniumnitrogen did not show any definite constant change; the urea nitro-gen concentration remained the same or increased. The latterincrease is in agreement with previous results (18, 57).
Experiments of short duration give a fair idea of the manner inwhich the injected salt is distributed in the blood. In the case ofammonium chlorid both of the injected ions leave the blood stream
3 The actual food of these diets contained approximately 800 cc. of water, andfrom 0.6 to 0.8 gram chlorid, from 0.5 to 0.7 gram sodium and from 1.6 to 1.8grams potassium. Complete details in article. "The therapeutic use of dietslow in water and mineral content" (31).
156
luaa~~~°'laod Isq aoNbum uao IO °°UWoI ) (NCO,0 IC114 | %O C1 m'mSsusuasogTusaJnl ~~00 m _- 00 Ce Noo_00 CN _
luUa3Tad¢- U2U |~in0°||
lua:) iad |0
tU90! *E g- *Q U g Mjuaalad~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
xasm| > |u |o|ou |
a2| 0 O 0 |eCa | |o. .I on .-n~n~n;-L
NORMANM. ]KEITH AND MARYWEELAN
Cd
4404J
0rn 4i 4
Cd 0 C,
ce
157
rA
I
r4l)C14
1.6,-4S-40.iv
9r.0
Lf.04i
C144.)0=1.-n
cd
o aoDLbo
*t
eI
qzK
*t
otS
U)
MSDI 00
ACTION OF AMMONIUMCHLORID
with remarkable rapidity, the chlorid so rapidly that a definite in-crease in plasma chlorids may not be detected two minutes afterinjection. The ammonia nitrogen shows an increase but becomesnormal in from half an hour to two hours.
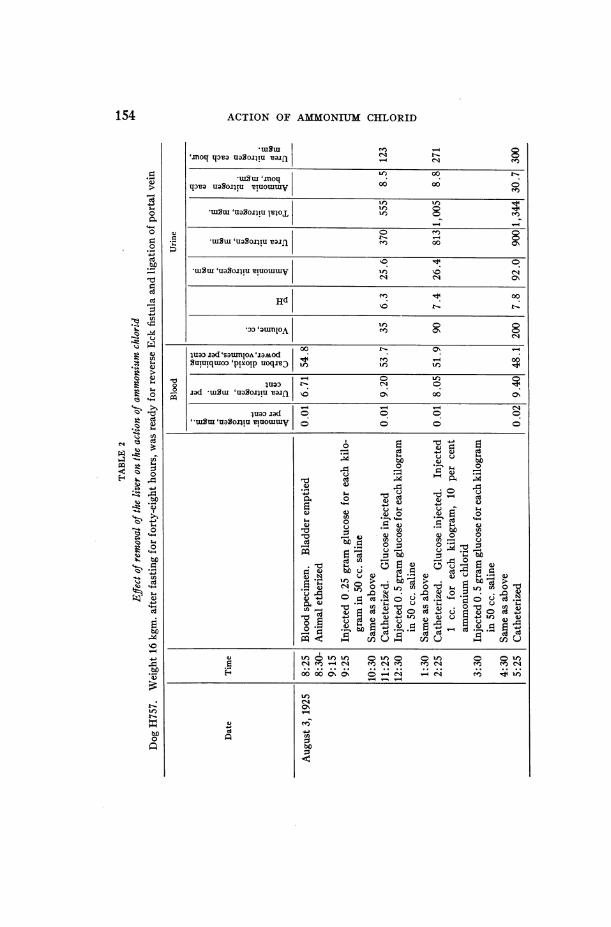
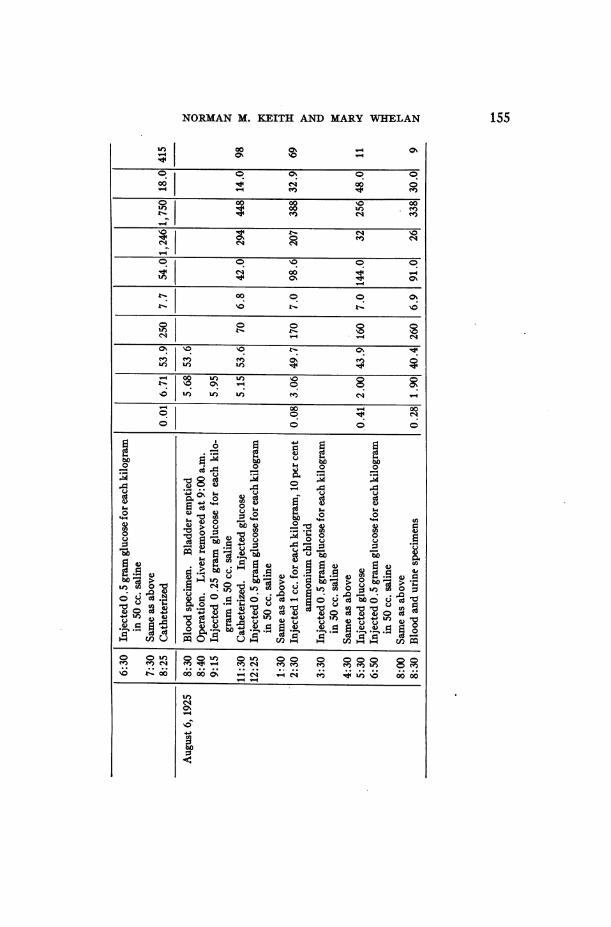
The rapid decrease in the ammonia with concomitant rise in theurea content of the blood and increased excretion of urea in the urinein dogs I127 and G175 indicates a quick formation of urea from theammonium ion of the injected salt. An experiment was carried outby Bollman, Mann and Magath (dog A757, table 2) to ascertainwhether urea could be formed from ammonium chlorid in a dog whoseliver has been removed. The control experiment had been made afterthe animal's inferior vena cava and portal vein had been ligated.After removal of the liver and the injection of ammonium chlorid,urea formation diminished and the ammonia nitrogen in the bloodremained abnormally high for six hours. The result of this experi-ment indicates that the ammonium ion is not readily synthesized tourea in the dog with its liver removed, quite the contrary to whatoccurs in the normal dog. This was to be anticipated from the workof Bollman, Mann and Magath.
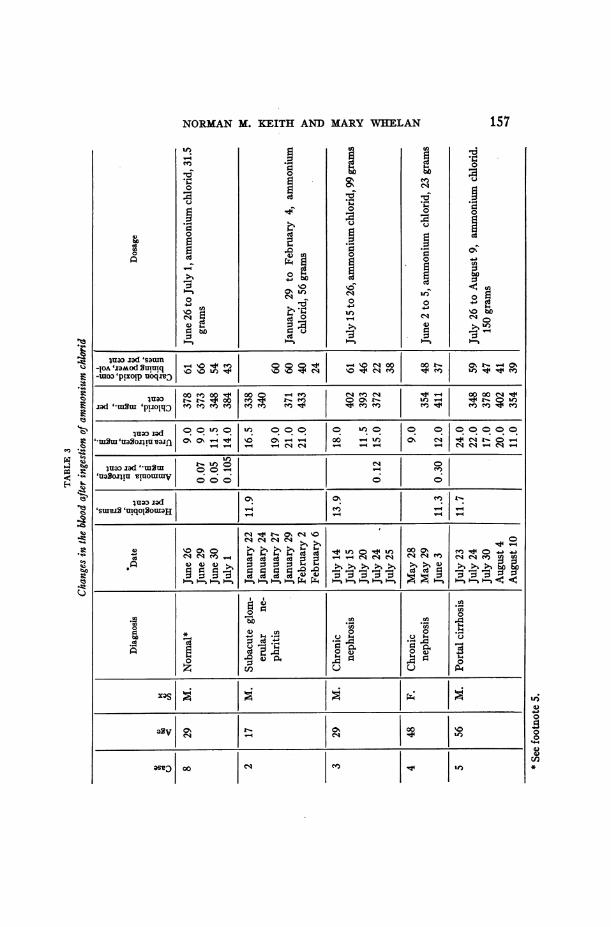
In human patients after prolonged ingestion of ammonium chloridpractically all showed an increase in blood-urea (table 3). A nor-mal man (Case 8) ingested 31.5 grams of ammonium chlorid in threedays (10.5 grams a day) and his blood-urea nitrogen rose from 9 to14 mgm. for each 100 cc. However, one patient (case 5, table 3)having cirrhosis of the liver with ascites showed a gradual decreasein blood-urea even during the continuous ingestion of 150 grams ofthe salt for fifteen days. This variation in the blood-urea contentafter ingestion of ammonium chlorid has suggested a possible rela-tionship between the urea content of the blood, and the presence orabsence of water available for its elimination. During this periodin the same case, there was no marked disturbance in the carbon di-oxid capacity of the plasma. The carbon dioxid combining power ofthe plasma was 39 per cent by volume at the end of fifteen days,having been 41 per cent by volume on the eleventh day and 59 atthe beginning of the period. Nevertheless, in most cases the carbondioxid combining-power of the plasma underwent a decided dropabout the fourth or fifth day after the daily ingestion of the usual
158
NORMANM. KEITH AND MARYWHELAN
amount of the salt, 9 to 10 grams each day (a total of about 40 grams).The plasma chlorid was usually increased. This increase was particu-larly marked in cases in which the plasma chlorid was low at the be-ginning of the ingestion of the ammonium chlorid.
In a few cases the ammonia-nitrogen content of the blood was de-termined before and after several days' ingestion of the ammoniumchlorid. A demonstrable increase in the blood-ammonia has not beenencountered often. Even after the ingestion of 81 grams of am-monium chlorid (9 grams each day) in one case the ammonia nitrogenof the blood was only 0.12 mgm. for each 100 cc. A value as highas 0.30 mgm. was obtained in a single case. If the ingestion of am-monium chlorid should result in the accumulation of ammonia inthe blood the usual methods for the determination of urea wouldnot give the true value of the blood-urea. But the small valueswhich have been obtained thus far in man would not produce anappreciable difference in the urea values since even the highestamount, 0.30 mgm. of ammonia nitrogen, would be equal to only0.65 mgm. of urea.
In this series no studies on the sodium, potassium, calcium, andmagnesium in the serum were made, but a recent study in a singlecase (case 6, table 4) after the patient had ingested 39 grams of am-monium chlorid showed no change in the sodium in the serum. Ina previous experimental study on dogs, the sodium, potassium, cal-cium, magnesium and chlorids were determined immediately afterthe intravenous injection of ammonium chlorid, but no change inthese ions was noted. Gamble, Blackfan and Hamilton have alsoshown that ammonium chlorid causes no appreciable change in theamount of fixed base in the plasma.
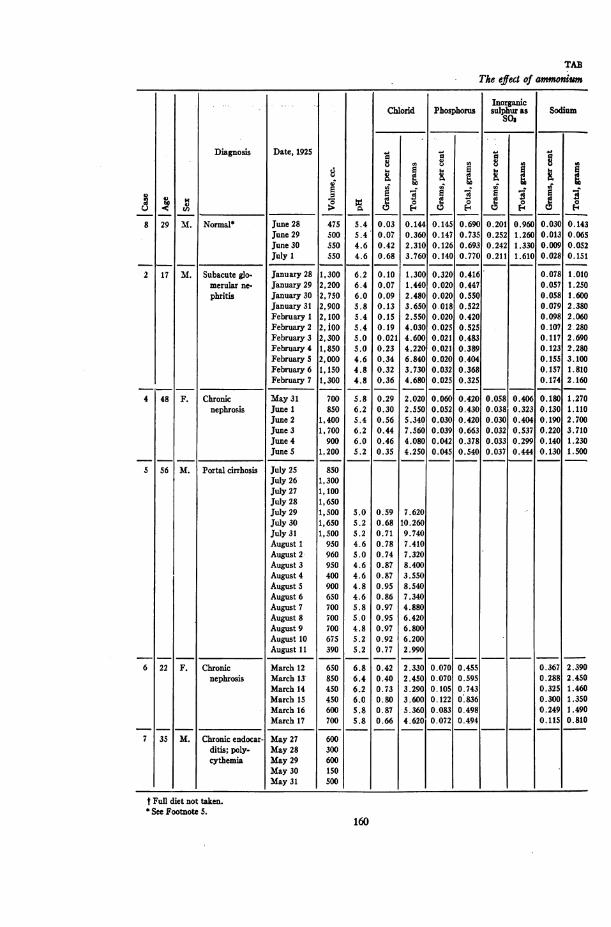
Urine. The ingestion of ammonium chlorid by a normal subject(case 8) and by two patients (cases 6 and 7) produced no change inthe volume of the urine, whereas in the other patients (cases 2, 4,and 5) there was a definite diuresis. In the latter the urine nearlydoubled in volume and the volume remained large as long as the saltwas ingested (table 4). The cases include nephritis, nephrosis withedema, cirrhosis of the liver with ascites and edema, and endocarditiswith ascites and edema. During the first period (ingestion of am-monium chlorid) in cases 2, 4 and 5, the excretion of urine equalled
159
TAB
The effect of ammonitum
InorganicChlorid Phosphorus sulphur as Sodium
So$
Diagnosis Date, 1925
d~~~~~~~~~~~~8
8 29 M. Normal June 28 475 5.4 0.03 0.144 0.145 0.690 0.201 0.960 0.030 0.143June 29 500 5.4 0.07 0.360 0.147 0.735 0.252 1.260 0.013 0.065June 30 S50 4.6 0.42 2.310 0.126 0.693 0.242 1.330 0.009 0.052July 1 550 4.6 0.68 3.760 0.140 0.770 0.211 1.610 0.028 0.151
2 17 M. Subacute glo- January 28 1,300 6.2 0.10 1.300 0.320 0.416 0.078 1.010merular ne- January 29 2,200 6.4 0.07 1.440 0.020 0.447 0.057 1.250phritis January 30 2, 750 6.0 0.09 2.480 0.020 0.550 0.058 1.600
January 31 2,900 5.8 0.13 3.650 0.018 0.522 0.079 2.380February 1 2,100 5.4 0.15 2.550 0.020 0.420 0.098 2.060February 2 2, ioo 5.4 0.19 4.030 0.025 0.525 0.107 2 280February 3 2,300 5.0 0.021 4.600 0.021 0.483 0.117 2.690February 4 1,850 5.0 0.23 4.220 0.021 0.389 0.123 2.280February 5 2,000 4.6 0.34 6.840 0.020 0.404 0.155 3.100February 6 1,150 4.8 0.32 3.730 0.032 0.368 0.157 1.810February 7 1,300 4.8 0.36 4.680 0.025 0.325 0.174 2.160
4 48 F. Chronic May 31 700 5.8 0.29 2.020 0.060 0.420 0.058 0.406 0.180 1.270nephrosis June 1 850 6.2 0.30 2.550 0.052 0.430 0.038 0.323 0.130 1.110
June 2 1,400 5.4 0.56 5.340 0.030 0.420 0.030 0.404 0.190 2.700June 3 1,700 6.2 0.44 7.560 0.039 0.663 0.032 0.537 0.220 3.710June 4 900 6.0 0.46 4.080 0.042 0.378 0.033 0. 299 0.140 1.230June S 1,200 5.2 0.35 4.250 0.045 0.540 0.037 0.444 0.130 1.500
5 56 M. Portal cirrhosis July 25 85000July 26 1,300July 27 1,100July 28 1,650July 29 1,500 5.0 0.59 7.620July 30 1,650 5.2 0.68 10.260July 31 1,500 5.2 0.71 9.740August 1 950 4.6 0.78 7.410August 2 960 5.0 0.74 7.320August 3 950 4.6 0.87 8.400August 4 400 4.6 0.87 3.550August 5 900 4.8 0.95 8.540August 6 650 4.6 0.86 7.340August 7 700 5.8 0.97 4.880August 8 700 5.0 0.95 6.420August 9 700 4.8 0.97 6.800August 10 675 5.2 0.92 6.200August 11 390 5.2 0.77 2.990
6 22 F. Chronic March 12 650 6.8 0.42 2.330 0.070 0.455 0.367 2.390nephrosis March 13 850 6.4 0.40 2.450 0.070 0.595 0.288 2.450
March 14 450 6.2 0.73 3.290 0.105 0.743 0.325 1.460March 15 450 6.0 0.80 3.600 0.122 0.836 0.300 1.350March 16 600 5.8 0.87 5.360 0.083 0.498 0.249 1.490March 17 700 5.8 0.66 4.620 0.072 0.494 0.115 0.810
7 35 M. Chronic endocar- May 27 600ditis; poly- May 28 300cythemia May 29 600
May30 150May31 500
t Full diet not taken.See Footnote 5.
160
£
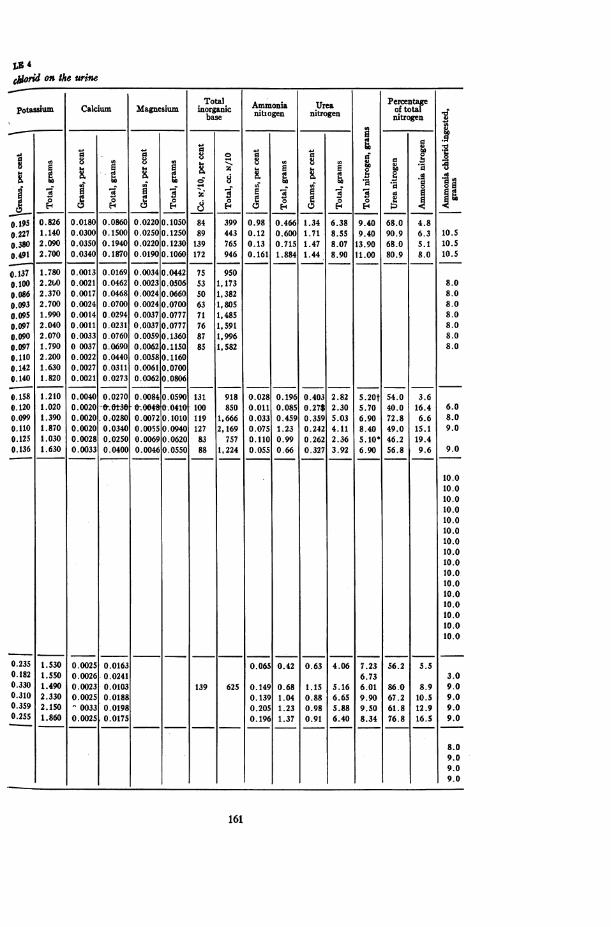
on the urine
Total ~~~~~~~~PercentageCalcium Magnesium Tnotgali Ammonia Urea of totalbaseClunIi| c|nitiogen nitrogen nitrogen
03
Ei . . E t ; f a J aCa 10 0~~~~~~~~
5 0.826 0.0180 0.0860 0.0220 0. lOS0 84 399 0.98 0.466 1.34 6.38 9.40 68.0 4.827 1.140 0 .0300 0. lS00 0 .0250 0. 1250 89 443 0.12 0.600 1.71 8.55 9.40 90.9 6.3 lO.Si02.090 0.0350 0. 1940 0.0220 0. 1230 139 765 0.13 0.715 1.47 8.07 13.90 68.0 S. I10lOS
91 2 .700 0.0340 0. 1870 0.0190 0. 1060 172 946 0. 161 1.884 1.44 8.90 tl.00 80.9 8.0 lO.S
_) ) . ... .)
371. 780 0 00 13 0 .0 169 0 .0034 0 .0442 75 950002.260 0.0021 0.0462 0.0023 0.0506 53 1, 173 8.0662.370 0.0017 0.0468 0.0024 0.0660 S0 1, 382 8.032 .700 0.0024 0 .0700 0.0024 0.0700 63 1, 805 8.0951 . 990 0 . 00 1 4 0 02 94 0 003 7 0 . 07 7 7 7O11, 485 8 0
7 2.040 0.0011 0.0231 0.0037 0.0777 76 1,591 S.e02.070 0.0033 0.0760 0.0209 0.1360 87 13996 8.0
7 1.790 0 0037 0.0690 0-0062 0.1250 89 1 582 8.010 2.200 0.0022 0.0440 0.0058 0. 11607 1.630 0.0027 0.0311 0.0061 0.0700
1 .820 0.0021 0.0273 0.0362 0.0806
1.2.10 0.0040 0.0270 0.0084 0.0590 131 918 0.028 0.196 0.403 2.82 S.20t 54.0 3.6321.020 0.0020 -0.0-30 0.0040 0.047 100 850 8.011O.085 0.27S 2.30 5.70 40.0 16.4 6.05 1.390 0.0021 0.0280 0.0072 0.1010 119 1,666 0.033 0.4590.4385 5.03 6.90 72.8 6.6 8.0
10 1.870 0.0012 0.0231 0.00.575.940 7 2,169 0.075 1.23 0.242 4.11 8.40 49.0 1 809.025 1.030 0.0028 0.0250 0.0069 0.0620 83 7570.7110 0.9 0.262 2.36 5. 10* 46.2 19.4
7 1.630 0. 0033 0.0400 0.004620.150 88 1,5224 .055 0.66 0.327 3.92 6.90 56.8 0969 0
102.2000.00220.04400.00580.1160 ~ ~ ~ ~ ~ ~ ~ ~ 10.421.6300.00270.03110.00610.0700 ~ ~ ~ ~ ~ ~ ~ ~ 10.
10.0
40 1.8200.00210.02730.0620.080610.0258 1.210 0.00250.270 0.0400901131 0.028 0.196 0.403 2.82 7.23 54.0 3.61820 1 .020 0 .002640t0 0-0.0240180001 .8 .2*23 5.70 43.1. 6.0
81301.390 O0.00200020 0.007011 119 1666 0.0339 0.459 0.359 5.03 6.901 72.8 6.6 8.0p.10 1.870 0.00205.340 0.05008817 ,6 0.0759 1.23 0.242 4.11 8.40 49.0 15.1 9.0
259 1.1030 0.00280.250 0.090029885 0.1105 0.99 0.262 2.36 5.10* 461.2 19.4 .3651t.8630 0.0033 [0.0400 0.06005 88 _1,240.5 0.6630.32 3.2 .9018 56.8 9.6. 9.0
10.010.010.0
10.010.010.010.010.010.010.0
1821.5500.0026.0.0241 6.73 3~~~~~~~~~~~1.0
10.010.0
2351.5300.00250.0163 0.065 0.42 0.63 4.06 7.23 56.295.
8.0
161
ACTION OF AMMONIUMCHLORID
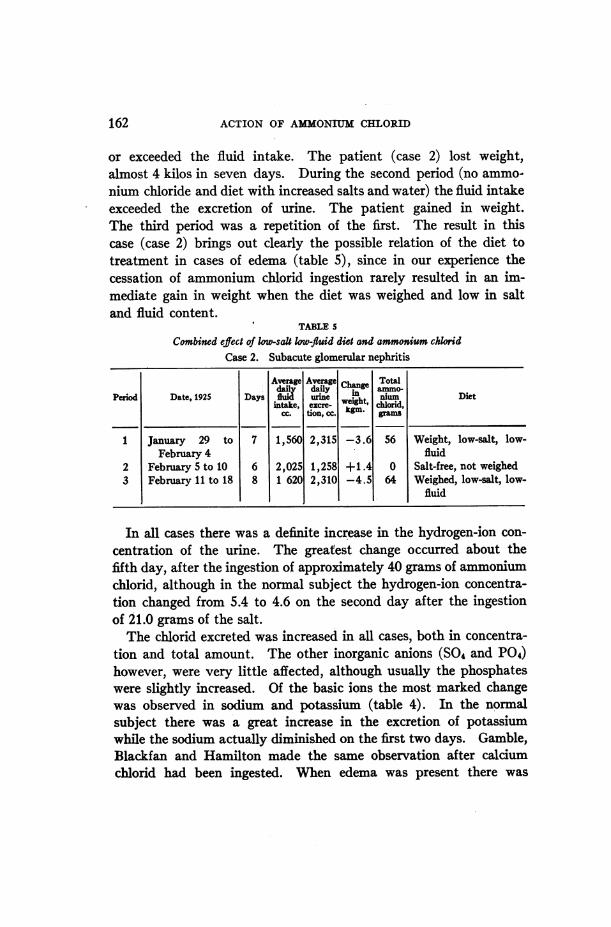
or exceeded the fluid intake. The patient (case 2) lost weight,almost 4 kilos in seven days. During the second period (no ammo-nium chloride and diet with increased salts and water) the fluid intakeexceeded the excretion of urine. The patient gained in weight.The third period was a repetition of the first. The result in thiscase (case 2) brings out clearly the possible relation of the diet totreatment in cases of edema (table 5), since in our experience thecessation of ammonium chlorid ingestion rarely resulted in an im-mediate gain in weight when the diet was weighed and low in saltand fluid content.
TABLE 5
Combined effect of low-salt low-fluid diet and ammonium chlo7idCmse 2. Subacute glomerular nephritis
Averge Average Cne Totaldail da~y ammwo.
Peiod Date, 1925 Days urine Weiht nium Dietintake, excre- chlorid,
CC tion,kcc. grams
1 January 29 to 7 1,560 2,315 -3.6 56 Weight, low-salt, low-February 4 fluid
2 February 5 to 10 6 2,025 1,258 +1.4 0 Salt-free, not weighed3 February 11 to 18 8 1 620 2,310 -4.5 64 Weighed, low-salt, low-
fluid
In all cases there was a definite increase in the hydrogen-ion con-centration of the urine. The greatest change occurred about thefifth day, after the ingestion of approximately 40 grams of ammoniumchlorid, although in the normal subject the hydrogen-ion concentra-tion changed from 5.4 to 4.6 on the second day after the ingestionof 21.0 grams of the salt.
The chlorid excreted was increased in all cases, both in concentra-tion and total amount. The other inorganic anions (SO4 and P04)however, were very little affected, although usually the phosphateswere slightly increased. Of the basic ions the most marked changewas observed in sodium and potassium (table 4). In the normalsubject there was a great increase in the excretion of potassiumwhile the sodium actually diminished on the first two days. Gamble,Blackfan and Hamilton made the same observation after calciumchlorid had been ingested. When edema was present there was
162
NORMANM. KEITH AND MARYWBIELAN
usually an increase in the sodium and potassium excreted, the in-crease in sodium being the more marked. Changes in calcium andmagnesium were slight and difficult to evaluate. The total amountsexcreted were slightly increased. The sum of the basic ions, calcu-lated as cubic centimeters of one-tenth normal alkali, always showeda progressive increase after the ingestion of ammonium chlorid, indi-cating that inorganic basic ions are excreted in large amounts in com-bination with chlorid. Ammonia nitrogen, urea nitrogen, and totalnitrogen increased in all cases, the increase in the last being accountedfor by the nitrogen in the ammonium chlorid ingested.
After the ingestion of ammonium chlorid a certain amount of theammonia appears in the urine; the greater proportion, however, isexcreted as urea. The hydrochloric acid which is formed causesacidosis, which in turn causes an increase in the excretion of am-monia and of fixed base. Of the fixed base, sodium is as a rule thechief component, but, if a sufficient amount is not available, an in-crease in the excretion of potassium occurs.
Basal metabolism. Determinations of the basal metabolic ratewere made on three different mornings while a patient aged forty-eight, with chronic nephritis and edema, was recieving 10 grams ofammonium chlorid daily. After he had taken 30 grams the rate was+1, after 40 grams, -5, after 65 grams, 0. Two hours before the
last rate was determined the patient had received 5 grams of am-monium chlorid. Such results indicate that the ingestion of am-monium chlorid by patients with nephritis and edema has no measura-ble effect on the basal metabolic rate.
ORGANICMERCURYCOMPoUNDS4
Saxl and Heilig were the first to discover that novasurol caused amarked diuretic response in cases of cardiac edema. They demon-strated a relative and an absolute increase in the chlorids excreted inthe urine. Bohn showed that this occurred in rabbits. Nonnenbruchand Muhling showed that in normal persons novasurol caused an
4The organic mercury compounds used in this investigation were novasuroland salyrgan. The former was supplied by the Winthrop Chemical Company,New York, and the latter by Metz and Company, New York.
163
ACTION OF AMONIUMCHLORID
0
C;014
U20
z
6C4
rWeq0
co0z
c)C4
0
0z
jOA'1ga1od wnq o 0 V 0-wao: 'p!xoip uoqnjaoIf
IuaoiJd I°d'*uljt 'stuoqdsoqj (
'IO '-4 00jad 'tt wm'plI3 O 0 _
lua3 jad|°° °°"wtum 'umlssvloa ° 00 0o -0
zad '-uitu 'um4VpoS0|d' 'p.UOjq3 I#X#eVX )I f) IV CE CE Ce) CE
' uaodu 00 00 00 0 00su mqol9~~~~~~m00a C, 0
iuao~ ~jad'su S. .Fi i43gS'ojo 00 V V 00 - )
ci8°e e84 88888ici
*@*- * *-Cs -
c44c C1~4C0 o o o U)oo Co0H_ o
--4U) ao4)
.~~~~. .000
xas* 1
0v H0
I
4,)
C.)
z3
164
$tcb0
.
0W
1. ;1-1
NORMANM. KEITH AND MARYWHELAN
increase in the chlorids excreted in the urine, but the latter showedthat diuresis did not always occur. We ourselves confirmed theseobservations in two normal subjects and a dog. In further studieswe found that there was a relative and absolute increase in the out-put of sodium. Saxl and Heilig, and Miihling, emphasized the earlyappearance of mercury qualitatively in the urine after the adminis-tration of novasurol. Wehave been able to recover quantitativelya large percentage of the mercury injected (48.5 to 85.6) in the urineof the subsequent twenty-four hours.
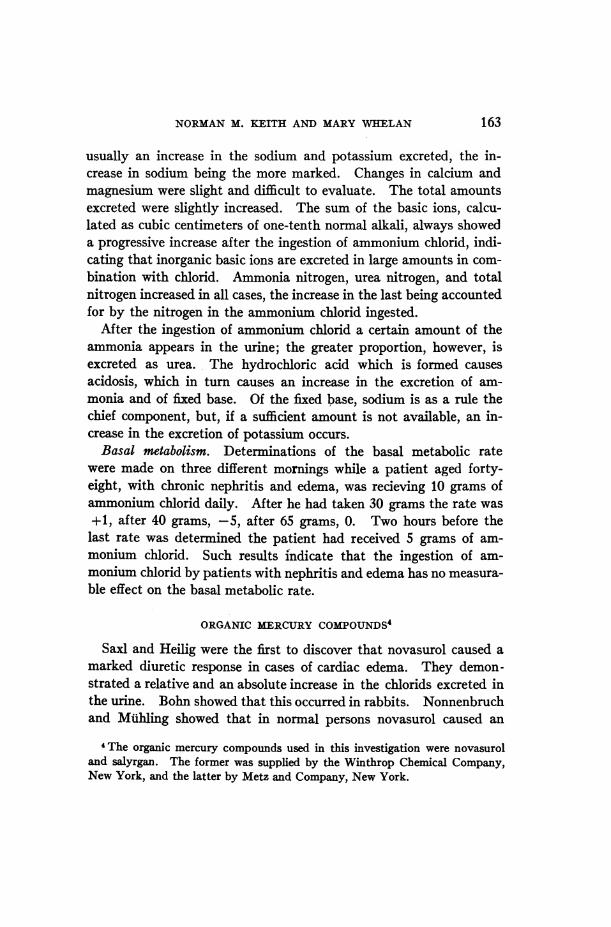
Blood. In the present study the normal subjects and patientswere under the same control conditions with regard to diet and fluidintake as those in the previous experiments with ammonium chlorid.Analysis of the blood and serum in two normal men before and afterthe injection of novasurol (table 6) showed no constant changes inthe concentration of hemoglobin, chlorid, sodium, potassium; calciumor phosphates. The carbon dioxid combining-power of the plasmaremained within normal limits. Nonnenbruch in an experimentconducted under similar control conditions noted no variation in thechlorid concentration, but a slight rise in the protein content duringdiuresis. No significant changes in the rest nitrogen, uric acid orcreatinin were noted by Muhling.
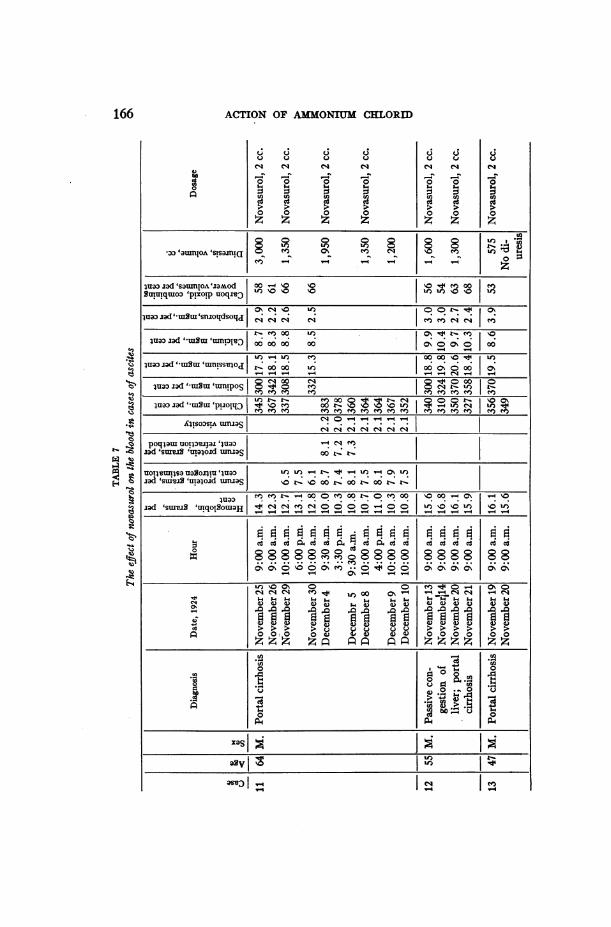
Studies of the blood in three cases of ascites similarly failed to showany constant changes (table 7). These inconstant findings are es-sentially in agreement with previous studies reported by Saxl andHeilig, Miihling, and Bleyer. Crawford and McIntosh report afall in plasma chlorid for from three and a half to four and a halfhours after the injection of novasurol with a later slow rise, also afall in serum protein in the first one and a half hours after the injec-tion in two cases of edema of cardiac origin. That such early changesoccur invariably has still to be corroborated by further work. Theconstancy of the normal values for the carbon dioxid combining-powerof the plasma in our cases is worthy of note.
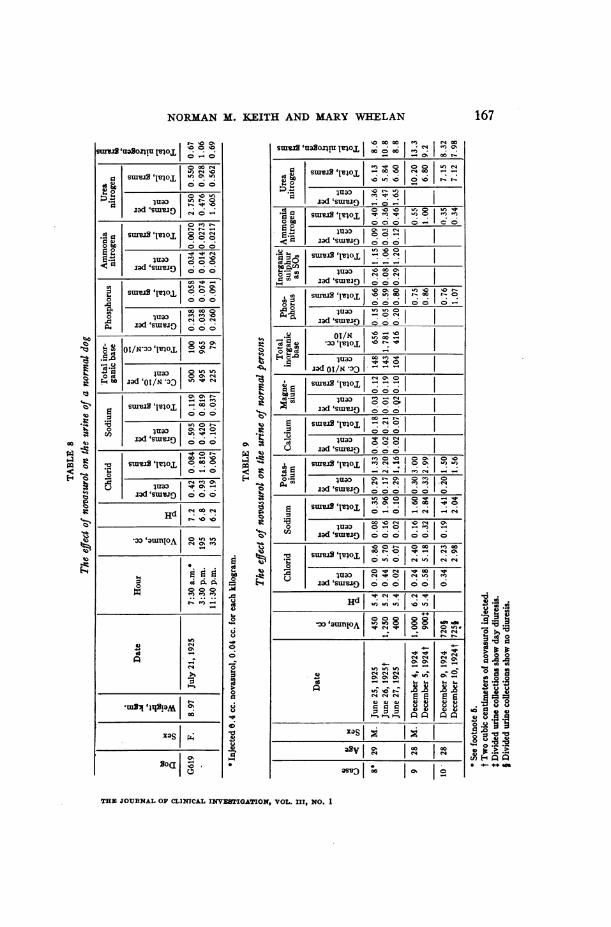
Urine. An experiment was made on a normal dog (dog G619) toascertain the effect of novasurol on the urine (table 8). The animaldid not receive food or water during the experiment which lastedtwenty-four hours. The time was divided into three eight-hourperiods, and a specimen of urine was obtained by catheter at the end
165
ACTION OF AMk{ONIUM CHLORID
0
C c t
0 0 0 0
U) U) U)
v O4 v 9
0 0 0 0
zn z z z
0 0
0 0
zz
C;
u
cg(9
0
-3o~~~~~° °Su°n8oA°s u)meN- z
iuaa iad 'saumoloaZMod 00\-' 00u#|BuTu!quoI) 'plxoip uoqz I ' I I
iuwaad 'tmSu'sn.zojdsoqj j e
oo)0 If) 0%\ tr i'ua:) jad uiau IjW 000000 00 IOuo I I\0
I0 00 e 00 00 '3 00)4uaa jad 'BI'uiui mansseloa oo )ooo 0 C~U~Z~I~UI UT1ISI)O c-00 00 If) 00 O\000 0%
-- - - - N_-
00t.0C4 0 t'0 %luapo ad uIoui sua'UMPS| 8 en t-cf t-
dua:xS'uad d umnll.xS 00t t-
iuIo3 'e*'3n . 00 \0 to_ _4_ ,4llsoasu umias
polqlam uol3vilai-'00ua0| '0enzad 'stuES'u2lqood utlas '- ''t'3 3
UO4uujsQxlsuasanlu 'Jua:) |- uz 4 r - fiad 's uiv 'ula4oid uirua 0 r- \0 oo X- oo' r- 0o x r
jad 'S uiwg 'luxqolotu9|°00 00-0M. %C o\ |
* ,-4 0-5 - C4- 4* 4* .*
; Mv gy jE^MflY;C~ c
'I)'30%0 0~~~~~0M -40 %40~
>aS > >> >
0.0
ooo 4)4) 000~~~~00 0
0~~~~~~~~~~
p.4~~~~~~~~~~~~~~~~~~~0sI ___ __
166
NORMANM. 1]EITH AND MARYWHELAN
I o 0os'uaNloXm~I o,!°O0 00 14
lId'SLUEJO 4 0 No
surealmo,, g4O gI Id 'StU J 00 0 0l~~~~~~-t I, ( 4
jad 'swiv!: 0 a
O ~~~~~~~~000-d
Go00 00
.0 luaoo ~ .10Cud ,IsOj! - C) O
0 -000
od'WdJ0 0 0~01
o- bI Iaolx3o or o
CN 0 to | lua'|O 0000
rn jad Isuaw3jD
U 2U0/)' °I~ °° 0 o
00 | -lad solaI s s 1w° 1o °
p sad 'su18s0 %OO o
0
IIS
raw sm,,I .0o
04.4
t
-r0
Ca
i9.R
01 121asJwr I ~ ~00(: 10 t
oo, o 0
ea I3IObO _____ _ 0 0 0 0 -'
ad s_xu_ _
Oo~ ~ ~sua uavlilj o o I*,
- lad 'suoa o00
Sg V1a 'S11Ie oo o
to~~~~~~~as/oPit I WN ,o o o
___aiR 0100mI|__b+
A ._ a 01o/N *3
b boOoCO
sun 1s S'll°oL o o o
X - In CD
- ad'suxvo 555C's- s 1°1°'0SI0j
lOad 's.uIO 555o'o
u jad .SJ
o'm o °I0I 1 °'
a PBo Xua e 100o -<k uI 0d'sIU IJ0 Oo 10010o
ISwr 1loLL I1~O '°I: m > >
<~ ~ ~ id K2lua IecIs
ja sm[v N
x Va V 10v1 0I00
qb c 0- 0 0. 0
OJOG 2000 0.0
Swvs vfgT - CI~I!! i 1:Igit in Wo r 3 *
A! to10
0
THE JOTURNALOF CLINICAL INVESTIGATION, VOL. III, NO. 1
167
o bo.1 o
<0
0
,I*-4
0
0 1~*t
I-o
I
00002
02QN
*0 .
.q i
~00~
. iroPo000
a ._ ._
]30.0
0**-
ACTION OF AMMONIUMCHLORID
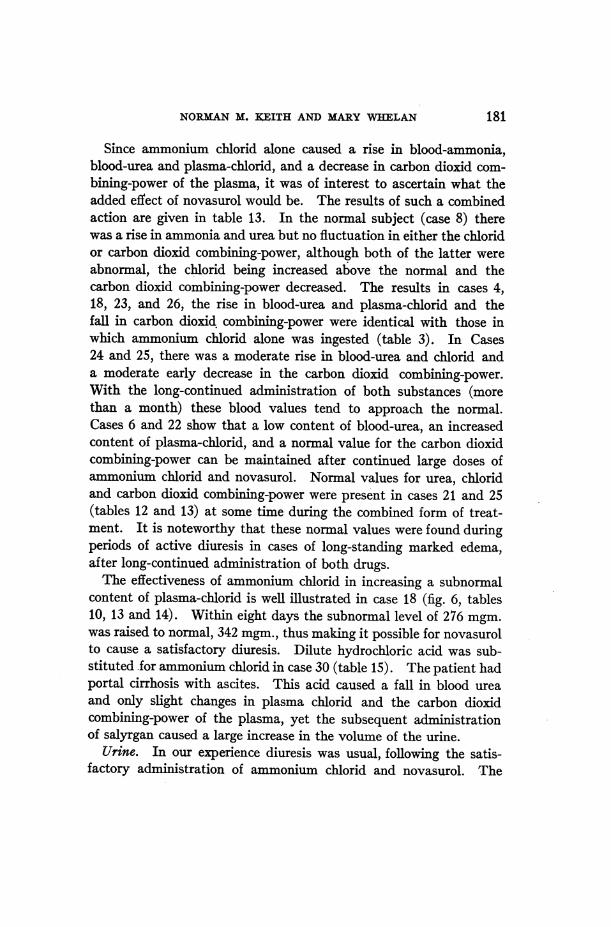
of each period. Novasurol was injected at the beginning of the secondperiod. Thus, we had a control period of urine excretion before andafter the exhibition of novasurol. Following the injection of nova-surol marked diuresis occurred, accompanied by a high concentra-tion of chlorid, sodium and total inorganic fixed base in the urinewhich was maintained, resulting in a striking increase in their totalexcretion. A moderate rise in the output of nitrogen, urea andammonia with little change in the amount of phosphorus or in thehydrogen-ion concentration also occurred. The noteworthy urinaryfindings in the third period were a decrease in the volume of the urineand in the output of chlorids, sodium and total inorganic base, evenbelow that of the first control period. The phosphorus excreted wasslightly increased while the urea and total nitrogen approximatedthose of the first period.
A similar experiment was carried out over a three-day period in anormal man5 (case 8, table 9). His diet was as accurately controlledas that for the patients in the series. As in the dog, novasurol causedan increase in the excretion of water, chlorids, sodium, total inorganicbase, and total nitrogen. The excretion of potassium and magne-sium was increased, but there was no appreciable change in the outputof calcium, phosphorus, sulphate, urea or ammonia. The hydrogen-ion concentration was unchanged. On the third day, or post-nova-surol period, the excretion of chlorids, sodium and total inorganicbase fell below that of the first day. This result corresponded closelyto that obtained in the experiment on dog G619. Nonnenbruch'sexperiment with a dry controlled diet in a normal student gave similarresults as to the chlorid. He did not carry out the other analyses.The continuous increase in the excretion of potassium is of note.
The urinary findings of two other normal subjects (cases 9 and 10,table 9) correspond to the results in the two previous experimentsexcept that frank diuresis was not produced and the excretion ofpotassium remained unaltered. In one normal subject (case 9) theurine excreted during the day was increased, but the twenty-four-hour output approximated that of the previous twenty-four hours.
6 An active healthy physician with the findings of a normal man except for amild type of orthostatic albuminuria.
168
NORMANM. KEITH AND MARYWHELAN
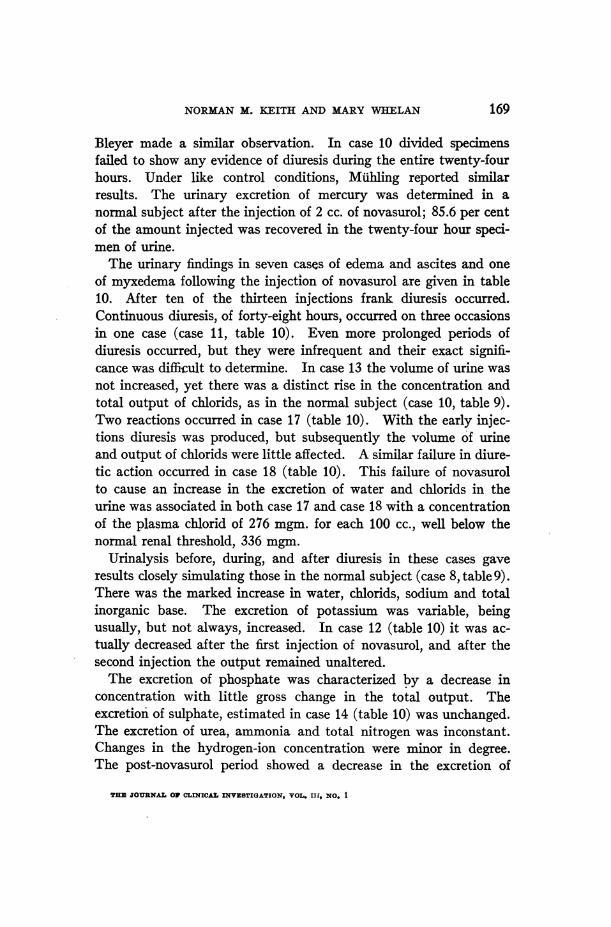
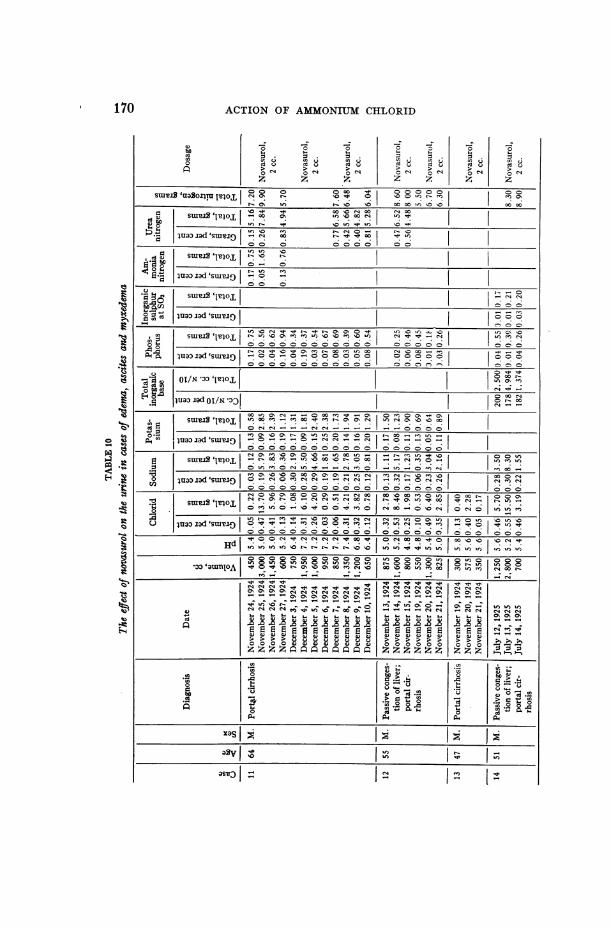
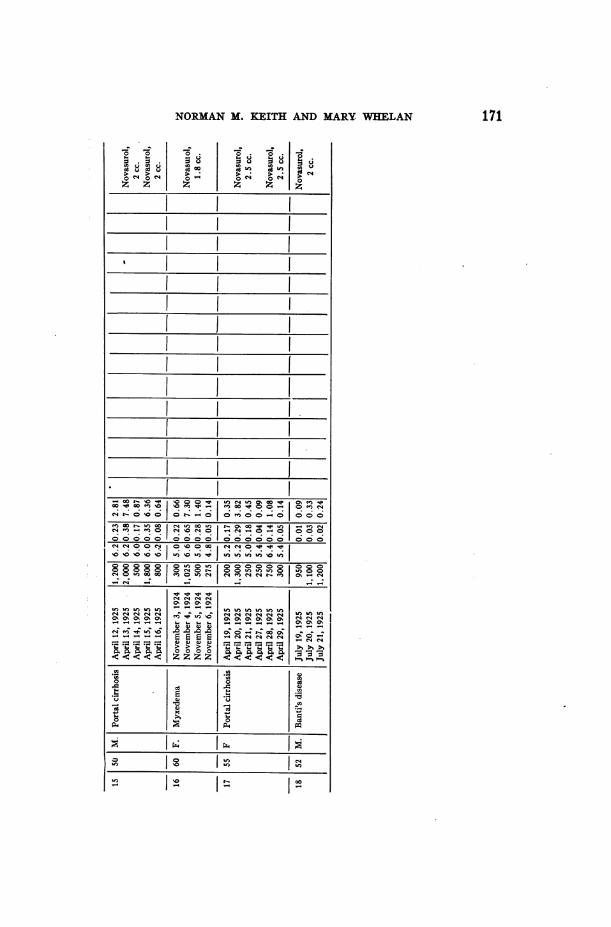
Bleyer made a similar observation. In case 10 divided specimensfailed to show any evidence of diuresis during the entire twenty-fourhours. Under like control conditions, Miihling reported similarresults. The urinary excretion of mercury was determined in anormal subject after the injection of 2 cc. of novasurol; 85.6 per centof the amount injected was recovered in the twenty-four hour speci-men of urine.
The urinary findings in seven cases of edema and ascites and oneof myxedema following the injection of novasurol are given in table10. After ten of the thirteen injections frank diuresis occurred.Continuous diuresis, of forty-eight hours, occurred on three occasionsin one case (case 11, table 10). Even more prolonged periods ofdiuresis occurred, but they were infrequent and their exact signifi-cance was difficult to determine. In case 13 the volume of urine wasnot increased, yet there was a distinct rise in the concentration andtotal output of chlorids, as in the normal subject (case 10, table 9).Two reactions occurred in case 17 (table 10). With the early injec-tions diuresis was produced, but subsequently the volume of urineand output of chlorids were little affected. A similar failure in diure-tic action occurred in case 18 (table 10). This failure of novasurolto cause an increase in the excretion of water and chlorids in theurine was associated in both case 17 and case 18 with a concentrationof the plasma chlorid of 276 mgm. for each 100 cc., well below thenormal renal threshold, 336 mgm.
Urinalysis before, during, and after diuresis in these cases gaveresults closely simulating those in the normal subject (case 8, table 9).There was the marked increase in water, chlorids, sodium and totalinorganic base. The excretion of potassium was variable, beingusually, but not always, increased. In case 12 (table 10) it was ac-tually decreased after the first injection of novasurol, and after thesecond injection the output remained unaltered.
The excretion of phosphate was characterized by a decrease inconcentration with little gross change in the total output. Theexcretion of sulphate, estimated in case 14 (table 10) was unchanged.The excretion of urea, ammonia and total nitrogen was inconstant.Changes in the hydrogen-ion concentration were minor in degree.The post-novasurol period showed a decrease in the excretion of
THE JOURNALOF CLINICAL INVESTIGATION, VOL. Ill, NO. 1
169
o- o oo \oo 0 Co co
t.E suIu2'l In \0 00 C, to
bOzV) O OOC)<
ig~~bo N sosot,oe
A. luxaorad'suar |-iO°g°° °°°°°
SIoUL'I It ooo
93 cn |e uaD jado/*IsI I eo oa~~~~~~~t Wl z° -n \0 bN 0m Ox
S.WX uold'W^1 O_ C, 0_ O O
10M
ce Wao Inboso W C -o4 ao0
jux) jad'sS O f0 C! X 0 0 _ oooq O U0 00OOC
O luaz) iad OSWIN-:OC-4
0NOoXX_ eecs- rmd
_ luu lllo 10 09 ll 0:O0000 O O
0~~~I' amO Xov mt+t-) 00-
Siuovaltoj- oU) oo Lo
09*_1_l0I-CN0
mao to .w ( ^O|e oo_§0'n, 11) 00
\0s| as Ir M 11 >3\| 00
lua:)i) |si! Co I Cm I- I _)00C )C )( )C ! )C
170 ACTION OF AMONIUMCHLORID
cdb)Cd
t~
a
.a
--Z --Z -Z0 0 0w w w= 0 =%cr. U cn U rn UCd 0 ed u cd u> C14 > >0 0 0 "
z z z
0 0I.. w:z ::%tn v In Ucd U cd u
0 C-1 0 cli
114
ecd u
t4>d u
NORMANM. KEITH AND MARY. WHELAN
0
0.
C4 0 "
z z
0 t:
.; 0
. i
9
I~~~~" l~"!1 C!_
toc_ _- [*"_
_ e In_
I.~~~a * * 0 1.
~~OO'~~) C Q~~~ - Co~-0 D 0e0 N.cs0- 0
00000 ooool ~~~~~~~~~~~~~~~~~~~~~ &5o~~~~i
cO U~~~~~~~~~~~~~~~~~~~~i
- -o -~~~~~~~~~~~~~L
171
ACTION OF AM[ONIUM CHLORID
'4o
*C..'
-6
.40
0
0 .05. 5.4
C1 1
0
0
C._
0
0
* vz
5-4
u) * 30_
00 N
oz
0cs
0
Ci4
'4i
(-4)
4)
0C.
En
C1 bO
o
ON
on 0
C.)
05.4
Ui)040z
%Ooo00o %-o 4 U0) 0000OC4 " V o oo C 00sthJZ'iemoJ 0Ot°Ot '.NC 0 )V°0'4U)000 X ° t
0 o \o to in m
100eUo40 V ) C14 4 SOm0>t \0 00I) W 0 U t -
000000 000000000000 00
.Rd04 CS . \ \ 00 14 C 00 00 00 \0%
00 00 00 00 \0U+U) \i \o\o inU) iU) U)iU) LU) U)U
0000000000o 0000000 0° ° 8 °c°ao aumino 8 U) u) UoV) 8 o I u)V) r2i1, in V- t Wo \0 00 14 d4 V0) 0 00 in m U)
C1440% Cs
C4C'4 in%in0%0%0%0%0%0%0%0%0%0%000%C\0' -4C4q - - - - - - -- - -
-1c4C4C4.0
C11--- - --"m 4 - - e4c1e4 C.4 SO.
zZ
.n En.eIA~~~~~~~~~~~~~~U
~~ ~ ~ ~ ~ -U
0
0 0z~~~~~-'
_ _ _ _ _ z_ _ _ _ _ _ _ _ _
%0
172
M *
.4
0
0
0z
1)
NORMANM. KEITH AND MARYWHELAN
4bo
*S0
0
0Cs
U)
0Q 3gi u
C4eqC4 -
5-.
0 0z z
0eq
la0
0:au
0
0%
q.u
0 0
0 0>
go
C-)
eq
Az
bO
0
00
c2U3u
4.10U)
-
1
A
I..,b)O
_v
o 0
0
~0
0 zd
.5 .0 0
04- 0
CE)
- CE)
8i 0
V 4 4OCE V-
*CE)1 ~if
Aouoz z6
(EDlI0 if;eQ ~ O 00 qOU 0%0'IO ) in f)4 %0C4 -4S %c44 C4 CDCD - °q -° -N % Z;Z m os ° 8 > I-NO o_4 e7 %Ou)u, e0 C _I _0 % eoow w
m 000C0 00) 00 00 0000o-
0oooeq eqOo0%0O00O%%O
Of %0 i) _ )1f)1f) 4 if) if U) f)X %00 o r
* %* %*) * -* -* . .* * * * *. . ..
0000
oooe 0oo0oooo ooo oooo o~e
U0%0%0% 0U ) )U v )U U )U U) if) if)
°88°°g °° eqqeqeqe°8°°°8e
4 s )4) 4) - - - - 4-4 4-4 -)U-U)-4
o,0,. U)U%UgU)U)I_4)4)4) )U sOsO so ^^o le r C> _0
@ i Q oio
zz
C __________NmW l l >S
0e 0
p4~~~~~~~~~~~~~~~~~~~~~
CD
173
is
.200404)4)
Cl)
174 ACTION OF AMMONIUMCHLORID
chlorids, sodium and total fixed base, as in the normal control experi-ments.
COMBINEDEFFECTS OF AMMONIUMCHLORID AND ORGANIC
MERCURYCOMPOUNDS
By the extensive use of any new therapeutic agent one soon learnsto limit its use to certain specific conditions. Ammonium chloridproduced striking diuresis in our early cases of edema. We then
Novasurol 20 cc. 2.0 c e
C.yT10l 2 + 6 7 Il
3500O-__-----:i1: --X
Wooeighe lo a diet
71000 it| -_i-_2_$4l
OFltuid intake 0 UJrine outpuit .-.Bod,y weight*Fixed base 0 Ammonia al Hydrochloric acidw
S Sttlphtwic acid B Phosphoric acidSPhosphoric acid has been calcullatedw as 0.1 M4. solu±tions
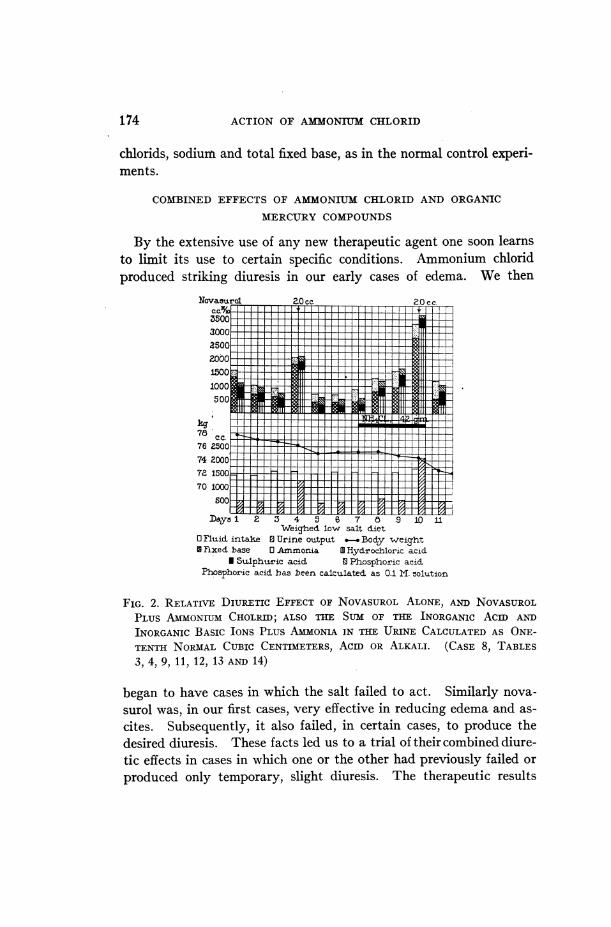
FIG. 2. RELATIVE DIURElTIC EFFECT OF NOVASUROLALONE, AND NOVASUROLPLUS AMONIUMCHOLRID; ALSO THE SUM OF THE INORGANIC ACID AND)INORGANIC BASIC IONS PLUS AMMONlAIN THE URINE CALCULATEDAS ONE-TENTH NORMALCUBIC CENTIMETERS, ACID OR ALKALI. (CASE 8, TABLES3, 4, 9, 11, 12, 13 AND 14)
began to have cases in which the salt failed to act. Similarly nova-surol was, in our first cases, very effective in reducing edema and as-cites. Subsequently, it also failed, in certain cases, to produce thedesired diuresis. These facts led us to a trial of their combined diure-tic effects in cases in which one or the other had previously failed orproduced only temporary, slight diuresis. The therapeutic results

NORMANM. KEITH AND MARYWHELAN
of ammonium chlorid and novasurol in combination has, in manycases, been really remarkable, the loss of weight due to removal ofpreviously retained fluid amounting to as much as 70 pounds (31.8kgm.) in from five to six weeks.
Comparison of the results obtained before and after the use ofammonium chlorid and novasurol combined are well demonstratedin table 11. In the normal control, case 8, the volume of urine isdistinctly greater, 2100 cc., after the combined drugs than after nova-surol alone, 1250 cc. (fig. 2). In case 13 novasurol produced no diu-resis on November 19, whereas with the combined drugs the outputof urine six days later reached 3200 cc.
Such results established the efficacy of this form of treatment on asound basis. Wehave since made numerous studies directed chieflytoward elucidating further the problem of the action of these sub-stances. Interesting changes in the acid-base equilibrium, waterbalance, the concentration of chlorid and other inorganic ions,.and inthe formation of urea and ammonia have occurred which are of bio-logic significance and may be useful in throwing light on other alliedproblems.
Blood. Studies of blood concentration were carried out in detailin case 21 (table 12). The patient received the usual constant diet,low in water and salt (3 grams of ammonium chlorid daily as a sub-stitute for sodium chlorid), throughout his stay of five weeks. Nova-surol was given on seven days, with marked diuresis (a maximum of2900 cc.). During four of the periods of diuresis the hemoglobinincreased in concentration, and in one the plasma protein increasedin like manner. The plasma water showed some minor hourlyvariations which were not constant. The plasma chlorid remainedunaltered during one period, but fell distinctly at the end of thetwenty-four hours in another. The carbon dioxid combining-powerof the plasma deviated from the normal once with a moderate fall.No changes of significance were observed in the concentration ofsodium, potassium, calcium and phosphate in the serum. In anormal subject and in a patient with portal cirrhosis, who were re-ceiving 10 grams of ammonium chlorid daily (cases 8 and 22, table 12)the chlorid concentration fell slightly in one but remained constantin the other.
175

4)400
ACTION OF AMMONtUMCHLORID
eq En
o. S S S 8 3C14 0 ~~.0
sn0oqdsotqj
wnisuu'4X umlsflI o ~ i
Z_ _ _ _ _ _ _ 0% 0%
U) '0oa 0 C00
I-rgr '=906n!U 'sa P0°°l[ ° c4
wond sommoArn 00od 0to 0-unqwoo pxos mcaltpou IsIC I
jlui J2d'subou '^nojd pv '0 o ooo
iuo szd 'sOUJlIOA 'Zaho0d Sot U) E) CE) 00 e 00I~~ ~ ~~o o b C) 'u) c4 U)e s
uao JSad' suI'=opO o )O OO Oin
~~~co ce o ci CL ei ci 00 CL4
d
00 0 00 0 0sC14 eqCN\o0 e\ s
00 U 0% U) ~ 4U) + a
1u0zd"SmPiop:Ish1dX-I aE g '0#
g } .~~~~~~94 V.!
.~~~~~~~~~~~~~~~~'4.
0 000~~ 00
CE)2 CE)CE)CE
t1> ~ ~~~~~ cis
00 000000 0%eq~~Ca)0%%%qE'00
xas~~~~~~~~~~~av~~~~~~~.4q e
176
I
(:1
A14)
mosl 00

NORMANM. KEITH AND MARYWHELAN
C)
C.)
014
0z
(3
0~14-40C12
0z
%OC4"C! 0 ~ ~ ~~0 C
1-~~~~~~~~~~~; ~;s
) '000to 40 00 0 %o s- o 0o 0r9 \0r_s _I _e _ %0
ce Cd C: 41:i ci 6. ci ci c iQ gg 8 °O ° Q° 8 o 8
OO000C000
os~ ~ ~~ leoeCh
- - - -
G G) 0% 's -
~~~ ~~~~. ez z z z z
0
0__________I#L________vz
177
If)to
0
00
-4)4.)
En)

ACTION OF AMMONIUMClHLORID
c00tp
0
Cl
0
cl~
00Clq
EnO
z
9
blo
(c)4S"6
0S-
0u9
00
55
C4
-l0
S-0
Oci
0
a)
En
bi)
"'I0UC)
o Q
0N4
(c)0
C0e u
m u)
M 0
_Cl _Cl
0 0
01 01w C"l 1cicci
0 0
En O cn 4
0Cu>z 1-4 >z -.
"600
1<
Cl0
0%0)
C UC)Cl U) Cl Cl
0c0
U) U) cn)0 c0 - 0
z zz
00
C-
C)
Cl4C.4
01~C
0
c;C)4-l0
C^ 0
0.,
cd 0ci)
> bO0 0
i-,:
lu;u iad 'satunlOA t- \4 \I 00 \ 0 00 ) #
'i;mod SuIuiqm oop!xotp uoq,3 swelutl
luaI jad oo 0 o O t too \O 0 o -oe v\o
wua3 id ' waui 'ua-01!uTU OU0IWtU pOOlJ 5 5
juacz.ad ' uiOui 00% c -. 0 9c4 O° 0
'usSo2ol!u vain poo)llt C,4 00 i° t t- 00 C 0%
eq m00 m \O '-00m00 10 4
00 1f) 0)0%4--0
e>4(})2 )000%a~e'ia a~~i e'X ied i ca an
0 ~~~~~~ 0 0) ci)0 0 Y Y S S S S S¢ Y Y¢0W¢
z QD Q
0s~~~~J 000 $-XQS 4|S12
a51 o|ChC1
178
"0300
.0
0
03
C)
0
0
c-ccc, 03- cc-
0
g-.c03
.03
03"03
cO
0
0
EN
00as'DI °°I

NORMANM. KEITH AND MARYWHELAN
14bO)0U)
1-40la
*-4
43 . _
o
o 0
0
o . 4
r 14
44 0~
44 o 4)
0ds0
u)2
aIC.)04
g o
o 68U
bo uo.4
,'IobO 0
o gto
-4 4
c4
o-~~~
*~~~~~~'
cd cd
0%U
-, C')
C-4 44)444444 44d4444
.'t*U0
C44*-6
0
C')
-)0
04
00
1000
04
I44~~~~~~~~~~~~~~~~~~~~~obc
CS)
0
C- CC C-) C- ,
cd~~~~~~cd d d d Cd CdC's cn o
c '
0
C-)
_4
-44
0
c4Ei
cn
-4
a
0
0
U)
Cl)
14444
C4C0
c4OCA)
0
C4 C') C') C') C')
0 0 0 0 0,, 2 2- i-
bn > > > >bUD =s 0
.04 to 0 00 00 0% 0 00 11)4~QmO00 U) NO 00 C4N -U'-4 00U)~4U) 14UIto U) C o I oo It 0 Uo) in mIU \o%%o
ON \~ 0\0 00 U) lq 00 00 \%.0 0C') \0 0 C'4ON \0t-. 00 ciUl) in t- t- 00 4
00)m 00 00000 0 m m 0 mC inU) 00g 0 \ mU 00 00 \0
b o o oo e e oo X £w - o 4 -o'-4 C)4 t- U)
_44c 4 | '|c4 444c 4 n E El EUE | Cl2D D
c4 ec4 44 444444*4)4)4)4)¢ ¢ ¢ ¢ ¢ M__ _M 43 we4iCl00C/ 4i 4 44 C
A I mI mCE)
4.)bb.b4.) 4b0 0
Q U_ _ 0 _ _ _ _ i4___. ; __ __ _ __ _ _ __ _
1- J0I __ __ __
Ul)
179
14bObo
8
-O
1.40
"C
0
>4oO
- U) -.4
O - 0
AAZ
0C')C','
1C')
ACTION OF AMMONIU[ CHLORID
En
UI)
*W
8440
.C C
o3, 0
144
C) a
o C'4 eC) _,Ut o )o
Qc =C
,O t0 4 en
EnEl44o
0
C)
0u
4 -
o
;uao.ud 'satUnloAli'zaod RuSuqwoo inu)° q
.p!X uoqjw eWsvId
4monad "-f s C14 - U)
4Ua d"Itutu 'uaS-mJ1u vluouau pooIE[
4ua jad'ruSw 0°0uo ) 'o'naSonl!u umain pool| °- 0 0 3
V- -e4 4 C~4 C4
U) aU) %
044
d d voNvCd C 0 0
En F neC) 0
0 0 o 00,xS|%| boU
U
_ _ _ _ _ _ _ _ _ _ _
aSvn E
180
:m*.
U)
S0
00
IL)CD)O
NORMANM. KEITH AND MARYWHELAN
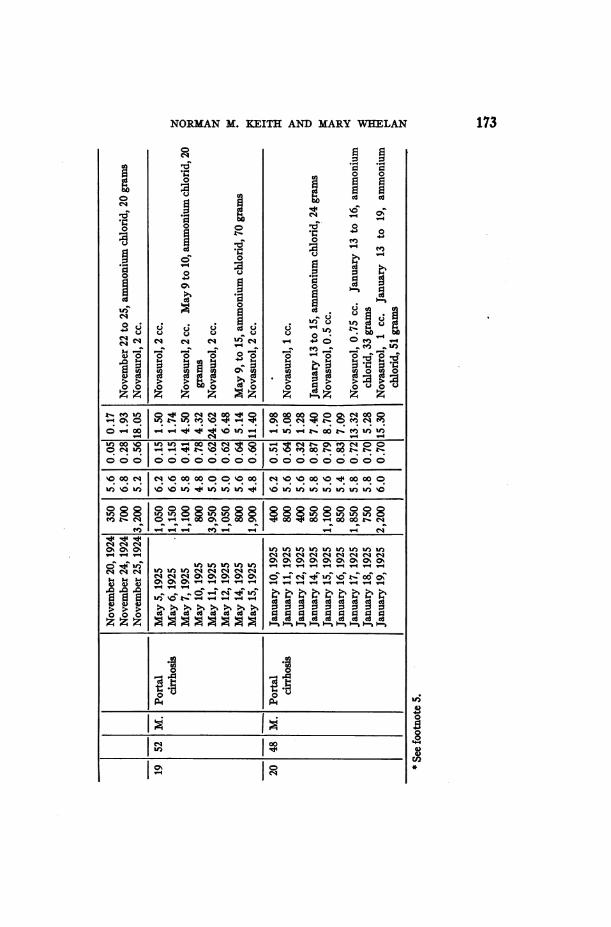
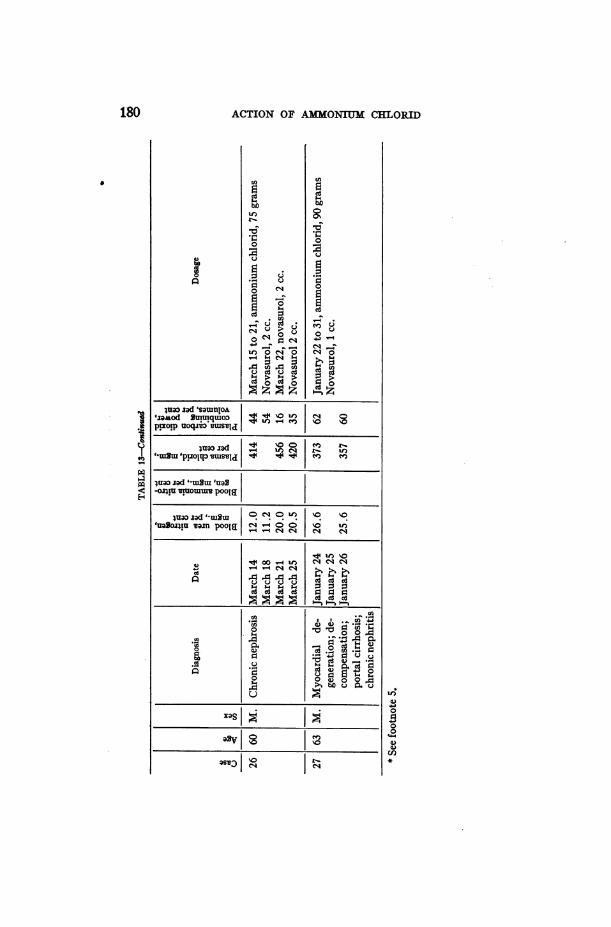
Since ammonium chlorid alone caused a rise in blood-ammonia,blood-urea and plasma-chlorid, and a decrease in carbon dioxid com-bining-power of the plasma, it was of interest to ascertain what theadded effect of novasurol would be. The results of such a combinedaction are given in table 13. In the normal subject (case 8) therewas a rise in ammonia and urea but no fluctuation in either the chloridor carbon dioxid combining-power, although both of the latter wereabnormal, the chlorid being increased above the normal and thecarbon dioxid combining-power decreased. The results in cases 4,18, 23, and 26, the rise in blood-urea and plasma-chlorid and thefall in carbon dioxid* combining-power were identical with those inwhich ammonium chlorid alone was ingested (table 3). In Cases24 and 25, there was a moderate rise in blood-urea and chlorid anda moderate early decrease in the carbon dioxid combining-power.With the long-continued administration of both substances (morethan a month) these blood values tend to approach the normal.Cases 6 and 22 show that a low content of blood-urea, an increasedcontent of plasma-chlorid, and a normal value for the carbon dioxidcombining-power can be maintained after continued large doses ofammonium chlorid and novasurol. Normal values for urea, chloridand carbon dioxid combining-power were present in cases 21 and 25(tables 12 and 13) at some time during the combined form of treat-ment. It is noteworthy that these normal values were found duringperiods of active diuresis in cases of long-standing marked edema,after long-continued administration of both drugs.
The effectiveness of ammonium chlorid in increasing a subnormalcontent of plasma-chlorid is well illustrated in case 18 (fig. 6, tables10, 13 and 14). Within eight days the subnormal level of 276 mgm.was raised to normal, 342 mgm., thus making it possible for novasurolto cause a satisfactory diuresis. Dilute hydrochloric acid was sub-stituted .for ammonium chlorid in case 30 (table 15). The patient hadportal cirrhosis with ascites. This acid caused a fall in blood ureaand only slight changes in plasma chlorid and the carbon dioxidcombining-power of the plasma, yet the subsequent administrationof salyrgan caused a large increase in the volume of the urine.
Urine. In our experience diuresis was usual, following the satis-factory administration of ammonium chlorid and novasurol. The
181
TABThe effect of combined ammonium
29
MM)
M.
Diagnosis Date, 1925
Normal July 1
48 F. Chronic nephrosis
July 2July 3June 4June 5June 6June 7
Blood
14.
laed a00E Gi 8
16.0
14.021.612.0
s-E tk
B 1._-. ~ 4)OF
(.
384 55
384 43390 43
411 37
550
2,100500
9001,2003,1001,050
m
4.6
4.65.06.05.25.65.4
Chlorid ISodium
0.68
0.550.220.460.350.52O.S3
ia
.-r0
3.76
11.471.224.084.25
16.005.61
7 35 M. Chronic encar- June 21 300 5.2 0.38 1.15ditis, polycy
Jthemia June 22 13.0 366 48 1,750 5.2 0.56 9.27June 23 2,050 4.810.56 11.44
- _ .__ ________ June 24 1,000 5.610.51 5.04 _ _52 M. Banti's disease,
ascites
Portal cirrhosis
Portal cirrhosis
181 M. Chronic nephrosis
20 48 M.
22 27 F.
26 1 60 1 M. I Chronic nephrosis
July 31
August 1August 2August 3August 4August 5August 6January 18
January 19August 15May 10
May 11May 12September 2
September 3September 4August 16
TotalAugust 17August 18August 19September 27September 28
September 29September 30October 1March 24
March 25March 26
21.6
21.0
17.0
366
372
33
46
14.3 404 36
9.7 396 486.9 366 58
14.0 376 48
12.4 370322
5268
18.0 1324170
20.0 420 35
700
2,6502,2001,3003,1751, 150
950750
2,200850850
3, 7001, 550
500
3,700550
1,700
2,0251, 9505,675
7005, 710
715700600
500400
750
5.6
6.66.26.46.46.25.65.8
6 04.65.6
5.05.45.6
5.45.66.4
5.47.2
5.45.45.05.45.8
5.2
5.6
5.4
0.16
0.430.400.380.410.360.130.70
0.700.520.66
0.640. 560.69
0.530.480.61
0.560.56
0.51
0.530.470.170.16
0.260.29
0.34
11.458.704.98
12.904.141.555.28
15.304.345.64
23.768.823.39
19.502.64
10.40
11.4210.9932.813.57
30.493.341.190.97
1.321.15
2.52
Q
114
0;
0.03
Eto4.4
0~.15
0.20 4.150. 03 0.200.140.130.280.26
0.130.100.180.150.050.030.34
1.231.508.682.70
3.442.312. 294.730.530.332.53
Potas-sium
08 to
x. a
9 ;'0.49 2.70
0.13 2.840.24 1.330.12 1.030.14 1.630.06 1.760.10 1.06
0.170.150.090.090.070.050.15
4.513.231.172.860.850.471.09
Calciun
8
ga0.03
0.010.020.0030.0030.0040.006
0.03
14
0.19
0.3011
0.020.04,0.130.06
0.391 8.6210.0811.8010.02 10.37
0.131 1.10I0.0811.1110.03 0.42
0.300.210.01
0.200.020.38
0.350.40
0.030.240.040.020.01
0.020.02
3. 11
11.193.270.05
7.550.146.43
7.097.76
21.280.20
11.280.250.130.05
0.110.08
0.84
0.060.100.21
0.080.100.03
0.010.01
0.120.100.06
2.051.501.05
3.150.570.58
0.230.251.060.914.750.38
2, 800 5.4 0.51 14.88 0.28 7.84 0.03 0.761. 300 7.0 0.46 5.94 0.27 3.52 0.04 0.58
0.02 0.590.01 0.24
0.00510.08
0.004 0.080.004 0.09
0.25
.27 63 M. Chronic myocar- January 24 26.0 373 62 1,330 4.6 0.66 9.24 0.39 5.92 0.13 1.74 0.18 0.24dial degenera-tion; chronic January 25 2,850 4.4 0.66 19.50 0.44 12.68 0.07 2.05 0.18 0.52nephritis; por- January 26 24.4 357 60 1,650 4.6 0.46 7.500.29 4.62 0.10 1.60 0.13 0.22tal cirrhosis ._._____.
29 20 F. Polyserositis March 1 300 6.4 0.65 1.94 0.07 0.22 0.12 0.37 0.005 0.01
March 2 12.0 402 48 2,400 6.2 0.64 15.26 0.30 7.32 0.07 1.64 0.001 0.27March 3 400 6.0 0.58 2.30 0.06 0.25 0.11 0.4610.003 0.01
Se_ otoe5ul itnttkn
t Full diet not taken.
182
X
8'
18
24
1 .13 10.131 0.9410.171*106
-1-125 1 26 M. Polyserositis
o 0sl.65
0 See footnote S.
14
-hlorid and novasurol on blood and urine
* Phos- ~~~Inorganic Toteal inor Am- Uephorus s gani base on nitrogen 8
as03 ~~~nitrogen
8n4) k Dosage
-i 4 ~~~~~ 4 ~~~ li 4E
4-
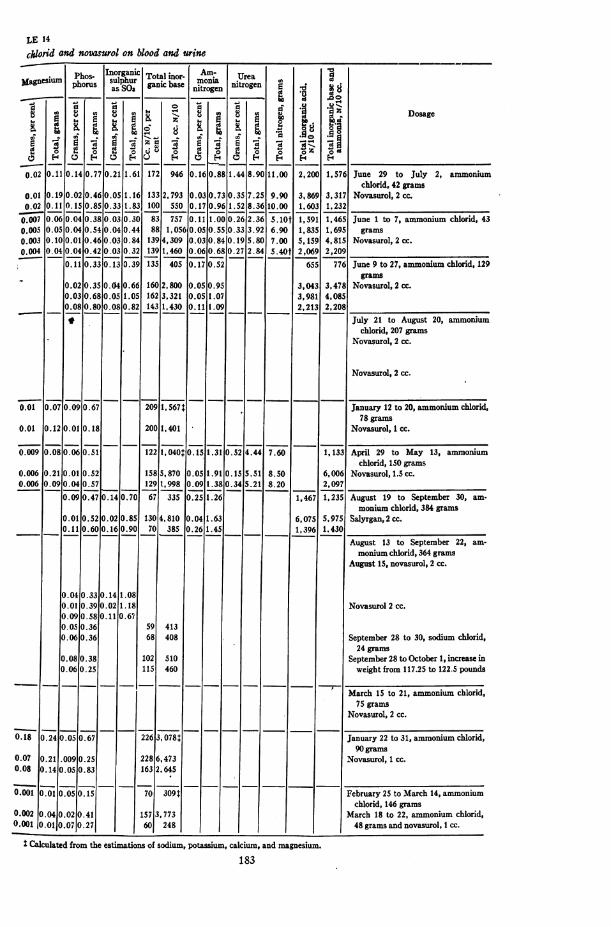
0.02 0.11 0.14 0.77 0.21 1.61 172 946 0. 16 0.88 1.44 8.90 11.00 2, 200 1, 576 June 29 to July 2, ammoniumchlorid, 42 grams
-i.0l 0.190 .02 0.46 0.05 1.16 133 2, 793 0.03 0.73 0.35 7.25 9.90 3,869 3,317 Novasurol, 2 cc.'0.02 0.11 0. 1S 0.85 0.33 1.83 100 550 0.17 0.96 1.52 8.36 10.00 1,603 1,232.007 0.060 .04 0.38 0.03 0.30 83 757 0.11 1.00 0.26 2.36 S.lOt 1,591 1,465 June 1 to 7, ammonium chlorid, 430.005 0.05 0.04 0.54 0.04 0.44 88 1, 056 0. OS0.555 0. 33 3.92 6.90 1,835 1,695 grams0.003 0.100 .01 0.46 0.03 0.84 139 4,309 0.03 0.84 0.19 5.80 7.00 5,159 4,815 Novasurol, 2 cc.e.004 0.04 0.04 0.42 0.03 0.32 139 1,460 0.06 0.68 0.27 2.84 5.40t 2,069 2,209
0.11 0.33 0.13 0.39 135 405 0.17 0.52 655 776 June 9 to 27, ammoniwm chlorid, 129grams
0.02 0.35 0.04 0.66 160 2,800 0.05 0.95 3,043 3,478 Novasurol, 2 cc.0.03 0.68 0.05 1.05 162 3,321 0.05 1.07 3,981 4.0850.08 0.80 0.08 0.82 143 1,430 0.11 1.09 2,213 2,208 .-* July 21 to August 20, ammonium
chlorid, 207 gramsNovasurol, 2 cc.
Novasurol, 2 cc.
0.01 0.07 0.09 0-67 209 1, 567- January 12 to 20, ammonium chlorid,78 grams
0.01 0.120.010.18 200 1,401 Novasurol, 1 cc.
. .08 0.06 0.51 122 1, 040 0.15 1.31 0.52 4.44 7.60 1,133 April 29 to May 13, ammoniumchlorid, 150 grams
0.006 0.21 0.01 0.52 158 5,870 0.05 1.91 O.5 5.51 8.50 6,006 Novasurol, 1.5 cc.0.006 0.09 0.04 0.57 129 1,998 0.09 1.38 0.34 5.21 8.20 2.097
0.09 0.47 0.14 0.70 67 335 0.25 1.26 1,467 1,235 August 19 to September 30, am-monium chlorid, 384 grams
0.01 0.52 0.02 0.85 130 4,810 0.04 1.63 6,075 5,975 Salyrgan, 2 cc.0.11 0.60 0.16 0.90 70 385 0.26 1.45 1,396 1.430
August 13 to September 22, am-monium chlorid, 364 grams
August 15, novasurol, 2 cc.
0.04 0.33 0.14 1.080.01 0.39 0.02 1.18 Novasurol 2 cc.0.09 0.58 0.11 0.670.05 0.36 59 4130.06 0.36 68 408 September 28 to 30, sodium chlorid,
24 grams0.08 0.38 102 S10 September 28 to October 1, increase in0.06 0.25 115 460 weight from 117.25 to 122.5 pounds
March 15 to 21, ammonium chlorid,75 grams
Novasurol, 2 cc.
0.18 0.24 0.05 0.67 226 3, 0781 January 22 to 31, ammonium chlorid,90 grams
0.07 0.21 .009 0.25 228 6,473 Novasurol, I cc.0.08 0.140 .05 0.83 163 2.645
0.001 0.01 0.05 0.15 70 309t February 25 to March 14, ammoniumchlorid, 146 grams
0.002 0.040 .02 0.41 157 3.773 March 18 to 22, ammonium chlorid,0.001 0.0101.07 0.27 _ _ 60 248 48 grams and novasurol, I cc.
Z Calculated from the estimations of sodium, potassium, calcium, and magnesium.
183

ACTION OF AI ONIUM CHLORID
=0 'utSAItis0(94
.= 'Ilu | oo 00 4 o0iad O0 'pl: °:U0ltpojp4H 00 (9
.- .- l_ ^
OT/N * 'sIuo0u-uI snld asvq pan,
1-Ul to v; 10;s o - u ) k-o eqw0 o mi Inu)o
v- c- V cNs
I00 (10Cooeso 4u'3 'S0)t~ ~U~Siou~ - )(spl9Usom) t.- In e u
uas 0%o 0-o0nmulo Jo .uaJ ..o U..x9d iuagopiu vmouiuy V- - V-
0o0 000s Ul) t (9osmua IUQBoP!Ullm ol,t. .0 o .
'uaSonmi sxOU .j (9 ) U) (9 U) t0 I0 0 00 0 0
t-. 4 t0U)0 ) 000 U)smo U 0 ( 00.oo
luago;qj lf l el
01/ r- in o 00 m o
'as,eq olwlioutlio UI)-1°t- in 4 U 0 t
L - - - -- - -9 00v-4--4 - -4 - -4 (911)4
.0 soe 40% U) 00 o) %t
V-4 C-~4) 4 to.CoN ON 8
os
stvl IMPS00 000t m00 00(90 e ) 00 0000S=stu~.i 'lJ0dS0 00 00 00 (U) - ) - 00OO OO O O O, O~O-- O
- C-O- 0000 0 00 0USlr C!o 00 0 00_ 0
si zmqdlns 3MV2°ulI . . .
009 00suruJ2 lp.ol; .U)...
(900 (90 0 0 0 00 %0Rd t- 10 %O t- to WI)
00U)Ujuao.zads luigm'p!oR[o |t°o
o lua: zad 'sa|unO -joA 'J4aMod Suunq-Iuo: 'p!xolp uoqjto
)luas2d 0OJe'tWUZt 'uaSoJliu saIfl 00
-4 U) u) 0 00 0%4n i).4A A
aaYsI e
C4
184
4.X
4)*
4)
4)
ob
4)
4.
4)
8 8 § 8 8 too § too too'33 louinlOA t- c-4 t- 00 t- k- 00
1. -t;
NORMANM. KEITH AND MARYWHELAN
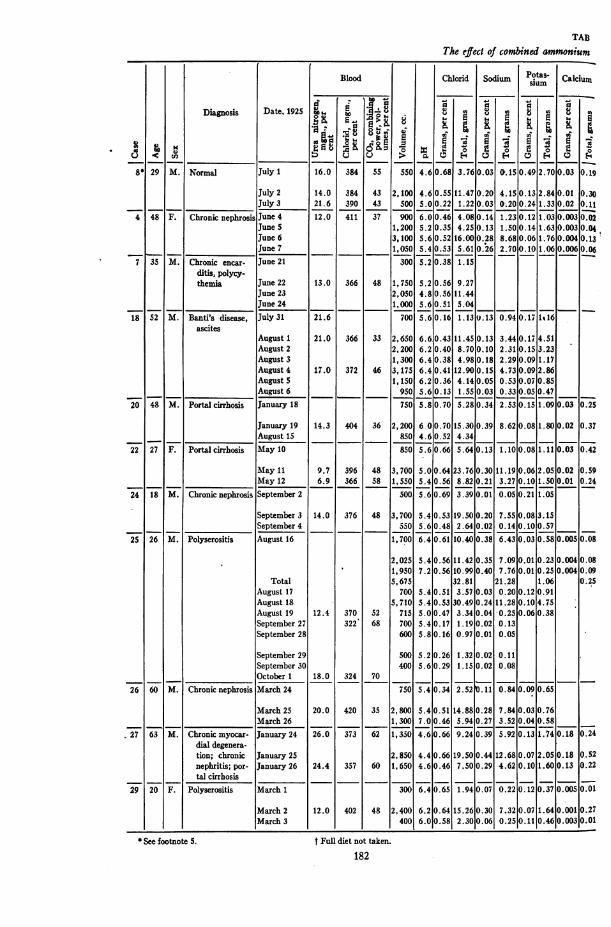
largest output of urine occurred in cases 22, 24 and 25 (table 14).In a period of between two and three weeks the actual volume ofurine excreted daily by each of these patients on days of diuresisonly, amounted to from 16.5 to 30 liters. In case 25 (table 14) theactual loss of weight during the five to six weeks of treatment was70 pounds (31.8 kgm.), and is mentioned to demonstrate the possi-bility of repeated marked diuresis in removing retained fluid fromthe body. On the other hand, two patients (cases 17 and 18, tables10 and 13, fig. 6), showed no diuresis when the plasma chlorid levelwas below normal. The amount of mercury excreted in the urineby each of four patients on days of diuresis, when undergoing thecombined treatment, was found to range from 48.5 to 81.3 per centof that injected. The hydrogen-ion concentration of the urine showedno characteristic changes, though minor variations occurred. Thechlorids excreted, except by patients with an abnormally low contentof plasma chlorid, always showed a sustained or increased concentra-tion, 0.36 to 0.70 gram per cent, and marked total increase. Themaximal output of chlorid occurred in case 25 (table 14), 32.8 gramsin twenty-four hours. Similarly, the sodium excreted showed anincreased or sustained concentration, 0.05 to 0.44 gram per cent, andlarge total increase. The evenly sustained excretion of chlorid andsodium at a high level, during this twenty-four-hour period is of note.In case 25 when the amount of chlorid excreted in one period oftwenty-four hours amounted to 32.8 grams the sodium excretedtotalled 21.3 grams. Thus, on that particular day of the diuresis,total amounts of chlorid and sodium were excreted in the propor-tions of 6:4, the ratio of the two ions in the salt, sodium chlorid.Weshall point out that such a ratio of the ions does not always occur.Potassium is usually excreted at a lower concentration during days ofdiuresis, but the total output is sustained or increased. The varia-tions in the excretion of potassium, particularly in relation to theexcretion of chlorid and sodium, are well exemplified during twoperiods of diuresis, August 16 and 18, in case 25 (table 14). In thetwo experiments the total volume of urine was the same and the totalchlorid differed by only 2 grams, whereas the sodium differed by 10grams and the potassium by 3.7 grams. Thus when the chloridexcreted was stationary, there was a fall of 10 grams in the sodium
185
186 ACTION OF AMMONIUMCHLORID
but an increase of 3.7 grams in the potassium. Whereas in the firstexperiment almost all the chlorid was excreted as sodium chlorid, inthe second the total excretion of sodium and potassium combineddid not furnish sufficient base for the large output of chlorid. The
&ovasuvol Zc.c.
4500'-4000 O X02jg3500|3000 A2
502500-
2000
44 4
62i ll T T TIIBIC 1 ff-T 111160Zi fllE1 Eil 1 I 1 M1 T111¢:clbL58 AilBllE1LlR91 11IILllI -tlII ]I 1 2112I 91uuifl31L11ILI11fIIl[l111111111561 ill
s11Bllisal111BElS4811llllMIIi11'1 9l zl 511- 1 u1II1TII1T111ITII. W 1Si - L >63000ttXtti4Wlllll-1uilITTlf44 IH. IIiI II III -I I l; II-II1lLX xlii
S00 I__LI - ]I 1 1 M .
Days1 23 4 5 6 7 8 9 10 11 aL 13 14 15 16 17 1819Weiglhe d low salt diet
OFluid, intake 12Urine output -.bodiy weight I Fixed base 0 AAmmoniADHydrochloric acidc U Sulphuric acid, Phosphoric acid
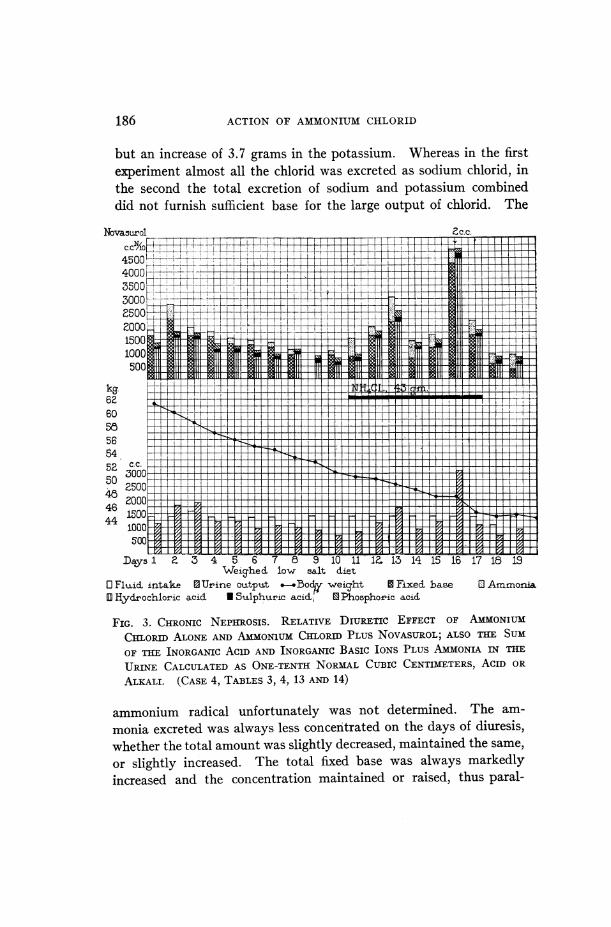
FIG. 3. CHRONIC NEPHROSIS. RELATIVE DIURETIC EFFECT OF AMMONIUM
CHLORID ALONEAND AMMO0NUMCHLORmPLUS NOVASUROL;ALSO THE SUM
OF THE INORGANIC AC1D AND INORGANIC BASIC IONS PLUS AMMONIA iN THE
URINE CALCULATEDAS ONE-TENTH NORMALCUBIC CENTIMETERS, AcID OR
ALKALI. (CASE 4, TABLES 3, 4, 13 AND 14)
ammonium radical unfortunately was not determined. The am-
monia excreted was always less concentrated on the days of diuresis,whether the total amount was slightly decreased, maintained the same,or slightly increased. The total fixed base was always markedlyincreased and the concentration maintained or raised, thus paral-
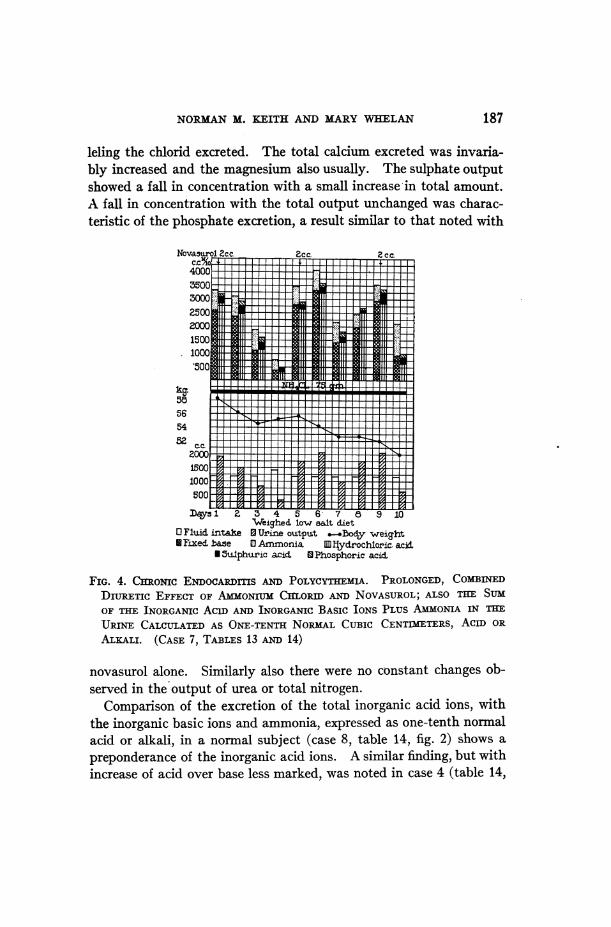
NORMANM. KEITH AND MARYWHELAN 187
leling the chlorid excreted. The total calcium excreted was invaria-bly increased and the magnesium also usually. The sulphate outputshowed a fall in concentration with a small increase in total amount.A fall in concentration with the total output unchanged was charac-teristic of the phosphate excretion, a result similar to that noted with
Novasurol 2c.c. cc2 c.
4000ll3! m l S
5004250
1000500
aqs2 3 4 5 6 7, 9 10Weighe4 low es.lt d.iet
OFl1iid. intle 0Urin outpu.t .-.od.y weiaht* Faxed. ase 0 Ammonia. [Wiydrochioric acid.
USulphuric acid WPhosphoric acid.
FIG. 4. CHRONIC ENDOCAuRDSAND POLYCYTTIEMIA. PROLONGED, COMBINEDDInUREIC EFFECT OF AMMONIUMCIrLoRID AND NOVASUROL;ALSO TIHE SUJMOF THE INORGANIC AC1D AND INORGANIC BASIC IONS PLUS AMMONIA IN THEEURINE CALCULATEDAS ONE-TENTH NORMWALCUBIC CENTIMETERS, ACID ORALKALI. (CASE 7, TABLES 13 AND 14)
novasurol alone. Similarly also there were no constant changes ob-served in the output of urea or total nitrogen.
Comparison of the excretion of the total inorganic acid ions, withthe inorganic basic ions and ammonia, expressed as one-tenth normalacid or alkali, in a normal subject (case 8, table 14, fig. 2) shows apreponderance of the inorganic acid ions. A similar finding, but withincrease of acid over base less marked, was noted in case 4 (table 14,
Salyx' an 1. c.C 2c.c.
54005000 C
4600 ---1
42001___i
3800t
1000
262100 F - 4la ooor T T__ 1_14S00r r T __T
600.
76 yl313325We±g1ied. low saiL diet
O FviAd intke 0 U.rine otitpu.t.-3o&y weight gIFixed. base70 Ammonia25 D Hydochloric acid
* Sulphtiric acid 0 Phosphox'ic aci~ NTratable acdity U 0r2a."nic acidsNIi4CL . total amoi±nt givren 31 inseven days ane.3Uin five days
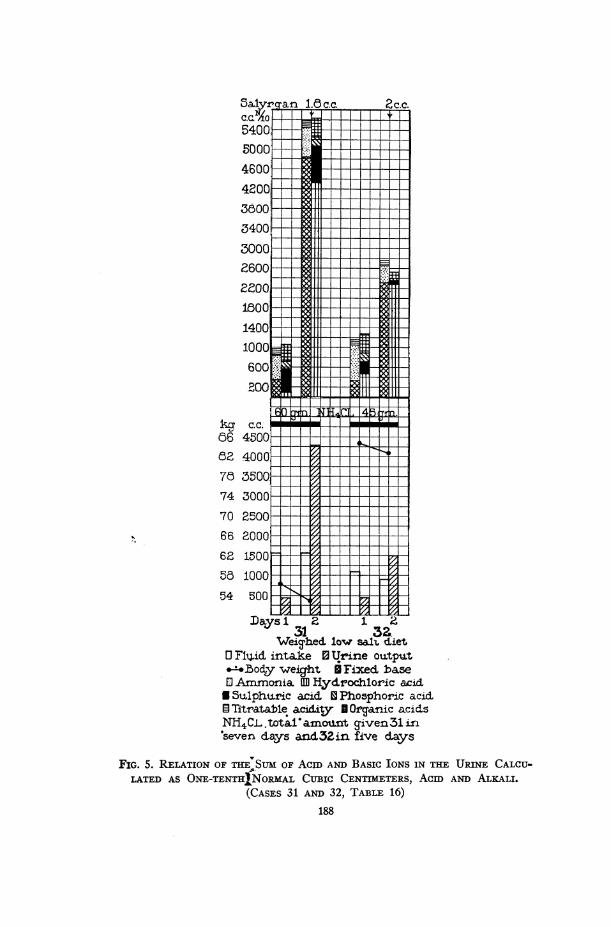
FIG. 5. RELATION OF THE,,S1T OF ACID AND BASIC IONS IN THE URINE CALCU_.LATED AS ONE-TENTHINORMWALCUBIC CENTDIETERS, ACID AND ALEALI.
(CASES 31 AND 32, TABLE 16)
188
NORMANM. KEITH AND MARYWHEILAN
__ _01/'S,1 ;}°L o co-;
01,3,100l 00
)- 0'"
)5) M0 1 C4 in0oD u)J I °)ON00 en
100'to- ~ ~ 0 00t a~a uaozod s |~ 3 1 4W 00~00C'70
.> 01/N. 'IflOtI 0.00 'noi
____ i,Td0l/N c33 oI ' " i00).) loao <Io 00o
0)e 0000'0nooo '
siJ' 100 00
.o |luat's=ur | "10o3 00ooool o
Hd C)Q1| o
aumRo U_0R 0*0*
iuojd lsmwj y1 MC!C!C
00 00
u smr. a2211 |ooT
W.4~ ~ ~ ~ 0'0 00t
1.4 C;Q00 O'-C'0
0'0 0 0'
00 00
Ed
tUfI;lunOA OL)
'0 4
0' ~ ~ 0
0)0
0)~~~~~
0~~~~0
0 Ia 0~~~~~C C
0 *~~~ 0b
xasI~Iza2vI~I
189
.A
*;
k.0
-oI
0
00.
-Q1
.0
0
0z
0
z0
'0
0
'A)
coU
'A
cis
a 0)
10 0'
cd
0. 2
es
co
o
0
'0
nEn
cd cd0 .n
P4C1.C¢
as;) I ell c14
ACTION OF AMMONIUMCHLORID
fig. 3). In case 7 (fig. 4) and case 24 (table 14), the total inorganicacid closely approximated the total basic ions. The phosphate ionwas calculated as one-tenth molar solution, it thereby having beenassumed that it had bound one equivalent of base.
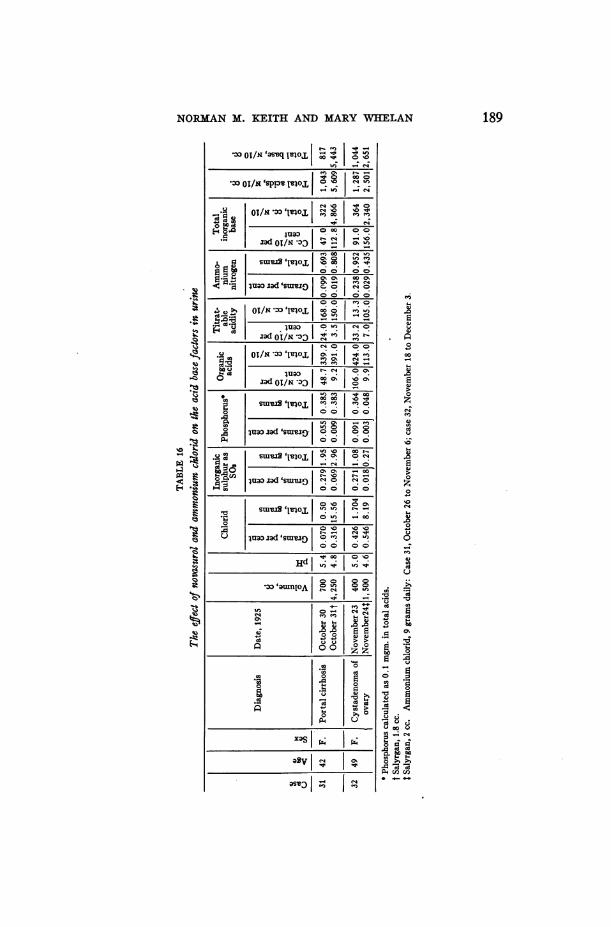
Two patients with marked ascites (case 31 and 32) with only anoccasional trace of albumin in the urine manifested definite diuresisafter the combined treatment. The titratable acid, and total or-ganic acids were determined in addition to the total inorganic acid,basic ions and ammonia (table 16 and fig. 5). The amount of thetotal acid excreted closely parallels that of the total base and thetitratable acid. These results again emphasize the importance ofthe specific excretion of chlorid along with fixed base when diuresis isproduced by the combined action of ammonium chlorid and organicmercury compounds.
OTHERDIURETICS
The urinary findings of two patients with diuresis after the use oftheocin, digitalis, and novasurol are recorded in table 17. In thediuresis produced by theocin and digitalis there is an increase inchlorid, sodium and fixed base similar to that produced by novasurol.Steyrer reported diuresis with increase in the chlorid excreted follow-ing the administration of digitalis to a patient with cardiac decom-pensation. Katsuyama and Pototzski noted that after caffein de-rivatives had been administered to rabbits, the chlorid and sodiumexcreted in the urine were increased. Bock found that, besidesthe increase in the chlorid and sodium, the potassium content of theurine was increased during caffein diuresis. Meinertz first reportedan increase in the chlorid excreted after the use of caffein derivativesin clinical cases of edema. In the single case in this series in whichall three diuretic agents were administered (case 14, table 17), nova-surol brought about the maximal excretion of chlorid, sodium andfixed base, although the amount of water excreted equaled that afterdigitalis. Jendrassik, in 1891,6 gave calomel to a series of patients
6 Jendrassik's advocacy of the use of calomel for its diuretic effect was basedon certain remarkable instances of diuresis obtained in cases of obstinate edemain Wagener's clinic in Budapest. The calomel treatment for edema was givena trial in numerous clinics at this period, but because of the coexisting diarrhea,and at times harmful effects on the kidney, its use as a diuretic was generallyabandoned.
190

o1/x *>0 lIeo'L o o~ t- o o>^ eF
_. e ~~~~N C1 N 00 C
0 C)~~~ 0 0 UO UO os
on _2 sa{~~~~~~~~~ UIS9Onm 00
ujuao ~ \jadls-m - U *gSW'lms mZm m N
S~~H
t ~~~ ~~SlIXXslO w (2 CN CN)
-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~--~ ~~~~~u dezeNou
0) 000 0
.b r ~~~~~o U Cso :eu
ce co .- 4
° Cdo+ e
n I S SX XARS I a
, n'e
o2s SI
191NORMWANM. KhEITH AND MARYWHEIIEAN
oS
_-4
Ce
1-
r .l
_ ;4
*;,
4-."
v
asvz | d,
*0 *0 .0CZ, (oi u
bototO boo
cn cn - V
4-,O-- O
^ ^ 2 28 @*Q@C)-s B j a B ~En
o o o ,
Eva - H H-H
5 EiIIt. 9!bo bo
t- 00 W-4
e e. .q . .4u u0 0(L) v
.0 4H H
.i. -.i
. -4
0 .(. (3u U
4i 4i,4) 0
.- ...4
p 1::.
ACTION OF AMONIUMCHLORID
with cardiac edema and noted a similar increase in the urinary ex-cretion of water and chlorids.
Comparative findings in the blood and urine. In three patients withmarked edema (cases 7, 22 and 24, table 14) who were given thecombined treatment a great diuresis occurred when the carbon dioxidcombining-power of the plasma was very slightly below the normal,48 per cent by volume, and the blood urea was within normal limits,but the plasma-chlorid level was definitely increased. Urinalysisrevealed: (1) acidity of the urine with little if any change in hydro-gen-ion concentration, from the previous day, (2) marked increase inchlorid, sodium and total fixed base, (3) a small but definite increasein ammonia, (4) very close balance between the total inorganic acidions, and those of the total inorganic base with ammonia included,and (5) in one case (case 22) an increase in the urea and total nitro-gen. The only distinct difference between these results and thoseof the normal subject (case 8, table 14) is the absence in the formercases of a distinct decrease in the alkali reserve of the plasma.
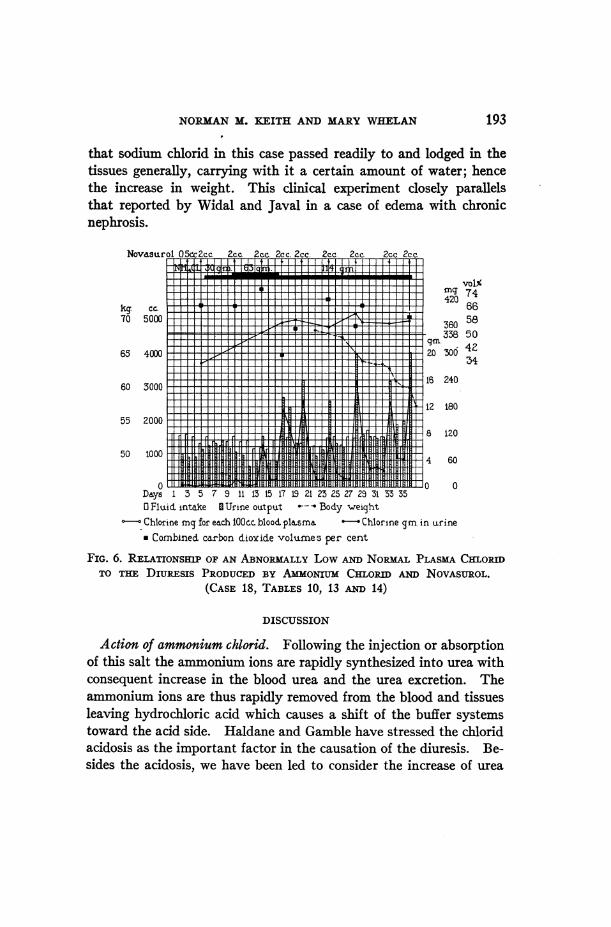
Cases 17 and 18 (tables 10 and 13) clearly show the close relation-ship between a low level of plasma chlorid and the consequent lowurinary excretion of chlorid and the diuretic action of novasurol.With the level in the plasma below normal and in the presence ofmarked edema, practically no excretion of chlorid occurred nor diddiuresis take place, but when the content was raised to the normallevel in case 18 by administering ammonium chlorid, chlorid, fixedbase and water were excreted in large amounts. There was no defi-nite relationship between decreased alkali reserve in the plasma andactive diuresis, the latter occurring when the former varied between37.5 and 76 per cent by volume (fig. 6).
The effect of sodium chlorid, as contrasted with that of ammoniumchlorid, in an organism which tends to retain fluid readily, is wellshown in case 25 (table 14). The patient's weight had been reducedfrom 84 to 53 kgm. (185 to 117 pounds) by the combined use ofammonium chlorid and novasurol. For three days he was given atotal of 24 grams of sodium chlorid, but the volume of the urine andthe chlorid, sodium, and fixed base excreted remained approximatelystationary, nor did the low plasma chlorid show any change. Thepatient gained 2.4 kgm. in weight. These results clearly indicate
192
NORMANM. BKEITH AND MARYWHELAN 193
that sodium chlorid in this case passed readily to and lodged in thetissues generally, carrying with it a certain amount of water; hencethe increase in weight. This clinical experiment closely parallelsthat reported by Widal and Javal in a case of edema with chronicnephrosis.
Novdsurol 05ccZcc. 2cc. 2cc. 2cc. 2cc. 2cc. 2cc. 2cc 2cc._11 d1 ti l It iL lSmI 1I It 1l
mq 74420 6kg. cr- IIT __X______X_66
_____ _ __ z-T _ ________=_-' m338 50
65 40002__r_
Fv8---l I1 16 240 360 3000
55 2000
50 1000
0~~~~~~~~~~~~~~~~~46
Days 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 350 Fluid into.ke I Urine output -- Body weightChlorine mg for each 00acc blood. plusma Chlorine gm. in urine* Combined carbon dioxide volumes per cent
FIG. 6. RELATIONSHIP OF AN ABNORMALLYLow A NORmALPLASMACHLORDTO THE DiuREsis PRODUCEDBY AMMONIUmCHLoRu AND NOVASUROL.
(CASE 18, TABLES 10, 13 mNm 14)
DISCUSSION
Action of ammonium chlorid. Following the injection or absorptionof this salt the ammonium ions are rapidly synthesized into urea withconsequent increase in the blood urea and the urea excretion. Theammonium ions are thus rapidly removed from the blood and tissuesleaving hydrochloric acid which causes a shift of the buffer systemstoward the acid side. Haldane and Gamble have stressed the chloridacidosis as the important factor in the causation of the diuresis. Be-sides the acidosis, we have been led to consider the increase of urea
ACTION OF AMMONIUMCHLORID
and the increase per se of chlorid in the blood and tissues, as possiblefactors in inducing diuresis.
If the resulting acidosis is the sole cause of the diuretic action ofammonium chlorid the ingestion of acids should have a similar effect.Begun, Herrmann and Miinzer studied the effect of the ingestion ofa 12.3 per cent solution of hydrochloric acid, 170 and 85 cc., respec-tively, in two normal men. During the period of acid ingestion theyobserved an increase in the excretion of chlorid, ammonia nitrogenand titratable acid in the urine. In one case there was no diuresis,and in the other the moderate increase in the volume of urine wasdue to an increase in the intake of water. One of our patients (case 30,table 15) was given, by mouth, 116 cc. of 10 per cent hydrochloric acid,in daily amounts varying from 8 to 48 cc. for four days. Thisamount of hydrochloric acid contains 11.3 grams chlorin, equal tothat in 16.5 grams of ammonium chlorid. The ingestion of theacid caused a very slight increase in the plasma chlorid and de-crease in carbon dioxid combining-power of the plasma. Studiesof the urine showed that the acid had no definite diuretic action.The excretion of chlorid and ammonia was increased. Sodiumand potassium showed some variation for it seemed that anincrease in soditum was accompanied by a decrease in potassiumand vice versa, while the total fixed base excretion remained con-stant. In this experiment the acid ingestion produced evidencesof acidosis without diuresis; however, the lack of increase in thevolume of the urine may have been due to the relatively small amountof acid ingested. These results with hydrochloric acid and the factthat the normal subject (case 8) developed acidosis without diuresisin three days after taking 31.5 grams of ammonium chlorid, indicateclearly that acidosis can be produced by chlorid without a parallelincrease in the volume of urine. Further experiments with otherinorganic acids as sulphuric and nitric acids, are needed to decidethe question as to whether such disturbance in the acid-base equi-librium towards the acid side in the tissues will cause liberation ofwater. In interpreting such experiments the possible specific actionof the anion must also be considered.
An abnormally low level of plasma chlorid with little or no chloridexcreted in the urine has been demonstrated in cases of severe renal
194
NORMANM. KEITH AND MARYWHELAN
insufficiency with and without demonstrable edema, lobar pneumonia,extensive superficial burns, war-gas poisoning, the toxic syndromeassociated with upper intestinal obstruction, and in two cases ofportal cirrhosis with edema and ascites in this series (cases 17 and18, table 10). In one of the latter (case 18) when the ascites andedema were extensive the ingestion of ammonium chlorid graduallyraised the lowered chlorid plasma threshold to the normal level andthus permitted an increase in excretion through the kidney.
At first glance the administration of a chlorid in large amountsto an organism literally loaded down with chlorids and water seemsmost illogical. However, it proved to be a life-saving measure inthe case just described. The exact manner in which the chloridcurrent was thus diverted from the general tissues toward the bloodstream and hence through the kidney is not easily explained. So-dium chlorid had no such effect in case 25 (table 14). On the otherhand, it augmented the current of chlorid and water toward the tis-sues. This simple clinical experiment shows the important relation-ship between retained sodium and retained water, as pointed out byMeyer and Blum. Besides the acidity factor, due to ammoniumchlorid, the status quo of the ions already present, and the specificaction of the chlorid ion itself must also play a part in causing suchan important shift in the movement of the body fluids.
Action of organic mercury compounds. A large percentage of theinjected mercury is excreted in the urine. Diuresis is accompaniedby an increased excretion of chlorid and fixed base. The latter ischiefly due to the increased elimination of sodium although potassiumin certain instances made up a considerable fraction. The urineexcreted the day following diuresis contained small amounts ofchlorid and sodium, but the average amount of potassium. Thelatter urinary findings are similar to those noted by Benedict duringstarvation, in which condition there is known to be a retention ofchlorid and sodium. There was no conclusive evidence during thisdiuresis of any marked change in the acid-base equilibrium of theblood or urine. Wedid note the absence of diuresis when the plasmachlorid content was well below the normal threshold. Further wehave been unable to show any constant changes in the compositionof the blood during the period when a large quantity of fluid must
195

ACTION OF AMMONIUMCHLORID
necessarily be liberated from the tissues and transported within theorganism. These negative findings are in harmony with those ofHaldane and Priestley in the blood of normal man after the ingestionof a large quantity of water. Greene and Rowntree had to give amuch larger amount of water to animals to produce changes in bloodconcentration. The liberation of ascitic fluid by organic mercurycompounds in cases of serious hepatic disease without any demon-strable renal impairment would lead one to believe that the specificaction was in the tissues remote from the kidneys. The specificaction in renal edema suggests an effect both on the general tissuesand kidneys. Experiments on the perfused isolated kidney mightbe crucial in determining the specific site of action.
Combined action of ammonium chlorid and organic mercury com-pounds. Following the combined administration of ammoniumchlorid and organic mercury compounds, marked diuresis was therule. The diuresis occurred more consistently than before, when thediuretic substances were given singly, and large accumulations offluid within the body were removed in a comparatively short period.Both substances have the same fundamental property of removingchlorid and fixed base as well as water from the organism, and theircombined action may thus be simply a cumulative one. Full diuresisdid occur when the blood plasma values for urea, chlorid and thecarbon dioxid combining-power were normal. However, even withthe normal plasma content of urea, chlorid and carbon dioxid com-bining-power, the urinary findings showed an increased excretion ofammonia which indicated definite acidosis. Such results point to apossible compensatory regulation of the acid-base equilibrium in theplasma when the tissues are still more acid in reaction than normal.Thus the acidosis produced by an acid-forming salt, after a longperiod of ingestion, may be closely analogous to a case of compen-sated acidosis in diabetes mellitus. In our experience novasurolalone did not cause a demonstrable change in the acid-base equilib-rium of the body, whereas when combined with ammonium chloridthere was always evidence, in the plasma or urine, of acidosis. Wehave thus demonstrated that ammonium chlorid can produce acidosisin the organism with or without diuresis; that novasurol can bringabout diuresis when there is no acidosis; and that the combined
196
NORMANM. KEITH AND MARYWHELAN
exhibition of ammonium chlorid and novasurol causes the mostmarked diuresis when acidosis is present. From such facts onemust conclude that an abnormal acid reaction in the tissues need notper se cause diuresis, but since it ocurs when the diuretic response ismost regular and marked, it must be considered a possible factor inliberating water from the tissues.
When diuresis follows the use of the caffein diuretics and digitalisthe urine shows a decided increase in the chlorid and fixed baseexcreted. If acidosis favors diuresis, the combined use of an acid-forming salt and theocin, for example, might cause diuresis after theo-cin alone has failed. Weare at present carrying out some experi-ments to test this possibility.
Urea has long been recognized as possessing diuretic propertiesand has been used as a therapeutic agent in different types of edema.Crawford and McIntosh have lately reported beneficial effects fromits use in cases of cardiac edema. Their results show clearly that theincreased elimination of water is accompanied by an increased ex-cretion of urea, but with only slight irregular increases in chlorids.Here then the mechanism of diuresis is quite distinct from that in-volved when ammonium chlorid or an organic mercury compound,caffein or digitalis, is administered. Similarly, hypertonic solutionsof glucose and saccharose have been employed experimentally toproduce marked diuresis and subsequent dehydration. Some of ourunpublished data indicate that, like urea, these sugars may notnecessarily cause a distinctly increased excretion of chlorid and fixedbase. From a practical therapeutic standpoint those substanceswhich remove water, chlorid, and fixed base from edematous patientsremove both the retained fluid and its inorganic dissolved constit-uents and therefore accomplish a more complete withdrawal thandiuretics of the urea and sugar type.
The removal of accumulated fluid, in cases of cardiac and nephriticedema, and in cases of ascites associated with disease of the liver, is afundamental problem in therapeutics. This excess fluid is eitherretained within the cells themselves, in the tissues or in the bodycavities. It may leave the cells, tissues or body cavities spontane-ously. Digitalis, the caffein derivatives, acid-forming salts, organicmercury compounds or urea may bring about diuresis when it does not
1.97

ACTION OF AMMONIUMCHLORID
occur spontaneously. The site of action of these diuretics would seemto be diffuse and not limited to one specific organ, the kidney. Theexact quantitative levels at which salts can pass from the edematoustissues into the blood stream and from the blood stream throughthe kidney may be affected by these drugs. That abnormal levelsdo exist in edematous conditions and can be altered has been wellshown in cases of this series. These diuretics may also act by per-mitting salts and water to pass through cells previously impervious,as the renal cell in oliguria and the peritoneal endothelium in the as-cites of cirrhosis of the liver.
SUMMARY
Following the administration of ammonium chlorid and its absorp-tion into the blood stream it has been shown experimentally that theammonia is quickly synthesized to urea. The liberated hydrochloricacid increases the chlorid content of the blood and tissues with theproduction of acidosis. Under the conditions of these experimentsdiuresis may or may not occur after the exhibition of an adequateamount of ammonium chloride. Ammonium chlorid in man causesan increased excretion of chlorid, fixed inorganic base (particularlysodium and potassium), ammonia, urea, and total nitrogen in theurine.
Organic mercury compounds cause an increased excretion of chloridand inorganic fixed base, without evidence in the blood or urine of achange in acid-base equilibrium. The basic ions, sodium and potas-sium, may be excreted independently. Diuresis occurs usually butnot always. Changes in the concentration of the blood are incon-stant and never marked in degree, even when the diuresis is great.Eighty-five per cent of the injected mercury can be recovered in thesubsequent twenty-four-hour specimen of urine.
Ammonium chlorid and organic mercury compounds used in com-bination produce diuresis when singly they fail to do so. Theycause acidosis, an increase in the chlorid content of the blood, and anincrease in the excretion of water, chlorid, fixed inorganic base, chieflysodium and potassium, and ammonia. In one case in which therewas a subnormal plasma chlorid level the combined drugs failed to
198
NORMANM. KEITH AND MARYWHELAN
produce diuresis. Ammonium chlorid was then given until thechlorids reached the normal level, when organic mercury producedsatisfactory diuresis.
The evidence at hand indicates that the activity of these diureticsis not limited to the kidney, but that extrarenal factors enter intoconsideration.
BIBLIOGRAPHY
1. Baird, N. M., Douglas, C. G., Haldane, J. B. S., and Priestley, J. G.: JourPhysiol., 1922-1923, lvii, xli. Ammonium Chloride Acidosis.
2. Begun, A., Herrmann, R., Miinzer, E.: Biochem. Ztschr., 1915, lxxi, 255-267.Uber Acidosis und deren Regulation im menschlichen Korper.
3. Bell, R. D., and Doisy, E. A.: Jour. Biol. Chem., 1920, xliv, 55-67. RapidColorimetric Methods for the Determination of Phosphorus in Urine andBlood.
4. Benedict, F. G.: Washington, D. C., Carnegie Institute, 1915, No. 203, p.285. A Study of Prolonged Fasting.
5. Bleyer, Leo: Klin. Wchnschr.., 1922, i, 1940-1942. Erfahrungen uber dieNovasurol-diurese.
6. Blum, L.: Verhandl. d. Kong. f. inn. Med., 1909, 122-126. Ueber die Rollevon Salzen bei der Enstehung von Oedenaen.
7. Bock, J.: Skandinav. Arch. f. Phys., 1911, xxv, 239-246. tJber die Auss-cheidung der Alkalimetalle bei der Purindiurese.
8. Bohn, Hans: Klin. Wchnschr., 1923, ii, no. 1, 352-353. ExperimentalleStudien uber die diuretische Wirkung des Novasurols.
9. Bollman, J. L., Mann, F. C., and Magath, T. B.: Amer. Jour. Physiol., 1924,lix, 371-392. Studies on the Physiology of the Liver. VIII. Effect ofTotal Removal of the Liver on the Formation of Urea.
10. Boothby, W. M., and Sandiford, Irene: Philadelphia, Saunders, 1920, 117pp. Basal Metabolic Rate Determinations.
11. Briggs, A. P.: Jour. Biol. Chem., 1922, liii, 13-16. A Modification of theBell-Doisy Phosphate Method.
12. Crawford, J. H., and McIntosh, J. F.: Arch. Int. Med., 1925, xxxvi, 530-541. The Use of Urea as a Diuretic in Advanced Heart Failure.
13. Crawford, J. H., and McIntosh, J. F.: Jour. Clin. Invest., 1925, 1, 333-358.Observatfons on the Use of Novasurol in Edema Due to Heart Failure.
14. Fiske, C. H.: Jour. Biol. Chem., 1922, li, 55-61. A Method for the Estima-tion of Total Base in Urine.
15. Folin, Otto: Jour. Biol. Chem., 1905, i, 150-159. The Determination ofSulphates and Total Sulphur in Urine.
16. Folin, Otto, and Bell, R. D.: Jour. Biol. Chem., 1917, xxix, 329-335. Appli-cations of a NewReagent for the Separation of Ammonia. I. The Col-orimetric Determination of Ammonia in Urine.
199

200 ACTION OF AMONTUMCHLORID
17. Folin, Otto, and Wu, Hsien: Jour. Biol. Chem., 1919, xxxviii, 81-110. ASystem of Blood Analysis.
18. Gamble, J. L., Blackfan, K. D., and Hamilton, Bengt: Jour. Clin. Invest.,1925, i, 359. A Study of the Diuretic Action of Acid Producing Salts.
19. Gillespie, L. J.: Amer. Chem. Soc. Jour., 1920, xlii, 742-748. ColorimetricDetermination of Titration Curves Without Buffer Mixtures.
20. Greene, C. H., and Rowntree, L. G.: Amer. Jour. Physiol., 1924, lxviii, 111.Changes in the Concentration of the Blood Following the Administrationof Excessive Quantities of Water.
21. Haden, R. L.: Jour. Lab. and Clin. Med., 1923, viii, 411-414. A Method forthe Determination of Hemoglobin.
22; Haldane, J. B. S.: Jour. Physiol., 1921, lv, 265-275. Experiments on theRegulation of the Blood's Alkalinity.
23. Haldane, J. B. S., and Priestley, J. G.: Jour. Physiol., 1915-1916, 1, 296-303. The Regulation of Excretion of Water by the Kidneys. I.
24. Harvey, S. C.: Arch. Int. Med., 1910, vi, 12-18. The Quantitative Deter-mination of the Chlorids in the Urine.
25. Jendrassik, E.: Deutsch. Arch. f. klin. Med., 1885-1886, xxxviii, 499-524.Das Calomel als Diureticum.
26. Jendrassik, E.: Deutsch. Arch. f. klin. Med., 1890-1891, xlvii, 226-288.Weitere Untersuchungen uiber die Quecksilberdiurese.
27. Katsuyama, K.: Ztschr. f. physiol. Chem., 1899, xxviii, 587-594. Ueberder Einfluss des Theins auf die Ausscheidung von Alkalien im Harne.
28. Katsuyama, K.: Ztschr. f. physiol. Chem., 1901, xxxii, 235-240. Ueberden Einfluss einiger harntreibender Mittel auf die Ausscheidung vonAlkalien im Harne.
29. Keith, N. M.: Amer. Jour. Physiol., 1924, lxviii, 80-96. ExperimentalDehydration: Changes in Blood Composition and Body Temperature.
30. Keith, N. M., Barrier, C. W., and Whelan, Mary: Jour. Amer. Med. Assn.,1925, lxxxv, 799-806. The Diuretic Action of Ammonium Chlorid andNovasurol in Cases of Nephritis with Edema.
31. Keith, N. M., Smith, Florence, and Whelan, Mary: Arch. Int. Med., 1926,xxxvii, 550-558. The Therapeutic Use of Diets Low in Water and MineralContent.
32. Keith, N. M., and Thomson, W. W. D.: Quart. Jour. Med., 1918, xi, 229-266. War Nephritis. A Clinical, Functional and Pathological Study.
33. Keith, N. M., and Whelan, Mary: Amer. Jour. Physiol., 1925, lxxii, 195-196.The Effect of Novasurol on the Composition of Blood and Urine.
34. Kramer, Benjamin, and Tisdall, F. F.: Jour. Biol. Chem., 1921, xlvi, 339-349. A Clinical Method for the Quantitative Determination of Potassiumin Small Amounts of Semm.
35. Kramer, Benjamin, and Tisdall, F. F.: Jour. Biol. Chem., 1921, xlvi, 467-473. A Simple Method for the Direct Quantitative Determination ofSodium in Small Amounts of Serum.
NORMANM. KEITH AND MARYWHELAN 201
36. Kramer, Benjamin, and Tisdall, F. F.: Jour. Biol. Chem., 1921, xlvii, 475-481. A Simple Technique for the Determination of Calcium and Mag-nesium in Small Amounts of Serum.
37. Lewis, D. S., and Rivers, T. M.: Bull. Johns Hopkins Hosp., 1916, xxvii,193-201. Chemical Studies on a Case of Bichloride Poisoning.
38. MacCallum, W. G., Lintz, Joseph, Vermilye, H. N., Leggett, T. H., andBoas, E.: Bull. Johns Hopkins Hosp., 1920, xxxi, 1-7. The Effect ofPyloric Obstruction in Relation to Gastric Tetany.
39. Meinertz, J.: Therap. Monatsh., 1904, xviii, 275-285. Versuche uberDiurese insbesondere iiber die Wirkung des Theocinnatrium aceticum.
40. Meyer, L. F.: Verhandl. d. Versamml. d. Gesellsch. f. Kinderh., 1909, xiv.41. Moraczewski, v. W.: Arch. f. path. Anat. u. Physiol. u. f. klin. Med., 1896,
cixvi, 424-452. Ueber den Chlor- und Phosphorgehalt des Blutes beikrankhaften Zustanden.
42. Miihling, Adolf: Miinchen. med. Wchnschr., 1921, lxviii, no. 2, 1447-1449.Studie uiber die diuretische Wirkungsweise von Quicksilber. Ausgefiihrtmit dem organischen Quecksilberpraparat Novasurol.
43. Nash, T. P., and Benedict, S. R.: Jour. Biol. Chem., 1921, xlviii, 463-488.The Ammonia Content of the Blood, and Its Bearing on the Mechanismof Acid Neutralization in the Animal Organism.
44. Nonnenbruch, W.: Munchen. med. Wchnschr., 1921, lxviii, ii, 1282-1283.Ueber die Wirkung des Novasurols auf Blut und Diurese.
45. Potozky, C.: Arch. f. d. ges. Physiol., 1902, xci, 584-594. Beitrage zurDiurese. Ueber den Einfluss einiger Diuretica auf die Kochsaltzausscheid-ung, insbesondere beim kochsalzarmen Thiere.
46. Priestley, J. G.: Jour. Physiol., 1915-1916, 1, 304-311. The Regulation ofExcretion of Water by the Kidneys. II.
47. Rowntree, L. G., Keith, N. M., and Barrier, C. W.: Jour. Amer. Med. Assn.,1925, lxxxv, 1187-1193. Novasurol in the Treatment of Ascites in HepaticDisease.
48. Saxl, P., and Heilig, R.: Wien. klin. Wchnschr., 1920, xxxiii, 943. Ueberdie diuretische Wirkung von Novasurol- und anderen Quecksilberinjek-tionen.
49. Smith, Mirlard: Jour. Biol. Chem., 1921, xlv, 437-447. The Determinationof Chlorides in Trichloro-acetic Acid Filtrates from Whole Blood andPlasma.
50. Steyrer: Beitr. z. chem. Physiol. u. Path., 1902, ii, 312. tlber osmotischeAnalyse des Hams.
51. Tisdall, F. F., and Kramer, Benjamin: Jour. Biol. Chem., 1921, xlviii, 1-12.Methods for the Direct Quantitative Determination of Sodium, Potassium,Calcium and Magnesium in Urine and Stools.
52. Underhill, F. P.: The Lethal War Gases. New Haven, Yale UniversityPress, 1920.
202 ACTION OF AMMONIUMCHLORID
53. Underhill, F. P., Carrington, G. L., Kapsinow, Robert, and Pack, G. T.:Arch. Int. Med., 1923, xxxii, 31-49. Blood Concentration Changes inExtensive Superficial Burns, and Their Significance for Systemic Treatment.
54. Van Slyke, D. D., and Cullen, G. E.: Jour. Biol. Chem., 1914, xix, 211-228.A Permanent Preparation of Urease, and Its Use in the Determinationof Urea.
55. Van Slyke, D. D., and Palmer, W. W.: Jour. Biol. Chem., 1920, xli, 567-585.Studies on Acidosis. XVI. The Titration of Organic Acids in Urine.
56. Van Slyke, D. D., and Stadie, W. C.: Jour. Biol. Chem., 1921, lix, 1-42.The Determination of the Gases of the Blood.
57. Whelan, Mary: Jour. Biol. Chem., 1925, lxiii, 585-620. The Effect ofIntravenous Injection of Inorganic Chlorides on the Composition of Bloodand Urine.
58. Widal, F., and Javal, A.: Bull. et m6m. Soc. de med. d. h6p. de Par., 1903,3 s., xx, 733-749. La cure de d6chloruration; son action sur l'oedeme,sur l'hydration et sur l'albuminurie a certaines periodes de la nephritee'pithe'liale.
59. Wong, San Yin: Jour. Biol. Chem., 1923, lv, 431-435. The Use of Persul-fate in the Estimation of Nitrogen by Folin's Direct Nesslerization Method.


![[XLS] · Web view1 7/2/2018 1000000 100000. 2 7/2/2018 100000 100000. 3 7/2/2018 200000 200000. 4 7/2/2018 100000 100000. 5 7/2/2018 1000000 500000. 6 7/2/2018 100000 100000. 7 7/2](https://static.fdocuments.in/doc/165x107/5e9a7b97e698772c56054a6e/xls-web-view-1-722018-1000000-100000-2-722018-100000-100000-3-722018-200000.jpg)
![[XLS] · Web view9/4/2014 100000000 100000 0 9/11/2014 500000 500000 0 9/23/2014 1900000000 5000000 0 9/27/2014 5000000 100000 0 9/30/2014 1750000000 50000000 0 9/1/2014 100000 100000](https://static.fdocuments.in/doc/165x107/5aa500977f8b9ab4788c9998/xls-view942014-100000000-100000-0-9112014-500000-500000-0-9232014-1900000000.jpg)











![[XLS]reports.mca.gov.inreports.mca.gov.in/Reports/MasterDataExcels/company... · Web view500000 500000 100000 100000 100000 100000 12/3/2015 100000 100000 3/3/2015 4/3/2015 100000](https://static.fdocuments.in/doc/165x107/5a9ec0867f8b9a0d158bcbbb/xls-view500000-500000-100000-100000-100000-100000-1232015-100000-100000-332015.jpg)


