
Chlamydiae
42
22/2/23 microbiology 8-year co urse 1 Chlamydiae
description
Â
Transcript of Chlamydiae

23/4/22 microbiology 8-year course 1
Chlamydiae

23/4/22 microbiology 8-year course 2
Biological Features Structure and chemical composition Developmental cycle Staining properties Antigens Growth and metabolism Characteristics of host-parasite relationship Classification

23/4/22 microbiology 8-year course 3
Structure and chemical composition
a nonreplicating, infect
ious particle called the
elementary body (EB)
an intracytoplasmic for
m called the reticulate
body (RB)

23/4/22 microbiology 8-year course 4
Structure and chemical composition

23/4/22 microbiology 8-year course 5
Structure and chemical composition The elementary body, which is covered by a rigid cell wall, contains a DNA ge
nome with a molecular weight of 66 X 107 (about 600 genes, one-quarter of th
e genetic information present in the DNA of Escherichia coli).
A cryptic DNA plasmid (7,498 base pairs) is also found. It contains an open re
ading frame for a gene involved in DNA replication.
the elementary body contains an RNA polymerase responsible for the transcri
ption of the DNA genome after entry into the host cell cytoplasm and the initiati
on of the growth cycle.
Ribosomes and ribosomal subunits are present in the elementary bodies. Thro
ughout the developmental cycle, the DNA genome, proteins, and ribosomes ar
e retained in the membrane-bound reticulate body.

23/4/22 microbiology 8-year course 6
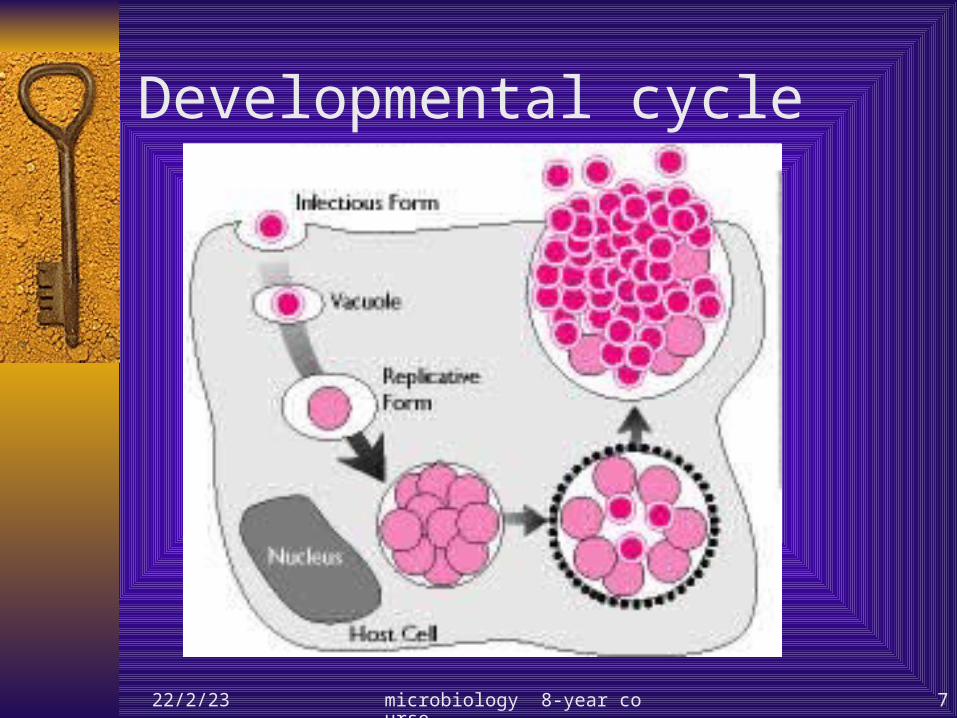
Developmental cycle
EBs attach to the microvilli of susceptive cells. Penetration into the host cell via endocytosis or pinocytosis and for
ming phagosomes Fusion of lysomes with the EB-containing phagosome are inhibited EBs reorganize into the metabolically active RBs. RBs synthesize their own DNA, RNA and protein but lack the neces
sary metabolic pathways to produce high-energy phosphate compounds.
Energy parasites. RBs replicate by binary fission and inclusion forms. RBs begin reorganizing into EBs. Cell ruptures and releasesthe infective Ebs. The developmental cycle takes 24~ 48 hours.
23/4/22 microbiology 8-year course 7
Developmental cycle
23/4/22 microbiology 8-year course 8
Staining properties
EBs stain purple with Giemsa stain—in contrast to the blue
of host cell cytoplasm.
RBs stain blue with Giemsa stain.
The Gram reaction of chlamydiae is negative or variable and
is not useful in identification.
Inclusions stain brightly by immunofluorescence ,with group-
specific,species-specific, or serovar-specific antibodies.

23/4/22 microbiology 8-year course 9
Antigens Group(fenus)-specific antigens:
– heat-stable LPS as an immunodominant component.– Antibody to these antigens can be detected by CF an
d immunofluorescence Species-specific or serovar-specific antigens
– Antigens are mainly outer membrane proteins(MOMP).
– Specific antigens can best be detected by immunofluorescence,particularly using monoclonal antibodies.

23/4/22 microbiology 8-year course 10
Growth and metabolism Unable to synthesize ATP and depend on the host cell for energy requirement
s.
Grow in cultures of a variety of eukaryotic cell lines
– McCoy cells are used to isolate chlamydiae
– C pneumoniae grows better in HL or Hep-2 cells.
– All types of chlamydiae proliferate in embryonated eggs,particularly in th
e yolk sac.
The replication of chlamydiae can be inhibited by many antibacterial drugs.
– Cell wall inhibitors (penicillins) result in the production of morphologicall
y defective forms but are not effective in clinical diseases.
– Inhibitors of protein synthesis (tetracyclines,erythromycins)are effective
in most clinical infections.
– C trachomatis strains synthesize folates and are susceptible to inhibition
by sulfonamides.

23/4/22 microbiology 8-year course 11
Classification
C trachomatis
– Biovar trachoma
– Biovar lymphogranuloma venereum
– Biovar mouse
C pneumoniae
C psittaci
C pecorum 兽类衣原体

23/4/22 microbiology 8-year course 12
Transmission
23/4/22 microbiology 8-year course 13
Pathogenicity
transmission Who is at risk Virulence factor Clinical syndromes Epidemiology immunity

23/4/22 microbiology 8-year course 14
Transmission
C. trachomatis
– Sexually transmitted;most frequent bacterial pathogen in
united states.
– Infected patients , who may be asymptomatic.
– Inoculation through break in skin or membranes.
– Passage to new born at birth.
– Trachoma spread to eye by means of contaminated hand,
droplets,clothing, and flies.
23/4/22 microbiology 8-year course 15
Transmission C. pneumoniae
– Person-to-person spread by inhalation of infectious aerosols.
– No animal reservoir
C. psittaci– Infection acquired by contact with infected bir
d or animal(may appear healthy).– Person-to-person infection very uncommon.

23/4/22 microbiology 8-year course 16
Who is at risk?
C. trachomatis– People with multiple sexual partners.– Homosexuals,who are more at risk for LGV.– Newborns born of infected mothers.– Reiter’s syndrome: young white men.– Trachoma:children,particularly those in crow
ded living conditions where sanitation and hygiene are poor.

23/4/22 microbiology 8-year course 17
Who is at risk?
C. pneumoniae– High prevalence of infections throughout life;m
ost infections asymptomatic.– Diease most common in adults.
C. psittaci– Disease most common in adults.– Occupations at increased risk include veterinari
ans,zookeepers,pet shop workers,and employees in poultry processing plants

23/4/22 microbiology 8-year course 18
Virulence factors
C. trachomatis– Intracellular replication,– prevention of phagolysosomal吞噬溶酶体 fusi
on, – survival of infectious EBs as a result of cross-li
nkage of membrane proteins.

23/4/22 microbiology 8-year course 19
Virulence factors
C. pneumoniae– Intracellular replication;– prevention of phagolysosome吞噬溶酶体 fusi
on;– ability to infect and destroy ciliated epithelial c
ells of respiratory tract,smooth muscle cells,endothelial cells,and macrophages;
– extracellular survival of infectious EBs.

23/4/22 microbiology 8-year course 20
Virulence factors
C. psittaci– Intracellular parasite,– prevention of phagolysosomal fusion,– survival of infectious EBs as result of cross-link
age of membrane proteins.

23/4/22 microbiology 8-year course 21
Clinical syndromes
C. trachomatis– Trachoma
– Adult inclusion conjunctivitis
– Neonatal conjunctivitis
– Infant pneumonia
– Ocular lymphogranuloma
venereum
– Urogenital infections
– Reiter’s syndrome
– Lymphogranuloma venereum
23/4/22 microbiology 8-year course 22
Clinical syndromes
C. pneumoniae– Bronchitis– Pneumonia– Sinusitis鼻窦炎– Pharyngitis– atherosclerosis动脉粥样硬化

23/4/22 microbiology 8-year course 23
Clinical syndromes
C. psittaci– psittacosis

23/4/22 microbiology 8-year course 24
Epidemiology Trachoma
– Trachoma is still prevalent in Africa and Asia, and sporadic cases occur all over the world.
– The disease flourishes in hot, dry areas where there is a shortage of water and where standards of hygiene are low.
– The agent is spread to the eyes by flies, dirty towels, fingers, or cosmetic eye pencils.
– The initial infection usually occurs in childhood, and the active disease eventually appears (mostly by 10 to 15 years of age). Trachoma may leave a residuum of permanent lesions that can lead to blindness.
– Chlamydia trachomatis also resides in the genital tract, cervix, and urethra of adults, and genital infection is spread sexually.

23/4/22 microbiology 8-year course 25
Epidemiology Lymphogranuloma venereum
– Lymphogranuloma venereum persists in the genital tract of infected persons.
– LGV is a chronic sexually transmitted disease caused by serotype L1,L2,and L3.
– Because C trachomatis is able to infect both the eyes and the urogenital tract, antitrachoma campaigns involving only ocular treatments are futile.
– It occurs sporadically in North America ,Australia ,and Europe but is highly prevalent in Africa, Asia and South America.
– Male homosexuals are the major reservoir of disease.– Acute LGV is seen more frequently in men,primarily because sym
ptomatic infection is less common in women.

23/4/22 microbiology 8-year course 26
Epidemiology
Chlamydia pneumoniae – Chlamydia pneumoniae spreads in human populations
by respiratory tract infections.
– It is the agent of atypical pneumonia in hospitalized patients as well as in young individuals with an acute respiratory disease.
– It has caused epidemics in Scandinavia.
– Studies of the prevalence of antibodies to C pneumoniae in humans around the world showed that it also prevails in Japan, Panama, and North America.

23/4/22 microbiology 8-year course 27
Epidemiology
Chlamydia psittaci– the cause of psittacosis in birds and occasionall
y in humans,– it is carried by wild and domestic birds, includi
ng poultry. – The severity of psittacosis in humans has been
considerably reduced by the susceptibility of C psittaci to antibiotics.

23/4/22 microbiology 8-year course 28
Immunity
C. trachomatis– Untreated infections tend to be chronic with per
sistence of the agent for many years.– Little is known about active immunity.– The coexistence of latent infection,antibodies,a
nd cell-mediated reactions is typical of many chlamydial infections.

23/4/22 microbiology 8-year course 29
Immunity
C. pneumoniae– Little is known about active or potentially prote
ctive immunity.– Prolonged infections can occur with C. pneumo
niae, and asymptomatic carriage may be common.

23/4/22 microbiology 8-year course 30
Immunity
C. psittacosis– Immunity in animals and humans is incomplete.– A carrier state in humans can persist for 10
years after recovery.– During this period, the agent may continue to
be excreted in the sputum.– Live or inactivated vaccines induce only partial
resistance in animals.– They have not been used in humans.

23/4/22 microbiology 8-year course 31
Diagnosis
Most diseases caused by the chlamydiae are diagnosed on the basis of their clinical manifestations.
Eye damage caused by C trachomatis is typical, as are the vesicles in the infected urogenital tract.
Diagnosis of pneumonitis requires laboratory testing
23/4/22 microbiology 8-year course 32
Diagnosis Chlamydia trachomatis can be identified microscopically i
n scrapings from the eyes or the urogenital tract. Inclusion bodies in scraped tissue cells are identified by iodine staining of glycogen present in the cytoplasmic vacuoles in infected cells.
To isolate the agent, cell homogenates that contain the chlamydial elementary bodies are centrifuged onto the cultured cells (e.g., irradiated McCoy cells).
After incubation, typical cytoplasmic inclusions are seen in the cells stained with Giemsa stain or iodine.

23/4/22 microbiology 8-year course 33
Diagnosis Staining with iodine can distinguish between inclusion bod
ies of C trachomatis and C psittaci, as only the former contain glycogen.
Each chlamydial agent can also be identified by using specific immunofluorescent antibodies prepared against either C trachomatis or C psittaci.
Homogenates or exudates of infected tissues also have been used to isolate the agent in the yolk sac of embryonated eggs.

23/4/22 microbiology 8-year course 34
Diagnosis
Sera and tears from infected humans are used to detect anti-Chlamydia antibodies by the complement fixation or microimmunofluorescence tests.
The latter is useful for identifying specific serotypes of C trachomatis.
Fluorescent monoclonal antibodies are used to stain C trachomatis elementary bodies in urethral and cervical exudates.

23/4/22 microbiology 8-year course 35
Diagnosis It is possible to diagnose C trachomatis in tissue biopsy sp
ecimens by in situ DNA hybridization with cloned C trachomatis DNA probes.
DNA from C trachomatis isolates can be examined by restriction endonuclease analysis.
The DNA cleavage pattern of C trachomatis isolates differs greatly from that of DNA from C psittaci isolates.
DNAs of the agents of trachoma and lymphogranuloma venereum differ in their cleavage patterns, and this allows identification of the biovars

23/4/22 microbiology 8-year course 36
Diagnosis Chlamydia pneumoniae DNA has 10 percent homology
with C trachomatis or C psittaci; C pneumoniae isolates have 100 percent homology. Chl
amydia pneumoniae isolates can be diagnosed by hybridization with a specific DNA probe that does not hybridize to other chlamydiae.
Two additional serologic tests are in use: the microimmunofluorescence test with C pneumoniae-
specific elementary body antigen, and the complement fixation test, which measures Chlamydia antibodies.
23/4/22 microbiology 8-year course 37
Prevention and control C. trachomatis
– It is difficult to prevent C. trachomatis infections because the population with endemic disease frequently has limited access to medical care.
– It is difficult to eradicate the disease within a population and to prevent reinfections.
– Chlamydia conjunctivitis and genital infections are prevented through the use of safe sexual practices and the prompt treatment of symptomatic patients and their sexual partners.

23/4/22 microbiology 8-year course 38
Prevention and control
C. pneumoniae– Treatment is with tetracycline or erythromycin.– Failures are common.– Retreament maybe required.

23/4/22 microbiology 8-year course 39
Prevention and control
C. psittaci– Tetracycline or erythromycin is used for treatm
ent.– Infections should be controlled in domestic and
imported pet birds using chlortetracycline.

23/4/22 microbiology 8-year course 40
Treatment C. trachomatis
– Ocular,genital & respiratory infections– In endemic areas,sulfonamides,erythromycins,and tetracyclines have
been used to suppress chlamydiae and bacteria that cause eye infections.
– Genital infections & inclusion conjunctivitis– It is essential that chlamydial infections be treated simultaneously in b
oth sex partners and in offspring to prevent reinfection.– tetracyclines are commonly used in non pregnant in fected females.– Erythromycin is given to pregnant women.
– LGV– The sulfonamides and tetracyclines have been used with food results
especially in the early stages.– Little is known about active immunity.

23/4/22 microbiology 8-year course 41
Treatment
C. pneumoniae– It is susceptible to the macrolides and tetracyclines and
to some fluoroquinolones.
– Treatment with doxycycline, azithromycin,or clarithromycin appears to benefit patients with the infection.
– The symptoms may continue after routine courses of therapy with erythromycin,doxycyclinbe, or tetracycline.
– These drugs should be given for 10- to 14-day courses.

23/4/22 microbiology 8-year course 42
Treatment C. psittacosis
– tetracyclines. Are the drugs of choice and should be continued for 10 days.
– It may not free the patient from the agent.– Intensive antiviotic treament may also delay the
normal course of antibody development.– Strains may become drug-resistant.– With antibiotic therapy the mortality rate is 2 ﹪
or less.


















