
Chiva today 2014
42
CHIVA TODAY 2014 From theory to scientific evidence C. Franceschi (Paris France Cremona ITALY)
-
Upload
claude-franceschi -
Category
Health & Medicine
-
view
197 -
download
1
Transcript of Chiva today 2014

CHIVA TODAY 2014From theory to scientific evidence
C. Franceschi (Paris France Cremona ITALY)

To raise new questions, new possibilities, to To raise new questions, new possibilities, to regard old problems from a new angle, regard old problems from a new angle, requires creative imagination and marks real requires creative imagination and marks real advance in scienceadvance in science
Albert EinsteinAlbert Einstein

CHIVA cure-Conservative -Hemodynamic-Venous Insufficiency -Ambulatory Treatment


CHIVA’S STORY
-An hemodynamic pattern proposed 26 years ago.
-Proved 20 years later by Controlled Randomized Trials
and COCHRANE review

Friedrich TRENDELENBURG 1890
Benjamin BRODIE 1846
Tomaso RIMA 1775- 1843
Everard HOME 1799
Ambroise PARE 1509-1590
CHIVA Precursors
Georg Clemens PERTHES 1900
William HARVEY 1578-1657

1788-1899: Ligation of Saphena Vein
Trendelenburg
1988: CHIVA
Varicocentric
Ablative
1906 Stripping Mayo Babcok
1947 Sclerosis
2000 RF, Laser, Foam
Short Story
90 years 90 years blackoutblackout
Varicocentric Ablative
Emodinamicocentric Conservative

19771986
CHIVA was possible thanks to diagnosis improvement based on Ultrasound Duplex Scan
1988
2009

HEMODYNAMIC CONCEPTS PUBLISHED
IN 1988.
Varicose veins and trophic changes are not the cause but the effect of overloading pressure/flow
The consequent treatment consists of correcting this hemodynamic impairment in order to collapse
the varicose veins, restore the tissue health and reduce the varicose recurrence thanks to
overloading flows disconnection and draining veins conservation, included varicose.

HEMODYNAMIC CONCEPTS PUBLISHED
IN 1988.
AND BY THE WAY preservation of the
saphena veins, possibly vital in case of necessary arterial
bypass

HEMODYNAMIC CONCEPTS
1-Dynamic Fractioning of the Hydrostatic Pressure
2-Closed and Open Shunts
3-Vicarious Varicose Recurrence
4-Saphena Conservation for Future Arterial By-pass
5-Anato-functional Mapping.

i P
o P
p P
c P
s g P
ig P
i P
o P
p P
c P
gs P
g s P
20032003
Identification of pelvic leak points: Inguinal (IP) Perinaeal (PP), Clitorudian (CP) Obturator OP) Gluteal ( SGP and IGP)
Franceschi C, Bahnini A. Treatment of lower extremity venous insufficiency due to pelvic leak points in women. Ann Vasc Surg. 2005 Mar;19(2):284-8
ANATOMIC LOCATION OF PELVIC LEAK POINTS

Hemodynamic aspects of Venous Insufficiency
Diagnosis and Treatment

Signs: Edema, Varices, trophic changes, Ulcer
ONE cause
TransMural Pressure Excess
TMP
Venous Insufficiency Disease

TMP
=Pressure
Extra-Venous Extra-Capillary
Pressure Endo-VenousEndo-Capillary
minus

TPM is increased by
1-Hydrostatic Pressure Overloading ( gravitational)
Causes
Valve Incompetence, flow block
2-Residual Pressure Overloading ( micro-circulation)
3-M.Pump Pressure Overloading ( shunts)

CHIVA cure :
1/Hydrostatic Pressure column fractionning : restore the dynamic fractionning of the hydrostatic column during walking
2/Closed and deviated shunts disconnection : suppresses flow/pressure overloading supplied by the VM Pump during walking
3/Draining Veins conservation: avoids residual pressure excesses responsible for spider veins and varicose recurrence
4/ Venous Capital Conservation for future possible need of arterial by-pass

CHIVA doesn’t depend on the varicose veins
evolution, downwards or upwards
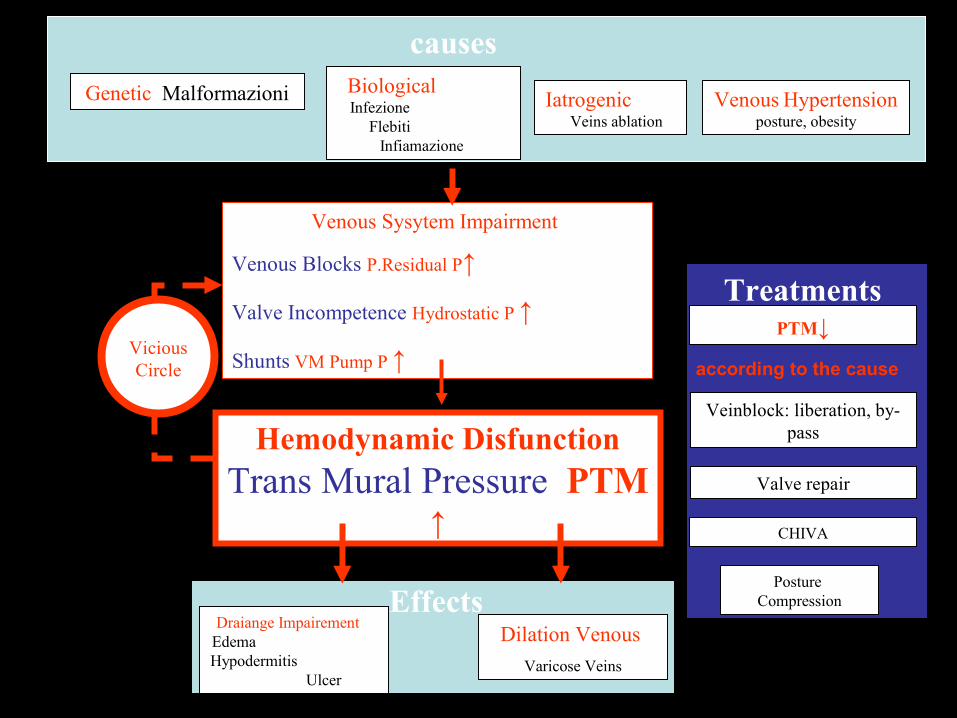
Treatments
Venous Sysytem Impairment
Venous Blocks P.Residual P↑
Valve Incompetence Hydrostatic P ↑
Shunts VM Pump P ↑
Hemodynamic Disfunction Trans Mural Pressure PTM
↑
causes
Genetic Malformazioni Biological Infezione
Flebiti Infiamazione
Iatrogenic Veins ablation
EffectsDilation Venous
Varicose Veins
Draiange Impairement Edema Hypodermitis
Ulcer
Vicious Circle
PTM↓
Posture Compression
Veinblock: liberation, by-pass
Valve repair
CHIVA
Venous Hypertension posture, obesity
according to the cause

Varico Centric Hemodinamico Centric
TMP REDUCTION TMP REDUCTION
P ExtraVenous Pressure IncreaseP ExtraVenous Pressure Increase
-Compression-Compression
IntraVenous Pressure DecreaseIntraVenous Pressure Decrease
-Posture-Posture
-Liberation-Liberation
VEINS ABLATIONVEINS ABLATION
-Phlebectomy-Phlebectomy
-Sclerosis-Sclerosis
-Laser-Laser
-Radio Frequency -Radio Frequency
IMPAIRS the DRAINAGE IMPAIRS the DRAINAGE Tissue sufferingTissue suffering
Vicarious Recurrence Vicarious Recurrence
Destruction of the VENOUS Destruction of the VENOUS CAPITALCAPITAL
CHIVACHIVA
-HP Fragmentation -HP Fragmentation -Shunt Disconnection-Shunt Disconnection--Drainage respect Drainage respect -Venous capital preservation-Venous capital preservation
TREATMENTS

OOSSOO
SFSF
vv aa
MM
Flow/pressurFlow/pressure overloade overload
Vicarious Vicarious flowflow
Fistole Fistole Artéro-Artéro-Venosus Venosus fistulefistule
Closed Closed shuntshunt
Venous Venous malformationmalformation
TMPTMP increases with flow and pressure overload due to increases with flow and pressure overload due to various causesvarious causes
Hydrostatic Hydrostatic Pressure Pressure excessexcess

CHIVA is not only avaricose treatment
CHIVA is also the treatment of the cause of the venous insuficiency
i.e the TMP excess.
When TMP is reduced to normal, all signs and symptoms are cured: Varicose veins, Edema, Hypodermitis, Ulcer

CHIVA doesn’t depend on the direction of the
varicose progression , downwards or upwards

CHIVA cure
- EVIDENCE BASED MEDICINE
- Randomized Controlled Trials

1- Varicose Vein Surgery Stripping versus the CHIVA method: a Randomized Controlled Trial Josep oriol
Pares and al Annals of Surgery * Volume 251, Number 4, April 2010 [ISRCTN52861672]. [ISRCTN52861672]. (international (international
standard randomised controlled trial number )www.controlled-trials.comstandard randomised controlled trial number )www.controlled-trials.com
2- Minimally Invasive Surgical management of primary venous Ulcer vs. Compression Treatment: a randomized Clinical Trial
P.Zamboni and allEur J vasc Endovasc Surg 00,1 6 (2003)
3- Clinical and random study comparing two, surgical techniques for varicose vein treatment : immediate results
Iborra and allAngiologia 2000:6, 253-258
4-Varicose Vein Stripping vs Haemodynamic Correction (CHIVA): a Long Term Randomised Trial.
Carandina, C. and al.Eur J Vasc Endovasc Surg xx, 1e8 (2007)
doi:10.1016/j.ejvs.2007.09.011

1- Varicose Vein Surgery Stripping versus the CHIVA method: a Randomized Controlled Trial Josep oriol
Pares and al Annals of Surgery * Volume 251, Number 4, April 2010 [ISRCTN52861672]. [ISRCTN52861672]. (international (international
standard randomised controlled trial number )www.controlled-trials.comstandard randomised controlled trial number )www.controlled-trials.com
2- Minimally Invasive Surgical management of primary venous Ulcer vs. Compression Treatment: a randomized Clinical Trial
P.Zamboni and allEur J vasc Endovasc Surg 00,1 6 (2003)
3- Clinical and random study comparing two, surgical techniques for varicose vein treatment : immediate results
Iborra and allAngiologia 2000:6, 253-258
4-Varicose Vein Stripping vs Haemodynamic Correction (CHIVA): a Long Term Randomised Trial.
Carandina, C. and al.Eur J Vasc Endovasc Surg xx, 1e8 (2007)
doi:10.1016/j.ejvs.2007.09.011

0
10
20
30
40
50
60
70
464 465 459 453 458 457
6m 12m 24m 36m 48m 60m
%
Ph-M
Ph-ED
TC
St -MC
St -ED
TC
5ans. 550 Patients
Up to 18 months: NO differenceUp to 18 months: NO difference
Difference increases with time after 2 yearsDifference increases with time after 2 years
CHIVA
Stripp. Duplex guided
Stripp. Clinical
5 years follow up : Recurrence rate: 5 years follow up : Recurrence rate: CHIVA vs stripping CHIVA vs stripping

0
10
20
30
40
50
60
70
464 465 459 453 458 457
6m 12m 24m 36m 48m 60m
%
Ph-M
Ph-ED
TC
St -MC
St -ED
TC
5ans. 550 Patients
Duplex Guided Vs Clinical : NO differenceDuplex Guided Vs Clinical : NO difference
Duplex is USLESS for strippingDuplex is USLESS for stripping
CHIVA
Stripp. Duplex guided
Stripp. Clinical
5 years follow up : Recurrence rate: 5 years follow up : Recurrence rate: CHIVA vs stripping CHIVA vs stripping

1- Varicose Vein Surgery Stripping versus the CHIVA method: a Randomized Controlled Trial Josep oriol
Pares and al Annals of Surgery * Volume 251, Number 4, April 2010 [ISRCTN52861672]. [ISRCTN52861672]. (international (international
standard randomised controlled trial number )www.controlled-trials.comstandard randomised controlled trial number )www.controlled-trials.com
2- Minimally Invasive Surgical management of primary venous Ulcer vs. Compression Treatment: a randomized Clinical Trial
P.Zamboni and allEur J vasc Endovasc Surg 00,1 6 (2003)
3- Clinical and random study comparing two, surgical techniques for varicose vein treatment : immediate results
Iborra and allAngiologia 2000:6, 253-258
4-Varicose Vein Stripping vs Haemodynamic Correction (CHIVA): a Long Term Randomised Trial.
Carandina, C. and al.Eur J Vasc Endovasc Surg xx, 1e8 (2007)
doi:10.1016/j.ejvs.2007.09.011

KAPLAN-MEIR ESTIMATIONKAPLAN-MEIR ESTIMATION1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
00
1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
0000 250250 500500 500500750750 10001000
TIME (days)TIME (days)
CHIVACHIVA
compressioncompression
Minimally invasive surgical management of primary venous Minimally invasive surgical management of primary venous ulcers vs. compression treatment: a randomized clinical trial.. ulcers vs. compression treatment: a randomized clinical trial.. Zamboni Pand al A. Zamboni Pand al A. EJ V E S. 2003EJ V E S. 2003

1- Varicose Vein Surgery Stripping versus the CHIVA method: a Randomized Controlled Trial Josep oriol
Pares and al Annals of Surgery * Volume 251, Number 4, April 2010 [ISRCTN52861672]. [ISRCTN52861672]. (international (international
standard randomised controlled trial number )www.controlled-trials.comstandard randomised controlled trial number )www.controlled-trials.com
2- Minimally Invasive Surgical management of primary venous Ulcer vs. Compression Treatment: a randomized Clinical Trial
P.Zamboni and allEur J vasc Endovasc Surg 00,1 6 (2003)
3- Clinical and random study comparing two, surgical techniques for varicose vein treatment : immediate results
Iborra and allAngiologia 2000:6, 253-258
4-Varicose Vein Stripping vs Haemodynamic Correction (CHIVA): a Long Term Randomised Trial.
Carandina, C. and al.Eur J Vasc Endovasc Surg xx, 1e8 (2007)
doi:10.1016/j.ejvs.2007.09.011

Clinical and random study comparing two, surgical techniques for varicose vein treatment : immediate results
Iborra and allAngiologia 2000:6, 253-258
immediate results: NO DIFFERENCE In accordance with O.Pares where
CHIVA vs Stripping difference starts after the 18th month!

1- Varicose Vein Surgery Stripping versus the CHIVA method: a Randomized Controlled Trial Josep oriol
Pares and al Annals of Surgery * Volume 251, Number 4, April 2010 [ISRCTN52861672]. [ISRCTN52861672]. (international (international
standard randomised controlled trial number )www.controlled-trials.comstandard randomised controlled trial number )www.controlled-trials.com
2- Minimally Invasive Surgical management of primary venous Ulcer vs. Compression Treatment: a randomized Clinical Trial
P.Zamboni and allEur J vasc Endovasc Surg 00,1 6 (2003)
3- Clinical and random study comparing two, surgical techniques for varicose vein treatment : immediate results
Iborra and allAngiologia 2000:6, 253-258
4-Varicose Vein Stripping vs Haemodynamic Correction (CHIVA): a Long Term Randomised Trial.
Carandina, C. and al.Eur J Vasc Endovasc Surg xx, 1e8 (2007)
doi:10.1016/j.ejvs.2007.09.011

1,75
1,8
1,85
1,9
1,95
2,05
2,1
2,15
2,2
2,25
2
P<0.038
Stripping
CHIVACHIVA
BEST SCORESBEST SCORES
18%
35%
0
5
10
15
20
25
30
35
CHIVA Stripping
RECIDIVE1O years follow up : Recurrence rate: 1O years follow up : Recurrence rate:
CHIVA vs stripping CHIVA vs stripping Objective evaluation
S.Carandina, and alS.Carandina, and al. . E J V E Surg. 2008E J V E Surg. 2008
CHIVAStripping

1 COCHRANE REVIEWCHIVA vs Stripping
Less recurrences, less complications
Bellmunt-Montoya S, Escribano JM, Dilme J, Martinez-Zapata MJ. CHIVA method for the treatment of chronic venous insufficiency. Cochrane Database of Systematic Reviews 2012 , Issue 2 . Art. No.: CD009648. DOI:10.1002/14651858.CD009648 .

EVIDENCES Level Grade meta-analyses de RCT
Ia A Strong
Au moins un RCT Ib
Au moins une étude clinique bien conduite sans randomisation
IIa B Mid
Au moins un autre type d’étude clinique bien programmé et quasi expérimental
IIb
Au moins un autre type d’étude clinique bien programmée et non expérimentale
III
Opinions de comités d’experts ou expérience d’autorités reconnues
IV C Weak
Other venous technics at this level????
Stripping still Gold standard? CHIVA ?
CHIVA (4 RCT)CHIVA (4 RCT)
+ Cochrane Library REVEW

Retrospective study CHIVA vs LASER.Chan, C.-Y.a , Chen, T.-C.b , Hsieh, Y.-K.a , Huang, J.-H.c Retrospective comparison of clinical outcomes between endovenous laser and saphenous vein-sparing surgery for treatment of varicose veins (2011) World Journal of Surgery, 35 (7), pp. 1679-1686.Conclusion: The CHIVA patients had less pain postoperatively and a significantly higher sclerotherapy-free period compared to patients in the EVL group.

GUIDELINES• The care of patients with varicose veins and associated chronic venous
diseases: Clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum
• Peter Gloviczki, MD, and al. JVS 2011 • Results with preservation of the saphenous vein. Results with CHIVA. Two
RCTs188,191 compared standard treatment(compression or high ligation, stripping, and phlebectomy) with CHIVA approaches with specific anatomic patterns of reflux (types I and III shunts). For the specific venous anatomy evaluated in these trials, such techniques were better than compression in preventing ulcer recurrence and were at least equivalent to stripping of varicose veins. Although the first two RCTs focused on a small group of patients with varicose veins, the trial of Pares et al deserves credit for including the full spectrum of patients with primary varicose veins. CHIVA is a complex approach, and a high level of training and experience is needed to attain the results presented in this RCT. However, the results achieved by a few outstanding interventionists does not support offering this procedure to all practitioners.Although CHIVA has called attention to the importance of directing surgical procedures toward the patient’s venous anatomy and function, it still requires considerable education of venous interventionists willing to learn this approach.

CHIVA requires considerable education of venous interventionists willing to learn this approach” (Peter Gloviczki, MD, and al. JVS 2011) because it relies on new hemodynamic concepts of the venous pathophysiology and a proper DUS assessment method. CHIVA performed by who doesn’t know enough about them is not CHIVA and leads to failure as a study demonstrated it (Milone M, Salvatore G, Maietta P, Sosa Fernandez LM, Milone Recurrent varicose veins of the lower limbs after surgery. Role of surgical technique (stripping vs. CHIVA) and surgeon's experience.F. G Chir. 2011 Nov-Dec;32(11-12):460-3).So, conservation is possible in all the patients and CHIVA

…..today, treatments are performed in accordance with the evidence based medicine supplied by Randomized Controlled Trials ….and after a comprehensive information and consent of the patient.
President of Medicine Academy

CHIVA preserves the GSV for future arterial bypassOptimal management of infrainguinal arterial occlusive diseaseAuthors: Pennywell DJ, Tan TW, Zhang WWFull text: available on http://www.dovepress.com/article_18926.t34346121Risk factors:Age is the most important, nonmodifiable risk factor for PAD, with a prevalence of 0.9% in people under age 50 and 23.2% in people over the age of 80.1Open reconstruction:The most important determinant of success of an Infrainguinal lower extremity bypass (LEB) is the type and quality of conduit selected.2,17,52 Autogenous vein is superior to synthetic graft as conduit for LEB,2,53–55 and the great saphenous vein (GSV) is superior to other autologous alternatives.2,55,56 An essential step in preoperative planning is evaluation of the GSV with duplex mapping and identification of alternative vein conduits, if needed. An ideal vein conduit should be soft, compressible, at least 3 mm in diameter, and should not be calcified or sclerotic. If the ipsilateral GSV is unsuitable or unavailable, the contralateral GSV should be used.ConclusionOpen infrainguinal bypass remains the gold standard for revascularization in CLI, especially for patients at appropriate surgical risk and with suitable bypass conduit.

Is it professional not to give the best scientifically proved treatment to the patient?
Is it honest to tell the patient his saphena wouldn’t be usefull in case of arterial by-pass necessity?


















