
Chiranjeevi Maternal Health Financing Issues and Options Dr Amarjit Singh Commissioner Health &...
35
Chiranjeevi Chiranjeevi Maternal Health Maternal Health Financing Issues Financing Issues and Options and Options Dr Amarjit Singh Dr Amarjit Singh Commissioner Health & Commissioner Health & Secretary Family Welfare Secretary Family Welfare Government of Gujarat Government of Gujarat
-
Upload
alison-watts -
Category
Documents
-
view
218 -
download
0
Transcript of Chiranjeevi Maternal Health Financing Issues and Options Dr Amarjit Singh Commissioner Health &...

Chiranjeevi Chiranjeevi
Maternal Health Maternal Health Financing Issues Financing Issues
and Optionsand Options
Dr Amarjit SinghDr Amarjit SinghCommissioner Health & Commissioner Health &
Secretary Family Welfare Secretary Family Welfare Government of GujaratGovernment of Gujarat

Lessons from HSRsLessons from HSRs
Steer don’t rowSteer don’t row
Finance rather than directly provideFinance rather than directly provide
Explore options for PPPExplore options for PPP
Regulate quality, cost-effectivenessRegulate quality, cost-effectiveness
Protect the marginalised groupsProtect the marginalised groups

Every Minute...
Maternal Death Watch-Maternal Death Watch-GlobalGlobal
380 women become pregnant380 women become pregnant
190 women face unplanned or 190 women face unplanned or unwanted pregnancyunwanted pregnancy
110 women experience a 110 women experience a pregnancy related complicationpregnancy related complication
40 women have unsafe 40 women have unsafe abortionsabortions
1 woman dies from a 1 woman dies from a pregnancy-related complicationpregnancy-related complication


Gujarat – A ProfileGujarat – A Profile
Overview
Area 196,000 km 6% of India
Population 50.5 million 5% of India
Urbanization 37% India avg. 28%
SDP(2003-04)
Rs 1,425.60 billion(€ 26.40 bill.)
6.33% of India
Per Capita Income(2003-04)
Rs 26,979 (€ 496.24)
India average -Rs. 20,989
(€ 388.69)
Recognizing Gujarat potential the Planning Commission set a target growth rate of 10% p.a. for Gujarat
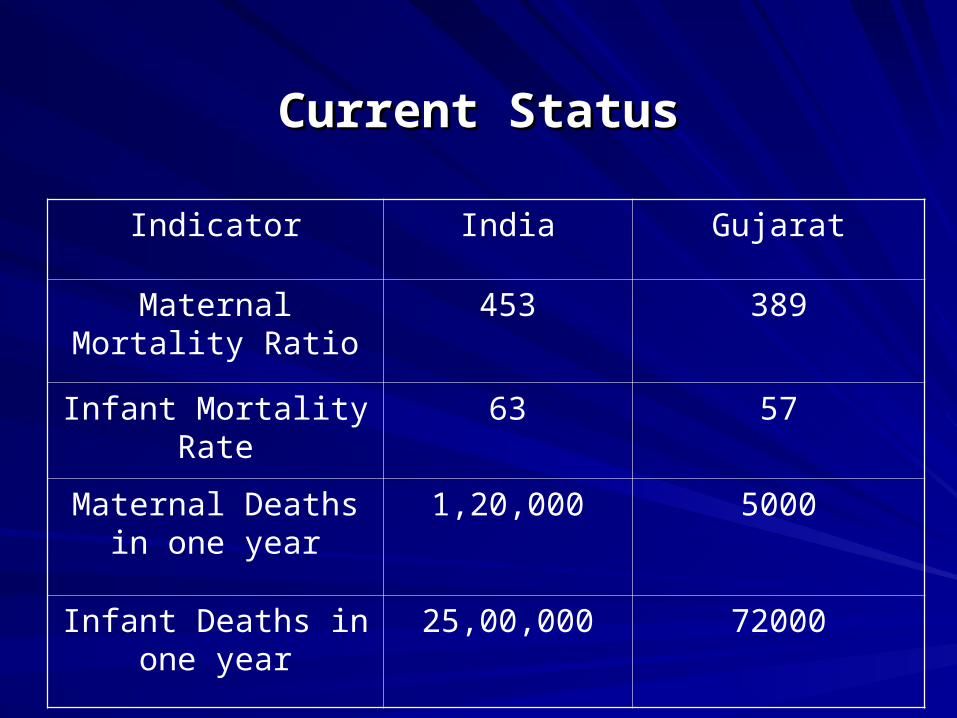
Current StatusCurrent Status
Indicator India Gujarat
Maternal Mortality Ratio
453 389
Infant Mortality Rate 63 57
Maternal Deaths in one year
1,20,000 5000
Infant Deaths in one year
25,00,000 72000

OBJECTIVES- OBJECTIVES-
Vision 2010, Population Policy & RCH Vision 2010, Population Policy & RCH IIII
Reduce MMR from 389 (in 1998) to Reduce MMR from 389 (in 1998) to 100 per 100,000 live births by 2010100 per 100,000 live births by 2010
Reduce IMR from 60 to 30 by 2010Reduce IMR from 60 to 30 by 2010
Stabilize population by reducing TFRStabilize population by reducing TFR from 3.0 to 2.1 by 2010from 3.0 to 2.1 by 2010

Infection14.9%
Haemorrhage24.8%
Indirect causes19.8%
Other direct causes
7.9%
Unsafe abortion
12.9%
Obstructed labour
6.9%
Eclampsia12.9%
Causes of Maternal Death

Timing of maternal deaths-Timing of maternal deaths-General ConditionsGeneral Conditions
Postpartum60%
During pregnancy
24%
During delivery
16%

Time from Time from onset of complication to deathonset of complication to death
PPHPPH 2 hour2 hour
APHAPH 12 hour 12 hour
Ruptured uterusRuptured uterus 1 day1 day
EclampsiaEclampsia 2 days2 days
Obstructed laborObstructed labor 1 day1 day
SepsisSepsis 6 days6 days

When do babies die
73.3
4.2
13.8
8.7
0 10 20 30 40 50 60 70 80
Week 4
Week 3
Week 2
Week 1

Maternal Mortality: Maternal Mortality: UK 1840–1960UK 1840–1960
0
100
200
300
400
500
MaternalDeaths
Improvements in nutrition, sanitation
Antibiotics, banked blood, surgical improvements
Antenatal care
Maine 1999.

Maternal Mortality ReductionMaternal Mortality ReductionSri Lanka 1940–1985Sri Lanka 1940–1985
0
400
800
1200
1600
2000
1940–45 1950–55 1960–65 1970–75 1980–85Ma
tern
al
De
ath
s p
er
10
0 0
00
liv
eb
irth
s
85% births attended
by trained personnel

New Global Understanding ofNew Global Understanding ofMMR ReductionMMR Reduction
Once major obstetric complication Once major obstetric complication develops- even a trained TBA or a nurse develops- even a trained TBA or a nurse cannot do much at home cannot do much at home
These complications require effective back These complications require effective back up by trained O&G expertsup by trained O&G experts
surgical interventions surgical interventions injections of antibiotic injections of antibiotic blood transfusion blood transfusion aggressive treatments aggressive treatments

Three Delays Responsible for Three Delays Responsible for Maternal DeathsMaternal Deaths
1.1. Delay in deciding to seek careDelay in deciding to seek care (Individual & family) (Individual & family) Lack of understanding of complicationsLack of understanding of complications Gender issues, Low status of womenGender issues, Low status of women Socio-cultural barriers to seeking careSocio-cultural barriers to seeking care Poor economic conditions of the familyPoor economic conditions of the family
2.2. Delay in reaching careDelay in reaching care ( Community & System) ( Community & System) Lack or underutilization of transport fundsLack or underutilization of transport funds Non availability of referral transport in remote placesNon availability of referral transport in remote places Lack of communication networkLack of communication network
3.3. Delay in receiving careDelay in receiving care (System) (System) Poor facilities, personnel and SuppliesPoor facilities, personnel and Supplies Poorly trained personnel with indifferent attitudePoorly trained personnel with indifferent attitude

Delay in problem recognition and decision makingSECOND DELAYSECOND DELAY
Delay in reaching a referral facility
FIRST DELAYFIRST DELAY
THIRD DELAYTHIRD DELAY
Delay in getting care at the health facility
WHY Do Women Die?WHY Do Women Die?

OptionsOptions
Improve Government Health ServiceImprove Government Health ServiceCompetent staffCompetent staff
Adequate infrastructural facilitiesAdequate infrastructural facilities
User friendly, good quality Competitive User friendly, good quality Competitive Services Services Marketing of servicesMarketing of services
Public Private PartnershipPublic Private Partnership
Outsourcing- Curative servicesOutsourcing- Curative services
Health Insurance Health Insurance

Maternal Health- GujaratMaternal Health- GujaratObjectives ( by 2010):Objectives ( by 2010):
Universalize coverage of antenatal care Universalize coverage of antenatal care (100%)(100%)
Increase the deliveries attended by SBAs Increase the deliveries attended by SBAs 90% 90%
Increase institutional deliveries by 80%Increase institutional deliveries by 80% increase access to Emergency Obstetric increase access to Emergency Obstetric
Care for complicated deliveries Care for complicated deliveries Increase coverage of Post Natal Care Increase coverage of Post Natal Care
(90%) (90%) Increase access to Early & Safe Abortion Increase access to Early & Safe Abortion
servicesservices Improve access to RTI/ STI servicesImprove access to RTI/ STI services Introduce AFHS in all PHC/ CHCsIntroduce AFHS in all PHC/ CHCs..

Broad IssuesBroad Issues
Non - availability of O & G specialistsNon - availability of O & G specialists
Accessibility of services-Tribal and Accessibility of services-Tribal and urban slumsurban slums
Poor utilization of services- Poor utilization of services- Low felt need of health & medical servicesLow felt need of health & medical services Lack of user friendly & quality public health Lack of user friendly & quality public health
servicesservices Costly private health and medical servicesCostly private health and medical services No health insurance coverageNo health insurance coverage

Chiranjeevi Yojna - OptionsChiranjeevi Yojna - Options
Service Coverage through Service Coverage through outsourcing- voucher systemoutsourcing- voucher system
Emergency Obstetric Care & Emergency Obstetric Care & Neonatal CareNeonatal Care
Private Gynecs/ GIA in their facilityPrivate Gynecs/ GIA in their facility
Payment to Gynecs for working in Payment to Gynecs for working in government hospitalgovernment hospital

Service ChargesService Charges
Normal delivery 85 800 68000
Complicated cases
Eclampsia 1000
Forceps/vacuum/breech 3 1000 3000
Episiotomy 800
Septicemia 2 3000 6000
Blood transfusion 3 1000 3000
Cesarean (7%) 7 5000 35000
Predelivery visit 100 100 10000
Investigation 100 50 5000
Sonography 30 150 4500
Dai 100 50 5000
Transport 100 200 20000179500

Service ChargesService Charges
Normal delivery 85 200 17000
Complicated cases
Eclampsia 300
Forceps/vacuum/breech 3 300 900
Episiotomy 300
Septicemia 2 300 600
Blood transfusion 3 300 900
Cesarean (7%) 7 1000 7000
Predelivery visit 100 100 10000
Investigation
Sonography 30 150 4500
Dai 100 50 5000
Transport 100 200 20000
65900

Population and BirthsPopulation and Births
Kachchh 1526321
Banas Kantha 2502843
Sabar Kantha 2083416
Panch Mahals 2024883
Dohad 1635374
Total 9772837
Total Births 234548
BPL births 96432

Implementation of Chiranjeevi - 1Implementation of Chiranjeevi - 1
District level FOGSI members workshops District level FOGSI members workshops organized for orientation on Chiranjeevi scheme organized for orientation on Chiranjeevi scheme and enrollment of doctors on the paneland enrollment of doctors on the panel
Honorable Health Minister wrote a letter about the Honorable Health Minister wrote a letter about the scheme to presidents of district and talukas in 5 scheme to presidents of district and talukas in 5 districts.districts.
District level Advocacy workshops of Presidents of District level Advocacy workshops of Presidents of district and taluka panchayat, along with BHO and district and taluka panchayat, along with BHO and Chiranjeevi panel doctors organized in each Chiranjeevi panel doctors organized in each district. district.

Implementation of Chiranjeevi - 2Implementation of Chiranjeevi - 2
In each district IEC activities were undertaken. In each district IEC activities were undertaken. Awareness through Gramsabhas Awareness through Gramsabhas
Rs 15000/ advance was given to each Rs 15000/ advance was given to each obstetrician. No delay in reimbursement to obstetrician. No delay in reimbursement to doctors.doctors.
Regular interaction with Chiranjeevi Panel Regular interaction with Chiranjeevi Panel doctors by CDHOsdoctors by CDHOs

Chiranjiv Yojna - performance as on June 2006
District Normal LSCS Complicated Total % LSCS
BK 3081 125 310 3516 3.6
Dahod 1842 113 430 2415 4.7
Kutch 1386 95 345 1826 5.2
P'mahal 4777 80 0 4857 1.6
SK 3422 383 0 3805 10.1
Total 14508 796 1085 16389 4.9

Specialist Involvement
DistrictTotal O&GSpecialists available
# enlisted under
chiranjivi
Total # of deliveries
Performed
Average delivery per O&G
BK 50 58 3516 61
Dahod 16 15 2415 161
Kutch 47 20 1826 91
P'mahal 29 20 4857 243
SK 73 45 3805 85
Total 215 158 16389 104

Miles to goMiles to go
District
BPL deliveries
workload for 6 months
BPL chiranjivi beneficiaries for
6 months
% age against BPL delivery workload for
6 months
BK 9464 3516 37
Dahod 7686 2415 31
Kutch 7576 1826 24
P'mahal 8100 4857 60
SK 15390 3805 25
Total 48216 16389 34
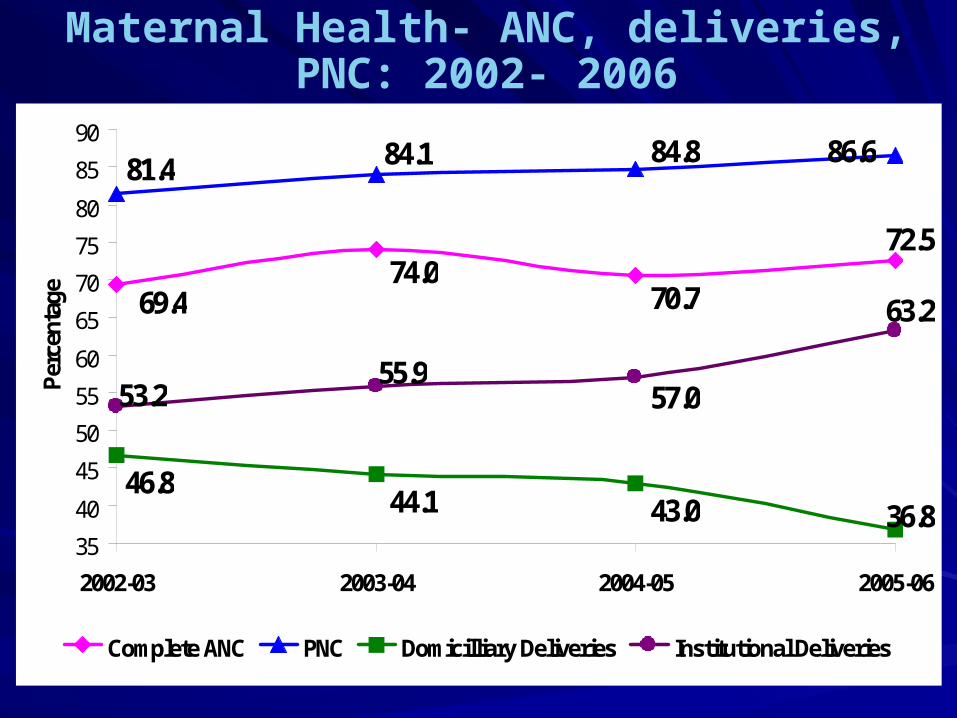
72.5
69.474.0
70.7
81.4 84.1 84.8 86.6
36.843.044.146.8
63.2
53.255.9
57.0
35
40
45
50
55
60
65
70
75
80
85
90
2002-03 2003-04 2004-05 2005-06
Per
cent
age
Complete ANC PNC Domicilliary Deliveries Institutional Deliveries
Maternal Health- ANC, deliveries, PNC: 2002- 2006

Effect on Government deliveriesEffect on Government deliveries
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
200000
2001-02 2002-03 2003-04 2004-05 2005-06
BeMOCs CHCs PHCs Sub Centre

IssuesIssues
Surge of demand - boon to the poorSurge of demand - boon to the poor
Unprecedented support from the private practitioners Unprecedented support from the private practitioners
Unindicated C-section in checkUnindicated C-section in check
Availability of bloodAvailability of blood
Still asking for additional funds from the BPLStill asking for additional funds from the BPL
Non-BPL beneficiaries also being attendedNon-BPL beneficiaries also being attended
Under utilisation of Public facilitiesUnder utilisation of Public facilities

Issues in expansionIssues in expansion
Additional day’s stay after deliveryAdditional day’s stay after delivery
Sanitary pads supplySanitary pads supply
More funds for accompanying person – DaiMore funds for accompanying person – Dai
Other services Sterilisation/ IUD/ RTI/ STI/ Other services Sterilisation/ IUD/ RTI/ STI/ HIV/AIDS/pap smearHIV/AIDS/pap smear
More charges for transportation in KutchMore charges for transportation in Kutch
Cost likely to increase to 2,00,000/100 deliveriesCost likely to increase to 2,00,000/100 deliveries

The bill for Gujarat & IndiaThe bill for Gujarat & India
BPL Population Delivery LoadEstimated BPL births
Costs @1795/delivery
Five pilot districts 4 months
16,389 Rs 29 million
Five districts (annual)
96432 Rs 172 million
Entire Gujarat BPL Beneficiaries
3,00,000 Rs 540 - 600 million
India --10000 million*

Our Mission:
“Save the lives of thousands of Mothers and
Children dying for no fault of theirs and prevent the spread of infections and
promote healthy life styles”
Working together for a healthy Bharat



















