CHINA INTERNATIONAL SYMPOSIUM (CIT)download.xuebalib.com/2nkmaNW2B4bD.pdf · Address for reprints:...
14
CHINA INTERNATIONAL SYMPOSIUM (CIT) Interleukin‐6, but Not C‐Reactive Protein, Predicts the Occurrence of Cardiovascular Events after Drug‐Eluting Stent for Unstable Angina SHAO‐ LIANG CHEN, M.D., F.A.C.C. 1,2 y YAN LIU, M.D., 1 LING LIN, M.D., 1 FEI YE, M.D., 1 JUN‐ JIE ZHANG, PH.D., 1 NAI ‐ LIANG TIAN, M.D., 1 JUN‐ XIA ZHANG, M.D., 1 ZUO‐ YING HU, PH.D., 1 TIAN XU, M.B.B.S., 1 LI LI, M.D., 2 BO XU, M.B.B.S., 3 FAISAL LATIF, M.D., 4 and THACH NGUYEN, M.D. 5 From the 1 Nanjing First Hospital, Nanjing Medical University, Nanjing, China; 2 Gansu Provincial People’ s Hospital, Lanzhou, China; 3 Beijing Fuwai Cardiovascular Hospital, Beijing, China; 4 Veteran Administration Medical Center, University of Oklahoma Heath Science, Oklahoma City, Oklahoma; and 5 St. Mary Medical Center, Hobart, Indiana Background: Evidences concerning the predictive value of baseline inflammatory biomarkers after drug‐eluting stent (DES) placement are controversial, mainly because the use of statin was not precisely defined. Objectives: The aim was to compare the differences between interleukin (IL)‐6 and high‐sensitivity C‐reactive protein (hs‐CRP) in predicting cardiovascular events 2 years after stenting in patients with unstable angina (UA) who had not received statin pretreatment. Methods: There were 1,896 patients included in this study. The primary end‐point was the occurrence of cardiac death or myocardial infarction (MI). Secondary endpoints included all‐cause death, stent thrombosis (ST), target lesion revascularization (TLR), target vessel revascularization (TVR), or a composite of major adverse cardiac events (MACE) at 2 years after the procedure. Results: During the median follow‐up of 2.77 years, 96 patients experienced cardiac death (n ¼ 37, 1.95%) or MIs (n ¼ 70, 3.69%), 94 TLRs, 123 TVRs, 215 MACEs, and 21 definite or probable STs. In multivariable Cox proportional‐hazards models and discrimination analysis, elevated IL‐6 levels were superior to hs‐CRP in predicting the occurrence not only of cardiac death or MI (HR 1.337, 95% CI 1.234–1.449, P < 0.001), but also of MACE and late‐occurring definite/probable ST. Incorporation of IL‐6 into conventional variables resulted in significantly increased c statistic for the prediction of end‐points, with the exception of TLR and TVR. Conclusion: Elevated IL‐6 levels were independent predictors of cardiac death or MI, MACE, and late ST in patients with UA who had not received statin pretreatment, suggesting a role for IL‐6 in the inflammatory risk assessment. Pathological studies have confirmed that atherosclerosis is a chronic inflammatory disease. Serum levels of high‐ sensitivity C‐reactive protein (hs‐CRP), matrix metalloproteinase, plasminogen activator inhibitor‐1, the complement components C3a or C5a, and interleukin(IL)‐6 were reported to provide strong and independent indications of the risk for future cardiovascular (CV) events, even among individuals who are thought to be free of vascular disease. (J Interven Cardiol 2014;27:142–154) Introduction Percutaneous coronary intervention (PCI) using a drug‐eluting stent (DES) has been extensively used for the treatment of atherosclerotic coronary artery disease. DES are an effective tool to reduce in‐stent restenosis (ISR), though not without risks of late stent thrombosis (ST), when compared to bare metal stents. 1,2 Accord- ing to the Academic Research Consortium Disclosure statement: The authors report no financial relationships or conflicts of interest regarding the content herein. y Dr. Shao‐Liang Chen is a Fellow of Jiangsu Provincial Cooperative Innovative Medical Center. Address for reprints: Shao‐Liang Chen, M.D., F.A.C.C., Cardiolo- gical Department, Nanjing First Hospital, Nanjing Medical University, Nanjing 210006, China. Fax: þ86‐25‐52208048; e‐mail: [email protected] © 2014, Wiley Periodicals, Inc. DOI: 10.1111/joic.12103 142 Journal of Interventional Cardiology Vol. 27, No. 2, 2014
-
Upload
trinhkhuong -
Category
Documents
-
view
216 -
download
0
Transcript of CHINA INTERNATIONAL SYMPOSIUM (CIT)download.xuebalib.com/2nkmaNW2B4bD.pdf · Address for reprints:...

CHINA INTERNATIONAL SYMPOSIUM (CIT)
Interleukin‐6, but Not C‐Reactive Protein, Predicts the Occurrence of
Cardiovascular Events after Drug‐Eluting Stent for Unstable Angina
SHAO‐LIANG CHEN, M.D., F.A.C.C.1,2y YAN LIU, M.D.,1 LING LIN, M.D.,1 FEI YE, M.D.,1
JUN‐JIE ZHANG, PH.D.,1 NAI‐LIANG TIAN, M.D.,1 JUN‐XIA ZHANG, M.D.,1
ZUO‐YING HU, PH.D.,1 TIAN XU, M.B.B.S.,1 LI LI, M.D.,2 BO XU, M.B.B.S.,3
FAISAL LATIF, M.D.,4 and THACH NGUYEN, M.D.5
From the 1Nanjing First Hospital, Nanjing Medical University, Nanjing, China; 2Gansu Provincial People’s Hospital, Lanzhou, China;3Beijing Fuwai Cardiovascular Hospital, Beijing, China; 4Veteran Administration Medical Center, University of Oklahoma Heath Science,Oklahoma City, Oklahoma; and 5St. Mary Medical Center, Hobart, Indiana
Background: Evidences concerning the predictive value of baseline inflammatory biomarkers after drug‐elutingstent (DES) placement are controversial, mainly because the use of statin was not precisely defined.Objectives: The aim was to compare the differences between interleukin (IL)‐6 and high‐sensitivity C‐reactiveprotein (hs‐CRP) in predicting cardiovascular events 2 years after stenting in patients with unstable angina (UA)who had not received statin pretreatment.Methods: There were 1,896 patients included in this study. The primary end‐point was the occurrence of cardiacdeath or myocardial infarction (MI). Secondary endpoints included all‐cause death, stent thrombosis (ST), targetlesion revascularization (TLR), target vessel revascularization (TVR), or a composite of major adverse cardiacevents (MACE) at 2 years after the procedure.Results: During the median follow‐up of 2.77 years, 96 patients experienced cardiac death (n¼ 37, 1.95%) or MIs(n¼ 70, 3.69%), 94 TLRs, 123 TVRs, 215 MACEs, and 21 definite or probable STs. In multivariable Coxproportional‐hazards models and discrimination analysis, elevated IL‐6 levels were superior to hs‐CRP inpredicting the occurrence not only of cardiac death or MI (HR 1.337, 95% CI 1.234–1.449, P< 0.001), but also ofMACE and late‐occurring definite/probable ST. Incorporation of IL‐6 into conventional variables resulted insignificantly increased c statistic for the prediction of end‐points, with the exception of TLR and TVR.Conclusion: Elevated IL‐6 levels were independent predictors of cardiac death orMI, MACE, and late ST in patientswith UA who had not received statin pretreatment, suggesting a role for IL‐6 in the inflammatory risk assessment.Pathological studies have confirmed that atherosclerosis is a chronic inflammatory disease. Serum levels of high‐sensitivity C‐reactive protein (hs‐CRP), matrix metalloproteinase, plasminogen activator inhibitor‐1, thecomplement components C3a or C5a, and interleukin(IL)‐6 were reported to provide strong and independentindications of the risk for future cardiovascular (CV) events, even among individuals who are thought to be free ofvascular disease. (J Interven Cardiol 2014;27:142–154)
Introduction
Percutaneous coronary intervention (PCI) using adrug‐eluting stent (DES) has been extensively used forthe treatment of atherosclerotic coronary artery disease.DES are an effective tool to reduce in‐stent restenosis(ISR), though not without risks of late stent thrombosis(ST), when compared to bare metal stents.1,2 Accord-ing to the Academic Research Consortium
Disclosure statement: The authors report no financial relationshipsor conflicts of interest regarding the content herein.yDr. Shao‐Liang Chen is a Fellow of Jiangsu Provincial CooperativeInnovative Medical Center.Address for reprints: Shao‐Liang Chen, M.D., F.A.C.C., Cardiolo-gical Department, Nanjing First Hospital, Nanjing MedicalUniversity, Nanjing 210006, China. Fax: þ86‐25‐52208048;e‐mail: [email protected]
© 2014, Wiley Periodicals, Inc.DOI: 10.1111/joic.12103
142 Journal of Interventional Cardiology Vol. 27, No. 2, 2014

classification,2 early ST was correlated with theinterventional procedures (edge dissection and appo-sition of stent), clopidogrel resistance, and mechanicalinjury resulting in significant elevation of inflammatorybiomarkers levels; however, the persistent localinflammatory reaction of vessel wall against non-erodable polymer from a DES was reported to berelated to the occurrence of late and too late ST.Among the inflammatory biomarkers implicated in
ST after DES, hs‐CRP is the most extensivelystudied.3–10 Unfortunately, data regarding the predic-tion of hs‐CRP levels for CVafter DES are conflicting:some studies5–12 reported that high hs‐CRP levelscorrelated with ST, but some investigators failed toagree.10,13,14 The principal reason for the conflictingresults appears to be the timing of statin treatment andhs‐CRP measurement not being precisely defined.6–14
Statins exhibit well‐known anti‐inflammatory proper-ties15; their beneficial effects in patients undergoingstent deployment have been documented in manyclinical studies.16–18 Thus, the real meaning of“baseline hs‐CRP levels” as reported in previousstudies has been recently challenged.19,20 Furthermore,IL‐6, as the upstream mediator of CRP, has beenreported to be an independent predictor of the long‐term risk of death or heart failure in patientsexperiencing acute coronary syndromes.21 Notably,Hwang et al.22 recently reported that patients present-ing with ST had the highest IL‐6 quartile measured3 months after DES. As a result, the aim of this presentstudy was to compare the predictive value of hs‐CRPand IL‐6 for CV within 2 years after DES in unstableangina (UA) without prior statin treatment.
Methods
Patient Population. The study population includ-ed consecutive patients with de novo coronary stenosistreated with a DES from 2008 to 2010. Patients wereexcluded if they had stable angina,18 myocardialinfarction (MI) <1 month prior to admission,18
cardiogenic shock, prior bare metal stent (BMS),active infection, inflammatory arthritis, inflammatorybowel disease, connective tissue disease, malignancies,recent (<2 months) surgery, or major trauma. Mostimportantly, patients already on statin treatment beforeadmission were excluded. This study was approved bythe Institutional Review Board and all patientsprovided written informed consent.
Measurement of hs‐CRP and IL‐6. The patientshad their hs‐CRP and IL‐6 levels measured atadmission. Venous blood samples were obtainedupon admission in the heparin‐containing tube andimmediately centrifuged at 3,000g for 20minutes at4 °C. The plasma component was separated and sent ondry ice to the core lab (Cardiovascular Laboratory,Medical University Center), where samples werestored at �70 °C. The hs‐CRP was assayed witha latex‐enhanced hs‐CRP immunoassay (COBASINTEGRA, Roche Diagnostics GmbH, Mannheim,Germany). The Luminex 100 system (Luminex Corp,Austin, TX, USA) and the Lincoplex Kit (LincoResearch, St. Charles,MO, USA)were used to evaluatethe serum concentration of IL‐6. The assays wereperformed in duplicate. All laboratory testing wasperformed by 2 technicians who were blinded to theclinical events, with intra‐ and interobserver variance<3% as assessed from the first 30 samples.Interventional Procedure. A bolus injection of
100–120 IU/kg of heparin was injected via an arterialsheath. An additional 3,000 IU of heparin was injectedto maintain an activated clotting time >280 seconds.PCI was performed according to standard protocol. Thechoice of specific type of sirolimus‐eluting (Cypher,Cordis, Johnson & Johnson, Miami Lakes, FL),paclitaxel‐eluting (Taxus, Boston Scientific, Natick,MA, USA), or zotarolimus‐eluting stent was left to theoperator’s discretion. Post‐stent dilation using anoncompliant balloon was recommended for all stentsand was also left to the operator’s discretion. Allprocedures were performed within 4 hours afteradmission.Medications. A loading dose of 300mg of aspirin
and 300mg of clopidogrel was given at admission.After the procedure, all of the patients were prescribedaspirin (300mg once daily for 1 month, then 100mgonce daily) indefinitely and clopidogrel (75mg oncedaily) for at least 12 months. Continuation ofclopidogrel beyond this duration was at the discretionof the physician. Statin treatment (20–40mg ofatorvastatin or 10–20mg of rosuvastatin) was startedimmediately upon admission after the blood draw forIL‐6 and hs‐CRP measurement and continued through-out the follow‐up period unless stopping the treatmentbecame necessary.End‐Points and Definitions. The primary end‐
point was the occurrence of cardiac death or MI. MIwas defined as the presence of new Q waves on theelectrocardiogram (ECG) or an elevation of the creatine
Vol. 27, No. 2, 2014 Journal of Interventional Cardiology 143
IL‐6 PREDICTS MACE AFTER DES

kinase‐MB isoenzyme or troponin of at least 3 timesgreater than the upper limit of normal in at least 2 serialblood samples. Secondary end‐points were all‐causedeath, ST, target lesion revascularization (TLR), targetvessel revascularization (TVR) and a composite ofmajor adverse cardiac events (MACE, includingcardiac death, MI or TVR). ST was classified asdefinite, probable, or possible, according to thedefinitions provided by the Academic ResearchConsortium (ARC).23 Regarding timing, ST wasdefined as early (<30 days), late (30 days to 1 year),or too late (>1 year). All events were adjudicated by anindependent committee of clinicians who were blindedto the IL‐6 and hs‐CRP values. Death was defined aseither all‐cause death or cardiac death. MI was definedas the presence of new Q waves on the EKG or anelevation of the creatine kinase‐MB isoenzyme ortroponin of at least 3 times greater than the upper limitof normal in at least 2 serial blood samples. TLR wasdefined as clinically driven revascularization of thetarget lesion. TVR was defined as the clinically drivenrevascularization of the target vessel. An hs‐CRP level�3mg/L was considered elevated,5 and this cutoffvalue was prespecified in the study protocol beforeexamination of the data. An IL‐6 level �5 pg/ml waspreviously considered elevated8; however, Hwanget al.22 reported that an IL‐6 level >8.4 pg/ml was anindependent predictive factor of ST, and the cutoffvalue of an IL‐6 level �9 pg/ml was defined beforebeginning data analysis in the present study.Follow‐Up. All clinical, procedural, and outcome
data were prospectively collected by independentresearchers who were blinded to the study design.Clinical follow‐up after the PCI was performed viaoffice visit or telephone contact at 1, 6, 12, 18, and24 months. All patients were encouraged to have anangiographic follow‐up 8 months after the indexprocedure. ISR was defined as stenosis >50% atfollow‐up. Quantitative coronary analysis (QCA) wasperformed by 2 technicians from the IntracoronaryImaging Department and they were blinded of thebiomarker values.Statistical Methods. Continuous variables were
expressed as the means�SD and compared by use ofthe t‐test or the Mann‐Whitney U‐test as indicated.Categorical variables were compared with the x2 orFisher’s exact test. Logarithmic transformation wasperformed to normalize the distribution of thebiomarkers. Survival curves were generated fromKaplan–Meier estimates and compared by use of the
log‐rank test. The relationships of the IL‐6 and hs‐CRPlevels to the end‐points were investigated with the useof 2 regression models in order to assess the predictivevalue of biomarkers24: the binary regression model,where each end‐point was designated as dependent,IL‐6 or hs‐CRP levels were considered covariates, andgoodness of fit was assessed by the Hosmer–Lemeshow test; and25 the multivariable Cox propor-tional‐hazards model, where all the confoundingfactors, including clinical, anatomical, and proceduralvariables (listed in Table 1), and IL‐6 or hs‐CRP levelswere treated as covariates, and each end‐point wasdesignated as dependent. In this model, the hazardratio (HR), 95% confidence interval (CI), and P valuefor either IL‐6 or hs‐CRP were automaticallycalculated. No relevant violations were observed.The receiver‐operator curve (ROC) for either IL‐6 orhs‐CRP levels was constructed to predict the occur-rence of each end point, and the area under the curve(c statistic) was automatically calculated. The differ-ence in the 95% confidence intervals for the c statisticbetween the IL‐6 and hs‐CRP levels for predicting thesame clinical event was compared with the Delong–Delong (Z) test (Analyze‐ItTM, Melbourne, Australia).The value of incorporating either IL‐6 or hs‐CRP in thecontext of clinical, anatomical, and proceduralcharacteristics for predicting each end‐point wasmeasured. First, all conventional confounding factors,including the patient, lesion, and procedural riskfactors (without biomarkers), were tested via thebinary regression model (rough model); then IL‐6 orhs‐CRP was incorporated into the model. A propensitywas automatically calculated for these 3 regressionmodels (rough model, rough modelþ IL‐6 levels,rough modelþ hs‐CRP levels). Again, the c statisticrelated to each propensity was gained from the ROCcurve and was used to evaluate the improvement inmodel discrimination when IL‐6 or hs‐CRP wasincorporated. The 95% confidence intervals fordifferences in the c statistic between the roughmodelþ IL‐6 (or rough modelþ hs‐CRP) and therough model were obtained by the Z test. The globalmodel fit was also compared by using boot strappedmultinomial logistic regression statistics with thepercentile method (200 replicates), which is a measurefor the log‐likelihood function; a low value indicates abetter fit. All reported P values are 2 sided, andP< 0.05 was considered to be statistically significant.SPSS 16.0 (SPSSTM Co., Chicago, IL, USA) was usedfor all statistical analyses.
144 Journal of Interventional Cardiology Vol. 27, No. 2, 2014
CHEN, ET AL.
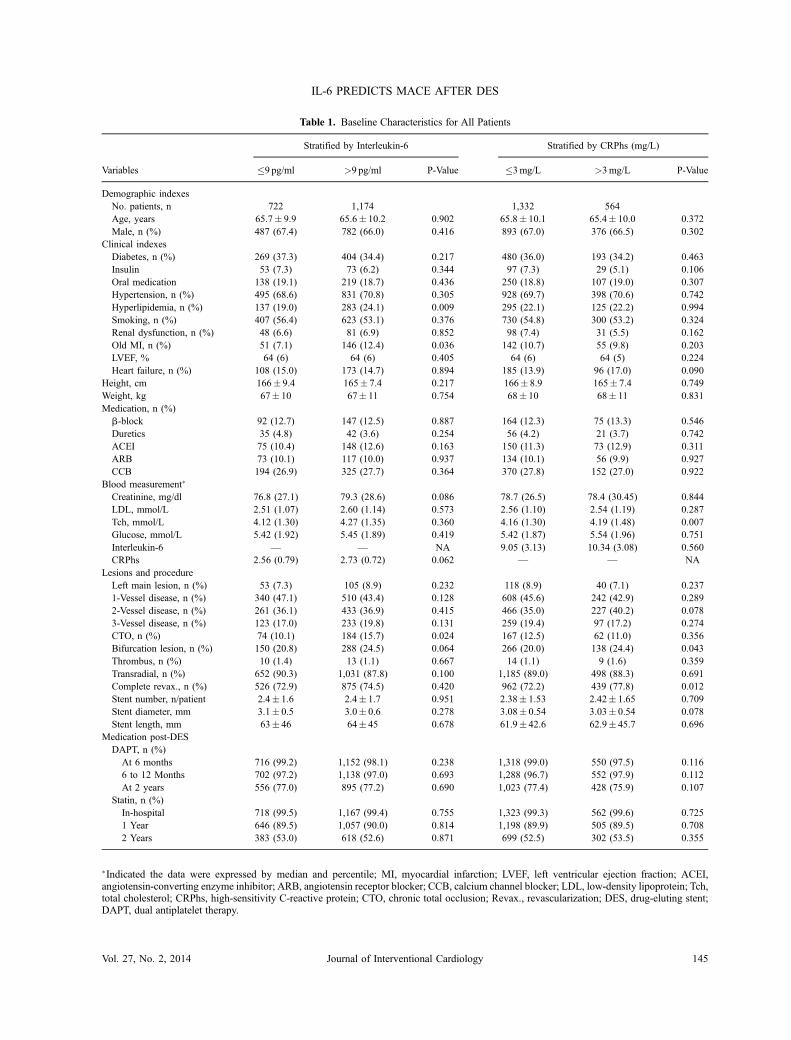
Table 1. Baseline Characteristics for All Patients
Variables
Stratified by Interleukin‐6 Stratified by CRPhs (mg/L)
�9 pg/ml >9 pg/ml P‐Value �3mg/L >3mg/L P‐Value
Demographic indexesNo. patients, n 722 1,174 1,332 564Age, years 65.7� 9.9 65.6� 10.2 0.902 65.8� 10.1 65.4� 10.0 0.372Male, n (%) 487 (67.4) 782 (66.0) 0.416 893 (67.0) 376 (66.5) 0.302
Clinical indexesDiabetes, n (%) 269 (37.3) 404 (34.4) 0.217 480 (36.0) 193 (34.2) 0.463Insulin 53 (7.3) 73 (6.2) 0.344 97 (7.3) 29 (5.1) 0.106Oral medication 138 (19.1) 219 (18.7) 0.436 250 (18.8) 107 (19.0) 0.307Hypertension, n (%) 495 (68.6) 831 (70.8) 0.305 928 (69.7) 398 (70.6) 0.742Hyperlipidemia, n (%) 137 (19.0) 283 (24.1) 0.009 295 (22.1) 125 (22.2) 0.994Smoking, n (%) 407 (56.4) 623 (53.1) 0.376 730 (54.8) 300 (53.2) 0.324Renal dysfunction, n (%) 48 (6.6) 81 (6.9) 0.852 98 (7.4) 31 (5.5) 0.162Old MI, n (%) 51 (7.1) 146 (12.4) 0.036 142 (10.7) 55 (9.8) 0.203LVEF, % 64 (6) 64 (6) 0.405 64 (6) 64 (5) 0.224Heart failure, n (%) 108 (15.0) 173 (14.7) 0.894 185 (13.9) 96 (17.0) 0.090
Height, cm 166� 9.4 165� 7.4 0.217 166� 8.9 165� 7.4 0.749Weight, kg 67� 10 67� 11 0.754 68� 10 68� 11 0.831Medication, n (%)b‐block 92 (12.7) 147 (12.5) 0.887 164 (12.3) 75 (13.3) 0.546Duretics 35 (4.8) 42 (3.6) 0.254 56 (4.2) 21 (3.7) 0.742ACEI 75 (10.4) 148 (12.6) 0.163 150 (11.3) 73 (12.9) 0.311ARB 73 (10.1) 117 (10.0) 0.937 134 (10.1) 56 (9.9) 0.927CCB 194 (26.9) 325 (27.7) 0.364 370 (27.8) 152 (27.0) 0.922
Blood measurement�
Creatinine, mg/dl 76.8 (27.1) 79.3 (28.6) 0.086 78.7 (26.5) 78.4 (30.45) 0.844LDL, mmol/L 2.51 (1.07) 2.60 (1.14) 0.573 2.56 (1.10) 2.54 (1.19) 0.287Tch, mmol/L 4.12 (1.30) 4.27 (1.35) 0.360 4.16 (1.30) 4.19 (1.48) 0.007Glucose, mmol/L 5.42 (1.92) 5.45 (1.89) 0.419 5.42 (1.87) 5.54 (1.96) 0.751Interleukin‐6 — — NA 9.05 (3.13) 10.34 (3.08) 0.560CRPhs 2.56 (0.79) 2.73 (0.72) 0.062 — — NA
Lesions and procedureLeft main lesion, n (%) 53 (7.3) 105 (8.9) 0.232 118 (8.9) 40 (7.1) 0.2371‐Vessel disease, n (%) 340 (47.1) 510 (43.4) 0.128 608 (45.6) 242 (42.9) 0.2892‐Vessel disease, n (%) 261 (36.1) 433 (36.9) 0.415 466 (35.0) 227 (40.2) 0.0783‐Vessel disease, n (%) 123 (17.0) 233 (19.8) 0.131 259 (19.4) 97 (17.2) 0.274CTO, n (%) 74 (10.1) 184 (15.7) 0.024 167 (12.5) 62 (11.0) 0.356Bifurcation lesion, n (%) 150 (20.8) 288 (24.5) 0.064 266 (20.0) 138 (24.4) 0.043Thrombus, n (%) 10 (1.4) 13 (1.1) 0.667 14 (1.1) 9 (1.6) 0.359Transradial, n (%) 652 (90.3) 1,031 (87.8) 0.100 1,185 (89.0) 498 (88.3) 0.691Complete revax., n (%) 526 (72.9) 875 (74.5) 0.420 962 (72.2) 439 (77.8) 0.012Stent number, n/patient 2.4� 1.6 2.4� 1.7 0.951 2.38� 1.53 2.42� 1.65 0.709Stent diameter, mm 3.1� 0.5 3.0� 0.6 0.278 3.08� 0.54 3.03� 0.54 0.078Stent length, mm 63� 46 64� 45 0.678 61.9� 42.6 62.9� 45.7 0.696
Medication post‐DESDAPT, n (%)
At 6 months 716 (99.2) 1,152 (98.1) 0.238 1,318 (99.0) 550 (97.5) 0.1166 to 12 Months 702 (97.2) 1,138 (97.0) 0.693 1,288 (96.7) 552 (97.9) 0.112At 2 years 556 (77.0) 895 (77.2) 0.690 1,023 (77.4) 428 (75.9) 0.107
Statin, n (%)In‐hospital 718 (99.5) 1,167 (99.4) 0.755 1,323 (99.3) 562 (99.6) 0.7251 Year 646 (89.5) 1,057 (90.0) 0.814 1,198 (89.9) 505 (89.5) 0.7082 Years 383 (53.0) 618 (52.6) 0.871 699 (52.5) 302 (53.5) 0.355
�Indicated the data were expressed by median and percentile; MI, myocardial infarction; LVEF, left ventricular ejection fraction; ACEI,angiotensin‐converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; LDL, low‐density lipoprotein; Tch,total cholesterol; CRPhs, high‐sensitivity C‐reactive protein; CTO, chronic total occlusion; Revax., revascularization; DES, drug‐eluting stent;DAPT, dual antiplatelet therapy.
Vol. 27, No. 2, 2014 Journal of Interventional Cardiology 145
IL‐6 PREDICTS MACE AFTER DES
Results
Patient Population. Between May 2008 andMay 2010, 5,278 patients who were implanted witha DES were prospectively included. Of these 3,382patients were excluded (1,504 patients with stableangina at admission, 901 with an MI [60 previous MIs,600 STEMIs, and 241 NSTEMIs] within the last30 days, 99 who received a BMS, 768 who had been onstatin treatment before admission, while 110 patientsmet other exclusion criteria). A total of 1,896 patientswith UA constituted the patient population.Baseline Characteristics. Table 1 shows the
baseline characteristics. Of 1,896 patients, 1,174(47.7%) had IL‐6 levels �9 pg/ml, and 564 (30.1%)had hs‐CRP levels �3mg/L. Compared to patientswith IL‐6 levels <9 pg/ml, patients with IL‐6 levels�9 pg/ml hadmore frequent hyperlipidemia, increasedserum creatinine, and glucose, more UA, and chronictotal occlusion. Compared to patients with hs‐CRPlevels �3mg/L, patients with levels <3mg/L hadlesser cholesterol levels, lesser bifurcation lesions, andunderwent more complete revascularization. The low,intermediate, and high quartiles of IL‐6 and hs‐CRP were <9.0 pg/ml, 9.0–11.65 pg/ml, >11.65 pg/ml, and 2.36mg/L, 2.37–3.07mg/L, >3.07mg/L,respectively.
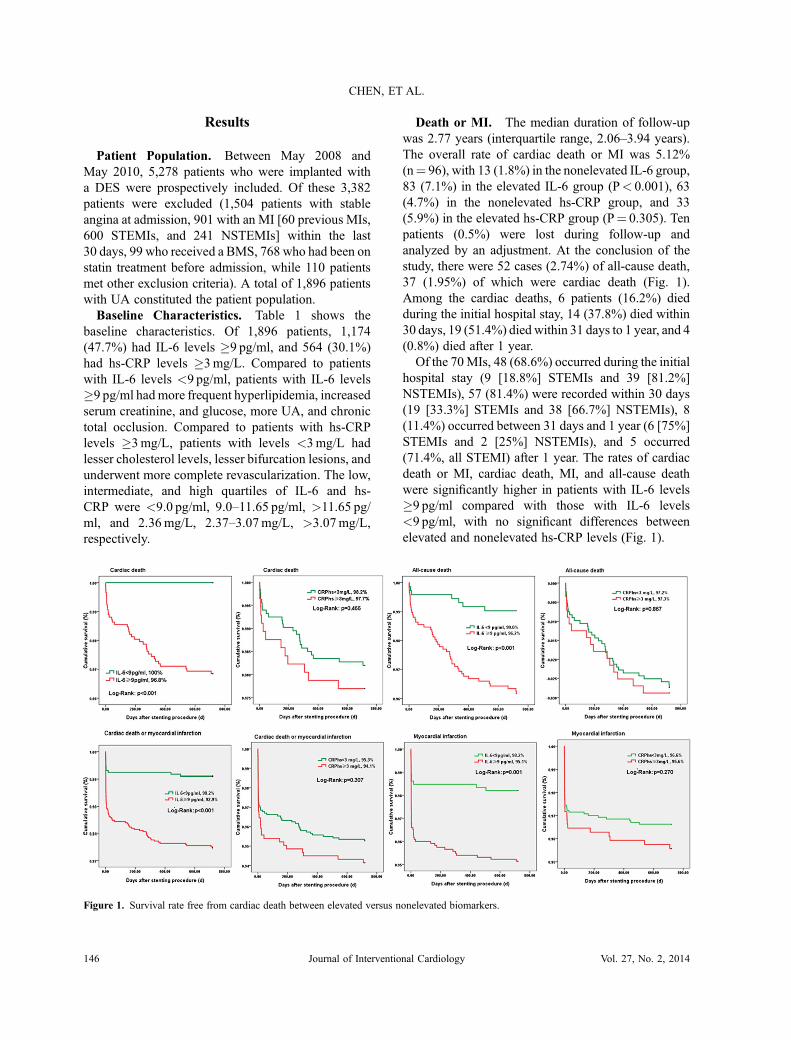
Death or MI. The median duration of follow‐upwas 2.77 years (interquartile range, 2.06–3.94 years).The overall rate of cardiac death or MI was 5.12%(n¼ 96), with 13 (1.8%) in the nonelevated IL‐6 group,83 (7.1%) in the elevated IL‐6 group (P< 0.001), 63(4.7%) in the nonelevated hs‐CRP group, and 33(5.9%) in the elevated hs‐CRP group (P¼ 0.305). Tenpatients (0.5%) were lost during follow‐up andanalyzed by an adjustment. At the conclusion of thestudy, there were 52 cases (2.74%) of all‐cause death,37 (1.95%) of which were cardiac death (Fig. 1).Among the cardiac deaths, 6 patients (16.2%) diedduring the initial hospital stay, 14 (37.8%) died within30 days, 19 (51.4%) died within 31 days to 1 year, and 4(0.8%) died after 1 year.Of the 70MIs, 48 (68.6%) occurred during the initial
hospital stay (9 [18.8%] STEMIs and 39 [81.2%]NSTEMIs), 57 (81.4%) were recorded within 30 days(19 [33.3%] STEMIs and 38 [66.7%] NSTEMIs), 8(11.4%) occurred between 31 days and 1 year (6 [75%]STEMIs and 2 [25%] NSTEMIs), and 5 occurred(71.4%, all STEMI) after 1 year. The rates of cardiacdeath or MI, cardiac death, MI, and all‐cause deathwere significantly higher in patients with IL‐6 levels�9 pg/ml compared with those with IL‐6 levels<9 pg/ml, with no significant differences betweenelevated and nonelevated hs‐CRP levels (Fig. 1).
Figure 1. Survival rate free from cardiac death between elevated versus nonelevated biomarkers.
146 Journal of Interventional Cardiology Vol. 27, No. 2, 2014
CHEN, ET AL.
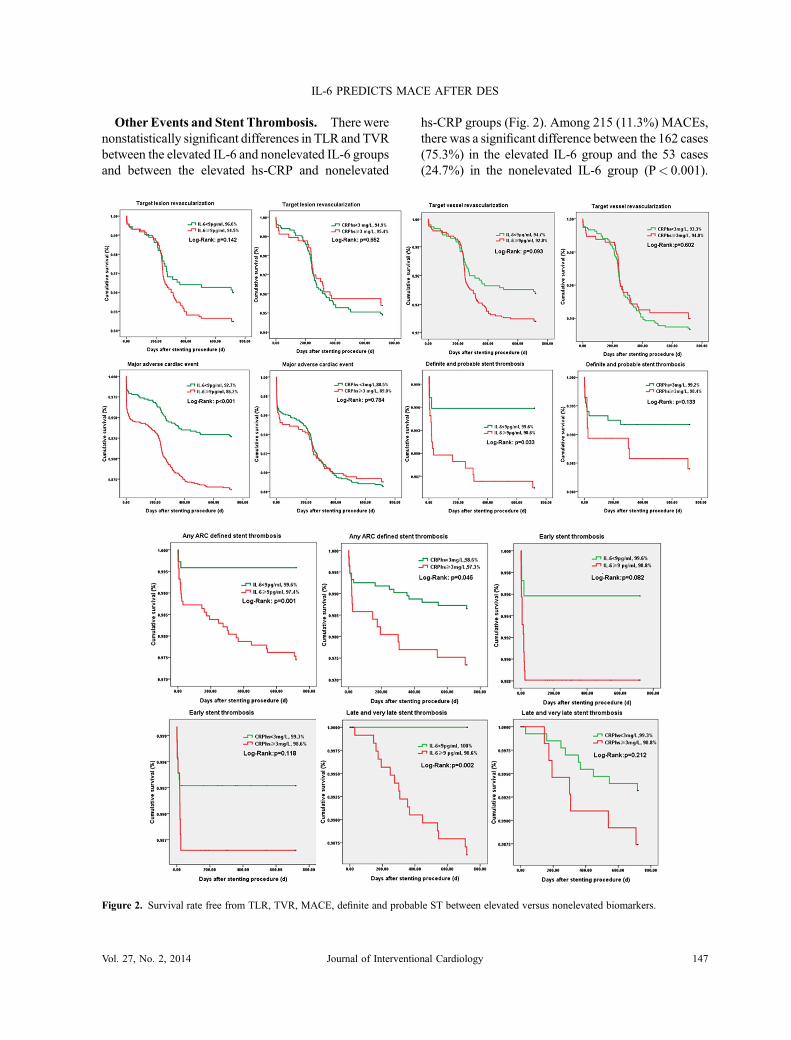
Other Events and Stent Thrombosis. There werenonstatistically significant differences in TLR and TVRbetween the elevated IL‐6 and nonelevated IL‐6 groupsand between the elevated hs‐CRP and nonelevated
hs‐CRP groups (Fig. 2). Among 215 (11.3%) MACEs,there was a significant difference between the 162 cases(75.3%) in the elevated IL‐6 group and the 53 cases(24.7%) in the nonelevated IL‐6 group (P< 0.001).
Figure 2. Survival rate free from TLR, TVR, MACE, definite and probable ST between elevated versus nonelevated biomarkers.
Vol. 27, No. 2, 2014 Journal of Interventional Cardiology 147
IL‐6 PREDICTS MACE AFTER DES

The MACE rate was 11.0% in the elevated hs‐CRPgroup versus 11.5% in the nonelevated hs‐CRP group(P¼ 0.812). There were 33 (1.7%) STs, with 21(63.6%) definite or probable, 12 (36.4%) possible, 16(48.5%) early, and 17 (51.5%) late or too late. Of the 21definite or probable STs, 14 (71.4%) were early, 6(28.6%) were late, and 1 (4.8%) was too late. Onepatient (4.8%) died and 14 (71.4%) presented with anMI. Among the patients with definite or probable ST,18 (85.6%) were on dual antiplatelet therapy and 3(14.4%) were on aspirin monotherapy at the time ofpresentation for ST. The definite and probable, anyARC‐defined, and late and too late ST in the elevatedIL‐6 group (n¼ 0) were significantly higher than in thenonelevated group (n¼ 16, 1.4%, P¼ 0.001). AnyARC‐defined STs in the elevated hs‐CRP group weresignificantly higher compared to the nonelevatedgroup. Eight months after the index procedure, 1,384(72.9%) patients had a repeat coronary angiography.The ISR rate was 5.4% (n¼ 39) in the nonelevated IL‐6group and 7.9% (n¼ 93) in the elevated IL‐6 group(P¼ 0.041); it was not significantly different betweenthe elevated and the nonelevated hs‐CRP groups (5.5%vs. 4.0%, respectively, P¼ 0.189). However, the IL‐6and hs‐CRP levels did not predict the occurrence ofISR.Regression Analysis. In crude models, elevated
levels of IL‐6 correlated with an increased rate ofcardiac death or MI, cardiac death, all‐cause death, MI,and MACE (Table 2). This correlation was further
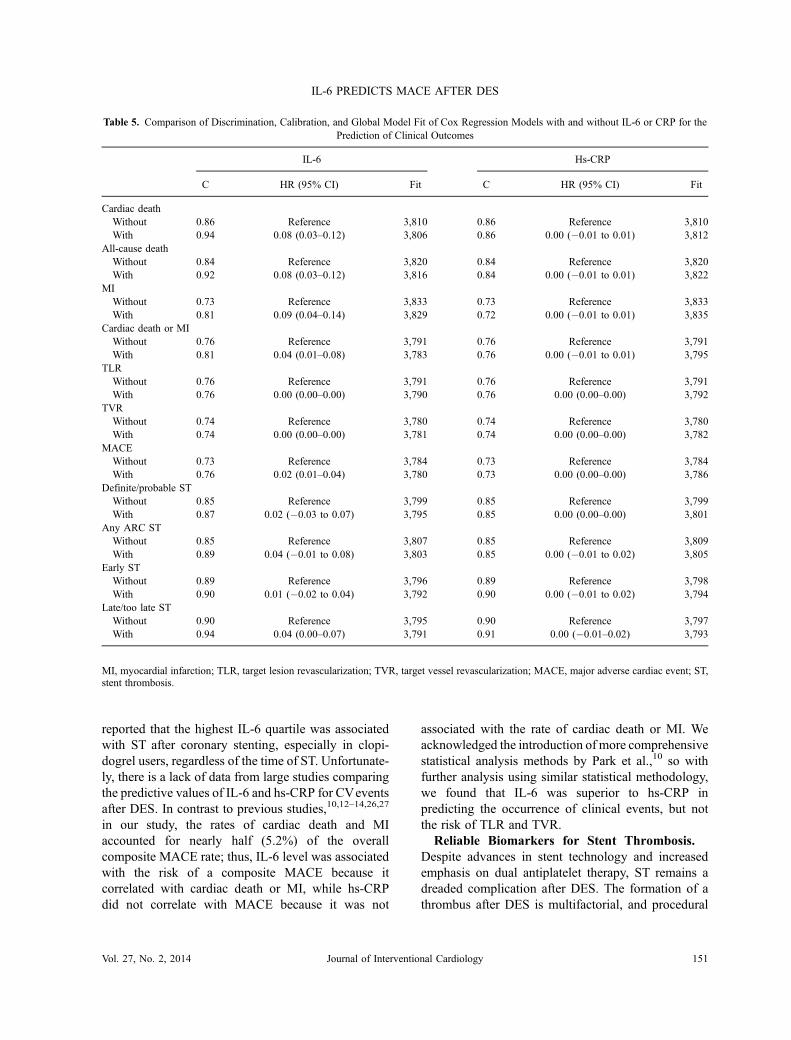
confirmed by a multivariable adjusted model. ElevatedIL‐6 levels were also a strong independent predictivefactor for definite and probable, any ARC‐defined,early and late, and too late ST by either crude ormultivariable adjusted models. There was no correla-tion of elevated hs‐CRP levels with the risk ofindividual clinical end‐point or the composite MACE(Table 3). Neither the crudemodel nor themultivariablemodel supported elevated hs‐CRP as an independentpredictive factor for definite and probable, early, or lateand too late ST. Interestingly, the crude model showedthat an hs‐CRP level �3mg/L was an independentpredictive factor for any ARC‐defined ST. Aftermultivariable adjustment for all confounding factorsfor ST, this independent association between thehs‐CRP level and the risk of any ARC‐defined STdisappeared (HR 2.12, 95% CI 0.881–5.133,P¼ 0.093). Table 4 demonstrates that IL‐6 levels hada stronger predictive value for definite and probable,any ARC‐defined and early ST according to the Z test.When the relation of IL‐6 or hs‐CRP levels to late‐occurring definite or probable ST was assessed,increasing IL‐6 levels were significantly associatedwith increased risks of late and too late ST (discrimi-nation 0.20, 95% CI 0.03–0.36, Z¼ 2.38, P¼ 0.0173),with a cut‐off value of 10.48 pg/ml (sensitivity 93.8%,specificity 72%). Table 5 summarizes the enhancedpower of IL‐6 over hs‐CRP and the traditional riskfactors for the prediction of cardiac death or MI andother events. After incorporation of IL‐6, the c statistic
Table 2. Crude and Multivariable Associations of Elevated IL‐6 Levels with Clinical Outcomes
Outcome
Crude Multivariable Adjusted
HR/(95% CI) P‐Value HR/(95% CI) P‐Value
ClinicalCardiac death 1.397 (1.323–1.475) <0.001 1.697 (1.453–1.981) <0.001All‐cause death 1.350 (1.278–1.426) <0.001 1.633 (1.431–1.864) <0.001MI 1.230 (1.144–1.324) <0.001 1.213 (1.092–1.348) <0.001Death or MI 1.303 (1.240–1.368) <0.001 1.337 (1.234–1.449) <0.001TLR 1.023 (0.932–1.122) 0.632 1.039 (0.929–1.161) 0.504TVR 1.034 (0.955–1.121) 0.408 1.044 (0.945–1.154) 0.392MACE 1.195 (1.138–1.245) <0.001 1.189 (1.117–1.264) <0.001
Stent thrombosisDefinite/probable 1.274 (1.133–1.434) <0.001 1.304 (1.088–1.563) 0.004Any 1.314 (1.214–1.421) <0.001 1.281 (1.115–1.472) <0.001Early 1.282 (1.137–1.446) <0.001 1.640 (1.203–2.235) 0.002Late/too late 1.344 (1.211–1.491) <0.001 1.306 (1.047–1.629) 0.018
MI, myocardial infarction; TLR, target lesion revascularization; TVR, target vessel revascularization; MACE, major adverse cardiac event.
148 Journal of Interventional Cardiology Vol. 27, No. 2, 2014
CHEN, ET AL.

increased significantly for the prediction of cardiacdeath or MI, cardiac death, all‐cause death, MI, and thecomposite MACE; there was no change for theprediction of TLR or TVR. Compared to the roughmodel, the c statistic with the addition of hs‐CRPshowed a nonsignificant slight increment for theprediction of definite and probable, any ARC‐definedand early ST. Importantly, when late‐occurring definiteand probable STwas analyzed, the c statistic increasedsignificantly (95% CI 0.00–0.007) after the addition ofIL‐6. In contrary, the c statistic and conventionalbaseline variables showed no change, a slight incre-ment, or even a decrement after the addition of hs‐CRP.
Discussion
The present study, to our knowledge, is the first studycomparing the predictive value of baseline IL‐6 and hs‐CRP levels for MACE after implantation of a DES in alarge cohort of consecutive patients with UA notalready on statin therapy. The major findings includedthe following24: Increased IL‐6 levels were associatedwith an increased risk of cardiac death or MI, with aresulting incremental value in predicting the compositeMACE, and25 IL‐6 was a stronger independentpredictive factor of late and too late ST.Inflammation as Biomarkers. Cardiac death and
MI are devastating complications after PCI. In order topredict these complications, several biomarkers have
been identified and their assays developed. However,their ability to predict hard outcomes after PCI remainslimited. As the evidence for atherosclerosis being aninflammatory disease increased,24 several inflammato-ry biomarkers have been identified, with hs‐CRP beingthe most popular. Several studies have reported the roleof either “baseline”10,12–14,26,27 or post‐DES11,13,28
levels of hs‐CRP in predicting ST after PCI. However,the level of these inflammatory biomarkers aresignificantly influenced by several factors, includingthe patient’s clinical status, mechanical endothelialinjury resulting from the PCI, edge dissection,apposition of struts, and medications,16,17 such asstatins. Regardless of whether a BMS or DES is usedand whether the patient presents with stable angina orNSTEMI, concentration of inflammatory cytokinesincreases immediately after stenting,29 suggesting thatthe elevation of inflammatory cytokines is related to theprocedure.30 HMG‐CoA reductase inhibitors (statins)have been shown to significantly decrease levels of hs‐CRP and other inflammatory biomarkers.31 In many ofthe aforementioned studies on hs‐CRP, the use ofstatins before admission and after the PCI procedurewas not precisely defined, which might explain the lackof consistency regarding the predictive value ofhs‐CRP for CV events after PCI. This drawback ofprevious studies was overcome in our study byexcluding patients already on statins, which establishedthe association of “real baseline” values of inflamma-tory biomarkers with the risk of clinical events.
Table 3. Crude and Multivariable Associations of Elevated CRP with Clinical Outcomes
Outcome
Crude Multivariable Adjusted
HR/(95% CI) P‐Value HR/(95% CI) P‐Value
ClinicalCardiac death 1.439 (0.834–2.481) 0.191 2.352 (0.957–5.784) 0.062All‐cause death 1.272 (0.801–2.021) 0.308 1.363 (0.639–2.907) 0.422MI 1.267 (0.850–1.888) 0.245 1.007 (0.573–1.770) 0.979Death or MI 1.262 (0.897–1.773) 0.181 1.067 (0.669–1.449) 0.786TLR 0.911 (0.641–1.295) 0.605 1.107 (0.695–1.765) 0.668TVR 0.895 (0.658–1.218) 0.481 0.976 (0.648–1.471) 0.908MACE 1.024 (0.814–1.289) 0.837 0.954 (0.709–1.283) 0.754
Stent thrombosisDefinite/probable 1.666 (0.799–3.473) 0.173 1.305 (0.417–4.080) 0.648Any 1.802 (1.020–3.183) 0.043 2.126 (0.881–5.133) 0.093Early 2.035 (0.946–4.377) 0.069 1.470 (0.102–21.205) 0.777Late/too late 1.554 (0.664–3.639) 0.310 3.186 (0.771–13.160) 0.109
MI, myocardial infarction; TLR, target lesion revascularization; TVR, target vessel revascularization; MACE, major adverse cardiac event.
Vol. 27, No. 2, 2014 Journal of Interventional Cardiology 149
IL‐6 PREDICTS MACE AFTER DES

Comparison between Biomarkers. So the ques-tion is which biomarker is better for predicting clinicalevents after DES. hs‐CRP is the most studiedbiomarker because it can be easily and inexpensivelymeasured with too high sensitivity. Six studies10,12–14,26,27 using DES for patients with angina (either stableor unstable) reported the consistent result that anelevated hs‐CRP level was associated with the risk ofdeath or ST, but did not predict the occurrence of ISR orTVR. Similarly, serum levels of matrix metalloprotei-nase, plasminogen activator inhibitor‐1, and thecomplement components C3a and C5a have been
demonstrated to be associated with the occurrenceof angiographic ISR.23,32,33 Notably, IL‐6, as theupstream mediator of CRP, could theoreticallybe expected to behave at least similarly to hs‐CRP inpredicting prognosis after implantation of a DES. IL‐6has been reported to be an independent predictor oflong‐term risk of death or heart failure in patients withacute coronary syndromes.21 A study by Kang et al.28
failed to demonstrate an association between changesin the hs‐CRP or IL‐6 levels and neointimal hyperpla-sia, evaluated by IVUS, following SES or PESdeployment. Furthermore, Hwang et al.22 recently
Table 4. Comparison of Area Under the ROC Curve between IL‐6 Versus CRP
Variables Area 95% CI SE Z P‐Value
Definite/probable STIL‐6 0.67 0.54–0.81 0.070 2.47 0.0067CRP 0.60 0.49–0.72 0.059 1.73 0.0417IL‐6 vs. CRP 0.07 �0.11 to 0.25 0.090 0.79 0.4304
Any ARC defined STIL‐6 0.72 0.63–0.81 0.046 4.86 <0.0001CRP 0.62 0.52–0.71 0.046 2.60 0.0047IL‐6 vs. CRP 0.10 �0.02 to 0.23 0.063 1.65 0.0990
Cardiac deathIL‐6 0.84 0.79–0.89 0.024 14.11 <0.0001CRP 0.56 0.47–0.65 0.045 1.37 0.0848IL‐6 vs. CRP 0.28 0.17–0.39 0.055 5.04 <0.0001
All‐cause deathIL‐6 0.75 0.68–0.82 0.037 6.90 <0.0001CRP 0.54 0.47–0.61 0.037 1.12 0.1314IL‐6 vs. CRP 0.21 0.11–0.31 0.050 4.22 <0.0001
MIIL‐6 0.64 0.58–0.71 0.032 4.52 <0.0001CRP 0.55 0.48–0.61 0.033 1.38 0.0830IL‐6 vs. CRP 0.10 0.02–0.17 0.038 2.60 0.0093
Cardiac death or MIIL‐6 0.70 0.65–0.75 0.026 7.61 <0.0001CRP 0.54 0.49–0.60 0.028 1.54 0.0615IL‐6 vs. CRP 0.15 0.089–0.22 0.035 4.46 <0.0001
TLRIL‐6 0.52 0.46–0.57 0.028 0.68 0.2469CRP 0.49 0.43–0.55 0.029 �0.38 0.6465IL‐6 vs. CRP 0.01 �0.08 to 0.10 0.046 0.19 0.8516
TVRIL‐6 0.53 0.48–0.58 0.025 1.15 0.1253CRP 0.49 0.44–0.54 0.025 �0.46 0.6777IL‐6 vs. CRP �0.02 �0.10 to 0.06 0.041 �0.41 0.6821
MACEIL‐6 0.61 0.57–0.65 0.020 5.52 <0.0001CRP 0.51 0.47–0.55 0.020 0.41 0.3413IL‐6 vs. CRP 0.10 0.06–0.15 0.024 4.3 <0.0001
IL, interleukin; CRPhs, high‐sensitivity C‐reactive protein; ST, stent thrombosis; MI, myocardial infarction; TLR, target lesion revascularization;TVR, target vessel revascularization; MACE, major adverse cardiac event.
150 Journal of Interventional Cardiology Vol. 27, No. 2, 2014
CHEN, ET AL.
reported that the highest IL‐6 quartile was associatedwith ST after coronary stenting, especially in clopi-dogrel users, regardless of the time of ST. Unfortunate-ly, there is a lack of data from large studies comparingthe predictive values of IL‐6 and hs‐CRP for CVeventsafter DES. In contrast to previous studies,10,12–14,26,27
in our study, the rates of cardiac death and MIaccounted for nearly half (5.2%) of the overallcomposite MACE rate; thus, IL‐6 level was associatedwith the risk of a composite MACE because itcorrelated with cardiac death or MI, while hs‐CRPdid not correlate with MACE because it was not
associated with the rate of cardiac death or MI. Weacknowledged the introduction of more comprehensivestatistical analysis methods by Park et al.,10 so withfurther analysis using similar statistical methodology,we found that IL‐6 was superior to hs‐CRP inpredicting the occurrence of clinical events, but notthe risk of TLR and TVR.Reliable Biomarkers for Stent Thrombosis.
Despite advances in stent technology and increasedemphasis on dual antiplatelet therapy, ST remains adreaded complication after DES. The formation of athrombus after DES is multifactorial, and procedural
Table 5. Comparison of Discrimination, Calibration, and Global Model Fit of Cox Regression Models with and without IL‐6 or CRP for thePrediction of Clinical Outcomes
IL‐6 Hs‐CRP
C HR (95% CI) Fit C HR (95% CI) Fit
Cardiac deathWithout 0.86 Reference 3,810 0.86 Reference 3,810With 0.94 0.08 (0.03–0.12) 3,806 0.86 0.00 (�0.01 to 0.01) 3,812
All‐cause deathWithout 0.84 Reference 3,820 0.84 Reference 3,820With 0.92 0.08 (0.03–0.12) 3,816 0.84 0.00 (�0.01 to 0.01) 3,822
MIWithout 0.73 Reference 3,833 0.73 Reference 3,833With 0.81 0.09 (0.04–0.14) 3,829 0.72 0.00 (�0.01 to 0.01) 3,835
Cardiac death or MIWithout 0.76 Reference 3,791 0.76 Reference 3,791With 0.81 0.04 (0.01–0.08) 3,783 0.76 0.00 (�0.01 to 0.01) 3,795
TLRWithout 0.76 Reference 3,791 0.76 Reference 3,791With 0.76 0.00 (0.00–0.00) 3,790 0.76 0.00 (0.00–0.00) 3,792
TVRWithout 0.74 Reference 3,780 0.74 Reference 3,780With 0.74 0.00 (0.00–0.00) 3,781 0.74 0.00 (0.00–0.00) 3,782
MACEWithout 0.73 Reference 3,784 0.73 Reference 3,784With 0.76 0.02 (0.01–0.04) 3,780 0.73 0.00 (0.00–0.00) 3,786
Definite/probable STWithout 0.85 Reference 3,799 0.85 Reference 3,799With 0.87 0.02 (�0.03 to 0.07) 3,795 0.85 0.00 (0.00–0.00) 3,801
Any ARC STWithout 0.85 Reference 3,807 0.85 Reference 3,809With 0.89 0.04 (�0.01 to 0.08) 3,803 0.85 0.00 (�0.01 to 0.02) 3,805
Early STWithout 0.89 Reference 3,796 0.89 Reference 3,798With 0.90 0.01 (�0.02 to 0.04) 3,792 0.90 0.00 (�0.01 to 0.02) 3,794
Late/too late STWithout 0.90 Reference 3,795 0.90 Reference 3,797With 0.94 0.04 (0.00–0.07) 3,791 0.91 0.00 (�0.01–0.02) 3,793
MI, myocardial infarction; TLR, target lesion revascularization; TVR, target vessel revascularization; MACE, major adverse cardiac event; ST,stent thrombosis.
Vol. 27, No. 2, 2014 Journal of Interventional Cardiology 151
IL‐6 PREDICTS MACE AFTER DES

characteristics are thought to correlate with the risk ofearly ST. Immediately after coronary stenting, the levelof inflammatory cytokines increases.29 More impor-tantly, the elevated concentrations of inflammatorycytokines normalize within a couple of weeks,27,34,35
and their impact on the clinical outcome is yet unclear.Previous studies21,3–9,11–14,22,27,29,30,31,34,35 did notfind hs‐CRP to be a predictor of ST, a finding replicatedby our study as well. In contrary, our multivariateanalysis determined that IL‐6, a predecessor of hs‐CRP,was a significantly reliable biomarker in prediction ofST. First, our observation was that the crude model andZ test were insufficient to provide the comparison of IL‐6 with hs‐CRP for the prediction of events, whencompared with multivariate adjusted model anddiscrimination analysis. Then, when late‐occurringdefinite or probable ST was assessed, the results fromthe crude, multivariate‐adjusted, Z test and discrimina-tion analyses reached a consistent finding: IL‐6 levelshad an incremental value in predicting late‐occurringdefinite or probable ST, suggesting that IL‐6 is a
reliable biomarker for the prediction of late‐occurringdefinite or probable ST because early ST is generallyrelated to the procedure itself. So, in the light of theresults by Hwang et al.,22 our data confirmed that IL‐6is a stable, comprehensive inflammatory biomarker forprediction of cardiac death or MI and late‐occurringdefinite or probable ST after DES placement (Table 6).Limitations. The present study had several limi-
tations. We did not measure other markers, such aseosinophil cationic protein,14 which has been reportedto be a more powerful biomarker in predicting CVevents after DES. However, since IL‐6 and hs‐CRP are2 easy and inexpensive measures, results from thepresent study have a stronger clinical relevance.Second, the dynamic changes of IL‐6 and hs‐CRPlevels after the PCI procedure were not routinelymeasured. Thus, we could not calculate their associa-tion with the risk of clinical events. According to thedesign of the current study, all patients were prescribeda statin immediately after admission.We do believe thatour real baseline biomarker levels are moremeaningful.
Table 6. Multivariable‐Adjusted� Hazard Ratios for Cardiac Death or MI, MACE, and Stent Thrombosis According to CRP or IL‐6 Levels Usingthe Pre‐Specific Classification and a Continuous Model
IL‐6 Hs‐CRP
HR 95% CI P‐Value HR 95% CI P‐Value
Cardiac death or MI#
Pre‐specific definedLow risk 1 (Ref) NoAverage risk 0.847 0.486–1.476 0.558 1 (Ref)High risk 1.231 1.076–1.408 0.003 0.638 0.169–2.404 0.507
Continuous model1‐SD increment�� 531.765 34.704–8148.160 <0.001 0.087 0.012–699.129 0.594
MACE#
Pre‐specific definedLow risk Reference NoAverage risk 1.123 0.849–1.486 0.416 1 (Ref)High risk 1.253 1.125–1.395 <0.001 0.417 0.165–1.056 0.065
Continuous model1‐SD increment�� 110.418 22.388–544.579 <0.001
Definite/probable ST#
Pre‐specific definedLow risk Reference NoAverage risk 0.247 0.057–1.061 0.060 1 (Ref)High risk 1.313 1.103–1.563 0.002 0.387 0.034–4.409 0.444
Continuous model1‐SD increment�� 1177.046 1028.1–1347.6 0.003 0.802 0.166–3.861 0.783
#For comparison of 3 groups by CDC/AHA cutoff points, P values for trend were denoted. ��Hazard ratios correspond to a 1‐SD increment in thenatural logarithm of CRP value.MI, myocardial infarction;MACE,major adverse cardiac event; ST, stent thrombosis. �Adjusted for covariates (fora list of covariates).
152 Journal of Interventional Cardiology Vol. 27, No. 2, 2014
CHEN, ET AL.

Third, we did not monitor whether patients’ lipidprofiles reached target levels. This would at leastpartially mask the impact of inflammatory status duringfollow‐up on event‐free survival rates. Since our maingoal was to identify the correlation of baselineinflammatory biomarkers with clinical events, andnearly 90% of patients took statin for 1 year after a DESplacement, patients’ lipid profiles during follow‐uphave less impact on our study goal. Fourth, we did notcompare the effect of pretreatment with a statin on thepredictive value of baseline inflammatory biomarkersfor more severe events, which will be our study in anear future. Finally, we did not compare the differencein ST between different DES, as the selection of stentwas at physician’s discretion.
Conclusion
IL‐6, an easily measured inflammatory marker, hadan incremental predictive value for cardiac death or MIand late‐occurring definite or probable ST after theimplantation of a DES among patients with UA whohad not received pretreatment with a statin. The use ofIL‐6 as an adjunct to the conventional assessments ofpatients, lesions, and procedural characteristics issuperior to hs‐CRP in identifying high‐risk patients.
References
1. Park DW, Seung KB, Kim YH, et al. Long‐term safety andefficacy of stenting versus coronary artery bypass grafting forunprotected left main coronary artery disease: 5‐year results fromthe MAIN‐COMPARE registry. J Am Coll Cardiol2010;56:117–124.
2. Mauri L, Hsieh WH, Massaro JM, et al. Stent thrombosis inrandomized clinical trials of drug‐eluting stents. N Engl J Med2007;356:1020–1029.
3. Buffon A, Liuzzo G, Biasucci LM, et al. Preprocedural serumlevels of C‐reactive protein predict early complications and laterestenosis after coronary angioplasty. JACC 1999;34:1512–1521.
4. Versaci F, Gaspardone A, Tomai F, et al. Predictive value of C‐reactive protein in patients with unstable angina pectorisundergoing coronary artery stent implantation. Am J Cardiol2000;85:92–95.
5. Chew DP, Bhatt DL, Robbins MA, et al. Incremental prognosticvalue of elevated baseline C‐reactive protein among establishedmarkers of risk in percutaneous coronary intervention. Circula-tion 2001;104:992–997.
6. Palmerini T, Marzocchi A, Marrozzini C, et al. Preprocedurallevels of C‐reactive protein and leukocyte counts predict 9‐month mortality after coronary angioplasty for the treatment ofunprotected left main coronary artery stenosis. Circulation2005;112:2332–2338.
7. Fournier JA, Delgado‐Pecellín C, Cayuela A, et al. The high‐sensitivity C‐reactive protein level one month after bare‐metal
coronary stenting may predict late adverse events. Rev EspCardiol 2008;61:313–1316.
8. de Winter RJ, Koch KT, van Straalen JP, et al. Creactive proteinand coronary events following percutaneous coronary angio-plasty. Am J Med 2003;115:85–90.
9. Gach O, Legrand V, Biessaux Y, et al. Long‐term prognosticsignificance of high‐sensitivity C‐reactive protein before andafter coronary angioplasty in patients with stable angina pectoris.Am J Cardiol 2007;99:31–35.
10. ParkDW,Yun SC, Lee JY, et al. C‐reactive protein and the risk ofstent thrombosis and cardiovascular events after drug‐elutingstent implantation. Circulation 2009;120:1987–1995.
11. Gaspardone A, Versaci F, Tomai F, et al. C‐reactive protein,clinical outcome, and restenosis rates after implantation ofdifferent drug eluting stents. Am J Cardiol 2006;97:1311–1316.
12. Choi DH, Park KW, Yang HM, et al. Renal dysfunction and highlevels of hsCRP are additively associated with hard endpointsafter percutaneous coronary intervention with drug elutingstents. Int J Cardiol 2011;149:174–181.
13. Dibra A, Ndrepepa G, Mehilli J, et al. Comparison of C‐reactiveprotein levels before and after coronary stenting and restenosisamong patients treated with sirolimus‐eluting versus bare metalstents. Am J Cardiol 2005;95:1238–1240.
14. Niccoli G, Schiavino D, Belloni F, et al. Pre‐interventioneosinophil cationic protein serum levels predict clinical out-comes following implantation of drug‐eluting stents. Eur Heart J2009;30:1340–1347.
15. Davignon J. Beneficial cardiovascular pleiotropic effects ofstatins. Circulation 2004;109:11139–11143.
16. Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin toprevent vascular events in men and women with elevatedC‐reactive protein. NEJM 2008;359:2195–2207.
17. Kubota N, Kasai T, Miyauchi K, et al. Therapy with statins andaspirin enhances long‐term outcome of percutaneous coronaryintervention. Heart Vessels 2008;23:35–39.
18. Pasceri V, Patti G, Nusca A, et al. Randomized trial ofatorvastatin for reduction of myocardial damage during coronaryintervention: Results from the ARMYDA study. Circulation2004;110:674–678.
19. Niccoli G, Montone RA, Ferrante G, et al. The evolving role ofinflammatory biomarkers in risk assessment after stent implan-tation. J Am Coll Cardiol 2010;56:1783–1793.
20. Tousoulis D, Papageorgiou N, Stefanadis C. Is C‐reactive proteina prognostic marker after angioplasty? Heart 2009;95:957–959.
21. Lindmark E, Diderholm E, Wallentin L, et al. Relationshipbetween interleukin‐6 and mortality in patients with unstablecoronary artery disease: Effects of an early invasive ornoninvasive strategy. JAMA 2001;286:2107–2113.
22. Hwang SJ, Park KW, KwonDA, et al. High plasma interleukin‐6is associated with drug‐eluting stent thrombosis‐possible role ofinflammatory cytokines in the development of stent thrombosisfrom the Korea stent registry. Circ J 2011;75:1350–1357.
23. Katsaros KM, Speidl WS, Kastl SP, et al. Plasminogen activatorinhibitor‐1 predicts coronary in‐stent restenosis of drug‐elutingstents. J Thromb Haemost 2008;6:508–513.
24. Libby P, Ridker PM, Maseri A. Inflammation and atherosclero-sis. Circulation 2002;105:1135–1143.
25. Rifai N, Ridker PM. Inflammatory markers and coronary heartdisease. Curr Opin Lipidol 2002;13:383–389.
26. Delhaye C, Maluenda G, Wakabayashi K, et al. Long‐termprognostic value of preprocedural C‐reactive protein after drug‐eluting stent implantation. Am J Cardiol 2010;105:826–832.
27. Park DW, Lee CW, Yun SC, et al. Prognostic impact ofpreprocedural C reactive protein levels on 6‐month angiographicand 1‐year clinical outcomes after drug‐eluting stent implanta-tion. Heart 2007;93:1087–1092.
Vol. 27, No. 2, 2014 Journal of Interventional Cardiology 153
IL‐6 PREDICTS MACE AFTER DES

28. KangWC,AhnTH,MoonCI, et al. Comparison of inflammatorymarkers and angiographic outcomes after implantation ofsirolimus and paclitaxel‐eluting stents. Heart 2009;95:970–975.
29. Gibson CM, Karmpaliotis D, Kosmidou I, et al. Comparison ofeffects of bare metal versus drug‐eluting stent implantation onbiomarker levels following percutaneous coronary interventionfor non‐ST‐elevation acute coronary syndrome. Am J Cardiol2006;97:1473–1477.
30. Saleh N, Svane B, Jensen J, et al. Stent implantation, but notpathogen burden, is associated with plasma C‐reactive proteinand interleukin‐6 levels after percutaneous coronary interventionin patients with stable angina pectoris. AHJ 2005;149:876–882.
31. Yoon SS, Dillon CF, Carroll M, et al. Effects of statins on seruminflammatory markers: The U.S. NHNES 1999–2004. JAtheroscler Thromb 2010;17:1176–1182.
32. Katsaros KM, Kastl SP, Zorn G, et al. Increased restenosis rateafter implantation of drug‐eluting stents in patients with elevatedserum activity of matrixmetalloproteinase‐2 and ‐9. JACC Interv2010;3:90–97.
33. Speidl WS, Katsaros KM, Kastl SP, et al. Coronary late lumenloss of drug eluting stents is associated with increased serumlevels of the complement components C3a and C5a. Atheroscle-rosis 2010;208:285–289.
34. Sardella G, Mariani P, D’Alessandro M, et al. Early elevation ofinterleukin‐1B and interleukin‐6 levels after bare or drug‐elutingstent implantation in patients with stable angina. Thromb Res2006;117:659–664.
35. Ozer N, Tangurek B, Firat F, et al. Effects of drug‐eluting stentson systemic inflammatory response in patients with unstableangina pectoris undergoing percutaneous intervention. HeartVessels 2008;23:75–82.
154 Journal of Interventional Cardiology Vol. 27, No. 2, 2014
CHEN, ET AL.
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具