
Childhood medulloblastoma: From genomics to improved...
45
Childhood medulloblastoma: From genomics to improved therapies Steve Clifford PhD
Transcript of Childhood medulloblastoma: From genomics to improved...
Childhood medulloblastoma:
From genomics to improved therapies
Steve Clifford PhD
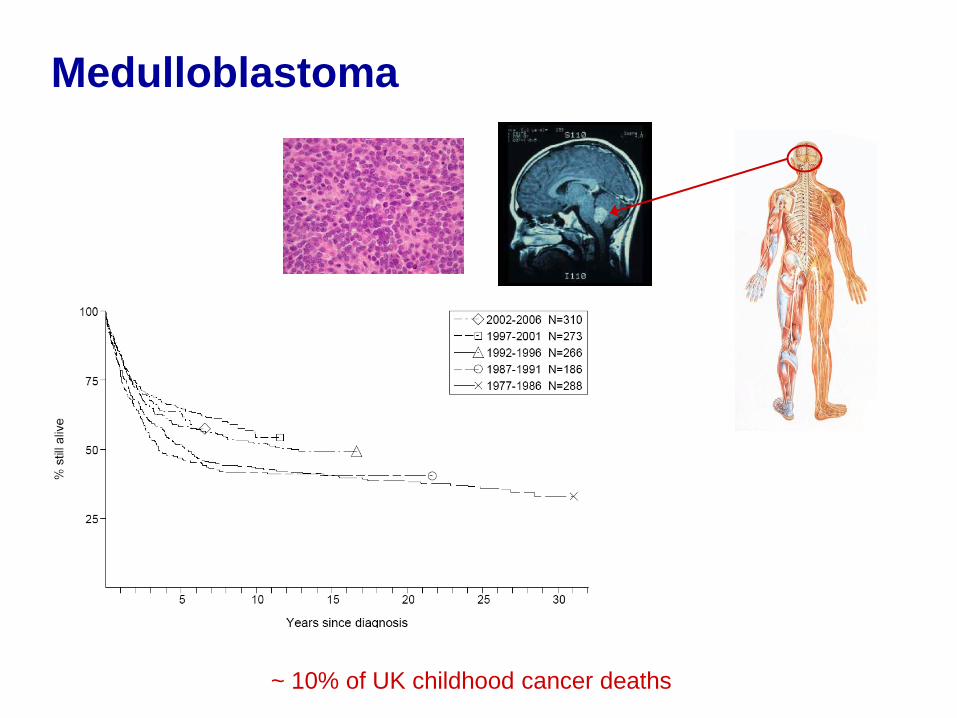
Medulloblastoma
~ 10% of UK childhood cancer deaths

Medulloblastoma:
Challenges and Goals
To improve outlook through :
Optimization and individualisation of current therapies
Maximisation of efficacy
Minimisation of side-effects
Development of new therapeutic approaches

Research Strategy
Clinical TrialsDevelopmental
Therapeutics
Exploratory Biology:
Biomarker and
Target Discovery
Translational research focused on improving
cancer therapy
Exploratory Biology:
Biomarker and Target
Identification

Li-Fraumeni syndrome family
S Clifford
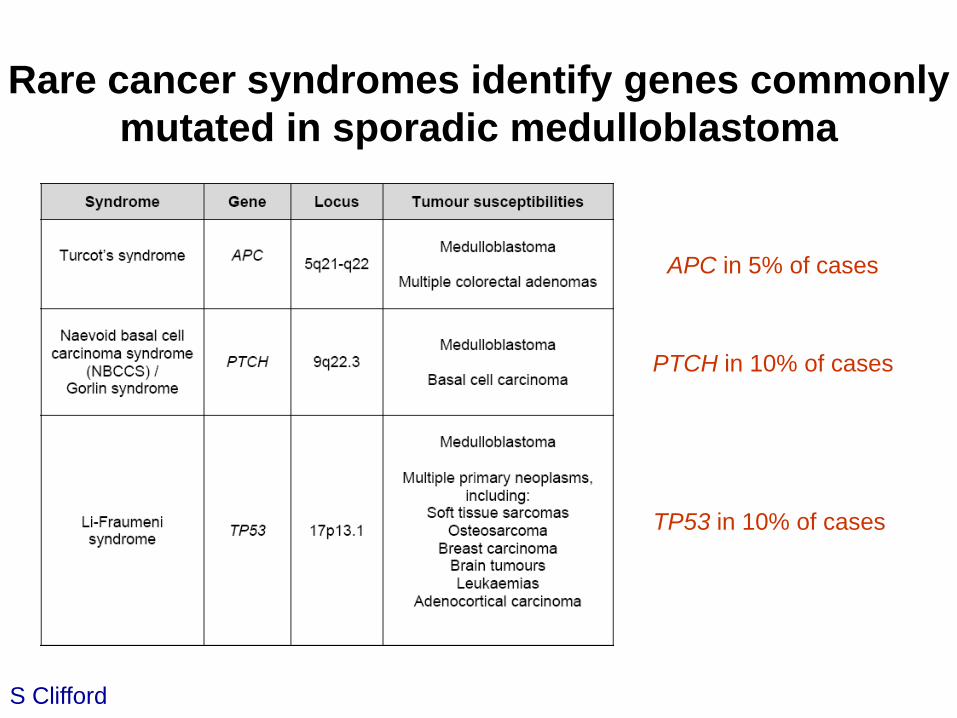
Rare cancer syndromes identify genes commonly
mutated in sporadic medulloblastoma
APC in 5% of cases
PTCH in 10% of cases
TP53 in 10% of cases
S Clifford
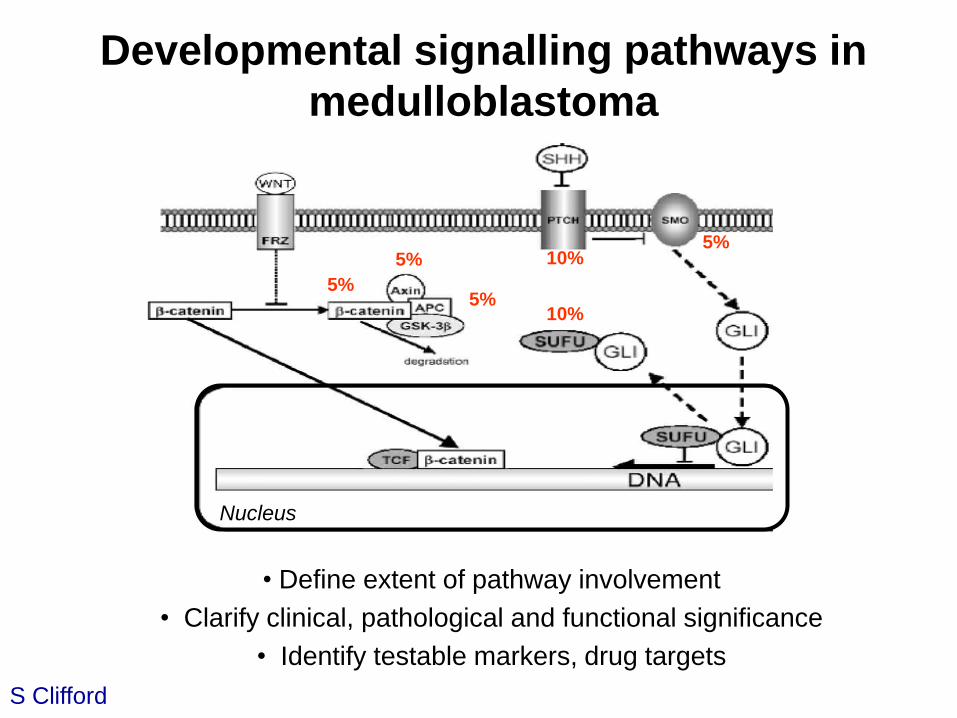
• Define extent of pathway involvement
• Clarify clinical, pathological and functional significance
• Identify testable markers, drug targets
5%
5%
5%
5%10%
10%
Nucleus
Developmental signalling pathways in
medulloblastoma
S Clifford

The SHH signalling pathway in
cerebellar development
Romer, J and Curran, T (2005). Cancer Research. 65: 4975.

SHH and Wnt/Wg
medulloblastoma subgroups
S Clifford
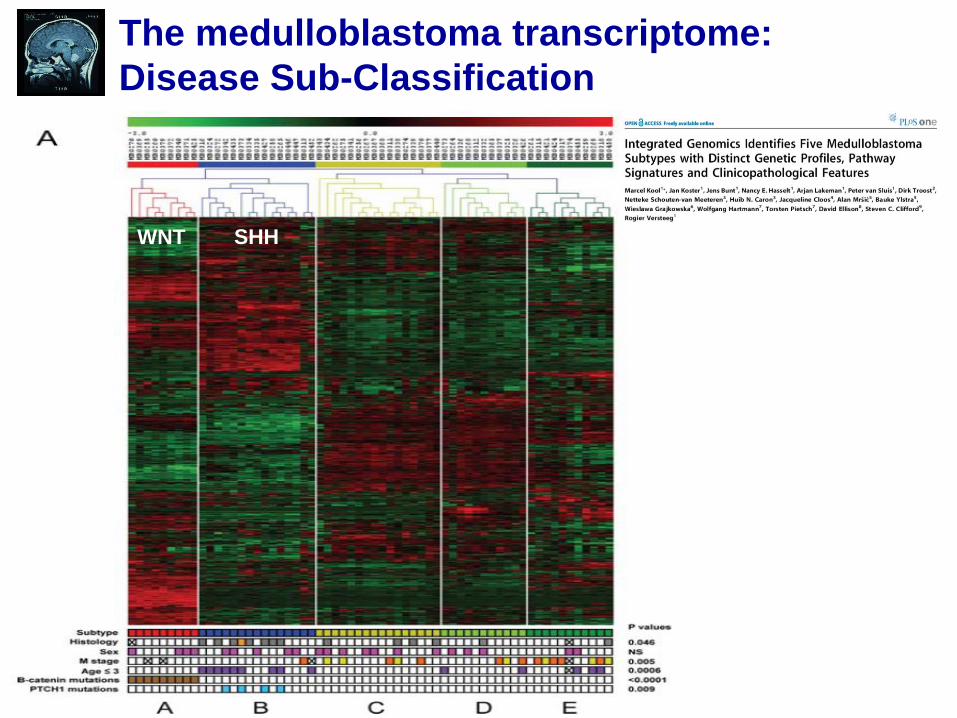
The medulloblastoma transcriptome:
Disease Sub-Classification
WNT SHH
Detailed molecular
characterisation of Wnt/Wg-active
medulloblastomas
S Clifford
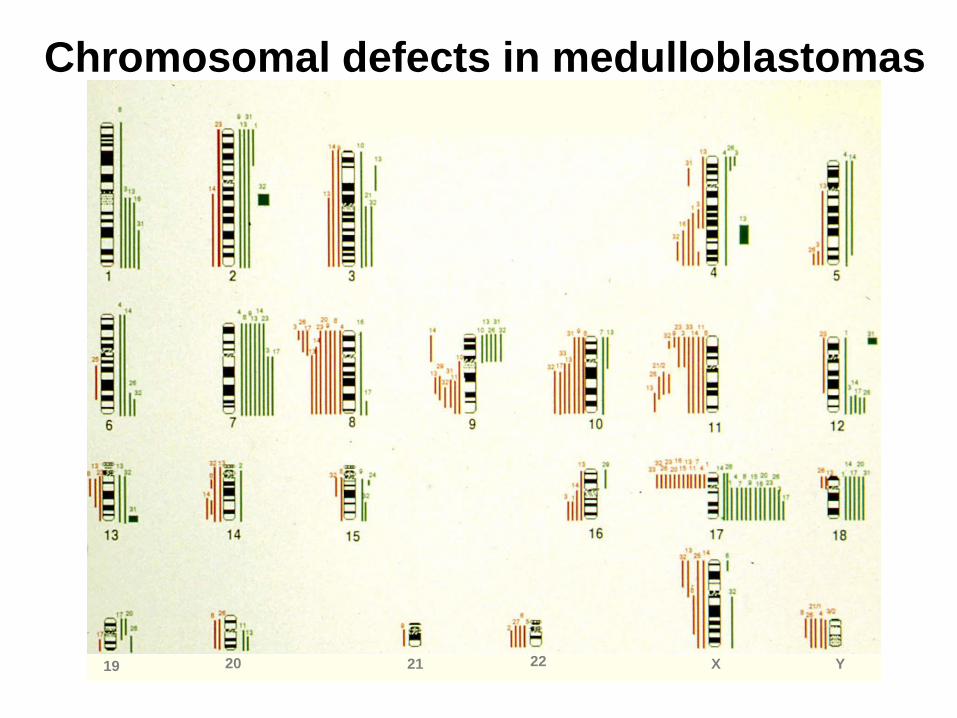
Chromosomal defects in medulloblastomas
19 20 21 22 X Y

Genomic analysis (array CGH):
Wnt/Wg sub-group medulloblastomas
• Monosomy 6 in all cases
• No evidence of
characteristic
medulloblastoma aberrations
(chr 7, 9, 16, 17 etc.)
• Few other defects
• Assessed 19 medulloblastomas
• Wnt/Wg activation
(b-catenin IHC; CTNNB1, APC
mutation)
• Associated chromosomal
defects
S Clifford
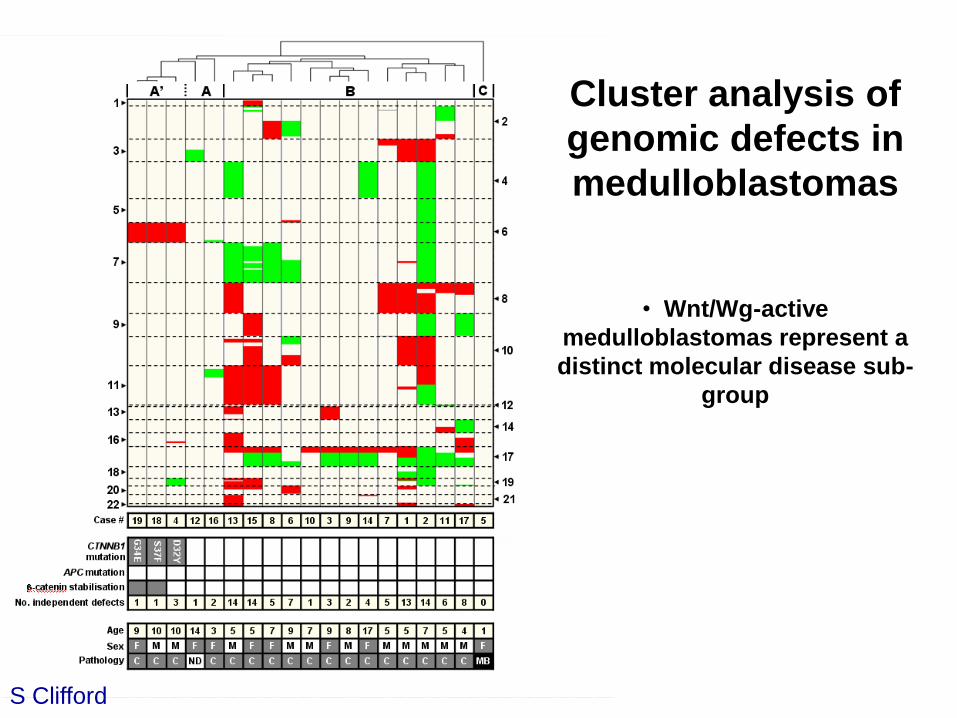
Cluster analysis of
genomic defects in
medulloblastomas
• Wnt/Wg-active
medulloblastomas represent a
distinct molecular disease sub-
group
S Clifford

DNA methylation, CpG islands
and epigenetic gene inactivation in cancer
Lindsey et al, 2005 Jones & Baylin. Nat Rev Genet., 2002
Wnt/Wg pathway activation and
chromosome 6 loss define a
distinct molecular sub-group of
medulloblastomas
S Clifford

Detailed molecular
characterisation of SHH-active
medulloblastomas
S Clifford
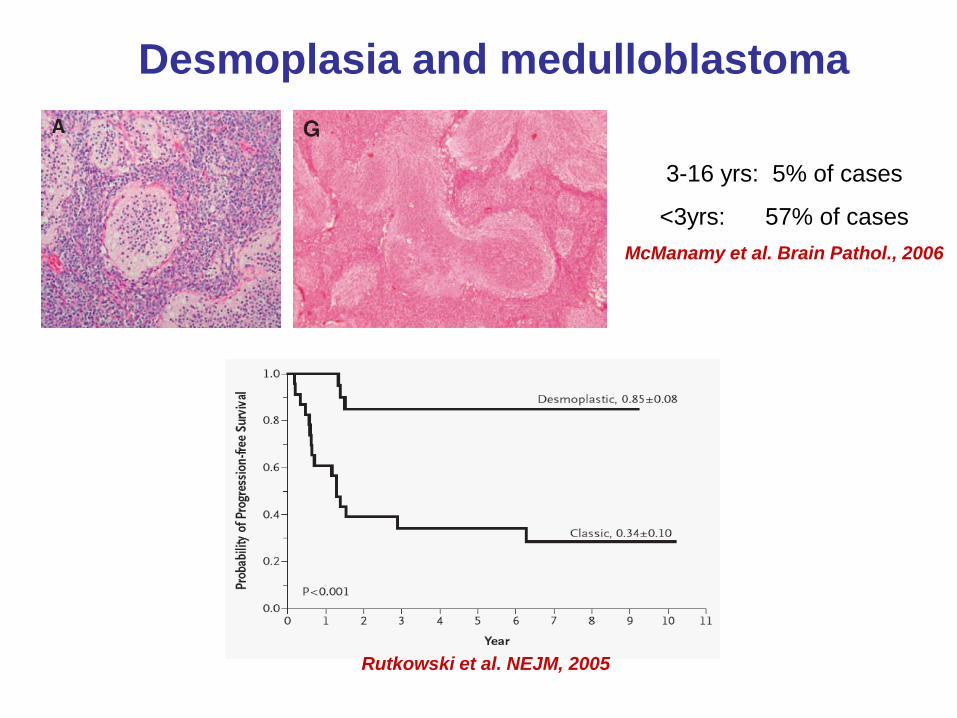
Desmoplasia and medulloblastoma
Rutkowski et al. NEJM, 2005
3-16 yrs: 5% of cases
<3yrs: 57% of cases
McManamy et al. Brain Pathol., 2006

Global analysis of the medulloblastoma epigenome:
Subgroup specific inactivation of COL1A2

A molecular sub-classification of
medulloblastoma
Pathway activation Wnt/Wg SHH ???
Major mutational
targets CTNNB1 PTCH1 ???
Marker
Chromosomal
defectsmono 6
15-25% ~60%~15%
b-catenin
stabilisation
mRNA
signature
17p loss (40%), 8p, 9q, 10q, 16q loss (all 30%), 7 gain,
MYC / MYCN amplification (each ~5%)
All FISH
Pathway activation SHH + SHH -
EpigeneticsCOL1A2 + COL1A2 -
Prognosis
Pathology desmoplastic
~50%~50%
Poor prognosisFavourable
prognosis
Non-
desmoplastic
Infant
medulloblastoma
(<3 yrs)

Biomarkers and Treatment
Individualisation

• SIOP / UKCCSG
• 1992-2000
• Pathology review and Biological studies - Newcastle
PNET3
S Clifford

1. Wnt/Wg sub-group tumours
S Clifford
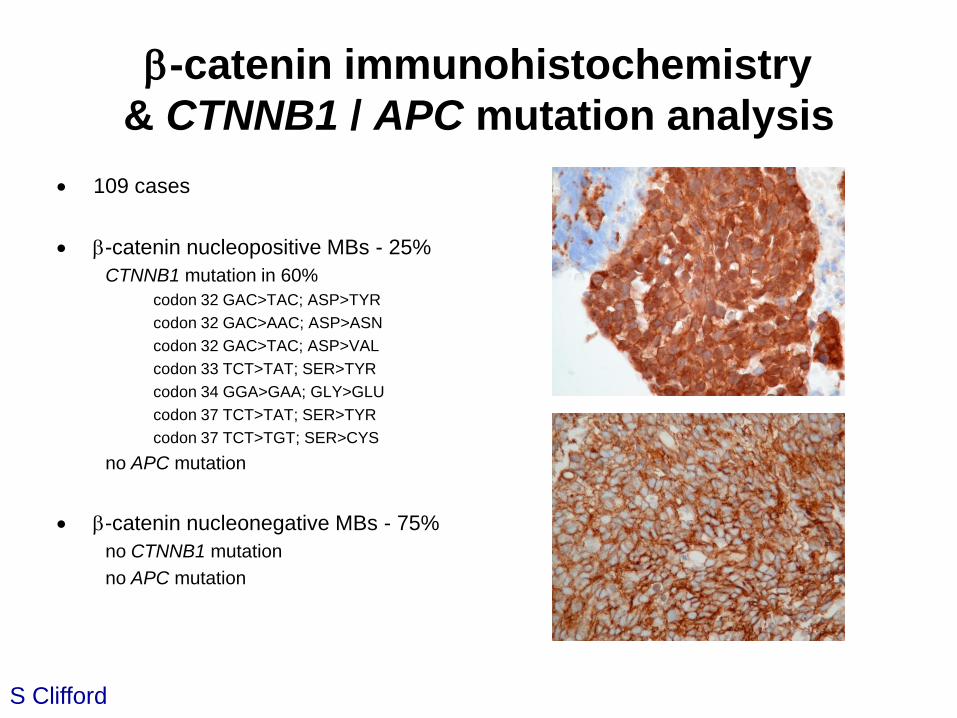
b-catenin immunohistochemistry
& CTNNB1 / APC mutation analysis
109 cases
b-catenin nucleopositive MBs - 25%
CTNNB1 mutation in 60%
codon 32 GAC>TAC; ASP>TYR
codon 32 GAC>AAC; ASP>ASN
codon 32 GAC>TAC; ASP>VAL
codon 33 TCT>TAT; SER>TYR
codon 34 GGA>GAA; GLY>GLU
codon 37 TCT>TAT; SER>TYR
codon 37 TCT>TGT; SER>CYS
no APC mutation
b-catenin nucleonegative MBs - 75%
no CTNNB1 mutation
no APC mutation
S Clifford
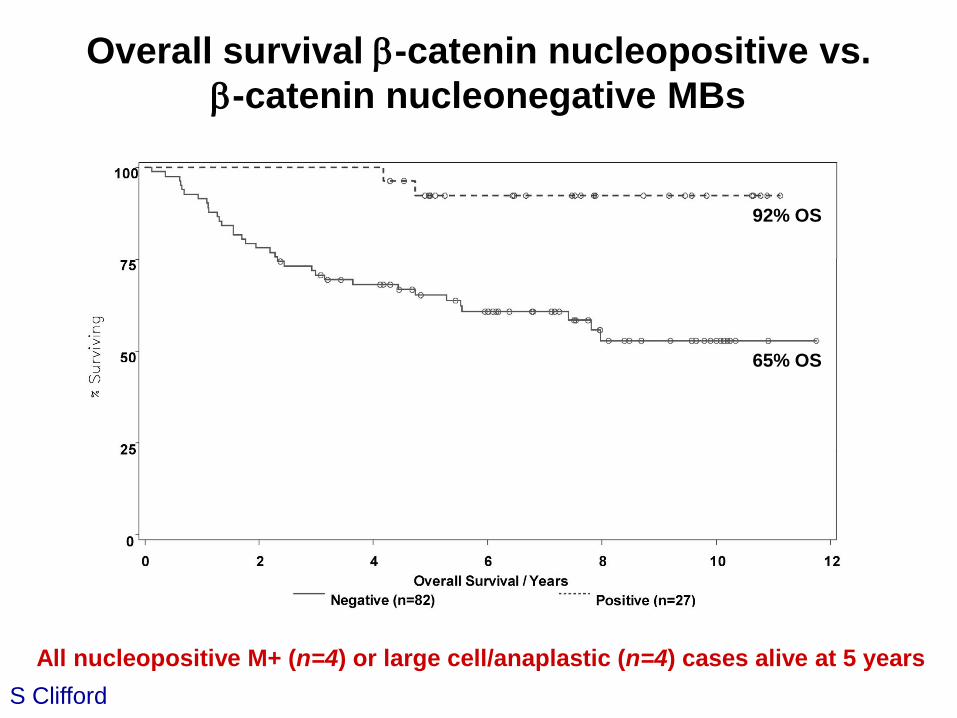
Overall survival b-catenin nucleopositive vs.
b-catenin nucleonegative MBs
92% OS
65% OS
All nucleopositive M+ (n=4) or large cell/anaplastic (n=4) cases alive at 5 years
S Clifford


Wnt activation assessed by b-catenin
immunostaining (15% of cases)
WNT group: 7 average, 3 high-risk
‘Other’ group: 42 average, 17 high-risk
Event-free survival - overall
2. MYC family amplification
S Clifford

Clinical Trials Biological Studies
in Medulloblastoma
• Markers showing consistent findings in ≥2 clinical trials cohorts
• Others (chromosome 17, ERBB2, TRKC etc) not yet validated

Putative medulloblastoma disease
risk stratification 2010 (≥3yrs old)• Favourable risk (~15%)
b-catenin nucleopositive and
MYC / MYCN non-amplified and
M0 and
Classic or desmoplastic histology
• Standard risk (~55%)b-catenin nucleonegative and
MYC / MYCN non-amplified and
M0 and
Classic or desmoplastic histology
• High risk (~30%)MYC / MYCN amplified or
M+ or
Large cell / anaplastic histology
b-catenin nucleopositive or nucleonegative
• Identification of further markers, validation and refinement ongoing
S Clifford
SIOP PNET Clinical trials:
PNET5 & PNET6 – biological stratification
• Starting 2010/11
• Upfront biological and pathological testing:
• Newcastle – UK / European co-ordinating centre
• Mandatory submission of frozen tumour material for testing
• ‘Real-time’ biological assessment for treatment stratification
• PNET5 – favourable risk medulloblastoma
• Reduced therapy / late-effects?
• PNET6 – standard risk medulloblastoma
• Maintain survival rates?
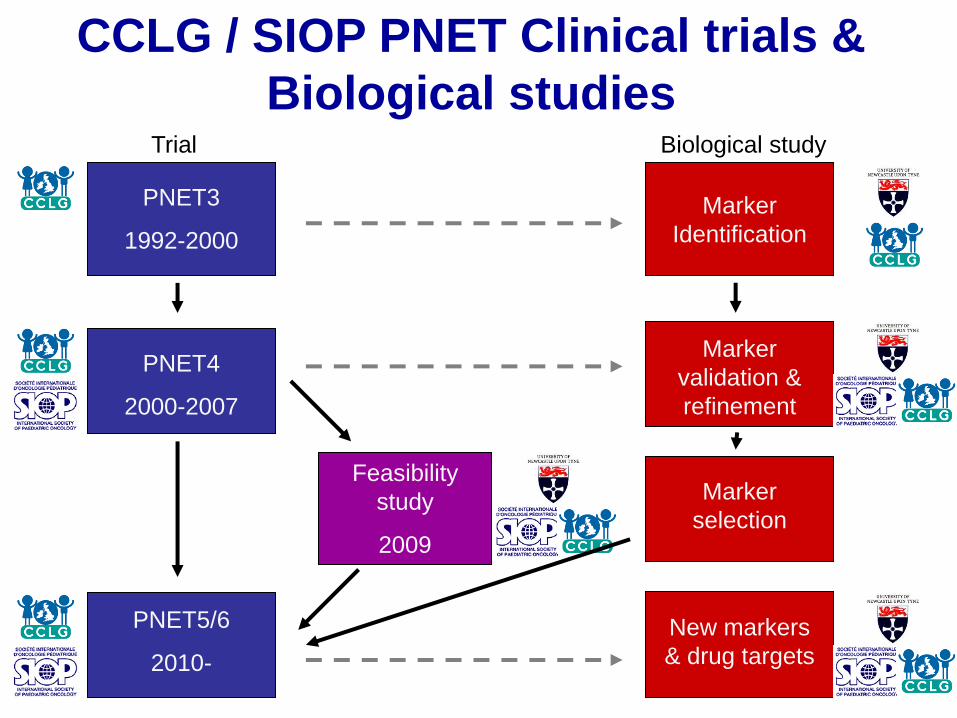
PNET3
1992-2000
PNET4
2000-2007
PNET5/6
2010-
Feasibility
study
2009
Marker
Identification
Marker
validation &
refinement
New markers
& drug targets
Marker
selection
CCLG / SIOP PNET Clinical trials &
Biological studiesTrial Biological study

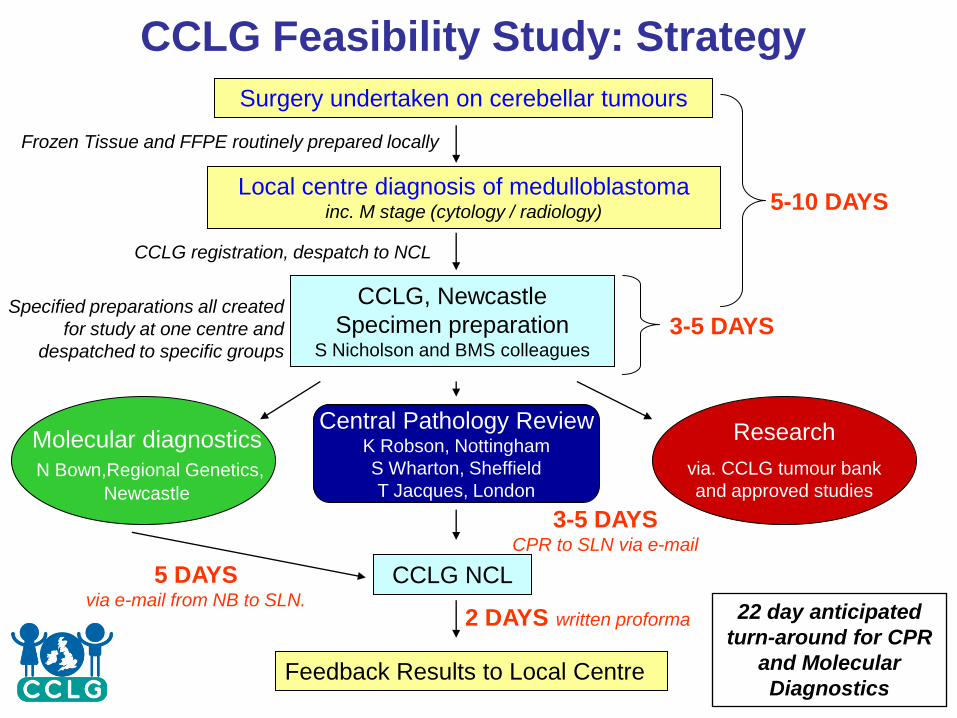
Surgery undertaken on cerebellar tumours
Local centre diagnosis of medulloblastomainc. M stage (cytology / radiology)
CCLG, Newcastle
Specimen preparation S Nicholson and BMS colleagues
Molecular diagnostics
N Bown,Regional Genetics,
Newcastle
CCLG NCL
Feedback Results to Local Centre
5 DAYSvia e-mail from NB to SLN.
3-5 DAYS
5-10 DAYS
3-5 DAYS CPR to SLN via e-mail
2 DAYS written proforma
Research
via. CCLG tumour bank
and approved studies
Frozen Tissue and FFPE routinely prepared locally
CCLG registration, despatch to NCL
Specified preparations all created
for study at one centre and
despatched to specific groups
22 day anticipated
turn-around for CPR
and Molecular
Diagnostics
Central Pathology ReviewK Robson, Nottingham
S Wharton, Sheffield
T Jacques, London
CCLG Feasibility Study: Strategy

PNET Clinical trials:
Future CCLG/SIOP biological studies in
Newcastle
• Refinement of favourable / average
risk medulloblastoma
• Infant medulloblastoma
• High-risk medulloblastoma
• Relapsed medulloblastoma
• sPNETs
S Clifford

Development of New Therapies
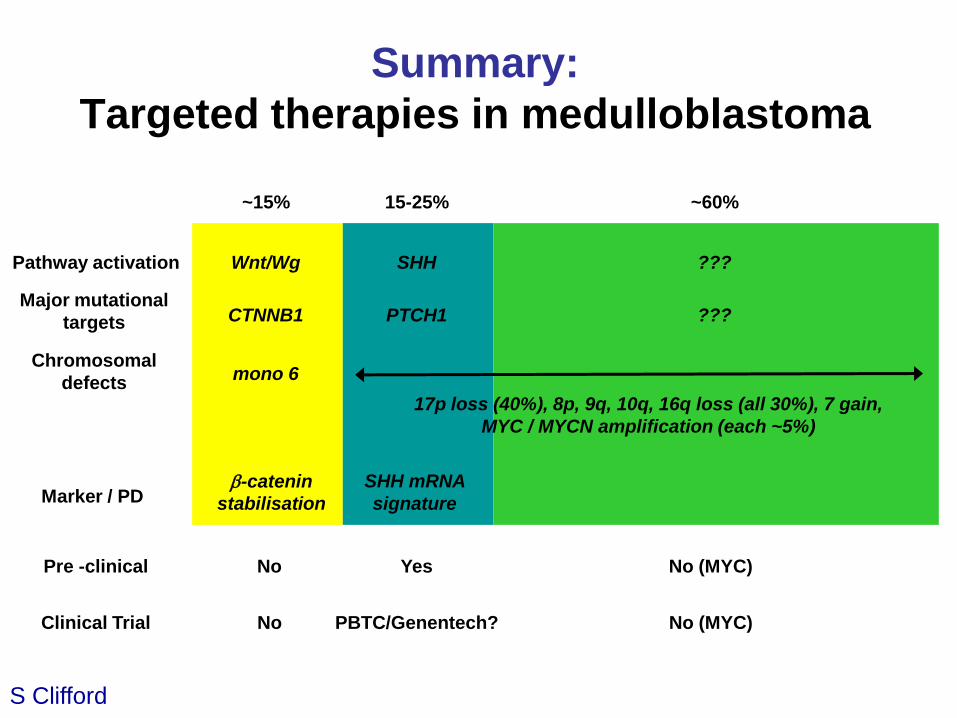
Summary:
Targeted therapies in medulloblastoma
Pathway activation Wnt/Wg SHH ???
Major mutational
targets CTNNB1 PTCH1 ???
Marker / PD
Chromosomal
defectsmono 6
15-25% ~60%~15%
b-catenin
stabilisation
SHH mRNA
signature
17p loss (40%), 8p, 9q, 10q, 16q loss (all 30%), 7 gain,
MYC / MYCN amplification (each ~5%)
S Clifford
Pre -clinical
Clinical Trial
No
No
Yes
PBTC/Genentech?
No (MYC)
No (MYC)
Cancer Cell. 6: 229-240, 2004.
• HhAntag691 (Curis/Genentech)
• Blocks SMO function (10x cyclopamine)
• Blood-brain penetration
• Assessment using PTCH (+/-) mouse MB modelS Clifford

Cancer Cell. 6: 229-240, 2004.
S Clifford

Delivery of agents targeting critical developmental
pathways to infants: potential issues
• SHH pathway activation more common in infant / desmoplastic tumours

Research Strategy
Clinical TrialsDevelopmental
Therapeutics
Exploratory Biology:
Biomarker and
Target Discovery
Translational research focused on improving
cancer therapy
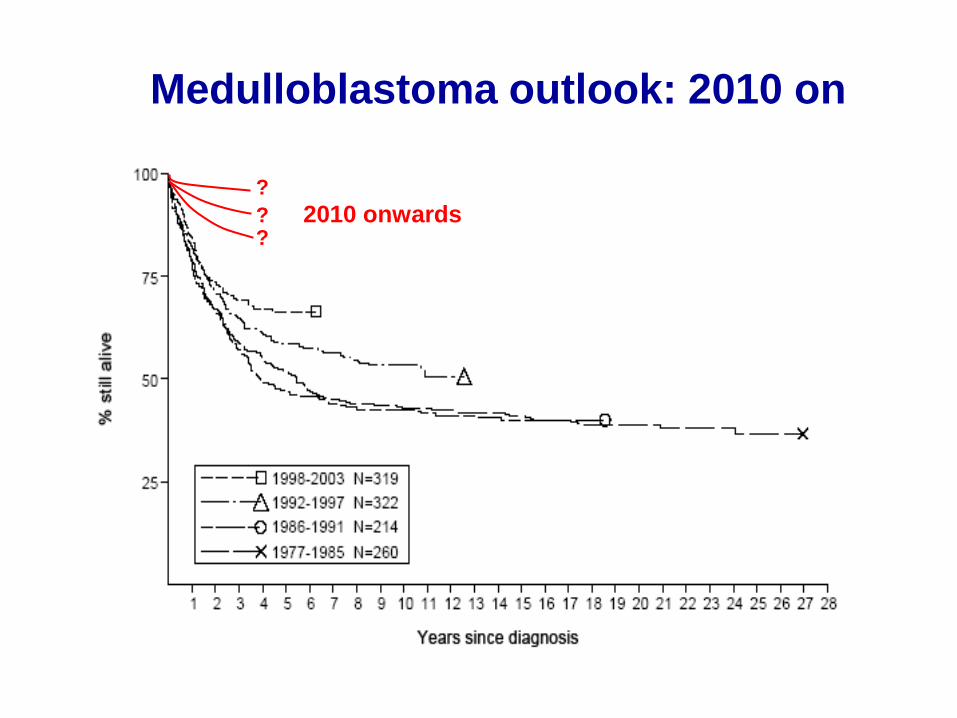
Medulloblastoma outlook: 2010 on
Data from UKCCSG annual scientific review, 2005
??
?
2010 onwards
Group leader:
Steve Clifford
Clinical lead:
Simon Bailey (NHS)
Academic Clinical Lecturer:
Britta Vormoor
Lecturer in Neuro-oncology:
TBA (Faculty / JGWP)
Post-doctoral Scientists:
Janet Lindsey (SPARKS)
Meryl Lusher (SDBTT)
Matthew Allen (EU)
Biomedical Scientists:
Sarah Leigh Nicholson (CRUK / SDBTT)
Kieran o’Toole
Clinical Fellows:
James Hayden (CLIC / NECCR)
Chris Howell (JGWP / Action Research))
Becky Hill (CRUK / JGWP)
PhD students:Hisham Megahed (Egypt Govt.)
Ed Schwalbe (KT Trust / NECCR)
Dolores Hamilton (MRC)
Newcastle Children’s Cancer Research Group
NICR Drug Development & Pharmacology Programmes
(Boddy / Curtin / Newell)
Mouse modelling (Jackson / Lastowska / Bacon)
Newcastle Clinical Neuro-oncology Team (Oncologists /
Neuro-surgeons / Neuro-pathologists / Research Nurses)
Regional genetics service (Bown)
Kids Cancer Kinome and ITCC European consortia
UK Children’s Cancer and Leukaemia Group (CCLG)
SIOP PNET group
Cancer Genome Project, Sanger Centre (Futreal)
St. Jude Children’s Research Hospital
(Ellison / Gilbertson / Roussel)
AMC Amsterdam (Kool / Versteeg)
Team, funding &
major collaborations












![The Normal patched Allele Is Expressed in Medulloblastomas ...cancerres.aacrjournals.org/content/60/8/2239.full.pdf · [CANCER RESEARCH 60, 2239–2246, April 15, 2000] The Normal](https://static.fdocuments.in/doc/165x107/5a74e6ed7f8b9a93088bf69f/the-normal-patched-allele-is-expressed-in-medulloblastomas-cancer-research.jpg)

![Homozygous f31-interferon - PNASarm [del(9p)], unbalanced translocation, or monosomy 9 is frequently observed in the malignant cells of patients with lymphoidneoplasias, including](https://static.fdocuments.in/doc/165x107/5e4cdd097e77c47fbe35a9e7/homozygous-f31-interferon-arm-del9p-unbalanced-translocation-or-monosomy.jpg)



