Child Poverty Research Day: Reducing Economic Poverty - Lucia Ferrone, 'Social Protection for SDG 1:...
20
unite for children Lucia Ferrone, UNICEF Office of Research—Innocenti On behalf of the Transfer Project November 18, 2016 GLOBAL COALITION TO END CHILD POVERTY – IDS, Brighton Social Protection for SDG 1: evidence and experiences from the Transfer Project
-
Upload
the-impact-initiative -
Category
Education
-
view
32 -
download
0
Transcript of Child Poverty Research Day: Reducing Economic Poverty - Lucia Ferrone, 'Social Protection for SDG 1:...

unite for children
Lucia Ferrone, UNICEF Office of Research—Innocenti On behalf of the Transfer Project
November 18, 2016GLOBAL COALITION TO END CHILD POVERTY – IDS, Brighton
Social Protection for SDG 1: evidence and experiences from the Transfer Project

2
Rise of social protection in Africa:Non-contributory Govt programming triples over last 15 years
Source: Cirillo & Tebaldi 2016 (Social Protection in Africa: Inventory of Non-Contributory Programmes): www.ipc-undp.org/pub/eng/Social_Protection_in_Africa.pdf

3
Typologies of programs & target groups
Source: Cirillo & Tebaldi 2016 (Social Protection in Africa: Inventory of Non-Contributory Programmes): www.ipc-undp.org/pub/eng/Social_Protection_in_Africa.pdf

4
Key feature of the African Model
• Programs tend to be unconditional (or with ‘soft’ conditions)• Targeting tends to be based on poverty & vulnerability • OVC, labor-constrained, elderly
• Important community involvement in targeting process• Payments tend to be manual, ‘pulling’ participants to pay-points• Opportunity to deliver complementary services

5
The Transfer Project
Who: Community of research, donor and implementing partners – focus on coordination in efforts and uptake of results
UNICEF, FAO, UNC, Save the Children, National GovernmentsMission: Provide rigorous evidence on of government-run large-scale (largely unconditional) social cash transfers (SCTs) Motivation:
Income poverty has highly damaging impacts on human development
Cash empowers people living in poverty to make their own decisions on how to improve their lives

6
Transfer Project Countries
Ethiopia, Ghana, Kenya, Lesotho, Malawi, Madagascar, South Africa, Tanzania, Zambia and Zimbabwe

7
Overview of programs & evaluations connected with Transfer Project
Country (program)
Targeting (in addition to poverty)
Sample size (HH)
Methodology LEWIE Youth Years of data collection
Ghana (LEAP) Elderly, disabled or OVC 1,614 Longitudinal PSM X 2010, 2012, 2016
Ghana (LEAP 1000) Pregnant women, child<2 2,500 RDD 2015, 2017
Ethiopia (SCTP) Labour-constrained 3,351 Longitudinal PSM X 2012, 2013, 2014
Kenya (CT-OVC) OVC 1,913 RCT X X 2007, 2009, 2011
Lesotho (CGP) OVC 1,486 RCT X 2011, 2013
Malawi (SCTP) Labour-constrained 3,500 RCT X X 2011, 2013, 2015
South Africa (CSG) Child <18 2,964 Longitudinal PSM X 2010, 2011
Tanzania (PSSN) Food poor 801 RCT X 2015, 2017
Zambia (CGP) Child 0-5 2,519 RCT X 2010, 2012, 2013, 2014
Zambia (MCTG) Female, elderly, disabled, OVC 3,078 RCT X 2011, 2013, 2014
Zimbabwe (HSCT) Food poor, labour- constrained 3,063
Longitudinal matched case-
controlX X 2013, 2014, 2017

8
Unique demographic structure of recipient households: Missing prime-ages
Malawi SCT Zimbabwe HSCT
0.0
1.0
2.0
3.0
4D
ensi
ty
0 20 40 60 80Age (years)
Zambia SCT (Monze)
0.0
1.0
2.0
3.0
4D
ensi
ty
0 20 40 60 80
Age (years)
0.0
1.0
2.0
3.0
4D
ensi
ty
0 20 40 60 80 100Age (years)
0.0
2.0
4.0
6D
ensi
ty
0 20 40 60 80 100Age (years)
Kenya CT-OVC
Zimbabwe HCSTMalawi SCTP

9
ProgramFemale
beneficiaries
(%)
Female-headed
households (%)
Ghana LEAP 44 60
Ghana LEAP 1000 100 11
Kenya CT-OVC 85 85
Malawi SCTP 84 84
Zambia CGP 99 -
Zambia MCTG 75 -
Zimbabwe HSCT 68 68
And three of five beneficiary HH are female-headed
Approximately two-thirds of beneficiaries are female
Figures for female-headed households may reflect evaluation sample, rather than beneficiary sample. Zambia studies did not collect information on headship.
Who gets the cash?

10
How can cash transfers impact child poverty?
Direct impact on monetary poverty:
• Immediate increase in consumption
• Long term effects: household economic strengthening, resiliency and financial wellbeing; productive impacts.
Indirect impact on different dimensions of poverty:
• Education
• Food security/Nutrition
• Health outcomes
Impact on MD poverty

11
Reductions on poverty measures
Ethiopia (24 months)
Kenya (24 months)
Lesotho (24 months)
Malawi (36months)
Zambia MCTG
(36 months)
Zambia CGP (48 months)
Zimbabwe (12 months)
Increase in household
income (%)
Reduction in poverty head count (pp)
Reduction in poverty gap (pp)
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
10 10
1.4
1211
10
0
Solid bars represent significant impact, shaded insignificant.Impacts are measured in percentage points, unless otherwise specified

12
Across-the-board impacts on food securityEthiopia
SCTPGhana LEAP
Kenya CT-
OVC
Lesotho CGP
Malawi SCTP
Zambia MCTG
Zambia CGP
Zim HSCT
Spending on food & quantities consumed
Per capita food expenditures ü ü ü ü ü ü ü ü Per capita expenditure, food items ü ü ü ü ü ü Kilocalories per capita ü üFrequency & diversity of food consumption Number of meals per day ü ü ü Dietary diversity/Nutrient rich food ü ü ü ü ü üFood consumption behaviours Coping strategies adults/children ü ü ü ü Food insecurity access scale ü ü ü
Green check marks represent significant impact, black are insignificant and empty is indicator not collected

13
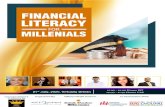
School enrollment impacts (secondary age children): Comparable to those from CCTs in LAC
02468
101214161820
8
3
78
15
89
12
6
9
6
10
Primary enrollment already high, impacts at secondary level. Ethiopia is all children age 6-16.Bars represent percentage point impacts; all impact are significant.

14
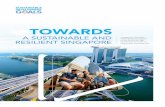
Significant impacts on spending on school-age children(uniforms, children’s shoes and clothing)
Ghana
(LEAP)
Leso
tho (C
GP)
Malawi (S
CTP)
Zambia
(MCTG)
Zambia
(CGP)
Zim (H
SCT) small
hh
Zim (H
SCT) large
hh05
101520253035
11
2630
23
32
11
5

15
Young child health and morbidityRegular impacts on morbidity, but less consistency on care seeking
Ghana LEAP
Kenya CT-OVC
Lesotho CGP
Malawi SCTP
Zambia CGP
Zimbabwe HSCT
Proportion of children who suffered from an illness/Frequency of illnesses ü ü ü ü ü üPreventive care ü ü üCurative care ü ü ü üEnrollment into the National Health Insurance Scheme üVitamin A supplementation ü
Supply of services typically much lower than for education sector.More consistent impacts on health expenditure (increases)

16
Role of supply side:
Example 1: Skilled attendance at birth improved in Zambia CGP, only among women with access to quality maternal health services
Example 2: Anthropometry in Zambia CGP improved among households with access to safe water source
Example 3: Impacts on schooling enrollment in Kenya CT-OVC are largest among households which face higher out of pocket costs (uniform/shoes requirement, greater distance to school) [program offsets supply side barrier]

17
Conclusion and way forward
UCTs can effectively reduce child poverty in different dimensions: monetary and MD poverty alike
Proven effective social protection tool in many domains Many myths about UCTs disproven by evidence But: they need investment on the supply side to complement the
impact in critical domains such as health, sanitation & water, etc What we need to know more: Impact on child MD poverty (we are working on it!) Impacts in different settings: universality of SDGs. Can the model be
exported? Social Protection in emergency settings
What’s the impact of combined interventions?

18
For more information• Transfer Project website: www.cpc.unc.edu/projects/transfer • Briefs: http://www.cpc.unc.edu/projects/transfer/publications/briefs
• Facebook: https://www.facebook.com/TransferProject • Twitter: @TransferProjct
Ghana, credit: Ivan Griffi

19
Acknowledgements Transfer Project is a multi-organizational initiative of the United Nations Children’s Fund (UNICEF) the UN Food and Agricultural Organization (FAO), Save the Children-United Kingdom (SC-UK), and the University of North Carolina at Chapel Hill (UNC-CH) in collaboration with national governments, and other national and international researchers.
Current core funding for the Transfer Project comes from the Swedish International Development Cooperation Agency (Sida), as well as from staff time provided by UNICEF, FAO, SC-UK and UNC-CH. Evaluation design, implementations and analysis are all funded in country by government and development partners. Top-up funds for extra survey rounds have been provided by: 3IE - International Initiative for Impact Evaluation (Ghana, Malawi, Zimbabwe); DFID - UK Department of International Development (Ghana, Lesotho, Ethiopia, Malawi, Kenya, Zambia, Zimbabwe); EU - European Union (Lesotho, Malawi, Zimbabwe); Irish Aid (Malawi, Zambia); KfW Development Bank (Malawi); NIH - The United States National Institute of Health (Kenya); Sida (Zimbabwe); and the SDC - Swiss Development Cooperation (Zimbabwe); USAID – United States Agency for International Development (Ghana, Malawi); US Department of Labor (Malawi, Zambia). The body of research here has benefited from the intellectual input of a large number of individuals. For full research teams by country, see: https://transfer.cpc.unc.edu/

20
Additional slides: General approach to modeling
• Probit or ordinary least squares (OLS) multivariate regressions
• Baseline balance/ successful randomization in all countries• For “once occurring outcomes” use endline cross section and
drop those who had already reported outcome at baseline• For outcomes changing over time (mental health, education,
aspirations), use difference-in-difference models• Control for baseline individual, household, community
characteristics & cluster standard errors• Weight for probability of appearing in sample (among all
eligible youth in any given household)