
CHF
37
CONGESTIVE HEART FAILURE CONGESTIVE HEART FAILURE (CHF) NYHA IV e.c Coronary (CHF) NYHA IV e.c Coronary Artery Disease (OMI Artery Disease (OMI Anteroseptal) Anteroseptal) Supervisor : Prof. dr. Peter Kabo, Ph.D, Sp.FK, Sp.JP(K) By : Muhammad Adhim Alwi C111 08 166
-
Upload
khairiyyah-suriatmajaya -
Category
Documents
-
view
6 -
download
0
description
chf cardiology
Transcript of CHF

CONGESTIVE HEART FAILURE CONGESTIVE HEART FAILURE
(CHF) NYHA IV e.c Coronary (CHF) NYHA IV e.c Coronary
Artery Disease (OMI Artery Disease (OMI
Anteroseptal) Anteroseptal)
Supervisor :
Prof. dr. Peter Kabo, Ph.D, Sp.FK, Sp.JP(K)
By :Muhammad Adhim AlwiC111 08 166

Patient Identity
• Name : Mr. S• Gender : Male• Age : 60 years old• Medical Record : 362481• Date of Admission : 11 January 2015• Address : Jln. Flamboyan, MKS
Anamnesis • Chief Complaint : Shortness of breath• Shortness of breath has been experienced since 2 years ago and worsened 1 week ago. It was experienced even the patient is at rest and relieved with ist own. The patient also complains chest pain which has been experienced since 7 years ago. Chest pain was felt on the left side of the chest with the characteristics of heavy feeling on the chest, duration of pain was < 5 minutes, did not radiate to the left arm and to the back.

Anamnesis
The pain exacerbates with exercise and lessen with rest. Dyspnea on effort (+), Orthopnea (-), Paroxysmal Nocturnal Dyspnea (+), Cough (+) intermittent since 1 year ago. Palpitation (+), Fever (-) Nausea (-) Vomit (-). Defecation and urination: normal.

Past Medical History• There is history of being admitted to the hospital 7 years ago with a diagnosis CAD and do installation balloons and rings .
• There is history of hypertension since 7 years ago but he doesn’t take the drugs regularly.
• There is history of smoking since 35 years ago but stopped 7 years ago.1 box per day.
• There is no history of fever, congenital heart disease, thyroid disease, and diabetes mellitus.
• There is also no family history with cardiovascular disease.

Risk Factors

Physical Examination
General Status:• Moderate illness/ Well nourished/ Conscious• Nutritional Status: Normal (BMI: kg/m²)
Weight : 55 kg BMI: 20.2 kg/m2
Height : 165 cm
Vital Signs:• Blood Pressure : 130/60 mmHg• Pulse Rate : 80 bpm• Respiratory Rate : 25 bpm• Temperature : 36.7 0C

Head and Neck Examinations:• Eye : Conjunctiva anemic (-/-), sclera icteric (-/-)• Lip : cyanosis (-)• Neck : No mass, no tenderness, JVP : R + 3 cmH2O
Chest Examination• Inspection : Symmetric left=right • Palpation : No mass, no tenderness, vocal fremitus
left=right• Percussion : Sonor left = right, lung-liver border in ICS VI
right anterior• Auscultation: Breath sound : vesicular Additional sound : Ronchi - -
Wheezing -/- - - + +
Physical Examination

Cardiac Examination•Inspection : Ictus cordis was not visible•Palpation : Ictus cordis was not palpable•Percussion :Right heart border in right parasternal line, left heart border two fingers from left midclavicular line ICS VI.•Auscultation : Heart sound : S I/II regular, no gallop, no additional sound
Physical Examination

Abdominal Examination• Inspection : flat, following breath movement• Auscultation : Peristaltic sound (+), normal• Palpation : No mass, no tenderness, no
palpable liver and spleen• Percussion : Tympani (+), ascites (-)
Extremities Examination• Pretibial edema -/-• Dorsum pedis edema -/-
Physical Examination

Electrocardiography(ECG)Electrocardiography(ECG)

Interpretation of ECG• Rhythm : Atrial fibrillation• HR / QRS rate : 80 bpm• Axis : Normoaxis • Regularity : Irregular• P wave : Difficult to assess• PR interval : Difficult to assess• QRS complex : 0.08 s (N: 0.06-0.11 s)• Q pathologies : V1, V2, V3• ST segment : Difficult to assess• T wave : Difficult to assess
Conclusion : Atrial Fibrillation Normal Ventricular Response, OMI anteroseptal

EchocardiographyEchocardiography

Conclution of Echocardiography• Systolic and diastolic dysfunction of the left ventricle• Ejection fraction 33%• Left ventricular hypertrophy• Trivial Mitral regurgitation• Thrombus in the left ventricle with a diameter 2.8 x 3.6
cm• Akinetik basal anteroseptal, mid anteroseptal and
anterior, apical anteroseptal, anterior, the other segments hipokinetik

Chest X-rays
Conclusion :•Normal Pulmonary•Cardiomegaly with dilatation aortae

Laboratory Finding
Test Result Normal value
WBC 11.1/ul 4.0 – 10.0 x 103
RBC 5.61/µl 4.0 – 6.0 x 106
HGB 16.7 gr/dl 14 – 18
HCT 49.1% 40 – 54
PLT 290 000/µl 150 – 400 x 103
Complete Blood Count
Electrolyte
Test Result Normal value
Na 146 mmol/l 136-145
K 4.5 mmol/l 3.5-5.1
Cl 113 mmol/l 97-111

Laboratory Finding
Test Result Normal value
GDS 98 mg/dl98 mg/dl <140
Ureum 22 mg/dl 10 – 50
Creatinine 1.5 mgr/dl < 1.3
SGOT 28 u/l <38
SGPT 34 u/l <41
Blood Chemistry
Cardiac Enzymes
Test Result Normal value
CK 77.7 U/L <167
CK-MB 15.4 U/L <25
Troponin-T <0.02 <0.05

Diagnosis
• CHF NYHA IV e.c CAD (OMI Anteroseptal)
• Atrial Fibrillation Normal Ventricular Response (AF NVR)

Management
• O2 2-4 lpm via nasal canul
• IVFD NaCl 0.9% 10 dpm• Fluid Balance• Inj. Furosemide 40 mg/12 hours/ IV• Fasorbid 10 mg 1-1-1 • Aspilet 80 mg 0-1-0 • Captopril 6,25 mg 1-1-1• Simvastatin 1 x 20mg • Digoxin 0.125 mg 1-0-0

Planning
• ECG control

DISCUSSION
Congestive Heart Congestive Heart Failure (CHF)Failure (CHF)

DEFINITION

Other Causes
Arrhythmias Valvular heart diseaseCongenital heart diseasePericardial diseaseHyperdynamic circulationAlcohol and drugs(chemotherapy)
Main Causes
Ischemic heart disease (35%-40%)Cardiomyopathy(dilated) (30-40%)Hypertension ( 15-20%)
Etiology of Heart Failure

Major Criteria Minor Criteria
Paroxysmal Nocturnal Dyspnea
Cardiomegaly
Gallop S3
Hepatojugular reflux
Increased of JVP
Rales or ronchi
Acute pulmonary edema
Extremity edema
Nocturnal cough
Decreased vital pulmonary
capacity (1/3 of maximal)
Hepatomegaly
Pleural effusion
Tachycardia (≥ 120bpm)
Dyspnea d’effort

Classification of CHF
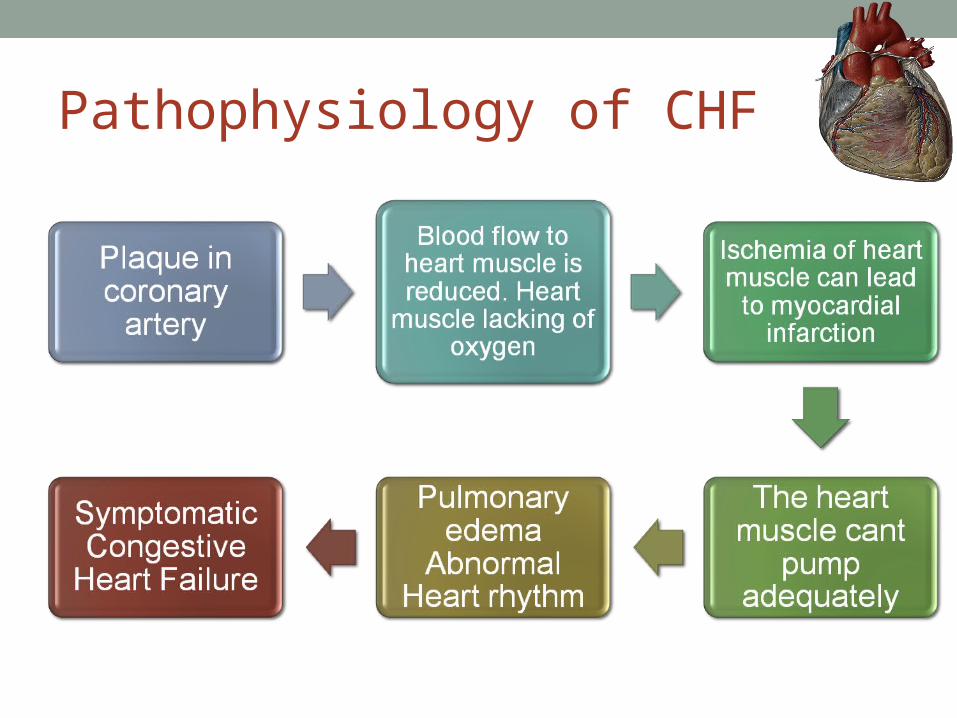
Pathophysiology of CHF

Treatment of CHF

Coronary Artery Disease
• Coronary artery disease is a narrowing of the small blood vessels that supply blood and oxygen to the heart.
• (CAD) occurs when the arteries that supply blood to the heart muscle (the coronary arteries) become hardened and narrowed due to buildup of a material called plaque (plaque) on their inner walls. This is known as atherosclerosis
• Eventually, blood flow to the heart muscle is reduced, and, because blood carries much-needed oxygen, the heart muscle is not able to receive the amount of oxygen it needs.

Causes CAD
• Coronary artery disease (CAD) is caused by atherosclerosis (the thickening and hardening of the inside walls of arteries). Some hardening of the arteries occurs normally as a person grows older.
• In atherosclerosis, plaque deposits build up in the arteries. Plaque is made up of fat, cholesterol, calcium, and other substances from the blood. Plaque buildup in the arteries often begins in childhood.


Plaque in the arteries can be:• Hard and stable. Hard plaque causes the artery walls to thicken and harden. This condition is associated more with angina than with a heart attack, but heart attacks frequently occur with hard plaque.
• Soft and unstable. Soft plaque is more likely to break open or to break off from the artery walls and cause blood clots. This can lead to a heart attack.

RISK FACTORS

INVESTIGATION• Electrocardiogram (ECG)• Treadmill Test• Echocardiography• Coronary Angiography• Multi-Slice Computed Tomography Scan (MSCT)• Cardiac Magnetic Resonance Imaging (Cardiac MRI)
• Radionuclear Medicine

TREATMENT
Lifestyle Changes• Eat a healthy diet • Quit smoking, if you smoke
• Exercise • Lose weight, if you are overweight or obese
• Reduce stress
Medicines• Cholesterol-lowering medicines
• Anticoagulants• Aspirin• ACE inhibitors• Beta blockers• Calcium channel blockers
• Nitroglycerin• Long-acting nitrates

TREATMENT
Special Procedures• Angioplasty (PTCA)• Coronary artery bypass surgery• Enhanced External Counterpulsation (EECP)
Cardiac Rehabilitation• Exercise training• Education, counseling, and training

THANKYOU


















