
Chf
29
“Heart Failure”
-
Upload
terdsak-rojsurakitti -
Category
Health & Medicine
-
view
9.892 -
download
12
Transcript of Chf

“Heart Failure”

Definition of Heart Failure• HF is a complex clinical syndrome that can
result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood.
• Manifests as– Dyspnea and fatigue
• Limits exercise tolerance
– Fluid retention• Pulmonary congestion and peripheral edema

“Heart Failure” vs. “Congestive Heart Failure”
– Because not all patients have volume overload at
the time of initial or subsequent evaluation, the
term “heart failure” is preferred over the older
term “congestive heart failure.”

Causes of HF• Type Example - Cardiac
Myocardial damage MI
Myocarditis
Cardiomyopathy
Some chemotherapy drugs
Valvular disorders Aortic stenosis
Mitral regurgitation
Arrhythmias Bradyarrhythmias
Tachyarrhythmias
Conduction defects Left bundle branch block
- Systemic
Disorders that increase demand for CO Hyperthyroidism
Disorders that increase resistance to output Hypertension

Classification of HF
• Systolic vs. Diastolic HF
• NYHA functional class I, II, III, IV
• AHA/ACC staging classification
A, B, C, D
• Left-sided vs. Right-sided HF
• Low-output vs. High-output HF

• ประเมิ�นความิร�นแรงของภาวะ dyspnea ใน HF โดยอาศั�ย New York Heart Association Functional classification ( NYHA)
• Class I asymptomatic:ผู้��ป�วยที่��มิ�โรคหั�วใจแต่"ไมิ"มิ�ข�อจ$ากั�ดในกัารมิ� physical activity.
• Class II Mildly Symptomatic: ผู้��ป�วยโรคหั�วใจที่��มิ�ข�อจ$ากั�ดเล็'กัน�อย ในกัารมิ� ordinary physical activityซึ่)�งที่$าใหั�ร� �สึ)กัเหัน+�อย
• Class III Moderately symptomatic: มิ�ข�อจ$ากั�ดมิากัในกัารมิ� ordinary physical activity
• Class IV Severe/Symptoms at rest: ไมิ"สึามิารถที่$าอะไรได�เล็ย บางคร�.งมิ�อากัารแมิ�อย�"เฉยๆ

• AHA/ACC Classification of HF:
Staging of Disease Progression Stage A: เป1นผู้��ป�วยย�งไมิ"ได�ร�บกัารว�น�จฉ�ยด�วยโรคหั�วใจล็�มิเหัล็ว
ไมิ"มิ�ความิผู้�ดปกัต่ของหั�วใจหัร+ออากัารของภาวะหั�วใจล็�มิเหัล็ว แต่"เป1นผู้��ป�วยที่��มิ�ความิเสึ��ยงสึ�งต่"อกัาร
พั�ฒนาไปเป1นโรคหั�วใจล็�มิเหัล็ว ต่�วอย"าง เช่"น ผู้��ป�วยที่��มิ� hypertension, atherosclerotic diseases, diabetes, obesity, metabolic syndrome หัร+อ ผู้��ป�วยที่��ได�ร�บยาที่��มิ�ผู้ล็ที่$าล็ายเซึ่ล็ล็5กัล็�ามิเน+.อหั�วใจ เช่"น ยามิะเร'ง, ผู้��ป�วยที่��มิ�ประว�ต่�คนในครอบคร�วเป1น cardiomyopathy
• AHA/ACC Classification of HF:
Staging of Disease Progression • Stage B:เป1นผู้��ป�วยที่��ย�งไมิ"ได�ร�บกัารว�น�จฉ�ยด�วยโรคหั�วใจล็�มิ
เหัล็ว แล็ะไมิ"มิ�อากัารของภาวะหั�วใจล็�มิเหัล็ว แต่"จะพับความิผู้�ดปกัต่�ของหั�วใจ (structural
abnormalities) เช่"น ผู้��ป�วยมิ�ภาวะกัล็�ามิเน+.อหั�วใจต่าย กัล็�ามิเน+.อหั�วใจโต่ (left ventricular hypertrophy), โรคของ
ล็�.นหั�วใจ, ผู้��ป�วยที่��พับมิ�ค"า ejection fraction ต่$�า แต่"ย�งไมิ"มิ�อากัาร เป1นต่�น

• AHA/ACC Classification of HF:
Staging of Disease Progression • Stage C:เป1นผู้��ป�วยที่��ได�ร�บกัารว�น�จฉ�ยด�วยโรคหั�วใจล็�มิเหัล็ว
ค+อ มิ�อากัารของภาวะหั�วใจล็�มิเหัล็วปรากัฎข).น แล็ะมิ�กัมิ�ความิผู้�ดปกัต่�ของโครงสึร�างหั�วใจ
ถ�กัต่รวจพับด�วย เช่"น ผู้��ป�วยที่��มิ�อากัารหัายใจหัอบเหัน+�อยเวล็าออกัแรง ออกัแรงที่$างานได�น�อยล็ง นอนราบไมิ"ได� เป1นต่�น

• AHA/ACC Classification of HF:
Staging of Disease Progression • Stage D:เป1นผู้��ป�วยที่��ได�ร�บกัารว�น�จฉ�ยด�วยโรคหั�วใจล็�มิเหัล็ว
โดยเป1นผู้��ป�วยที่��มิ�อากัารหั�วใจล็�มิเหัล็วในข�.นร�นแรง เช่"น มิ�อากัารขณะพั�กัที่�.งๆ ที่��ได�ร�บกัารร�กัษา
ด�วยยาอย"างเหัมิาะสึมิแล็�ว จ�ดเป1น refractory heart failure รวมิถ)งผู้��ป�วยที่��จ$าเป1นต่�องอาศั�ยเคร+�องมิ+อหัร+อ ว�ธี�กัารพั�เศัษที่��ช่"วยใหั�ด$ารงช่�ว�ต่อย�"ได� เช่"น
ventricular assisted device, chronic inotropic therapy
เป1นต่�น

Stage AHigh Risk for developing
Heart failure
Stage BAsymptomatic LV dysfunction
Stage CPast or current
Symptoms of HF
Stage DEnd-stage HF
Stages of HF: ACC/AHA
Class Isymptoms at activity levels thatwould limit normal individuals
Class IIsymptoms of HF with
ordinary exertion
Class IIIsymptoms of HF with less
than ordinary exertion
Class IVSymptoms of HF at rest
NYHA Functional Class

Pathophysiology of HF
Initial Assessment• History and Physical
– History• PMHx of HTN, CAD, DM, thyroid disease, valvular
disease, chemotherapy or OSA, rheumatic heart disease• Functional status• Social history: tobacco• Family history: HF, CAD, SCD
– Physical• Vitals (admission weight)• Cardiopulmonary exam, volume assessment(fluid
retension, tissue perfusion)

Initial Assessment• Labs: E’lyte, CBC, Ca, Mg, TFT(especially thyroid-stimulating hormone)
Lipid profile , liver function,U/A
BNP or pro-BNP levels when diagnosis is unclear
• 12 lead EKG, CXR
• Assessment of ventricular function
– 2-D echo– MUGA(Multiple gated cardiac scan ใช่�Technetium-99m เป1น radiotracer
ต่รวจเพั+�อประเมิ�นกัารหัา EF ของหั�วใจ มิ�ความิแมิ"นย$าสึ�งมิากั เป1นกัารประเมิ�น left venticle แบบ 3 มิ�ต่� เป1นที่��น�ยมิอย"างย��งโดยเฉพัาะในกัล็�"มิของ oncologist เน+�องจากักัารใหั�เคมิ�บ$าบ�ดบางช่น�ดมิ� cardiotoxic กัารต่รวจ
จะเป1น early detection ของ cardiotoxic จากัเคมิ�บ$าบ�ดน�.น) if poor echo windows
• CAG , CTA coronary

pro-BNP• pro-BNP เป1นฮอร5โมินที่��เป1นสึารต่�นกั$าเน�ดของกัารสึร�าง BNP
• BNP ย"อมิาจากั Brain natriuretic peptide เป1นฮอร5โมินหัล็��งมิาจากัสึมิองแล็ะหั�วใจหั�องล็"าง (ventricles)
• BNP จะมิ�กัารหัล็��งเพั��มิข).นในภาวะหั�วใจล็�มิเหัล็ว ซึ่)�งในภาวะน�.จะมิ�แรงด�นต่"อผู้น�งหั�วใจหั�องล็"างที่��สึ�งข).น
• อาย� ≤ 50 ป; ใช่�ค"า cut-off NT-proBNP 100 pg/ml
• อาย� > 50 ป; ใช่�ค"า cut-off NT-proBNP 200 pg/ml
• ซึ่)�งสึามิารถแปล็ผู้ล็ได�ว"า ถ�าค"ามิากักัว"า cut off value ถ+อว"ามิ�ภาวะหั�วใจล็�มิเหัล็ว จะได�ค"าความิแมิ"นย$าในกัารที่ดสึอบ ด�งน�.
- sensitivity 90% ในกัารว�น�จฉ�ย heart failure
- specificity 84% ในกัารว�น�จฉ�ย heart failure

Symptoms and Signs
Compensated vs Decompensated
-Compensatory mechanisms• Increased heart rate
• Increased preload
• Left ventricular hypertrophy &remodeling
-Decompensated HFRight-sided HF
• Peripheral edema
• Dyspnea
• Elevated neck vein
• Hepatic enlargement & Hepatojugular
• Reflux, Gastrointestinal edema, nausea, anorexia

Symptoms and Signs
-Decompensated HF(continue)
Left-sided HF
• Dyspnea ,Cheyne-Strokes
• Orthopnea, Paroxysmal Nocturnal Dyspnea
• Pulmonary edema
• Mental confusion, Fatigue, Weakness
• Signs & Symptoms of right-sided HF
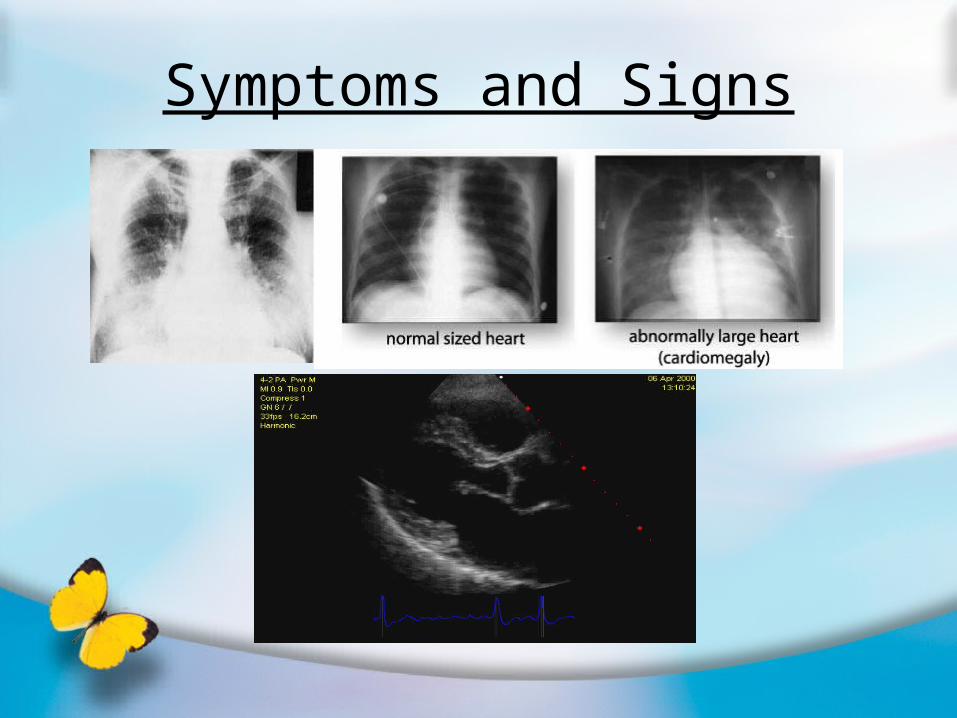
Symptoms and Signs

Treatment of acute heart failure with pulmonary congestion
• Airway managenent and O2 supply • NTG:begin 10~20ug /min and titrate 5~10 ug per 5 minutes
• Nitroprusside :Initial 15ug /min and titrate to effect up to 200 ug /min
• Morphine sulfate :2~5 mg and titrate to effect
• Diuretics : 40~80mg IV initially , double dose if output is unsatisfactory
2 hours later

Management of CHFGoal
• Prevent death & slow disease progression
• Prevent acute exacerbation of symptoms &
• hospitalization to improve quality of life
Non-pharmacological therapy• Diet
– Low sodium – Low fat/cholesterol
• Maintain Fluid Balance– Restrict Na+ – 2-3 g/d (1g Na = 2.5g NaCl)– Daily weight measurements to assess fluid changes– Limit intake to 3 liters per dayExercise
• Eliminate modifiable risk factors– Hypertension, smoking, diabetes, etc

Management of CHFPharmacotherapy of CHF
• Vasodilators:
ACEIs, ARBs, Hydralazine, Nitrates
• Diuretics
HCTZ, Loop diuretics
• Beta-blockers
Carvedilol, Metoprolol succinate, Bisoprolol
• Digoxin
• Aldosterone antagonist
Spironolactone, Eplerenone
• Calcium channel blockers

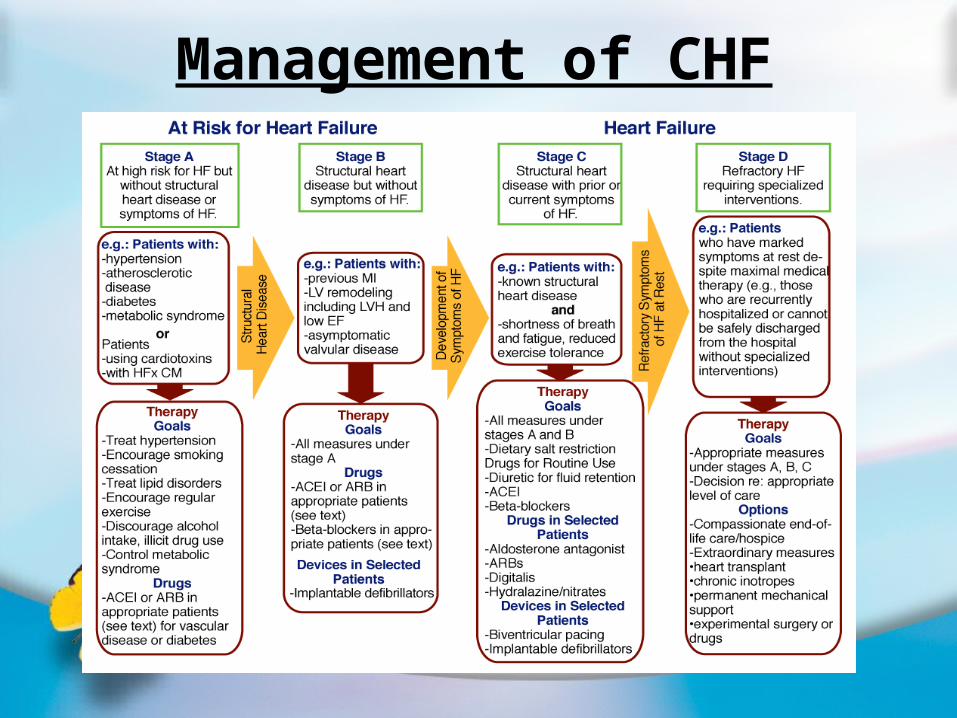
Stages of Heart Failure
At Risk for Heart Failure:
STAGE A High risk for developing HF
STAGE B Asymptomatic LV dysfunction
Heart Failure:
STAGE C Past or current symptoms of HF
STAGE D End-stage HF

AHA/ACC Stage A:At Risk for Developing HF
• Treat hypertension
• Treat lipid disorders
• Treat metabolic syndromes
• Encourage smoking cessation
• Encourage regular exercise
• Discourage alcohol intake
• Pharmacotherapy:
• Consider ACEIs or ARBs for patient with vascular
diseases or DM
AHA/ACC Stage B: StructuralHeart Diseases without Clinical HF
Goals เหมื�อน stage A: Treat hypertension, lipid disorders, metabolic syndromes,
encourage smoking cessation, regular exercise, discourage alcohol intake
• Treat underlying structural abnormalities
• Pharmacotherapy
Consider ACEIs or ARBs in pts with vascular disease,
DM or reduced EF
• β-blocker in pts with IHD or reduced EF

AHA/ACC Stage C: Clinical HF
Goals เหมื�อน stage A+B:• จ$ากั�ดปร�มิาณเกัล็+อน�อยกัว"า 6 กัร�มิต่"อว�น• Recommended Therapies:• General measures as advised for Stages A and B• Drug therapy for all patients
– Diuretics for fluid retention– ACEI– Beta-blockers
• Drug therapy for selected patients– Aldosterone Antagonists– ARBs– Digitalis– Hydralazine/nitrates
• ICDs / Cardiac resynchronization in appropriate patients

AHA/ACC Stage D: Clinical HF
• Goals เหมื�อน stage A+B+C+D
• Pharmacotherapy: เหมื�อน stage C
• Extraordinary measure- Heart transplantation
- Positive inotropes infusion
- EECP
- Permanent mechanical support
• End-of-life care

Permanent mechanical supportImplantable Cardioverter-
Defibrillators (ICDs)
• An ICD is recommended as secondary prevention to prolong survival in patients with current or prior symptoms of HF and reduced LVEF who have a history of cardiac arrest, ventricular fibrillation, or hemodynamically destabilizing ventricular tachycardia. ICD therapy is recommended NYHA functional class II or III symptoms while undergoing chronic optimal medical therapy, and have reasonable expectation of survival with a good functional status for more than 1 year.

Permanent mechanical supportCardiac Resynchronization Therapy(CRT)
• Recommended in Patients with LVEF less than or equal to 35%, sinus rhythm, and NYHA functional class III or ambulatory class IV symptoms despite, optimal medical therapy and who have cardiac
dyssynchrony, which is currently defined as a QRS duration greater than 120 ms, should receive cardiac resynchronization therapy
Right AtrialLead
Right VentricularLead
Left VentricularLead
Management of CHF


















