
Chet Rhoads The HDH Group November 19, 2014. 83% of firms with 25-49 employees offer health...
28
Short and Long Term Strategies for Controlling Health Insurance Costs Chet Rhoads The HDH Group November 19, 2014
-
Upload
margaretmargaret-arline-wilson -
Category
Documents
-
view
218 -
download
0
Transcript of Chet Rhoads The HDH Group November 19, 2014. 83% of firms with 25-49 employees offer health...

Short and Long Term Strategies for Controlling Health Insurance
Costs
Chet Rhoads
The HDH Group
November 19, 2014

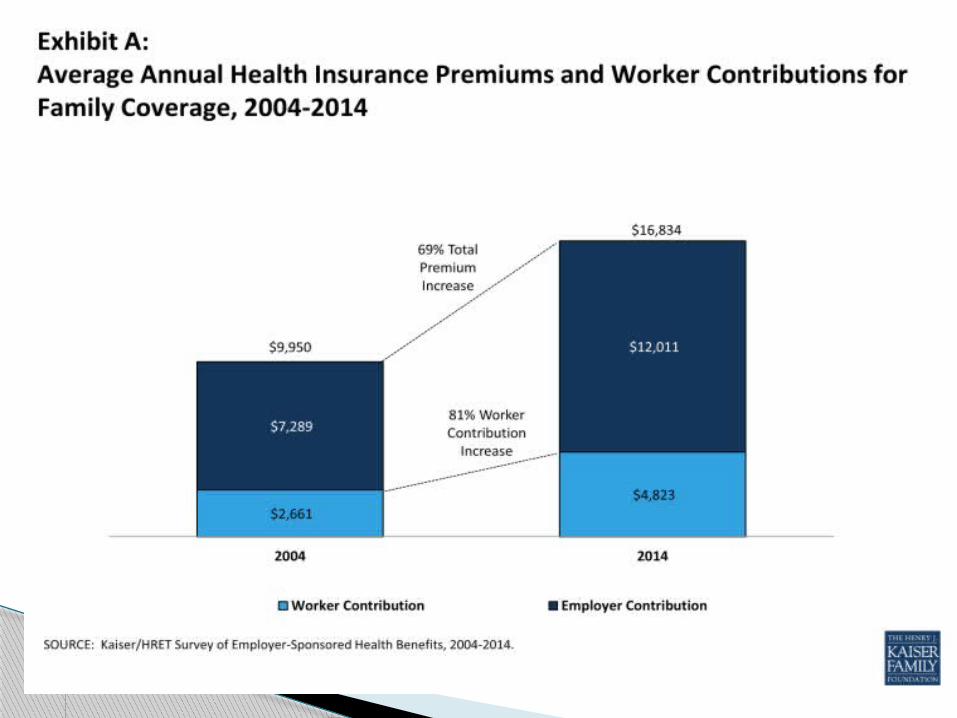
83% of firms with 25-49 employees offer health insurance
91% of firms with 50-199 employees offer health insurance
98% of firms with 200-999 employees offer health insurance
100% of firms with 1,000 employees or more offer health insurance
Percentage of Firms Offering Health Benefits


Most important Asset comes with a price Best talent in Labor Pool
◦ Innovation◦ Competitive Advantage◦ Compete with Global Markets◦ Relationship Pipeline
Competitive Wages are Comprised by unsustainable healthcare costs◦ Competitors that can control healthcare cost will
have the advantage of attaining/retaining best talent
Human Capital


Will not sustain healthcare costs over time
Typically transfers more of the burden on employee
Carriers and legislation can impose limits
Engagement of employee workforce limited
Short Term Strategies

Higher deductibles, versus higher employee contributions
Implement coinsurance for in-network services Higher ER co-pays Health Reimbursement Account (HRA)/Health
Savings Account (HSA) Spousal Mandate/Surcharge (Working Spouse
Provision) Prescription Drug Programs
◦ Mandatory Generic ◦ Mail Order◦ Formulary
What are the Short Term Strategies?

Sustain healthcare costs over time Encourage employees/dependents to make
better healthcare decisions Encourage employees/dependents to
conduct better behavioral lifestyles More latitude with carriers and legislation Over time, a culture is created for invested
and engaged workforce
Long Term Strategies

Alternative Funding Arrangements◦ Self-Funding – Cost Plus, Administrative Services
Only (ASO)◦ Captive
Prescription Drug Carve-Outs Defined Contribution/Private Exchange
Model Wellness Data Integrity
What are the Long Term Strategies?

Remit monthly premium to insurance carrier
Carrier in turn will pay:◦ Claims◦ Administration◦ Reinsurance
Fully-Insured

◦ Pros Predictable budget Less volatile compared to self-funding Carrier pays PPACA fees on client’s behalf Client not responsible for run-out claims
◦ Cons Carrier uses past claims experience to determine future rates Premium payments do not reflect real-time claims changes Carrier sets the pooling level ($125K) Administration built into the rates is higher than a self-funded
arrangement 2-3% annual fee on health insurance providers only applies
to fully-insured plans (2014) Premium taxes
Fully-Insured: Pros & Cons

A trade off of short term stability for long term cost savings
Assume more risk/opportunity for more reward Pay carrier a monthly or weekly administrative fee for
claims adjudication, billing, eligibility, customer service, etc…
Purchase Stop Loss Insurance◦ Specific: Protects client when claims incurred during policy
year on any one member exceed specific liability◦ Aggregate: Protects client when claims incurred during
policy period exceed a certain corridor above expected claims
Pay actual claims less stop loss reimbursements monthly Reserves – Held by Carrier or Client Settlement – Annually if carrier hold reserves
Self-Funding

◦ Pros Good years; ABC Company experiences immediate savings ABC Company chooses the amount of risk to retain via the specific
deductible Carrier does not profit as a result of good claims ABC Company holds onto excess reserves instead of paying them to a
carrier Avoid 2-3% fee on health insurance providers (2014) and premium taxes Administration of the plan less expensive Carrier renewal rates irrelevant (used for COBRA and budgeting)
◦ Cons Bad years; possibility of spending more than fully-insured rates More volatile compared to fully-insured (volatility a function of stop loss
specific deductible) Client responsible for run-out claims in the event of a carrier
change/termination of plan/layoffs Carriers do not remit PPACA fees on client’s behalf – Employer pays fees
annually based on members
Self-Funding: Pros & Cons

Captive◦ A member-owned insurance company◦ Initial captive structures were created for the
Fortune 500 (e.g. Exxon, IBM, Xerox)
Group Captive◦ Provided the advantages of a captive to small and
mid-market employers◦ Over 50% of mid-sized employers are in an
alternative risk program
What is a “captive”?


Medical Group Captive Self Funded
Medical Underwriting/could be declined Yes No
Timely reimbursements May hold til yr. end Yes
Group selects Stop Loss Spec Level Yes, but limited Yes
Good Cash Flow needed Yes Yes
Risk Levels 3 2
Risk Sharing Yes - in Captive level No
Liability capped Yes - at level 3 Yes - at level 2
Flexibility on renewal date No Yes
Up front cost Yes - Letter of Credit Reserves - possibly waived
Should be considered for long term Yes Yes
Able to terminate arrangement Yes - but lose any claim to Yes - but responsible for runoutrefund
Flexibility on plan design Yes Yes
Flexibility on Carrier Yes - limited Yes
Biometric screening/HRA required Yes No
Requires Wellness for all members Yes No
Flexibility/negotiation on fixed costs No Possibly
Claim lasering possible Yes - every renewal Yes - first year/not at renewals
No
Yes
Fully Insured
No
N/A
N/A
No
1 (carrier)
No
No
Possibly
No
Yes
No
No
Yes
Yes
Yes

Plan sponsor chooses a Pharmacy Benefit Manager (PBM) to administer and manage prescription drug benefits separate from the PBM contracted with the health plan
Plan sponsor ends up paying less in administrative fee by contracting directly with a PBM on a carve-out basis
Plan sponsors are able to remove fees that bear no relationship to the performance of their plan or the cost of providing a pharmacy benefit◦ Negotiating contract terms and conditions◦ Audit rights◦ Clinical management ◦ Risk management programs
Prescription Drug Carve-Out

Allows for aggressive price negotiations◦ Governs pricing, discounts and rebates
Allows for carve-out specialty Prescription Drugs
Customized Clinical Programs Medical Program must be self-funded to have
ability to carve Prescription Drug Program out Caution! – It is important that data feeds
between PBM and medical carrier/administrator take place for integration of pharmacy benefit claims and medical claims
Prescription Drug Carve-Out

Private Exchange Model Video
Defined Contribution Private Exchange Model

Employer Defines their Contribution (flexible choices to fit your management philosophy and budget).
Offers employees multiple benefits choices. Employees value choice and the ability to create a
benefit plan that fits their needs.
Affordable & Sustainable Cost
New Model:
Employees get to select the benefits that make sense for their lives
Chris & Family
Previously $1,000
Now is $750

Defined Contribution Helps Create Engaged Employees by:
• Providing choice• Providing decision making tools• Creating a purchasing venue that is easy for the
employee to evaluate the options and enroll in plans that make sense for them
Invested Consumer=Engaged Employee

Participatory Activities Only (Health Contingent) Outcomes Based (Health Contingent) Tobacco Program
Primary Feature Employees are asked to Employees are asked to Employees are asked to obtain a Tobacco has it's own unique incentive/participate in an event such participate in an activity certain health outcome within the surcharge amount as well as the as a biometric screening or related to a health factor. normal range to obtain an incentive requirement that tobacco usersHealth Risk Assessment. Example: an employee who or avoid a surcharge. Example: an do not need to quit using Generally verifiable scores outside the normal employee who scores outside the tobacco. They need only to participateinformation is used. range for BMI may be asked to normal range for BMI will not in a tobacco cessation program to
participate in a walking obtain the reward or avoid the qualify for an incentive or avoid a program to obtain a reward or surcharge. Generally VERIFIABLE surcharge. There is not l imit to the avoid a surcharge. Generally information is used. number of times a tobacco user maySELF-REPORTED information go through a cessation program andis used still qualify for the reward.
Typical Employer Objective Entry Level-Educate employees Provide employees with various Manage risk/Reduce claims & improve Reduce or eliminate tobacco usageabout their personal health activities to support good health productivity/Accountability
Meet the 5 Wellness Requirements * Does not apply Applies Applies Appliesfor Health Contingent ProgramsApplication of Based on participating Based on participating in an Based on reaching goals related Based on participation in a tobaccoIncentives/Surcharges in an event activity related to a health factor to a health outcome or factor cessation program or actually quittingMaximum Incentive/ No limit 30% of the individual 30% of the individual 50% of the individual monthly Surcharge eff. 1-1-14 monthly premium monthly premium premium, whether stand-alone or
integrated with other surchargesReasonable Alternative Not required to provide RAS RAS can be another less RAS can be an activity or an easier RAS MUST be a tobacco cessationStandards (RAS) strenuous activity. MD to achieve health standard. MD type of program
verification permitted to prove verification of health health condition conditions not permitted
Impact of Incentives/ Incentives will be treated as if they were not earned(effectively having no impact on the 9.5% A tobacco surcharge will be treated as Surcharges on the 9.5% calculation) while surcharges will be treated as if they apply to all employees (effectively if no employee qualified for the Affordability Test in 2015 reducing the 9.5% by the maximum possible surcharge available to any employee) surcharge (effectively having no(Final rules have not been released) impact on the 9.5% calculation)*Frequency, Size of Reward, Reasonable Design, Uniform Availability/RAS, Notice of RAS
Powered by:
Wellness Programs & ACA Summary

Delivering available, complete, accurate data on time
Transforming information into actionable knowledge that empowers the continuum of patient care◦ Significantly enhances patient and population health◦ Control cost
Creates venue to:◦ Optimize care◦ Improve outcomes◦ Control Costs
Data Integrity

Trust & Secure – Cleansing, Archiving, Safeguarding, and Controlling Data
Visibility – Online financial and clinical dashboards, population health trends and analysis
Insight – Data driven underwriting analysis, benchmarking and modeling for plan design
Optimize – Financial Risk Pools driven by predictive analytics
Data Integrity



Thank you for your attention.
Questions…?















![National Survey of Small Businesses...Among small firms that offer health insurance coverage, few provide employees with a choice of health plans. [Charts 7-8] • Seven in ten (71%)](https://static.fdocuments.in/doc/165x107/60186a70c01a6f6142210dca/national-survey-of-small-businesses-among-small-firms-that-offer-health-insurance.jpg)

