Chest trauma by dr.damodhar.m.v
97
Chest Trauma Dr.Damodhar.M.V Resident Surgeon, Security Forces Hospital Dammam, 1
-
Upload
drdamodhar-mv -
Category
Health & Medicine
-
view
49 -
download
2
Transcript of Chest trauma by dr.damodhar.m.v

1
Chest Trauma
Dr.Damodhar.M.V
Resident Surgeon,
Security Forces Hospital Dammam,

2
Injuries to chest: • Pnuemothorax• Haemothorax• Flail chest• Diaphragmatic injury• Aortic tear• Oesophageal rupture• Pulmonary contusion• Cardiac tamponade
Procedures:• Intercostal Drains• Tracheostomy
Contents

3
Sudden and dramatic
Directly -20 – 25% (1 in every 4) trauma deaths*
Contribute to 25-50% of the remaining deaths*
>16,000 deaths per year in west*
*Source: Brunicardi FC, Anderson DK, Billar TR, Dunn DL, Hunter JG, Mathews JB, Pollock RE: Schwartz Priniciples of Surgery, 9 th edition. HTTP: www.accessmedicine.com
Chest Trauma - Incidence

4
Superiorly - Clavicles
Inferiorly- Diaphragm
Laterally- Rib cage
Boundaries of Chest
5
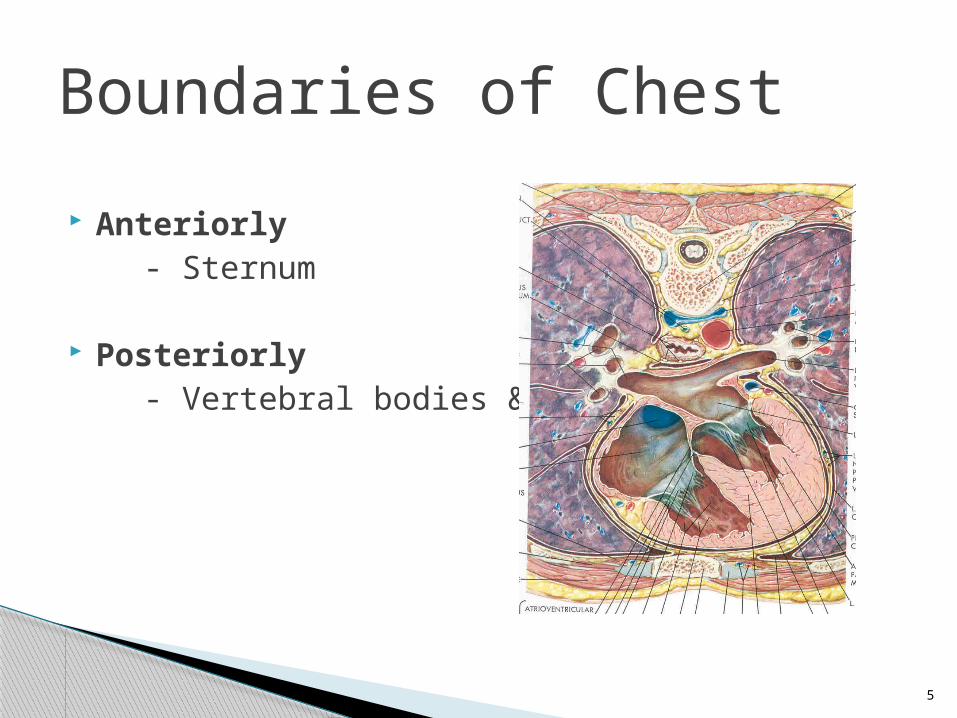
Anteriorly- Sternum
Posteriorly- Vertebral bodies & ribs
Boundaries of Chest

6
Chest wall and ribs
Lungs and pleura
Great and thoracic vessels
Heart and mediastinal structures
Diaphragm
Oesophagus
Thoracic duct
Tracheobronchial system
Contents- Thoracic cavity

7
Related to:
Mechanism of injury Location of injury Associated injuries Co-morbidities
Chest Trauma- Clinical Consequences

8
Blunt:
Mostly managed non-operatively
• Simple intubation & ventilation or• Chest tube placement
Mechanism of Injury

9
Penetrating:
• Low energy• Medium energy• High energy
Mechanism of Injury

10
• Rib fractures• Sternal fractures
• Open or Closed Pneumothorax • Unilateral / bilateral
• Hemothorax• Hemopneumothorax
Resulting Injuries

11
• Pneumo-mediastinum
• Pulmonary contusion
• Aortic Rupture
• Myocardial contusion
• Diaphragmatic rupture
Resulting Injuries

12
Primary acute killer of trauma patients inadequate delivery of O2 to tissues
HYPOXIA / HYPO-VENTILATION

13
Inadequate intravascular volume
BLOOD LOSS
Hypovolemia

14
Contusion Hematoma Alveolar collapse
Ventilation / Perfusion Mismatch

15
- Tension pneumothorax
- Open pneumothorax
CHANGES IN INTRATHORACICPRESSURE RELATIONSHIPS

16
Hypo perfusion of tissues (shock)
METABOLIC ACIDOSIS

17
ABCs
PRIMARY SURVEYAim to identify & treat immediately life threatening conditions
Management - Chest Trauma

18
- Resuscitation of vital functions
- Most life threatening injuries treated by- Airway control - Chest tube
Management - Chest Trauma

19
• Influenced by:• Mechanism of injury• High level of suspicion
• May show: Simple pneumothorax Hemothorax Pulmonary contusion Myocardial contusion Blunt aortic injury Rib fractures Diaphragmatic rupture
Detailed Secondary Survey

20
Adjuncts
CXR- basis for initiating other investigations
ALL wounds to thoracic cavity bounded back & front by
Neck & umbilicus for stabs Neck & pelvis for GSW
• MUST HAVE CXR, UPRIGHT if possible
Management- Chest Trauma

21
Focused Abdominal Sonography forTrauma (FAST)
All hemodynamically unstable blunt trauma patients
Adjuncts - FAST

22
Becoming a primary diagnostic tool fast (spiral) allow for reconstruction
Adjuncts - Cat Scan- (CT angio)

23
Penumothorax

24
Air in the pleural cavity is called Pneumothorax and when it is due to trauma it is called Traumatic Pneumothorax.
Types:
• Closed pneumothorax
• Open pneumothorax
• Tension pneumothorax
Pneumothorax

25
Air accumulates in pleural cavity through small rent in the lung due to fractured ribs.
Such rent in the lung subsequently closes and is known as pneumothorax.
Closed Pneumothorax

26
Closed Pneumothorax

27
Air enter the pleural cavity through a wound in the chest wall.
With each inspiration wound sucked into the pleural cavity.
• Sucking chest wound• Air enters pleural space• Ventilation impaired • Hypoxia results
Open Pneumothorax

28
Open Pneumothorax

29
Open Pneumothorax
30
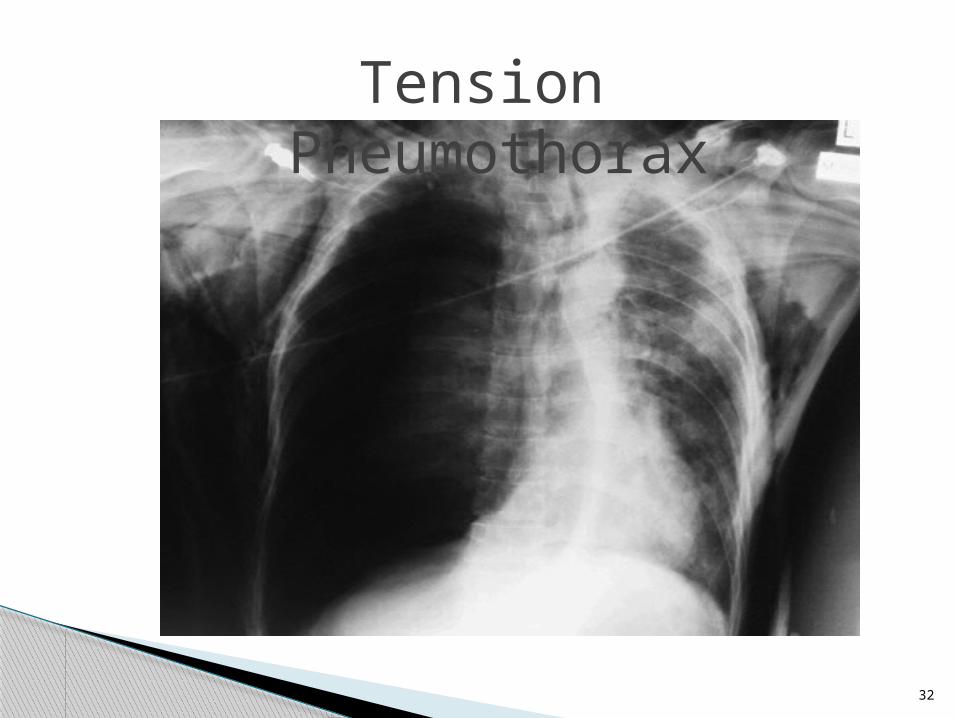
Lacerated lung communicates with branch of brachial tree.
This permits air to enter pleural cavity during inspiration, but does not permit the air to escape during expiration as rent in the lung becomes closed and the rent in the lung acts like a valve.
This causes collapse of lung on affected side.
Tension Pneumothorax

31
5T’s- Tachycardia
Tachyapnea
Tracheal shift
Tympanic note
Totally absent breath sounds on affected side
Clinical features of Pneumothorax
32
Tension Pneumothorax

33
Bilateral Tension Pneumothorax

34
Treatment : Closed pneumothorax: no active treatment. Air gets absorbed.
Open pneumothorax:Closure of the chest wall wound
Tension Pneumothorax:•Required urgent surgical intervention:•Wide bore needle inserted into pleural cavity into 2nd intercostal space 1 ½ inch lateral to sternum.
•This is followed by Underseal Intercostal Drainage.

35
Wide bore needle inserted into pleural cavity into 2nd intercostal space 1 ½ inch lateral to sternum
Tension Pneumothorax

36
Accumulation of blood in the pleural cavity due to trauma to the chest. Blood comes from
Contusion of lung Injury to parietal vessels Injury to heart and great vessels
HAEMOTHORAX

37
Clinical features
Dysponea Pain Cyanosis Decreased breath sounds Investigation- Chest X ray
Treatment ICD

38
HAEMOTHORAX

39
HAEMOTHORAX

40
Flail Chest

41
Flail chest occurs when a segment of the chest wall does not have bony continuity with the rest of the thoracic cage.
Usually defined as at least 2 fractures per rib (producing a free segment), in at least 2 ribs.
Develops in multiple rib fractures
Fracture occurs anteriorly at or near costochondral junction and posteriorly near the angles of the rib
This results in fragment of chest wall which becomes unstable having no bony connection & unable to contribute to lung expansion.
Flail Chest

42
The floating segment moves in during inspiration due to negative pressure in the pleural cavity
The floating segment moves out during expiration due to positive pressure in the pleural cavity
This results in paradoxical movement of the floating segment of the chest wall.
Known as Paradoxical respiration - that means floating segment moves in the opposite direction as the movement of the normal chest wall.
Flail Chest

43
Types
Anterior
Lateral
Posterior
Flail Chest

44
Anterior type:
Anterior ends of few ribs on both sides are fractured.
Hence, sternum along the anterior fragments of ribs of both sides becomes floating segment
Flail Chest

45

46
Lateral type:
Multiple rib fractures anteriorly and posteriorly.
Posterior type: Multiple ribs are fractured at their posterior angles on both sides Spinal column along with posterior fragments of ribs becomes
floating segments The effect of paradoxical movement is minimal.
Flail Chest

47
Flail Chest

48

49
Hypoventilation- Hypoxia
Mediastinal Flutter Mediastinum moves towards sound side during inspiration. Mediastinum moves towards affected side during expiration.
As the contents of Mediastinum are heart & great vessels, their movements result in severe shock.
Effects of Paradoxical Respiration

50
Mechanical ventilation highly effective in Flail chest.
It minimizes paradoxical respiration
Also acts as an effective “Internal Pneumatic Fixation” of the floating chest.
Treatment

51
DiaphragmaticRupture

52
- Rupture diaphragm may occur from:- Penetrating injuries - Crush injuries
- Left hemidiaphragm Ruptured more frquently by blunt trauma ( 9:1) Posterolaterally weakened due to gap for abdominal aorta & oesophageal hiatus
- Right Hemidiaphragm – protected by liver
Diaphragmatic Rupture

53
Left hemidiaphragm rupture Herniation of stomach , spleen , left transverse colon/ omentum
Right Hemidiaphragm rupture Herniation of liver
In penetrating injuries, herniation occurs rarely and slowly
Diaphragmatic Rupture

54
The symptoms of diaphragmatic rupture are similar to pneumothrax as the lung is compressed and hypoxemia develops
Chest x-ray Loss of the diaphragmatic contour Presence of bowel or NG tube in the chest Elevation of the hemidiaphragm
Intubation / mechanical ventilation needed for adequate oxygenation.
Diaphragmatic Rupture

55
Management Intubation / mechanical ventilation needed for adequate oxygenation.
Operative repair indicated in all cases.
All penetrating diaphragmatic injuries repaired via abdomen and not chest, to rule out hollow viscus injury.
Diaphragmatic Rupture

56
Diaphragmatic RupturePost traumatic air-filled viscus above the left hemidiaphragm as a consequence of diaphragmatic rupture.

57
Aortic Tear

58
• Most common cause of immediate death Motor-vehicle collisions or falls from heights 90% die immediately
The rupture is usually at the ligamentum arteriosum just distal to the left subclavian artery.
Clinical signs of traumatic aortic injury rarely present
Diagnosis based on high index of suspicion based on mechanism of injury, and imaging studies
Aortic Tear

59
Investigations:
Chest x-ray CT scan Aortography
Surgical Repair performed immediately due to fatal risk of haemorrhage.
Aortic Tear

Findings on Chest Radiograph Suggestive of a Descending Thoracic Aortic Tear
1. Widened mediastinum 2. Loss of aortic contour 3. Tracheal shift to right 4. Nasogastric tube shift 5. Left apical cap 6. Depression of the left main bronchus 7. Elevation of right main stem bronchus. 8. Obliteration of the aorticopulmonary window 9.Left sided haemothorax
Aortic Tear

Chest film findings associated with descending torn aorta include apical capping (arrows) and tracheal shift

62
Oesophageal Rupture

63
Oesophageal rupture
Most oesophageal injuries due to penetrating trauma
High index of suspicion necessary to diagnose

64
Clinical features:
Odynophagia
Subcutaneous/Mediastinal emphysema
Pleural effusion
Air in retro-oesophageal sapce
Unexplained fever within 24hrs of injury

65
Oesophageal rupture
Mortality rate rises exponentially if treatment delayed for more than 12-24 hrs.
Chest xray
Oesophagogram & Oesophagoscopy confirm diagnosis
Treatment: Operative repair & Drainage.

66
Widened mediastinum Bilateral airspace disease and pleural effusion
Left sided pleural effusion,
Subcutaneous emphysema
Pneumomediastinum
Left lower lobe atelectasis
Pulmonary edema
Oesophageal rupture

67
Esophagogram
Extravasation of dye into mediastinum and presence of a perforation in the lower left portion of the esophagus.
Oesophageal rupture

68
Pulmonary Contusion

69
• Pulmonary Contusion
• Term used to indicate consequences of blunt trauma to lung
Causes:
• Rapid deceleration of chest against automobile steering wheel
• Fall from height
• Blast injuries
• Fracture ribs / sternum
• Flail chest without any evidence of rib fracture
Pulmonary contusion

70
Contused lung characterized by:
Capillary disruption
Intra alveolar & interstitial haemorrhage
Oedema
Fluid obstruction of small airways
Leucocyte infiltration
Pulmonary contusion

71
Pulmonary contusion
Chest x ray- Fluffy infiltrate in contused lung
Increases in density within a day or two

72
- Pulmonary contusion frequently manifests itself as
Hypoxemia.
- May cause serious depression of respiratory function or loss of pulmonary compliance.
Treatment
- Contusion results in areas of consolidation & resolves spontaneously.
- Oxygen therapy
- Positive pressure with CPAP mask / Intubation and mechanical ventilation with PEEP.
- Adequate analgesia
Pulmonary contusion

73
Cardiac Tamponade

74
• Most frequently caused by penetrating thoracic injuries
• Blunt trauma- Myocardial rupture
Coronary artery laceration
Ascending dissection of aortic tear
• Accumulation of as little as 150ml may impair diastolic filling.
Cardiac Tamponade

75
• Beck’s triad Hypotension Neck veins distended Heart sounds muffled
• Paradoxical pulse
• Breath sounds equal
Cardiac Tamponade

76
Investigations:
Echo
Angiography
Treatment
• Treat for shock
• Fluid administration Titrate to peripheral pulse (90–100 mmHg)
• Monitor and treat dysrhythmias
• Monitor for: Hemothorax Pneumothorax
Cardiac Tamponade

77
Cardiac Tamponade

78
Myocardial Contusion

79
• Most common cardiac injury Blunt anterior chest injury
• May vary from superficial epicardial petechiae to transmural damage
• Same as myocardial infarction Chest pain Dysrhythmias Cardiogenic shock (rare)
• ECG- non specific ST-T wave changes
• ICU monitoring for 24hrs
• Treat as cardiac tamponade
Myocardial contusion

80
Myocardial contusion

81
Movement of diaphragm and thoracic structures causes partial defibrination of blood that is accumulated in pleural cavity.
So blood remains in liquid state for considerable period of time without being clotted.
Pleural enzymes in the cavity produces a clot lysin within few hours after bleeding stops.
Why blood in the pleural cavity will not clot?

82
Indications:
Pneumothorax
Haemothorax
Empyema thoracis
Massive pleural effusion
Intercostal drainage tube

83
•Procedure done local anesthesia
•Chest tube introduced into pleural cavity and connected to underwater drainage tube.
•For Pneumothorax- 2nd Intercostal space,mid clavicular line
•For Haemothorax-6th Intercostal space mid axillary line
Intercostal drainage

84
Mid-axillary line
Site:

85
Intercostal drainage

86
Intercostal drainage

87
Hemothorax – usually laceration of intercostals vessel, may require thoracotomy
Lung laceration especially when adhesions present
Diaphragm / abdominal cavity penetration - placed too low
Stomach colon injury - diaphragmatic hernia not recognizedTube placedsubcutaneously – not inpleural cavity
Tube placed too far = pain
Tube falls out = not secured properly
Chest tube insertion-complications

88
Subcutaneous emphysema

89
Tracheostomy

90
Tracheostomy (also referred to as pharyngotomy, laryngotomy, and tracheotomy)
A surgical procedure in which an incision on the anterior aspect of the neck and opening a direct airway through an incision in the trachea is made.
Relieves airway obstruction/protects airway

91
• Emergency Tracheostomy
• Elective Tracheostomy
Tracheostomy

92
Indications for tracheostomy Relief of Acute upper airway obstruction (Inhaled foreign body, large pharyngolaryngeal tumour ,acute
pharyngolaryngeal infections in children)
Potential upper airway obstruction (after major surgery involving the oral cavity,pharynx, larynx or neck)
Protection of the lower airway
Control of secretions
Ventilatory support in respiratory failure

93
Short horizontal incision made over 2nd or 3rd tracheal ring
Neck extended
2nd and 3rd tracheal rings incised vertically

94
Complications
Intraoperative complications
•Haemorrhage
•Injury to paratracheal structures, particularly the carotid artery, recurrent laryngeal nerve and oesophagus
•Damage to the trachea

95
ComplicationsEarly postoperative complications •Apnoea caused by a fall in the PCO2•Haemorrhage•Subcutaneous emphysema, pneumomediastinum and pneumothorax•Accidental extubation•Anterior displacement of the tube •Obstruction of the tube lumen •Tip occlusion against the tracheal wall•Infection•Swallowing dysfunction

96
ComplicationsLate postoperative complications
• Difficult decannulation
•Tracheocutaneous fistula
•Tracheo-oesophageal fistula
•Tracheal stenosis

Wishing you all a blessed time during the holy month of Ramadan
Dr.Damodhar.M.V