CHEMISTRY OF BONE
58
AND THE ROLE OF HORMONES IN MODELLING & REMODELLING By Dr Faiza Waseem
description
CHEMISTRY OF BONE. AND THE ROLE OF HORMONES IN MODELLING & REMODELLING By Dr Faiza Waseem. Bone. Inorganic (67%) Calcium hydroxyapatite Ca 10 (PO 4 ) 6 (OH) 2 along with sodium, magnesium, carbonate & fluoride. Organic (33%) component is called osteoid Type I collagen (28%) - PowerPoint PPT Presentation
Transcript of CHEMISTRY OF BONE

AND THE ROLE OF HORMONES IN MODELLING & REMODELLING
By Dr Faiza Waseem

Inorganic (67%)
◦ Calcium hydroxyapatite Ca10(PO4)6(OH)2
◦ along with sodium, magnesium, carbonate & fluoride.

Organic (33%) component is called osteoid◦ Type I collagen (28%)◦ Type V collagen is also present in small
amounts◦ Non-collagen structural proteins (5%)
Proteoglycans Sialoproteins Phosphoproteins Bone specific proteins: osteocalcin, osteonectin
◦ Growth factors and cytokines (Trace)

Bone undergoes continuous turnover or remodeling throughout life◦ About 20% of bone is undergoing remodeling at
any one time Bone remodelling consists of : resorption Followed by deposition of new bone tissue So adapts to physical & hormonal signals.

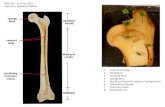
The cells involved in bone resorption and deposition are
osteoclast osteoblast/cyte


Osteoclasts are multinucleated Derived from pluripotent hematopoietic
stem cells. A ruffled border ATPase expels protons across the ruffled
border into the resorption area. pH lowered to 4 or less increases the solubility of hydroxy apatite

Demineralization occurs Lysosomal acid proteases released that
digest the matrix proteins


Mononuclear cells Synthesize most of the proteins found in
bone, growth factors and cytokines Responsible for the deposition of new bone
matrix (osteoid) & its mineralization Control mineralization by regulating the
passage of calcium and phosphate ions across their surface membranes.
The latter contain alkaline phosphatase which is used to generate phosphate ions from organic phosphates.

Alkaline phosphatase contributes to mineralization but in itself is not sufficient
Type 1 collagen is necessary Acidic phosphoproteins eg bone sialoprotein
act as sites of nucleation. Contain poly-Asp and poly-Glu stretches
that bind calciummineralization.

4% of compact bone and 20% of trabecular bone is renewed annually.

PTH & VITAMIN D stimulate osteoblasts Cortisteroids inhibit osteoblasts PTH & VITAMIN D also stimulate osteoclasts Calcitonin & estrogens inhibit osteoclasts.

Total calcium in the human body is 1-1.5 kg. 99% present in bone 1% in ECF SOURCES: milk, cheese, egg yolk, nuts The normal plasma calcium
level=9-11mg/dl


Vitamin D, after its activation to the hormone 1,25-dihydroxy Vitamin D3 is a principal regulator of Ca++.

Vitamin D is required for the intestinal absorption of calcium
Induces synthesis of calbindin Vitamin D acts independently on bone It increases the number and activity of
osteoblasts, the bone forming cells. Secretion of alkaline phosphatase by
osteoblasts is increased by vitamin D

Humans acquire vitamin D from two sources.
Vitamin D is produced in the skin by ultraviolet radiation and ingested in the diet.

Vitamin D3 synthesis occurs in keratinocytes in the skin.
7-dehydrocholesterol is photoconverted to previtamin D3, then spontaneously converts to vitamin D3.
Previtamin D3 will become degraded by over exposure to UV light and thus is not overproduced.
Also 1,25-dihydroxy-D (the end product of vitamin D synthesis) feeds back to inhibit its production.

Normal metabolism
Vit D
25-HCC (Liver)
Ca/PTH 1,25-DHCC 24,25-DHCC (Kidney) (Kidney)

The mitochondrial P450 enzyme 1-hydroxylase converts it to 1,25-dihydroxy-D, the most potent metabolite of Vitamin D.
The 1-hydroxylase enzyme is the point of regulation of D synthesis.
Feedback regulation by 1,25-dihydroxy D inhibits this enzyme.
PTH stimulates 1-hydroxylase and increases 1,25-dihydroxy D.

Phosphate inhibits 1-hydroxylase and decreased levels of PO4 stimulate 1-hydroxylase activity
If excess 1,25-(OH)2-D is produced 24-hydroxylated to remove it.

Normal daily requirement 200IU/day

Secreted by parathyroid glands ◦ Rapid response to reduced calcium (minutes)
Storage of PTH is only for about 1 hour.



Upon entry of pre-pro-PTH into endoplasmic reticulum, leader sequence is removed from the amino terminal to form the 90 a.a polypeptide pro-PTH.
Six additional a.a residues are removed from the amino terminal of pro PTH in the golgi apparatus and the 84 a.a polypeptide PTH is packaged in secretory granules and released as the main secretory product of the chief cells.

The overall action of PTH is to increase plasma Ca++ levels and decrease plasma phosphate levels.
PTH acts directly on the bones to stimulate Ca++ resorption and kidney to stimulate Ca++ reabsorption in the distal tubule of the kidney and to inhibit reabosorptioin of phosphate (thereby stimulating its excretion).
PTH also acts indirectly on intestine by stimulating 1,25-(OH)2-D synthesis.

Extracellular Ca 2+ regulates secretion of PTH◦ Low Ca 2+ increases◦ High Ca 2+ decreases

An acute decrease of calcium marked increase of PTH mRNA increased rate of PTH secretion and synthesis.
However , 80-90% of the proPTH synthesized is quickly degraded.
This rate of degradation decreases when Ca+2 conc are low
& it increases when Ca+2 conc are high. A Ca+2 receptor on the surface of the
parathyroid cell mediates these effects.

Regulation of secretion 1,25 dihydrocholecalciferol acts directlly on
the parathyroid gland to decrease prepro PTH mRNA.
Increased plasma phosphate stimulate PTH secretion by lowering plasma Ca2+ and inhibiting the formation of 1,25 dihydroxy cholecalciferol.
Magnesium is required to maintain normal parathyroid secretory response .

Secreted by the thyroid gland Human calcitonin has M.W 3400 and contains 32
amino acid residues . Effects are much less than those of PTH

Decreases serum calcium level Decreases the activity of osteoclasts and
increases that of osteoblasts Causes reduced bone turnover PTH and Calcitonin are antagonistic. Together they promote bone growth and
remodelling. In kidney calcitonin increases phosphorus
excretion. This action is similar to PTH.




A generalized progressive reduction in bone tissue mass per unit volume.
The ratio of mineral to organic elements is unchanged in the remaining normal bone.
Skeletal weakness Fractures Estrogens & IL-1and IL-6 involved in the
causation of osteoporosis.

The total bone mass of humans peaks at 25-35 years of age.
Men have more bone mass than women. A gradual decline occurs in both genders
with aging, but women undergo an accelerated loss of bone due to increased resorption during perimenopause.
Bone resorption exceeds formation.

Reduced risk:
◦Calcium in the diet
◦habitual exercise
◦avoidance of smoking and alcohol intake
◦avoid drinking carbonated soft drinks

Osteoporosis is the most common metabolic bone disease
WHO suggests that osteoporosis exists when bone density falls 2.5 standard deviations or more below the mean for young healthy adults of the same race and gender.


Gender (M>F), males have greater PBM than females
Race (Blacks >Whites) Genetics (osteoporosis runs in families and
this may be the predominant factor) Gonadal steroids (estrogen and testosterone
increase bone mass) Growth hormone (increases bone mass) Calcium intake (supplements work) Exercise (increases bone mass)


3 types Post-menopausal (Loss of oestrogen - incr
osteoclastic activity).In males a decline in testosterone –incr osteoclastic activity)
Idiopathic (occurs in children and young adults)
Involutional (elderly)

uncommon Nutrition - malnutr, malabs Endocrine - Hyper PTH, Cush, Drug induced - steroid, alcohol, smoking

Exercise, activity Calcium intake should be 1000-1500 mg/day
◦ Males and females should take in 1000-1500 mg/day◦ All adults greater than 65 years should take 1500 mg/day◦ Three glasses of milk or three cups of yogurt per day provide
1000-1500 mg/day Estrogen treatment
◦ Estrogen inhibits osteoclastic activity◦ This therapy needs to be individualized
Estrogen may increase the incidence of breast cancer, heart attacks, stroke, blood clots

Bisphosphonates inhibit osteoclasts & are are classified as anti-resorptive medications
Calcitonin :Probably least effective Rx Vitamin D
◦ 400 IU per day

◦ It is due to deficiency of Vitamin D during childhood. The full-blown condition in children is characterized by weakness and bowing of weight bearing bones, dental defects and hypoclacemia.


It is due to deficiency of vitamin D during adulthood, results from demineralization of bones, especially in women who have little exposure to sunlight.

Osteomal Osteopor
Ill Not illGeneral ache Asympt till #Weak muscles normalAlk ph incr normal

Inability to resorb bone Increased bone density Mutations in the gene encoding carbonic
anhydrase II(CA II).

◦ Excess parathormone cause bone resorption.

Hyperparathyroidism

◦ It is brittle bone disease characterized by abnormal fragility of bones.
◦ Over 90% of patients with osteo-genesis imperfecta have mutation in genes.
◦ The most frequent type results in the replacement of glycine by another bulkier amino acid, affecting formation of the triple helix.
◦ In general, these mutations result in decreased expression of collagen

• Or in structurally abnormal pro chains that assemble into abnormal fibrils, weakening the overall structure of bone.
When one abnormal chain is present ,it may interact with two normal chains, but folding may be prevented, resulting in enzymatic degradation of all of the chains.
This is called procollagen suicide

The scleras are thin & may appear blue owing to a deficiency of connective tissue.
Four types mild, extensive, severe and variable .
The extensive type occurring in the newborn is the most ominous.
Affected infants may be born with multiple fractures and not survive.