Chemically Modified Antisense Oligonucleotide Against ARL4C ... · Large Molecule Therapeutics...
12
Large Molecule Therapeutics Chemically Modified Antisense Oligonucleotide Against ARL4C Inhibits Primary and Metastatic Liver Tumor Growth Takeshi Harada 1 , Shinji Matsumoto 1 , Suguru Hirota 1 , Hirokazu Kimura 1 , Shinsuke Fujii 1 , Yuuya Kasahara 2,3 , Hidetoshi Gon 4 , Toshihiko Yoshida 4 , Tomoo Itoh 5 , Naotsugu Haraguchi 6 , Tsunekazu Mizushima 6 , Takehiro Noda 6 , Hidetoshi Eguchi 6 , Satoshi Nojima 7 , Eiichi Morii 7 , Takumi Fukumoto 4 , Satoshi Obika 2,3 , and Akira Kikuchi 1 Abstract ADP-ribosylation factor-like 4c (ARL4C) is identified as a small GTP-binding protein, which is expressed by Wnt and EGF signaling and plays an important role in tubulogenesis of cultured cells and the ureters. ARL4C is little expressed in adult tissues, but it is highly expressed in lung cancer and colorectal cancer and shown to represent a molecular target for cancer therapy based on siRNA experiments. This study revealed that ARL4C is highly expressed in primary hepatocellular carcino- ma (HCC) tumors and colorectal cancer liver metastases, and that ARL4C expression is associated with poor prognosis for these cancers. Chemically modified antisense oligonucleo- tides (ASO) against ARL4C effectively reduced ARL4C expres- sion in both HCC and colorectal cancer cells and inhibited proliferation and migration of these cancer cells in vitro. ARL4C ASOs decreased the PIK3CD mRNA levels and inhibited the activity of AKT in HCC cells, suggesting that the downstream signaling of ARL4C in HCC cells is different from that in lung and colon cancer cells. In addition, subcutaneous injection of ARL4C ASO was effective in reducing the growth of primary HCC and metastatic colorectal cancer in the liver of immu- nodeficient mice. ARL4C ASO accumulated in cancer cells more efficiently than the surrounding normal cells in the liver and decreased ARL4C expression in the tumor. These results suggest that ARL4C ASO represents a novel targeted nucleic acid medicine for the treatment of primary and metastatic liver cancers. Introduction The liver is an organ that develops primary and metastatic tumors. Hepatocellular carcinoma (HCC) is the fifth common type of cancer worldwide and the third leading cause of cancer death (1). The median survival is approximately 6 to 20 months after diagnosis for the intermediate and advanced stages, and the 5-year survival of patients with HCC is less than 30%. Even after apparently curative surgical resection, recurrent HCC develops in 80% of patients within 5 years because of intrahepatic metastasis. For unresectable HCC, different treatment modalities are avail- able, including radiation, radioembolization, systemic chemo- therapy, and molecularly targeted therapy. Oral sorafenib, which is a multityrosine kinase inhibitor, is currently the first-line treatment for advanced HCC but its effectiveness is limited (2). The liver is also a common site of metastasis from other solid tumors, especially tumors originating from the intra-abdominal organs, including the stomach, pancreas, colon, gallbladder, and ovary (3). Less than 10% to 15% of patients with liver-only solid tumor metastases are candidates for resection (4). For the majority of patients with primary and metastatic liver cancers who are not candidates for surgical resection, novel treatment approaches to control and potentially cure the liver tumors must be explored. ADP-ribosylation factor (ARF)-like proteins (ARL) are one of the subgroups of the ARF family of proteins in the small GTP- binding protein superfamily (5). ARF family proteins are essential regulators of the actin remodeling and membrane-trafficking pathways, including those involved in secretion, endocytosis, and phagocytosis (6). However, the functions of most ARLs remain unclear (7). ARF-like 4c (ARL4C), a member of ARL family proteins, is a target protein that is expressed as a result of Wnt/ b-catenin and EGF/RAS/MAPK signaling and plays an important role in both epithelial morphogenesis and tumorigenesis (8, 9). Immunohistologic analysis has revealed that ARL4C is fre- quently overexpressed in colorectal cancer, lung cancer, and tongue cancer but little detected in nontumor regions of these tissues (9, 10). In HCT116 colorectal cancer cells and A549 lung adenocarcinoma cells, ARL4C expression is upregulated by Wnt/ b-catenin or RAS/MAPK signaling (9). In addition, ARL4C is highly expressed in NCI-H520 lung squamous cell carcinoma cells because of DNA hypomethylation of the ARL4C gene (10). 1 Department of Molecular Biology and Biochemistry, Graduate School of Med- icine, Osaka University, Osaka, Japan. 2 Graduate School of Pharmaceutical Sciences, Osaka University, Osaka, Japan. 3 National Institutes of Biomedical Innovation, Health and Nutrition, Osaka, Japan. 4 Division of Hepato-Biliary- Pancreatic Surgery, Department of Surgery, Kobe University Graduate School of Medicine, Kobe, Hyogo, Japan. 5 Division of Diagnostic Pathology, Kobe Univer- sity Graduate School of Medicine, Kobe, Hyogo, Japan. 6 Department of Gas- troenterological Surgery, Graduate School of Medicine, Osaka University, Osaka, Japan. 7 Department of Pathology, Graduate School of Medicine, Osaka Univer- sity, Osaka, Japan. Note: Supplementary data for this article are available at Molecular Cancer Therapeutics Online (http://mct.aacrjournals.org/). Corresponding Author: Akira Kikuchi, Graduate School of Medicine, Osaka University, 2-2, Yamadaoka, Suita, Osaka 565-0871, Japan. Phone: 81-6-6879- 3410; Fax: 81-6-6879-3419; E-mail: [email protected] doi: 10.1158/1535-7163.MCT-18-0824 Ó2019 American Association for Cancer Research. Molecular Cancer Therapeutics Mol Cancer Ther; 18(3) March 2019 602 on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824
Transcript of Chemically Modified Antisense Oligonucleotide Against ARL4C ... · Large Molecule Therapeutics...

Large Molecule Therapeutics
Chemically Modified Antisense OligonucleotideAgainst ARL4C Inhibits Primary and MetastaticLiver Tumor GrowthTakeshi Harada1, Shinji Matsumoto1, Suguru Hirota1, Hirokazu Kimura1, Shinsuke Fujii1,Yuuya Kasahara2,3, Hidetoshi Gon4, Toshihiko Yoshida4, Tomoo Itoh5,Naotsugu Haraguchi6, Tsunekazu Mizushima6, Takehiro Noda6, Hidetoshi Eguchi6,Satoshi Nojima7, Eiichi Morii7, Takumi Fukumoto4, Satoshi Obika2,3, and Akira Kikuchi1
Abstract
ADP-ribosylation factor-like 4c (ARL4C) is identified as asmall GTP-binding protein, which is expressed by Wnt andEGF signaling and plays an important role in tubulogenesis ofcultured cells and the ureters. ARL4C is little expressed in adulttissues, but it is highly expressed in lung cancer and colorectalcancer and shown to represent a molecular target for cancertherapy based on siRNA experiments. This study revealed thatARL4C is highly expressed in primary hepatocellular carcino-ma (HCC) tumors and colorectal cancer liver metastases, andthat ARL4C expression is associated with poor prognosis forthese cancers. Chemically modified antisense oligonucleo-tides (ASO) against ARL4C effectively reduced ARL4C expres-sion in both HCC and colorectal cancer cells and inhibited
proliferation andmigrationof these cancer cells in vitro. ARL4CASOs decreased the PIK3CD mRNA levels and inhibited theactivity of AKT in HCC cells, suggesting that the downstreamsignaling of ARL4C in HCC cells is different from that in lungand colon cancer cells. In addition, subcutaneous injection ofARL4C ASO was effective in reducing the growth of primaryHCC and metastatic colorectal cancer in the liver of immu-nodeficient mice. ARL4C ASO accumulated in cancer cellsmore efficiently than the surrounding normal cells in the liverand decreased ARL4C expression in the tumor. These resultssuggest that ARL4C ASO represents a novel targeted nucleicacidmedicine for the treatment of primary andmetastatic livercancers.
IntroductionThe liver is an organ that develops primary and metastatic
tumors. Hepatocellular carcinoma (HCC) is the fifth commontype of cancer worldwide and the third leading cause of cancerdeath (1). The median survival is approximately 6 to 20 monthsafter diagnosis for the intermediate and advanced stages, and the5-year survival of patients with HCC is less than 30%. Even afterapparently curative surgical resection, recurrent HCC develops in80% of patients within 5 years because of intrahepatic metastasis.For unresectable HCC, different treatment modalities are avail-able, including radiation, radioembolization, systemic chemo-
therapy, and molecularly targeted therapy. Oral sorafenib, whichis a multityrosine kinase inhibitor, is currently the first-linetreatment for advanced HCC but its effectiveness is limited (2).The liver is also a common site of metastasis from other solidtumors, especially tumors originating from the intra-abdominalorgans, including the stomach, pancreas, colon, gallbladder, andovary (3). Less than 10% to 15% of patients with liver-only solidtumormetastases are candidates for resection (4). For themajorityof patients with primary and metastatic liver cancers who are notcandidates for surgical resection, novel treatment approaches tocontrol and potentially cure the liver tumors must be explored.
ADP-ribosylation factor (ARF)-like proteins (ARL) are one ofthe subgroups of the ARF family of proteins in the small GTP-binding protein superfamily (5). ARF family proteins are essentialregulators of the actin remodeling and membrane-traffickingpathways, including those involved in secretion, endocytosis,and phagocytosis (6). However, the functions of most ARLsremain unclear (7). ARF-like 4c (ARL4C), amember of ARL familyproteins, is a target protein that is expressed as a result of Wnt/b-catenin and EGF/RAS/MAPK signaling and plays an importantrole in both epithelial morphogenesis and tumorigenesis (8, 9).
Immunohistologic analysis has revealed that ARL4C is fre-quently overexpressed in colorectal cancer, lung cancer, andtongue cancer but little detected in nontumor regions of thesetissues (9, 10). In HCT116 colorectal cancer cells and A549 lungadenocarcinoma cells, ARL4C expression is upregulated by Wnt/b-catenin or RAS/MAPK signaling (9). In addition, ARL4C ishighly expressed in NCI-H520 lung squamous cell carcinomacells because of DNA hypomethylation of the ARL4C gene (10).
1Department of Molecular Biology and Biochemistry, Graduate School of Med-icine, Osaka University, Osaka, Japan. 2Graduate School of PharmaceuticalSciences, Osaka University, Osaka, Japan. 3National Institutes of BiomedicalInnovation, Health and Nutrition, Osaka, Japan. 4Division of Hepato-Biliary-Pancreatic Surgery, Department of Surgery, Kobe University Graduate School ofMedicine, Kobe, Hyogo, Japan. 5Division of Diagnostic Pathology, Kobe Univer-sity Graduate School of Medicine, Kobe, Hyogo, Japan. 6Department of Gas-troenterological Surgery, Graduate School ofMedicine, Osaka University, Osaka,Japan. 7Department of Pathology, Graduate School of Medicine, Osaka Univer-sity, Osaka, Japan.
Note: Supplementary data for this article are available at Molecular CancerTherapeutics Online (http://mct.aacrjournals.org/).
Corresponding Author: Akira Kikuchi, Graduate School of Medicine, OsakaUniversity, 2-2, Yamadaoka, Suita, Osaka 565-0871, Japan. Phone: 81-6-6879-3410; Fax: 81-6-6879-3419; E-mail: [email protected]
doi: 10.1158/1535-7163.MCT-18-0824
�2019 American Association for Cancer Research.
MolecularCancerTherapeutics
Mol Cancer Ther; 18(3) March 2019602
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

ARL4C is involved in the activation of Ras-related C3 botulinumtoxin substrate (RAC), the inhibition of ras homolog familymember (RHO), and the nuclear localization of Yes-associatedprotein (YAP) and transcriptional coactivator with PDZ-bindingmotif (TAZ) in these cancer cells. ARL4C depletion in cancer cellsreduced migration, invasion, and proliferation both in vitro andin vivo. Furthermore, the direct injection of ARL4C siRNA intoHCT116 xenograft tumors inhibited tumor growth in immuno-deficient mice (9). Therefore, ARL4C may represent a novelmolecular target for cancer therapy.
Oligonucleotide-based therapeutics has been recognized as apromising and potent systemic approach for the treatment ofincurable diseases (11–13). There are several types of oligonu-cleotides, including antisense oligonucleotides (ASO), siRNAs,aptamers, and miRNAs. At present, some ASO therapies againstcytomegalovirus retinitis, age-relatedmacular degeneration of theretina, homozygous familial hypercholesterolemia, Duchenemuscular dystrophy, and spinal muscular atrophy have receivedFDAapproval (14).However, nooligonucleotide drugs havebeenindicated for cancer. Oligonucleotide therapeutics have problemswith susceptibility to nuclease degradation, inefficient delivery totarget cells following systemic administration, and potentiallyserious nonspecific side effects, which result in unsatisfactoryin vivo gene silencing to warrant clinical trials. Therefore, chemicalmodification strategies have been developed to overcome theseobstacles (15). In particular, a combination of a 20,40-bridgednucleic acid (also known as a locked nucleic acid, LNA) andphosphorothioate linkages exhibits high target RNA binding,resistance to nuclease degradation, and acceptable pharmacoki-netics. Additional optimization of the bridged nucleic acids, inwhich the cyclic amide structure is introduced into the LNA(named amide-bridged nucleic acid, AmNA), has furtherimproved these characteristics (16).
Because ASOs tend to be delivered to the liver and the kid-ney (17), we investigated whether ARL4C is involved in theproliferation of liver cancer cells and if AmNA–ASO therapeuticsagainst ARL4C could represent a novel therapy for the primaryand metastatic liver tumors.
Materials and MethodsPatients and cancer tissues
This study involved 128 patients with HCC (stage I to IVA) withages ranging from 21 to 81 years (median, 69 years), who under-went surgical resection at Kobe University Hospital between Jan-uary 2010 and December 2012, and 115 patients with colorectalcancer with ages ranging from 28 to 91 years (median, 66 years),who underwent surgical resection at Osaka University Hospitalbetween June 2007 and February 2017. The HCC cases did notinclude patients with distant metastasis. The colorectal cancercases included stage 0 to IIIC (102 cases) and stages IVA and IVB(13 cases). Tumors were staged according to the Union for Inter-national Cancer Control (UICC) TNM staging system. Resectedspecimens were macroscopically examined to determine the loca-tion and size of tumors. Histologic specimens were fixed in10% (v/v) formalin and paraffin embedded. The specimens weresectioned at a 4-mm thickness and stained with hematoxylin andeosin (H&E) or immunoperoxidase for independent evaluation.
The protocol for this study was approved by the ethical reviewboard of theGraduate School ofMedicine, KobeUniversity, Japan(No. 180048) and the Graduate School of Medicine, Osaka
University, Japan (No. 13032) under Declaration of Helsinki,andwritten informed consent was obtained from all patients. Thestudy was performed in accordance with the Committee guide-lines and regulations.
Immunohistochemical studiesImmunohistochemical studies were performed as previously
described (9) with modification. When the total area of a tumorlesion showed >20% ARL4C staining, the results were defined asARL4C-positive. Three investigators assessed the sections inde-pendently in a blinded fashion.
MaterialsHCT116 cells were provided by Dr. T. Kobayashi (Hiroshima
University, Hiroshima, Japan) in November 2003. A549 cellswere provided by Dr. Y. Shintani (Osaka University, Suita, Japan)in January 2014. HCC cells (HLE, HLF, HuH-7, and PLC) werepurchased from the Japanese Collection of Research Bioresources(Osaka, Japan) in June 2015. HepG2 cells were purchased fromthe ATCC in July 2017. Mycoplasma testing and cell line authen-tication were not conducted. HLE, HLF, HuH-7, PLC, HCT116,and A549 cells were maintained in DMEM supplemented with10% FBS. HepG2 cells were grown in E-MEM (Wako; Catalog No.051-07615) supplemented with GlutaMAX I (Life Technologies;Catalog No. 35050-061), MEM Non-Essential Amino Acids (LifeTechnologies; Catalog No. 11140-050), and 10% FBS. HLE cellsstably expressing GFP (HLE/GFP) or ARL4C (HLE/ARL4C-GFP)and HCT116 stably expressing luciferase (HCT/Luc) were gener-ated using lentivirus as described previously (8, 9).
Anti-ARL4C and Anti-PIK3CD antibodies were purchased fromAbcam and Santa Cruz Biotechnology, respectively. Anti-phos-pho AKT (S473), anti-AKT, anti-Ki-67, and anti-YAP/TAZ anti-bodieswere obtained fromCell Signaling Technology. PD184161(a selective MEK1/2 inhibitor; ref. 18) and VivoGlo luciferin werefrom Sigma-Aldrich and Promega, respectively. SecinH3 [aninhibitor of ARF nucleotide-binding site opener (ARNO);ref. 19] and NSC23766 (a RAC inhibitor; ref. 20) were fromTOCRIS Bioscience and Merck Millipore, respectively.
Generation of ASOs targeting for ARL4CPhosphorothioate 15-mer or 19-mer ASOs containing AmNA
monomers or 6-carboxyfluorescein (FAM)-labeled ASO weresynthesized by GeneDesign based on the previously describedmethod (16, 21). The sequences of the ASOs are listed in Sup-plementary Table S1.
HLE, HCT116, and A549 cells were transfected with ASOsat 0.5 to 50 nmol/L and siRNAs at 10 to 20 nmol/L usingLipofectamine 3000 (Invitrogen) or RNAiMAX (Invitrogen) inantibiotics-free medium, respectively. The transfected cells werethen used for experiments conducted at 36 to 48 hours aftertransfection.
Xenograft liver tumor formation and in vivo ASO treatmentA HLE cell (1 � 107 cells) pellet was suspended in 100 mL of
Matrigel matrix high concentration (BD Biosciences) anddirectly injected into the liver of anesthetized 8-week-old maleBALB/cAJcl-nu/nu mice (nude mice; CLEA Japan). ASO (50 mg/body, approximately 2.5 mg/kg; 100 mg/body, approximately5 mg/kg) was administered subcutaneously twice per weekfrom day 0. The mice were euthanized 29 days after transplan-tation. Tumor weights were collected and subjected to histo-logic analyses.
ARL4C ASO Inhibits Liver Tumor Growth
www.aacrjournals.org Mol Cancer Ther; 18(3) March 2019 603
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

HCT116/Luc cells (2.5 � 105 cells) resuspended in 100 mL ofPBS were injected into the spleens of anesthetized 8-week-oldmale nude mice. Nineteen days after implantation, ASO(50 mg/body) was administered subcutaneously twice per week.The mice were euthanized 47 days after transplantation, andhistologic analysis was performed. Tumor sizes were measuredonce per week using the IVIS imaging system (Xenogen Corp.).For the in vivo imaging, 100 mL of VivoGlo luciferin (30 mg/mL)was administrated intraperitoneally and then bioluminescenceimaging was recorded 10 minutes after administration of lucif-erin. All protocols used for animal experiments in this studywere approved by the Animal Research Committee of OsakaUniversity, Japan (No. 21-048-1).
Clinical data analyses using open sourcesThe data of ARL4C mRNA expression in liver HCC and colo-
rectal cancer were obtained from the Gene Expression ProfilingInteractive Analysis (GEPIA) online database (http://gepia.cancer-pku.cn/). Tumors and normal samples in the GEPIA databasewere derived fromTCGA andGenotype-Tissue Expression (GTEx)projects. Differential analysis was performed using one-wayANOVA. P values below 0.05 were considered statistically signif-icant. The correlations of overall survival rates with ARL4CmRNAexpression in the colorectal cancer of the TCGA dataset wereanalyzed using OncoLnc (http://www.oncolnc.org) and visual-ized using GraphPad Prism (GraphPad Software). High and lowARL4C expression groups were classified by the median value ofARL4C expression of patientswith colorectal cancer in the dataset.Coexpression analysis using the TCGA dataset was performedusing the "R2: Genomics Analysis Platform (http://r2.amc.nl)"and visualized using GraphPad Prism. P values and r values werecalculated using GraphPad Prism.
In silico analysis of candidate genes for potential off-targeteffects of ARL4C ASOs
Potential off-target genes for the ARL4C ASOs [hARL4C ASO-1316-AmNA [15-mers] (ARL4C ASO-1316) and hARL4C ASO-3223-AmNA[19-mers] (ARL4CASO-3223)]were identifiedusingbasic local alignment search tools (BLASTþ programs) with thehuman genomic plus transcript (Human GþT) database (Build2.7.1) and Megablast algorithm.
Statistical analysesEach experiment was performed at least three times, and the
results are presented as the mean � SD. The cumulative proba-bilities of recurrence-free survival were determined using theKaplan–Meier method; the log-rank test was used to assess sta-tistical significance. The Student t test was used to determine thestatistical significance in other experiments; P values <0.05 wereconsidered statistically significant.
Other methodsCell migration assays and quantitative real-time PCR anal-
yses were performed as previously described (9). The primersand siRNAs used in these experiments are listed in Supplemen-tary Tables S2 and S3, respectively. The cell proliferation assaywas performed using the CyQUANT NF Cell Proliferation AssayKit (ThermoFisher Scientific) according to the manufacturer'sinstructions. Fluorescence was measured using a fluorescencemicroplate reader (Synergy HTX Multi-Mode Microplate Read-er; BioTek).
ResultsARL4C is expressed in primary and metastatic tumors
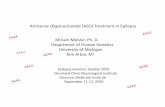
ARL4C expression was analyzed in primary HCC using immu-nohistochemistry. Tumors in which greater than 20% of thetumor lesions were stained with the anti-ARL4C antibody wereconsidered ARL4C-positive. Among the 128 HCC samples,ARL4C was detected and positive in 33 tumors (25.8%) but onlyminimally detected in matched nontumor regions (Fig. 1A).ARL4C staining was observed throughout the cytoplasm of theARL4C -positive tumor cells only. The dataset GEPIA, whichcombined TCGA and GTEx, revealed that although the ARL4CmRNA levels in HCC are not statistically higher than those innormal liver, there is trend to higher expression of ARL4CmRNAin HCC compared with normal liver (Supplementary Fig. S1).
Clinicopathologic examination revealed that ARL4C positivityis associated with vascular invasion (P ¼ 0.02; SupplementaryTable S4). Univariate analysis demonstrated that sex, tumornumber > 2, poorly differentiated type, lymph node metastasis,vascular invasion, stage IIIA to IVA, and ARL4C expression wereassociated with inferior relapse-free survival (SupplementaryTable S5). Multivariate analysis showed that tumor number >2is an independent prognostic factor (P ¼ 0.0003). In addition,ARL4C positivity tended to be independently associated withpoor prognosis (P ¼ 0.066; Table 1). Furthermore, relapse-free survival was significantly decreased in patients withARL4C-positive tumors compared with patients with ARL4C-negative tumors (P¼ 0.033; Fig. 1B). Taken together, these resultssuggest that ARL4C expression is correlated with the aggres-siveness of HCC.
In a previous colorectal study (9), the detailed relationshipbetween ARL4C expression and clinicopathologic parameters wasnot examined. In this study, 24.5% of the 102 stage 0 to IIICpatient with colorectal cancer tumors were ARL4C-positive (i.e.,>20% of the tumor cells within the tumor lesions were positive;Supplementary Table S4). The positivity was associated withtumor invasion, vascular invasion, and stage IIA to IIIC (Supple-mentary Table S4). Univariate analysis demonstrated that a tumorinvasion depth beyond the submucosa, vascular invasion, lym-phatic invasion, lymph node metastasis, stage IIA to IIIC, andARL4Cexpression are associatedwith inferior relapse-free survival(Supplementary Table S5). Multivariate analysis showed thatARL4C expression is an independent prognostic factor (P ¼0.0004; Table 1). Relapse-free survival was significantly decreasedin patients positive for ARL4C compared with patients negativefor ARL4C (P<0.0001; Fig. 1C). These results were consistentwithtwo public databases: the GEPIA dataset showed that ARL4CmRNA is expressed at higher levels in colorectal cancer than innormal colon tissue (Supplementary Fig. 1A); the TCGA datasetindicated that the ARL4C high expression groups has a decreasedoverall survival rate compared with the ARL4C low expressiongroups (P ¼ 0.003; Fig. 1D).
Colorectal cancer liver metastasis tumors (24 cases) wereexamined for ARL4C expression by IHC (Fig. 1E). The 24 casesincluded 11 cases of recurrent liver metastasis after colorectalcancer resection (metachronous liver metastasis) and 13 cases ofcolorectal cancer with liver metastasis (synchronous liver metas-tasis). For the metachronous liver metastasis cases, ARL4C wasexpressed in 11 (100%) and 9 (81.8%) cases of colon and livertumor lesions, respectively (Fig. 1E). For the synchronous livermetastasis cases, ARL4C was positive in 11 (84.6%) and 10(76.9%) cases of primary and metastatic tumor lesions,
Harada et al.
Mol Cancer Ther; 18(3) March 2019 Molecular Cancer Therapeutics604
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

respectively (Fig. 1E). In all cases, ARL4C was minimally detectedin nontumor regions. Therefore, ARL4C expression in colorectalcancer was associated with poor prognosis and the expressionfrequency increased in colorectal cancer cases with livermetastasis.
ARL4C ASOs decrease proliferation and migration of HCC andcolorectal cancer cells in vitro
To determine whether ARL4C could be a therapeutic target forthe treatment of liver tumors, ARL4C ASOs were generated andtheir effects on cancer cells were examined. ARL4C sequences,which consisted of 15 nucleotides, were chosen based on thesecondary structure of the ARL4C mRNA (22). Of the thousandsof ARL4C ASO candidates, the sequences that might cause hep-
atotoxicity were excluded, and 38 ARL4C ASO sequences wereselected by high-dimensional structure prediction of the ARL4CmRNA. All of the phosphodiester linkages in theASOs used in thisstudy were replaced by phosphorothioate linkages. Screeningexperiments using real-time PCR were performed to evaluate theknockdown efficiency of 38 ARL4C ASOs using A549 lung cancercells, which were previously used to demonstrate reduced ARL4Cprotein levels in response to ARL4C siRNA treatment (Supple-mentary Fig. S2A; ref. 9). The screeningwasperformed three times,and seven ARL4C ASOs, ASO-650, ASO-793, ASO-986, ASO-1065, ASO-1316, AS-1454, and ASO-3225 were selected forfurther evaluation.
Among the five HCC cell lines, HLE cells expressed the highestARL4C mRNA levels compared with HLF, PLC, and HuH-7 cells,
Figure 1.
ARL4C is expressed in HCC andcolorectal cancer liver metastases.A, HCC tissues (n¼ 128) werestained with an anti-ARL4Cantibody. Black boxes showenlarged images. B and C, Therelationship between relapse-freesurvival and ARL4C expression inpatients with HCC (B) and patientswith colorectal cancer withoutdistant metastases (C; n¼ 102) wasanalyzed.D, TCGA RNA-sequencingand clinical outcome data forcolorectal cancer were retrievedfrom OncoLnc (http://www.oncolnc.org/). High and low ARL4Cexpression groups were classified bythe median value of ARL4Cexpression of patients withcolorectal cancer in the dataset. Thedata were analyzed by Kaplan–Meiersurvival curves, and the log-rank testwas used for statistical analysis. E,Liver metastases of colorectalcancer (n¼ 24) were stained with ananti-ARL4C antibody. Black boxesshow enlarged images. Thepercentages of ARL4C-positivecases in the primary andmetastaticlesions frommetachronous orsynchronous colorectal cancer areshown in the right panel. Scale bars,200 mm (A); 100 mm (E).
ARL4C ASO Inhibits Liver Tumor Growth
www.aacrjournals.org Mol Cancer Ther; 18(3) March 2019 605
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

and HepG2 cells expressed little ARL4C mRNA (SupplementaryFig. S2B). Among the seven ARL4C ASOs, ASO-1316, ASO-1454,and ASO-3225 decreased ARL4C mRNA levels in both HLE andHCT116 cells without cytotoxicity (Fig. 2A). Transfection ofcontrol ASO did not significantly affect the expression of ARL4CmRNAs in HLE cells (Supplementary Fig. S2C). To optimize theeffects of these three ARL4C ASOs, ARL4C ASO-1312, ASO-1450,and ASO-3223 were designed with 19 nucleotides, including theoriginal 15 nucleotides. Among these six candidates, ARL4CASO-1316 and ARL4C ASO-3223 (19-mer including the targetsequence of ARL4C ASO-3225) were selected based on theirstrong downregulation of ARL4C mRNA expression in HLE cellsat low doses (Fig. 2B; Supplementary Fig. S2D).
Four candidate off-target genes for ARL4CASO-1316 and ASO-3223 were found by in silico analysis. These genes were neurolysin(NLN), sapiens F-box and leucine-rich repeat protein 19(FBXL19), keratin-associated protein 15-1 (KRTAP15-1), andsialic acid binding Ig-like lectin 6 (SIGLEC6). KRTAP15-1 andSIGLEC6 were expressed at only low levels in HLE cells (Supple-mentary Table S6). ARL4C ASO-1316 and -3223 did not signif-icantly affect the expression of NLN and FBXL9 mRNAs in HLEcells (Supplementary Fig. S2E). Thus, off-target effects resultingfrom treatment with ARL4C ASOs appear to be unlikely.
Both ARL4C ASO-1316 and ASO-3223 suppressed the migra-tion of HLE cells, which was rescued by the overexpression ofARL4C, excludingoff-target effectsby theARL4CASOs (Fig. 2CandD). ARL4C ASOs also inhibited HLE cell proliferation (Fig. 2E)under the conditions that ASO transfection reagents did not affectcell proliferation (Supplementary Fig. S2F). Inhibition of cellmigration by these ARL4C ASOs was also observed in HCT116cells (Supplementary Fig. S2G; ref. 9). Taken together, these resultssuggest that ARL4C ASOs decreased both the cell proliferation andmigration of ARL4C-expressing cancer cells in vitro.
ARL4C upregulates PIK3CD expression in HCCARL4C is expressed by Wnt/b-catenin and EGF/RAS signaling
and can induce the nuclear localization of YAP/TAZ via cellrelaxation by the appropriate inhibition of RHO signaling (8, 9).Treatment of HLE cells with PD184161, a selective MEK1/2inhibitor, but not by knockdown of b-catenin (a CTNNB1 geneproduct), decreased the expression of ARL4C mRNA, suggestingthat ARL4C is downstream of the MAPK pathway in HLE cells(Fig. 3A; Supplementary Fig. S3A). These findings were consistentwith the correlation analysis data of the TCGA dataset, whichshowed that themRNA expression levels of the target genes of theMAPK pathway (EGR1 and FOS), but not those of Wnt/b-cateninsignaling pathway (AXIN2 and LGR5), are positively correlated
with that of ARL4C in HCC (Supplementary Fig. S3B). Knock-down of ARL4C in A549 cells inhibited the nuclear localization ofYAP, which did not occur in HLE cells (Supplementary Fig. S3C).Therefore, the genes that are expressed downstreamof ARL4C andinvolved in the cell proliferation of HCCmight be different fromthose in lung cancer cells.
The phosphatidylinositol-3-kinase catalytic subunit d isoform(the PIK3CD gene product) is expressed in many cancers, includ-ing HCC (23–26). TCGA dataset analysis revealed that thePIK3CD mRNA expression level, but not that of PIK3CA andPIK3CB, is positively correlated with ARL4C expression in HCC(Fig. 3B; Supplementary Fig. S4A). ARF6 and RAC can act down-stream of ARL4C in colon and lung cancer cells (9). Treatment ofHLE cells with SecinH3 (an inhibitor of ARNO) or NSC23766 (aRAC inhibitor) decreased the PIK3CD mRNA level (Fig. 3C).Overexpression of ARL4C increased the PIK3CD mRNA level inHepG2 cells, and the increment was abrogated by SecinH3 orNSC23766 in HepG2 cells (Fig. 3D), suggesting that ARL4Cupregulates PIK3CD expression through ARF6 and RAC. Consis-tent with these findings, TCGA dataset analysis showed that themRNA expression levels of ARF6 and RAC1, but not ARF1, arepositively correlated with that of PIK3CD in HCC (Supplemen-tary Fig. S4B). PIK3CD knockdown inhibited proliferation andAKT activity in HLE cells (Fig. 3E and F; Supplementary Fig.S4C) under the conditions that siRNA transfection reagents didnot affect cell proliferation (Supplementary Fig. S4D). ARL4CASO-1316 and ASO-3223 decreased PIK3CD mRNA levels andinhibited AKT activity in HLE cells (Fig. 3G and H). In contrast,PIK3CD knockdown did not inhibit HCT116 cell proliferation(Supplementary Fig. S4C and S4E), and ARL4C ASOs did notaffect PIK3CD mRNA levels in HCT116 cells (SupplementaryFig. S4F). These results suggest that PIK3CD is a downstreamtarget of ARL4C in HCC but not colorectal cancer cells and thatARL4C ASOs inhibit cell proliferation by the suppression ofPIK3CD expression in HCC.
ARL4C ASO inhibits tumor growth in the liverThe effects of subcutaneous injection of ARL4C ASO-1316 and
ASO-3223 on liver tumors were examined in two mouse cancermodels: a primary liver tumor model in which HLE cells weretransplanted directly in the liver and a metastatic tumor model inwhich HCT116 cells were transplanted in the spleen and thenmetastasized to the liver.
HLE cells were injected into the liver, and mice were subcuta-neously injectedwith control ASOand twoARL4CASOs (Fig. 4A).ARL4C ASO-1316 suppressed HLE tumor formation and reducedtumor weight in a dose-dependent manner compared with
Table 1. Multivariate analysis of relapse-free survival of HCC and CRC (stage 0–IIIC) cases by Cox's proportional hazard model
HCC Parameters Number HR (95% CI) P value
Sex (male/female) 114/14 0.54 (0.28–1.12) 0.093Tumor number (>2/1) 55/73 2.37 (1.50–3.79) 0.0003Histology (poor/well or moderate) 31/96 1.57 (0.93–2.59) 0.09ARL4C expression (positive/negative) 33/95 1.62 (0.97–2.66) 0.066
CRC Parameters Number HR (95% CI) P valueLymphatic invasion (positive/negative) 60/41 3.29 (0.94–15.17) 0.063Lymph node metastasis (positive/negative) 34/68 1.93 (0.80–4.96) 0.14ARL4C expression (positive/negative) 25/77 4.51 (1.98–10.61) 0.0004
NOTE: Multivariate analysis was performed using covariates of which P value was under 0.05 in univariate analysis (Supplementary Table S2), and covariatesassociating with the expression of ARL4C (Supplementary Table S1) were excluded to avoid the multicollinearity. Child pugh score and lymph nodemetastasis wereexcluded from multivariate analysis because of small number of events.Abbreviations: CI, confidence interval; CRC, colorectal cancer.
Harada et al.
Mol Cancer Ther; 18(3) March 2019 Molecular Cancer Therapeutics606
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

control ASO (Fig. 4A). ARL4C ASO-1316 also inhibited ARL4Cand PIK3CD expression in the liver tumors and decreased thenumber of Ki-67-positive cells (Fig. 4B). ARL4C ASO-1316 didnot induce any histological damages or cell death in the non-tumor regions of the liver (Supplementary Fig. S5A). In contrast,ARL4C ASO-3223 (50 mg/body) did not significantly inhibit HLEtumor formation (Fig. 4A), the expression of ARL4C and PIK3CD,
or the numbers of Ki-67-positive cells (Fig. 4B) despite beingeffective in vitro (see Fig. 2).
Subcutaneous injection of 6-FAM-labeled ARL4C ASO-1316into nontumor bearing mice showed that the ASO is specificallydelivered to the liver compared with other organs, although itsincorporation was found to be weak by the assessment of thefluorescence intensity (Supplementary Fig. S5B). However, when
Figure 2.
ARL4C ASOs reduce ARL4C expression and inhibit cancer cell migration and proliferation in vitro. A, HLE or HCT116 cells were transfected with 25 nmol/L controlor ARL4C ASOs. ARL4CmRNA levels were determined by real-time PCR. The data are expressed as the fold-change of the ARL4CmRNA levels compared withthe control ASO. B, HLE cells were transfected with control or ARL4C ASOs at the indicated concentration, and the ARL4CmRNA levels were examined. C, HLEcells stably expressing GFP (HLE/GFP cells) or ARL4C-GFP (HLE/ARL4C-GFP cells) were treated with control ASO, ARL4C ASO-1316, or ARL4C ASO-3223 andthen subjected to the migration assay. Migration activity is expressed as the percentage of the GFP-expressing control cells. D, Lysates from HLE/GFP or HLE/ARL4C-GFP cells were probed with anti-ARL4C and anti-Hsp90 antibodies. Hsp90 was used as a loading control. E, HLE cells were treated with control ASO,ARL4C ASO-1316, or ARL4C ASO-3223 and then subjected to the proliferation assay. AU, arbitrary unit. The data are presented as the mean� SD of threeindependent experiments. � , P < 0.05. Scale bar, 100 mm (C).
ARL4C ASO Inhibits Liver Tumor Growth
www.aacrjournals.org Mol Cancer Ther; 18(3) March 2019 607
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

Figure 3.
ARL4C and PIK3CD expression levels are correlated in HCC. A, The ARL4CmRNA levels in HLE cells treated with 10 mmol/L PD184161 or transfected with10 nmol/L CTNNB1 siRNA were examined by real-time PCR. The data are expressed as the fold-change compared with the untreated control cells. B, Scatter plotshowing the correlation between the expression of ARL4C (X-axis) and PIK3CD (Y-axis) mRNAs obtained from the TCGA dataset (n¼ 371) using the R2:Genomics Analysis and Visualization Platform. The solid black line indicates the linear fit; r indicates the Pearson's correlation coefficient. C, The PIK3CDmRNAlevels in HLE cells treated with 25 mmol/L SecinH3 or 50 mmol/L NSC23766 were examined by real-time PCR. The data are expressed as the fold-changecompared with the control cells treated with DMSO. D, The PIK3CDmRNA levels in HepG2 cells expressing ARL4C treated with 25 mmol/L SecinH3 or 50 mmol/LNSC23766 were examined. The data are expressed as the fold-change compared with control cells transfected with empty vector and treated with DMSO. E andF, HLE cells were transfected with 20 nmol/L control or PIK3CD siRNA. HLE cells treated with the indicated siRNAs were subjected to the proliferation assay (E).HLE cell lysates were probed with anti-phosphorylated AKT (pAKT S473) and anti-AKT antibodies (F). The band intensities are shown as the arbitrary units in thebottom (F). G and H, HLE cells were treated with 25 nmol/L control or ARL4C ASOs. Real-time PCR analyses for PIK3CDmRNAwere performed (G). Lysates fromHLE cells were probed with anti-pAKT S473 and anti-AKT antibodies (H). The data are expressed as the fold-change compared with control cells transfected withcontrol ASO. AU, arbitrary unit. The data are presented as the mean� SD of three independent experiments. � , P < 0.05.
Harada et al.
Mol Cancer Ther; 18(3) March 2019 Molecular Cancer Therapeutics608
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

Figure 4.
ARL4C ASO inhibits HCC tumor formation. A, HLE cells (1.0� 107 cells) were implanted with Matrigel into the livers of nude mice on day 0. Starting on day 0, 50mg of control ASO (n¼ 10), ARL4C ASO-1316 (n¼ 8), and ARL4C ASO-3223 (n¼ 7) or 100 mg of control ASO (n¼ 6) and ARL4C ASO-1316 (n¼ 6) wereadministered subcutaneously twice a week. The mice were euthanized on day 29. Representative images of the liver tumors are shown (left). Tumor weightswere measured (right graphs). The data are plotted as box and whiskers where the median is represented by the line, the box represents the 25th to 75thpercentile, and the error bars show the 5th to 95th percentile. The white arrows indicate the positions of the tumors. � , P < 0.05. B, Sections from HLE liver tumorswere stained with anti-ARL4C, anti-PIK3CD, or anti-Ki-67 antibody. Ki-67-positive cells were counted, and the data are expressed as the percentage of positivelystained cells compared with the total number of cells. C, Four hours after subcutaneous injection of 6-FAM-ARL4C ASO-1316 into HLE tumor-bearing mice, thefluorescence intensity of various organs was measured. Br, brain; Lu, lung; He, heart; T, tumor lesion; Li, liver; Ki, kidney; Sp, spleen; Co, colon.D, Sections wereprepared from the tumor lesion of the liver from an ASO-treated mouse and stained with rhodamine phalloidin and Hoechst 33342 to show F-actin and thenucleus, respectively. N, nontumor region; T, tumor lesion. Bottom, enlarged images of the top images. The white arrowheads indicate the nuclei of HLE cells. Thedata are presented as the mean� SD of three independent experiments. � , P < 0.05. Scale bars, 10 mm (A); 100 mm (B); 200 mm (D, top); 10 mm (D, bottom).
ARL4C ASO Inhibits Liver Tumor Growth
www.aacrjournals.org Mol Cancer Ther; 18(3) March 2019 609
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

6-FAM-labeled ARL4C ASO-1316 was injected into HLE tumor-bearingmice, the ASOhighly accumulated in tumor lesions of theliver (Fig. 4C). Confocal imaging revealed that the ASO accumu-lated in nuclear punctate sites of tumor cells or hepatocytes(Fig. 4D; Supplementary Fig. S5C).
For the metastatic liver tumor model, HCT116/Luc cells wereinjected into the spleen, and the luminescence signal was detectedin the liver starting on day 19 (Fig. 5A). Control ASO and ARL4CASO-1316 and ASO-3223 were subcutaneously injected begin-ning on day 19, and the effect of treatment on tumor formationwas followed by biweekly bioluminescence measurements
(Fig. 5A and B). By day 47, ARL4C ASO-1316 suppressed thegrowth ofHCT116 livermetastasis (Fig. 5A). In the liver tumors ofthe ARL4C ASO-1316-treated mice, ARL4C expression and thenumber of Ki-67-positive cells were reduced (Fig. 5B and C). Incontrast, ARL4C ASO-3223 did not exhibit any antitumor activity(Fig. 5).
DiscussionIn this study, we examined whether ARL4C is involved in the
proliferation of cancer cells in the liver and if ARL4C ASO could
Figure 5.
ARL4C ASO inhibits metastatictumor formation by colorectalcancer cells in the liver. A, HCT116/Luc cells (2.5� 105 cells) wereimplanted into the spleen of nudemice. On day 19, luminescence wasvisible in the liver. Starting on day19, 50 mg of control ASO (n¼ 9),ARL4C ASO-1316 (n¼ 9), orARL4C ASO-3223 (n¼ 7) wereadministered subcutaneouslytwice per week until euthanasia onday 47. Representativebioluminescence images of theliver tumors taken on days 19, 35,and 47 are presented.Quantification of the tumorburden in the liver was performedusing IVIS/Kodak software (right).The data are presented asthe mean� SD of thebioluminescence intensity.B, Representative images of themetastatic HCT116 liver tumorstreated with ARL4C ASOs areshown.White arrowheads indicatethe positions of the tumors.Sections were prepared from thetumors and stained with anti-ARL4C antibody. C, The samesamples in (B) were stainedwith anti-Ki-67 antibody, andthe Ki-67-positive cells werecounted. The resultsare the mean� SD of threeindependent experiments andexpressed as the percentage ofpositively stained cells comparedwith the total number of cells.�, P < 0.05. Scale bars, 10 mm(B, top); 100 mm (B, bottom);50 mm (C).
Harada et al.
Mol Cancer Ther; 18(3) March 2019 Molecular Cancer Therapeutics610
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

represent a novel treatment for HCC and metastatic liver cancer.The key findings were: (i) ARL4C is a prognostic factor for HCCand colorectal cancer; (ii) ARL4C upregulated PIK3CD in HCC;and (iii) ARL4C ASO inhibited liver tumor formation in twoindependent mouse models.
ARL4C function in liver tumorsARL4C expression in HCC was correlated with vascular
invasion and inversely associated with relapse-free survival.Consistent with these findings, cell biology studies revealedthat ARL4C is involved in proliferation and migration of HCCcells. Thus, ARL4C expression may be associated with theaggressiveness of HCC. In colon, lung, and tongue cancer cells,ARL4C modulates actomyosin through the regulation of ARF6,RAC, and RHO, which results in the nuclear localization ofYAP/TAZ and cellular proliferation (8–10). Thus, the ARNO–
ARF6 pathway is a direct downstream signaling target of ARL4Cto regulate YAP/TAZ-dependent cancer cell proliferation (5).However, ARL4C did not affect YAP/TAZ subcellular localiza-tion in HCC cells but was involved in the expression ofPIK3CD, which is expressed in many cancers, including HCC,colorectal cancer, breast cancer, glioblastoma, and multiplemyeloma (23–26). In these cancers, PIK3CD is a therapeutictarget, and a selective PIK3CD inhibitor and microRNA-7,which targets PIK3CD, exhibit antitumor activity. The under-lying mechanism by which ARL4C induces PIK3CD expressionin HCC cells remains to be clarified although ARF6 and RAC arelikely to be involved in this process. Thus, ARL4C may activatemultiple downstream signaling pathways in a cancer cell-con-text manner.
ARL4C was expressed in 24.5% of colorectal cancer caseswithout distant metastasis. The frequency increased to 95% ofthe primary lesions in colorectal cancer with liver metastasis,and more than 80% of the metastatic liver lesions were positivefor ARL4C in these cases. Because ARL4C can stimulate migra-tion and invasion of colorectal cancer cells, it is thoughtthat liver metastasis occurs with high frequency in colorectalcancer expressing ARL4C. Indeed, the relapse-free survival waspoor in patients with colorectal cancer that were positive forARL4C. These results were supported by public databases.Taken together with the observations that ARL4C expressionin gastric cancer is associated with the depth of invasion,peritoneal dissemination, and poor prognosis (27), ARL4Cexpression may be a molecular marker for the prognosis ofthese cancers.
ARL4C ASO is a potential therapeutic for liver tumorsBecause knockdown or knockout of ARL4C inhibits the pro-
liferation of cancer cells (9, 10), ARL4C represents a potentialnovel target for cancer therapy. ARL4C is an intracellular proteinthat mediates a signal through protein–protein interactions (5).Therefore, one strategy for targeting ARL4C is the use of nucleicacids rather than low molecular compounds or antibodies.Oligonucleotide-based drugs are promising therapeutics in thatthey can be designed rapidly and rationally against virtually anygenetic target (15). The delivery and potency of the drugs arederived from the chemical structure of the oligonucleotidewhereas their target is decided by the nucleic acid sequence. Wedesigned and synthesized chemically modified ASOs, whichwere flanked by AmNA with a phosphorothioate backbone.
This type of ASO was shown to be stable in the blood andhighly incorporated into liver cells in vivo (16). Although LNAshave been associated with liver toxicity (28), the AmNA-ASOsinhibit targetmRNA expression in vivo and exhibit less toxicity tothe liver (29, 30).
From the thousands of candidate ARL4C ASOs, two ARL4CASOs, which showed the highest suppression of ARL4C expres-sion and inhibition of HCC and colorectal cancer proliferationin vitro, were selected for in vivo testing using mouse models ofprimary HCC and colorectal cancer liver metastasis. ARL4C ASO-1316, but not ARL4C ASO-3223, decreased the expression ofARL4C and inhibited tumor growth in both models. The resultsdemonstrate that the in vitro effects of ASOs do not always reflectthe in vivo effects probably due to differences in incorporationefficiency and inhibition of mRNA synthesis in intact cells in vivo.Themechanismsof cellular uptake, trafficking, anddistribution ofASOs and the proteins that bind and regulate ASOs remain to beclarified (13). Although it has been reported that ASO lengthmayplay a role in dystrophin exon skipping (31), at present it isnecessary to test the in vivo effects of all synthesized ASOs that areeffective in vitro.
ARL4C ASO-1316 specifically accumulated in the nuclei ofliver tumor cells and was indeed effective for liver tumors at lowdoses (twice per week with approximately 2.5 mg/kg) whencompared with doses shown in previous reports (e.g., 50 mg/kgMsi-2 ASO given daily for pancreatic cancer; 20 mg/kg Stat3ASO given daily for lymphoangiogenesis; refs. 32, 33). Histo-logic damage to the nontumor regions of the liver was notobserved following the administration of ARL4C ASO-1316.Because ARL4C-positive primary HCC is about 26% of totalHCC cases that we examined, the therapy using ARL4C ASOfor primary HCC may be limited. Nonetheless, it is expectedthat ARL4C ASO-1316 is appropriate for clinical use withoutside effects.
In conclusion, ARL4C is involved in liver cancer cell prolifer-ation through PIK3CD expression and ARL4C ASO represents thenovel treatment for primary and metastatic liver cancers.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: S. Matsumoto, A. KikuchiDevelopment of methodology: S. Matsumoto, S. Obika, A. KikuchiAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): T. Harada, S. Matsumoto, S. Hirota, S. Fujii,Y. Kasahara, H. Gon, T. Yoshida, N. Haraguchi, T. Mizushima, T. Noda,H. Eguchi, E. Morii, T. FukumotoAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S. Matsumoto, H. Kimura, Y. Kasahara, H. Gon,E. Morii, S. ObikaWriting, review, and/or revision of the manuscript: T. Harada, H. Kimura,T. Fukumoto, A. KikuchiAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): S. Hirota, T. Itoh, T. Noda, S. Nojima, A. KikuchiStudy supervision: T. Mizushima, A. Kikuchi
AcknowledgmentsThe authors would like to thank to Dr. Sae Murakami at Division of Clinical
and Translational Research Center, Kobe University Hospital, for helpingstatistical analyses. The authors also thank Drs. T. Kobayashi and A. Shintanifor donating cells. This work was supported by Grants-in-Aid for ScientificResearch to A. Kikuchi (2016-2020; No. 16H06374) and for Scientific Research
ARL4C ASO Inhibits Liver Tumor Growth
www.aacrjournals.org Mol Cancer Ther; 18(3) March 2019 611
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

on Innovative Areas "Integrated analysis and regulation of cellular diversity" toA. Kikuchi (2018-2019; No. 18H05101) from the Ministry of Education,Culture, Sports, Science and Technology of Japan; by the Project PromotingSupport for Drug Discovery to A. Kikuchi (2015-2018; No. DNW-15005) fromthe Japan Agency for Medical Research and Development, AMED, by IntegratedFrontier Research for Medical Science Division, Institute for Open and Trans-disciplinary Research Initiatives, Osaka University to A. Kikuchi; and by grantsfrom the Yasuda Memorial Foundation to A. Kikuchi.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received July 26, 2018; revised October 26, 2018; accepted January 10, 2019;published first January 15, 2019.
References1. Attwa MH, El-Etreby SA. Guide for diagnosis and treatment of hepatocel-
lular carcinoma. World J Hepatol 2015;7:1632–51.2. Llovet JM, Ricci S,Mazzaferro V,Hilgard P, Gane E, Blanc JF, et al. Sorafenib
in advanced hepatocellular carcinoma. N Engl J Med 2008;359:378–90.3. Sakisaka M, Haruta M, Komohara Y, Umemoto S, Matsumura K, Ikeda T,
et al. Therapy of primary and metastatic liver cancer by human iPS cell-derived myeloid cells producing interferon-b. J Hepatobiliary Pancreat Sci2017;24:109–19.
4. Steele G Jr, Ravikumar TS. Resection of hepatic metastases from colorectalcancer. Biologic perspective. Ann Surg 1989;210:127–38.
5. Matsumoto S, Fujii S, Kikuchi A. Arl4c is a key regulator of tubulogenesisand tumourigenesis as a target geneofWnt-b-catenin andgrowth factor-Rassignalling. J Biochem 2017;161:27–35.
6. D'Souza-SchoreyC,Chavrier P. ARFproteins: roles inmembrane traffic andbeyond. Nat Rev Mol Cell Biol 2006;7:347–58.
7. Burd CG, Strochlic TI, Gangi Setty SR. Arf-like GTPases: not so Arf-like afterall. Trends Cell Biol 2004;14:687–94.
8. Matsumoto S, Fujii S, Sato A, Ibuka S, Kagawa Y, Ishii M, et al. Acombination of Wnt and growth factor signaling induces Arl4c expressionto form epithelial tubular structures. EMBO J 2014;33:702–18.
9. Fujii S, Matsumoto S, Nojima S, Morii E, Kikuchi A. Arl4c expression incolorectal and lung cancers promotes tumorigenesis and may represent anovel therapeutic target. Oncogene 2015;34:4834–44.
10. Fujii S, Shinjo K,Matsumoto S, Harada T, Nojima S, Sato S, et al. Epigeneticupregulation of ARL4C, due to DNA hypomethylation in the 30-untrans-lated region, promotes tumorigenesis of lung squamous cell carcinoma.Oncotarget 2016;7:81571–87.
11. Chi X, Gatti P, Papoian T. Safety of antisense oligonucleotide and siRNA-based therapeutics. Drug Discov Today 2017;22:823–33.
12. Farooqi AA, Rehman ZU, Muntane J. Antisense therapeutics in oncology:current status. Onco Targets Ther 2014;7:2035–42.
13. Crooke ST, Wang S, Vickers TA, Shen W, Liang XH. Cellular uptake andtrafficking of antisense oligonucleotides. Nat Biotechnol 2017;35:230–7.
14. Stein CA, Castanotto D. FDA-approved oligonucleotide therapies in 2017.Mol Ther 2017;25:1069–75.
15. Khvorova A,Watts JK. The chemical evolution of oligonucleotide therapiesof clinical utility. Nat Biotechnol 2017;35:238–48.
16. Yahara A, Shrestha AR, Yamamoto T, Hari Y, Osawa T, Yamaguchi M, et al.Amido-bridged nucleic acids (AmNAs): synthesis, duplex stability, nucle-ase resistance, and in vitro antisense potency. Chembiochem 2012;13:2513–6.
17. Zanardi TA, Han SC, Jeong EJ, Rime S, Yu RZ, Chakravarty K, et al.Pharmacodynamics and subchronic toxicity in mice and monkeys ofISIS 388626, a second-generation antisense oligonucleotide that targetshuman sodium glucose cotransporter 2. J Pharmacol Exp Ther 2012;343:489–96.
18. Klein PJ, Schmidt CM, Wiesenauer CA, Choi JN, Gage EA, Yip-Schnei-der MT, et al. The effects of a novel MEK inhibitor PD184161 on MEK-ERK signaling and growth in human liver cancer. Neoplasia 2006;8:1–8.
19. Hafner M, Schmitz A, Grune I, Srivatsan SG, Paul B, Kolanus W, et al.Inhibition of cytohesins by SecinH3 leads to hepatic insulin resistance.Nature 2006;444:941–4.
20. Gao Y, Dickerson JB, Guo F, Zheng J, Zheng Y. Rational design andcharacterization of a Rac GTPase-specific small molecule inhibitor.Proc Natl Acad Sci USA 2004;101:7618–23.
21. Yamamoto T, Yahara A, Waki R, Yasuhara H, Wada F, Harada-Shiba M,et al. Amido-bridged nucleic acids with small hydrophobic residuesenhance hepatic tropism of antisense oligonucleotides in vivo.Org Biomol Chem 2015;13:3757–65.
22. Zuker M. Mfold web server for nucleic acid folding and hybridizationprediction. Nucleic Acids Res 2003;31:3406–15.
23. IkedaH,Hideshima T, FulcinitiM, PerroneG,MiuraN, YasuiH, et al. PI3K/p110d is a novel therapeutic target inmultiple myeloma. Blood 2010;116:1460–8.
24. Fang Y, Xue JL, Shen Q, Chen J, Tian L. MicroRNA-7 inhibits tumor growthandmetastasis by targeting the phosphoinositide 3-kinase/Akt pathway inhepatocellular carcinoma. Hepatology 2012;55:1852–62.
25. Chen JS, Zhou LJ, Entin-Meer M, Yang X, Donker M, Knight ZA, et al.Characterization of structurally distinct, isoform-selective phosphoinosi-tide 30-kinase inhibitors in combination with radiation in the treatment ofglioblastoma. Mol Cancer Ther 2008;7:841–50.
26. Sawyer C, Sturge J, Bennett DC, O'Hare MJ, Allen WE, Bain J, et al.Regulation of breast cancer cell chemotaxis by the phosphoinositide3-kinase p110d. Cancer Res 2003;63:1667–75.
27. Hu Q, Masuda T, Sato K, Tobo T, Nambara S, Kidogami S, et al. Identi-fication of ARL4C as a peritoneal dissemination-associated gene and itsclinical significance in gastric cancer. Ann Surg Oncol 2018;25:745–53.
28. Swayze EE, Siwkowski AM, Wancewicz EV, Migawa MT, Wyrzykiewicz TK,Hung G, et al. Antisense oligonucleotides containing locked nucleic acidimprove potency but cause significant hepatotoxicity in animals.Nucleic Acids Res 2007;35:687–700.
29. Shinkai K, Nakano K, Cui L, Mizuuchi Y, Onishi H, Oda Y, et al. Nuclearexpression of Y-box binding protein-1 is associated with poor prognosis inpatients with pancreatic cancer and its knockdown inhibits tumor growthand metastasis in mice tumor models. Int J Cancer 2016;139:433–45.
30. Cui L, Nakano K, Obchoei S, Setoguchi K, Matsumoto M, Yamamoto T,et al. Small nucleolar noncoding RNA SNORA23, up-regulated in humanpancreatic ductal adenocarcinoma, regulates expression of spectrin repeat-containing nuclear envelope 2 to promote growth and metastasis ofxenograft tumors in mice. Gastroenterology 2017;153:292–306.e2.
31. Harding PL, Fall AM, Honeyman K, Fletcher S, Wilton SD. The influence ofantisense oligonucleotide length on dystrophin exon skipping. Mol Ther2007;15:157–66.
32. Fox RG, Lytle NK, Jaquish DV, Park FD, Ito T, Bajaj J, et al. Image-baseddetection and targeting of therapy resistance in pancreatic adenocarcino-ma. Nature 2016;534:407–11.
33. Chiarle R, Simmons WJ, Cai H, Dhall G, Zamo A, Raz R, et al. Stat3 isrequired for ALK-mediated lymphomagenesis and provides a possibletherapeutic target. Nat Med 2005;11:623–9.
Mol Cancer Ther; 18(3) March 2019 Molecular Cancer Therapeutics612
Harada et al.
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824

2019;18:602-612. Published OnlineFirst January 15, 2019.Mol Cancer Ther Takeshi Harada, Shinji Matsumoto, Suguru Hirota, et al. Inhibits Primary and Metastatic Liver Tumor GrowthChemically Modified Antisense Oligonucleotide Against ARL4C
Updated version
10.1158/1535-7163.MCT-18-0824doi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2019/01/15/1535-7163.MCT-18-0824.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/18/3/602.full#ref-list-1
This article cites 33 articles, 6 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/18/3/602To request permission to re-use all or part of this article, use this link
on September 20, 2020. © 2019 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst January 15, 2019; DOI: 10.1158/1535-7163.MCT-18-0824