
Characterization of an Adult Mock Circulation for.8 2
10
Characterization of an Adult Mock Circulation for Testing Cardiac Support Devices GEORGE M. PANTALOS,* STEVEN C. KOENIG,* KEVIN J. GILLARS,* GURUPRASAD A. GIRIDHARAN,* AND DAN L. EWERT† A need exists for a mock circulation that behaves in a phys- iologic manner for testing cardiac devices in normal and pathologic states. To address this need, an integrated mock cardiovascular system consisting of an atrium, ventricle, and systemic and coronary vasculature was developed specifically for testing ventricular assist devices (VADs). This test config- uration enables atrial or ventricular apex inflow and aortic outflow cannulation connections. The objective of this study was to assess the ability of the mock ventricle to mimic the Frank–Starling response of normal, heart failure, and cardiac recovery conditions. The pressure–volume relationship of the mock ventricle was evaluated by varying ventricular volume over a wide range via atrial (preload) and aortic (afterload) occlusions. The input impedance of the mock vasculature was calculated using aortic pressure and flow measurements and also was used to estimate resistance, compliance, and inertial mechanical properties of the circulatory system. Results dem- onstrated that the mock ventricle pressure–volume loops and the end diastolic and end systolic pressure–volume relation- ships are representative of the Starling characteristics of the natural heart for each of the test conditions. The mock vas- culature can be configured to mimic the input impedance and mechanical properties of native vasculature in the normal state. Although mock circulation testing systems cannot re- place in vivo models, this configuration should be well suited for developing experimental protocols, testing device feed- back control algorithms, investigating flow profiles, and train- ing surgical staff on the operational procedures of cardiovas- cular devices. ASAIO Journal 2004; 50:37–46. M ock circulation systems have been used extensively for in vitro performance testing of cardiovascular devices. Although mock circulatory systems cannot replace animal and clinical trials, they form an essential and important step in the design and validation of cardiac devices. The earliest mock circula- tory systems were pulse duplicators driven by stepping motors and linear actuators 1–4 and were primarily used for testing heart valves. Mock circulation systems have been used for hemodynamic, hydrodynamic, and hemolysis studies of pros- thetic vessels and cardiac assist devices. 5–10 Several physical models of the circulation have been developed to simulate and match important physiologic parameters. 11–16 Elaborate con- trol schemes have been developed to mimic the physiologic behavior 17–19 of the cardiovascular system. Recently, Ferrari et al. developed a hybrid, numerical–physical model of the cir- culatory system with an electrohydraulic interface to over- come the lack of flexibility in using a purely physical mock circulatory system. 18 –19 Mock vasculatures, such as the Pennsylvania State Univer- sity mock circulation, 20 have been used primarily to test, de- sign, and validate the pumping performance of ventricular assist devices (VADs) and artificial hearts. To gain insight into VAD and other cardiac device responses to a wide range of operating conditions, a mock ventricle that responds to varying preload, afterload, heart rates, and clinical conditions (normal, failing, and recovering heart) that mimic Frank–Starling behav- ior is needed. It is also essential for a mock circulatory system to mimic the native cardiovascular system, particularly to changes in volume as well as a mock vasculature that can produce physiologically equivalent vascular input impedance. Additionally, it is desirable to be able to approximate the surgical cannulation by having ventricular, atrial, and aortic cannulation access sites for testing of different VAD designs. An in vitro circulatory system was developed to produce phys- iologically equivalent pressures, volumes, and flows for testing VADs. The objective of this study was to evaluate the ability of the mock circulation to faithfully reproduce normal, heart failure, and partial cardiac recovery physiologic states as a platform for testing circulatory support devices. Methods Experimental Design The objective of this study was to assess the ability of the mock circulation to mimic the Frank–Starling response of the natural heart and vasculature in normal, heart failure, and partial cardiac recovery states. The pressure–volume relation- ship, determined by varying ventricular volume over a wide range via atrial (preload) and aortic (afterload) occlusions, was used to evaluate the response of the mock ventricle. The mock vasculature was characterized using input impedance derived from aortic pressure and flow measurements, as well as esti- mates of vascular resistance, compliance, and inertial properties. The mock ventricle was configured to mimic native normal, Presented at the 2nd Joint EMBS-BMES Conference, October 23–26, 2002, Houston, Texas. From the *Jewish Hospital Heart and Lung Institute, Department of Surgery, University of Louisville, Kentucky; and †Department of Elec- trical and Computer Engineering, North Dakota State University, Fargo. Submitted for consideration March 2003; accepted for publication in revised form August 2003. Correspondence: George M. Pantalos, Ph.D., Jewish Hospital Cardiothoracic Surgical Research Institute, at the University of Louisville, 500 South Floyd Street, Room 102, Department of Surgery, University of Louisville, Louisville, KY 40202; E-mail [email protected]. DOI: 10.1097/01.MAT.0000104818.70726.E6 ASAIO Journal 2004 37
Transcript of Characterization of an Adult Mock Circulation for.8 2

Characterization of an Adult Mock Circulation for TestingCardiac Support Devices
GEORGE M. PANTALOS,* STEVEN C. KOENIG,* KEVIN J. GILLARS,* GURUPRASAD A. GIRIDHARAN,* AND DAN L. EWERT†
A need exists for a mock circulation that behaves in a phys-iologic manner for testing cardiac devices in normal andpathologic states. To address this need, an integrated mockcardiovascular system consisting of an atrium, ventricle, andsystemic and coronary vasculature was developed specificallyfor testing ventricular assist devices (VADs). This test config-uration enables atrial or ventricular apex inflow and aorticoutflow cannulation connections. The objective of this studywas to assess the ability of the mock ventricle to mimic theFrank–Starling response of normal, heart failure, and cardiacrecovery conditions. The pressure–volume relationship of themock ventricle was evaluated by varying ventricular volumeover a wide range via atrial (preload) and aortic (afterload)occlusions. The input impedance of the mock vasculature wascalculated using aortic pressure and flow measurements andalso was used to estimate resistance, compliance, and inertialmechanical properties of the circulatory system. Results dem-onstrated that the mock ventricle pressure–volume loops andthe end diastolic and end systolic pressure–volume relation-ships are representative of the Starling characteristics of thenatural heart for each of the test conditions. The mock vas-culature can be configured to mimic the input impedance andmechanical properties of native vasculature in the normalstate. Although mock circulation testing systems cannot re-place in vivo models, this configuration should be well suitedfor developing experimental protocols, testing device feed-back control algorithms, investigating flow profiles, and train-ing surgical staff on the operational procedures of cardiovas-cular devices. ASAIO Journal 2004; 50:37–46.
Mock circulation systems have been used extensively for invitro performance testing of cardiovascular devices. Althoughmock circulatory systems cannot replace animal and clinicaltrials, they form an essential and important step in the designand validation of cardiac devices. The earliest mock circula-tory systems were pulse duplicators driven by stepping motors
and linear actuators1–4 and were primarily used for testingheart valves. Mock circulation systems have been used forhemodynamic, hydrodynamic, and hemolysis studies of pros-thetic vessels and cardiac assist devices.5–10 Several physicalmodels of the circulation have been developed to simulate andmatch important physiologic parameters.11–16 Elaborate con-trol schemes have been developed to mimic the physiologicbehavior17–19 of the cardiovascular system. Recently, Ferrari etal. developed a hybrid, numerical–physical model of the cir-culatory system with an electrohydraulic interface to over-come the lack of flexibility in using a purely physical mockcirculatory system.18–19
Mock vasculatures, such as the Pennsylvania State Univer-sity mock circulation,20 have been used primarily to test, de-sign, and validate the pumping performance of ventricularassist devices (VADs) and artificial hearts. To gain insight intoVAD and other cardiac device responses to a wide range ofoperating conditions, a mock ventricle that responds to varyingpreload, afterload, heart rates, and clinical conditions (normal,failing, and recovering heart) that mimic Frank–Starling behav-ior is needed. It is also essential for a mock circulatory systemto mimic the native cardiovascular system, particularly tochanges in volume as well as a mock vasculature that canproduce physiologically equivalent vascular input impedance.Additionally, it is desirable to be able to approximate thesurgical cannulation by having ventricular, atrial, and aorticcannulation access sites for testing of different VAD designs.An in vitro circulatory system was developed to produce phys-iologically equivalent pressures, volumes, and flows for testingVADs. The objective of this study was to evaluate the ability ofthe mock circulation to faithfully reproduce normal, heartfailure, and partial cardiac recovery physiologic states as aplatform for testing circulatory support devices.
Methods
Experimental Design
The objective of this study was to assess the ability of themock circulation to mimic the Frank–Starling response of thenatural heart and vasculature in normal, heart failure, andpartial cardiac recovery states. The pressure–volume relation-ship, determined by varying ventricular volume over a widerange via atrial (preload) and aortic (afterload) occlusions, wasused to evaluate the response of the mock ventricle. The mockvasculature was characterized using input impedance derivedfrom aortic pressure and flow measurements, as well as esti-mates of vascular resistance, compliance, and inertialproperties.
The mock ventricle was configured to mimic native normal,
Presented at the 2nd Joint EMBS-BMES Conference, October 23–26,2002, Houston, Texas.
From the *Jewish Hospital Heart and Lung Institute, Department ofSurgery, University of Louisville, Kentucky; and †Department of Elec-trical and Computer Engineering, North Dakota State University,Fargo.
Submitted for consideration March 2003; accepted for publicationin revised form August 2003.
Correspondence: George M. Pantalos, Ph.D., Jewish HospitalCardiothoracic Surgical Research Institute, at the University ofLouisville, 500 South Floyd Street, Room 102, Department ofSurgery, University of Louisville, Louisville, KY 40202; [email protected].
DOI: 10.1097/01.MAT.0000104818.70726.E6
ASAIO Journal 2004
37

failing heart, and partial cardiac recovery test conditions, asdefined in Table 1. The fraction of the cardiac cycle for systolicduration of the mock ventricle was set to 37% for all testconditions. Heart rate (HR) was randomly selected at 80, 100,and 120 beats per minute (bpm) for each test condition. First,30 seconds of baseline hemodynamic measurements werecontinuously recorded for the normal state at a randomlyselected HR. Second, hemodynamic measurements were con-tinuously recorded while gradually reducing preload by oc-cluding atrial inflow with a turn style resistor clamp up to atrialcollapse and during return to baseline. Third, hemodynamicmeasurements were again continuously recorded while theafterload was gradually increased by occluding the aortic out-flow with a turn style resistor clamp up to total occlusion andfollowing release with return to baseline. The sequence of (1)baseline, (2) reducing preload (via atrial inflow occlusion), and(3) increasing afterload (via aortic outflow occlusion) at each ofthe three randomly selected HR in the normal state was re-peated for failing heart and partial cardiac recovery test con-ditions. Characterizing hemodynamic parameter values andventricular pressure–volume relationships were derived foreach test condition and compared with published humanphysiologic data.21,22
The mock vasculature and mock ventricle were appropri-ately adjusted (e.g., driveline pressure, peripheral resistance) tomimic normal21 and heart failure (elevated input impedance)22
test conditions. Thirty seconds of hemodynamic measurementswere continuously recorded in the normal and elevated after-load states. The vascular input impedance and vascular me-chanical properties (resistance, compliance, and inertance)were derived for each test condition and compared with hu-man physiologic data.
Mock Circulation
The mock circulation system consists of atrium, ventricle,and systemic and coronary vasculature components (Figures 1and 2). The artificial atrium20 is made of a flexible polyure-thane sphere 50 mm in diameter and is connected upstream ofthe inflow valve of the mock ventricle. The mock ventricleconsists of a flexing, segmented polyurethane sac inside apressurization chamber.23 The ventricular sac is hemiellipsoidshaped and is 70 mm across at the base and 83 mm long frombase to apex. The base is covered by a semirigid polymerdome 20 mm high with mounts for inflow (mitral) and outflow(aortic) prosthetic valves. For this particular set of experimentalconditions, custom made rigid mounted trileaflet polyurethanevalves24 were used so that a pressure–volume catheter could
be passed retrograde through the outflow valve into the ven-tricular sac. Appropriately mounted tissue or mechanicalvalves can be used for other test conditions not requiring theretrograde passage of the pressure–volume catheter. Meteredpulses of compressed air are delivered from a pneumatic con-troller (Utah Drive, CardioWest Technologies, Tucson, AZ) tothe pressurization chamber during systole compressing theventricular sac to form coapting quadrants, simulating contrac-tion of the normal and dysfunctional ventricle and the deliveryof the cardiac stroke volume (Figure 3). An artificial aorta(polyurethane tube segment) 25 mm in diameter is connecteddownstream of the outflow valve of the ventricular sac to themock systemic and coronary vasculature. The mock systemicvasculature consists of four integrated chambers each 10.1 cmin diameter that represent lumped proximal resistance, sys-temic compliance, peripheral resistance, and venous compli-
Table 1. Adult Mock Circulation Parameter Values forSimulating Normal, Failure, and Cardiac Recovery Physiologic
Conditions
Parameter Normal Failure Recovery
Mean AoP 95 mmHg 65 mmHg 80 mmHgCO 5.0 L/m 3.0 L/m 4.0 L/mLVPed 2–5 mmHg 15–25 mmHg 10–15 mmHgDLP 210 mmHg 80 mmHg 150 mmHg
AoP, aortic pressure; CO, cardiac output; LVPed, left ventricularend diastolic pressure; DLP, drive line pressure.
Figure 1. Illustration of adult mock circulation loop consisting ofa mock ventricle with atrial or apical inflow cannulation sites, mocksystemic vasculature with aortic root or descending thoracic aortaoutflow cannulation sites, and mock coronary vasculature. Alsoshown are transducers for measuring hemodynamic pressures,flows, and volume.
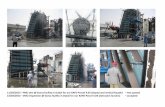
Figure 2. Photograph of adult mock circulation loop (left) andshown with a pulsatile ventricular assist device (VAD) connected tothe apex of the mock ventricle (right).
38 PANTALOS ET AL.

ance.25 The resistance chambers contain open cell foam ofdifferent densities compressed by sealed pistons to create therequired amount of resistance to flow. The compliance cham-bers have spring loaded pistons on roll sock diaphragms tocreate the required amount of arterial and venous compli-ance.26 Introduction ports for VAD uptake cannulae are incor-porated into the atrial wall and ventricular sac apex. Introducerports in the atrium, ventricle, aorta, and pressurization cham-ber enable insertion of pressure catheters. In line flow probes(Transonics, Ithaca, NY) are used for aortic, coronary, andVAD flow.
Instrumentation
A high fidelity, dual pressure–volume conductance catheter(Millar Instruments, Houston, TX) was inserted into the aorticintroducer port and passed retrograde through the outflow(aortic) valve and down to the ventricular apex for simulta-neous mock ventricular pressure, ventricular volume, and aor-tic pressure measurements. Single tip, high fidelity catheters(Millar Instruments, Houston, TX) were inserted into introducerports for measuring mock atrial pressure and mock ventricledriveline pressure. Aortic flow was measured with an in-line,transit time flow probe (Transonics, Ithaca, NY). Pressure andflow transducers were calibrated before and after to verify gainand offset accuracy. All instrumentation for hemodynamicmeasurement of pressures, flows, and volume are shown inFigure 1. Signal conditioning (amplification and offset) wasaccomplished using transducer amplifiers (Ectron, San Diego,CA), a transit time flowmeter (Transonics, Ithaca, NY), a vol-ume conductance unit (Leycom, Sigma V, Netherlands), andother peripheral conditioners integrated in a good laboratorypractice (GLP) compliant instrumentation system. Signal con-ditioned data were low pass filtered at 60 Hz, analog todigitally converted (AT-MIO-16E-10 and LabVIEW, NationalInstruments, Austin, TX) at a sampling rate of 400 Hz, andstored on a personal computer using custom data acquisitionsoftware.27
Data Analysis
Characterizing hemodynamic parameter values, ventricularpressure–volume relationships, vascular input impedance, andvascular mechanical properties (resistance, compliance, andinertance) were calculated using the Hemodynamic Evaluationand Assessment Research Tool (HEART) program28 and m filesdeveloped in Matlab (MathWorks, Natick, MA).
Hemodynamic Parameters
Mock circulation pressures, flows, and volumes were usedto calculate the following hemodynamic parameters: stroke
volume (SV) by integrating the aortic root flow, HR, and car-diac output (CO); left ventricular beginning (LVbd) and endingdiastolic (LVPed), peak systolic (LVPpksys) pressure, maximumLV peak positive (�dLVP/dt) and peak negative (�dLVP/dt)slopes, LV end diastolic (LVVed) and end systolic (LVVes)volumes, and LV ejection fraction (LVEF � LVSV � LVVed);left atrial mean pressure (LAPmean); aortic peak systolic (AoP-sys), end diastolic (AoPed), and mean (AoPmean) pressures;and aortic mean (AoFmean) and peak (AoFpk) flow. All hemo-dynamic parameters were calculated on a beat to beat basiswith all beats in each data set averaged to obtain a singlerepresentative mean value for each parameter.
Ventricular Pressure Volume Relationship
Pressure–volume loops were created by plotting ventricularpressure against ventricular volume, where each loop repre-sents one complete cardiac cycle (one beat). The LV volumedata was calibrated by adjusting the LV stroke volume (�LVVed � LVVes) to match the SV derived from aortic rootflow. Baseline pressure–volume loops for normal, failing heart,and cardiac recovery test conditions were generated. The enddiastolic pressure–volume relationship (EDPVR) and end sys-tolic pressure–volume relationship (ESPVR) were determinedfrom pressure–volume loops recorded during atrial inflow andaortic outflow occlusions.
Vascular Input Impedance
Vascular input impedance provides a rigorous way to rep-resent the afterload of the heart and depends in part on theresistance and elastance of the vasculature and the inertia ofthe blood. It may be influenced by pressure and flow wavereflections. Traditionally, clinicians rely on systemic resistance[(AoPmean � central venous pressure) � CO] instead of theterms of the input impedance influenced by elastance andinertial components. Any repeating waveform, including aorticpressure and flow waveforms, can be represented by a Fourierseries, which is a sum of cosines and sines of differing magni-tudes and phase angles at multiples of the fundamental fre-quency (harmonics). The input impedance of the mock vascu-lature was derived using aortic pressure and flowmeasurements during baseline recordings for each test condi-tion using Fourier analysis algorithms and m files developed inMatlab (MathWorks, Natick, MA). The magnitudes and phasesof the impedance for 10 harmonics were calculated as the ratioof the magnitudes of AoP and AoF and subtracting the phasesof AoP and AoF at each harmonic. An uncertainty analysis wasperformed to calculate the error in the input impedance termsresulting from experimental measurement errors.29
Vascular Mechanical Properties
The mechanical parameters of the mock vasculature wereestimated using the four element Windkessel model,30 asshown in Figure 4, and a frequency based parameter estima-tion routine.31 Briefly, the experimental impedance magni-tudes and phases are compared with the model derived im-pedance magnitudes and phases, and the lumped parameterelements (resistance, compliance, inertance, and characteristicimpedance) are adjusted iteratively until the error between theexperimental and model derived impedance is minimized.
Figure 3. Photographs of the mock ventricular sac filled at enddiastole (left) and compressed at end systole (right).
39MOCK CIRCULATION

Parameter estimates were made on a beat to beat basis andaveraged for all beats in each data set.
Results
The adult mock circulation produced physiologically equiv-alent hemodynamic waveform magnitudes and morphologyfor the normal, failing heart, and cardiac recovery test condi-tions (Figure 5). Notably, “ringing” in the aortic pressure wave-form coincident with the dicrotic notch was observed, which istypical of prosthetic valve closure function, particularly whenrigid mounted. The aortic pressure waveform shown in Figure5 was digitally filtered using the Matlab FILTFILT function,which is a zero phase forward and reverse digital filter. Char-acteristic cardiovascular parameters of the adult mock circu-lation for the normal, failing heart, and cardiac recovery stateswere comparable with physiologic parameters (Table 2). Ele-vated filling pressure (LVPed and LAPmean) and depressedstroke volume, peak aortic flow, contractility (�dLVP/dt), ex-ternal work (EW), ejection fraction (EF), and perfusion pressure(AoPmean) were successfully reproduced to mimic the failingheart test condition.
The pressure–volume relationship during baseline for nor-mal, failing heart, and partial cardiac recovery test conditionswere also indicative of the native left ventricle (Figure 6). In theheart failure state, the pressure–volume loops were shifted tothe right, and the area within the pressure–volume loops werereduced indicative of a larger heart with depressed function,including reduced SV, reduced stroke work, and reduced ejec-tion fraction. In the partial cardiac recovery state, the pressure–volume loops were shifted back leftward, and the area in-creased, mimicking a recovery was shifted back toward thenormal state.
The pressure–volume loops during atrial inflow and aorticoutflow occlusions show the response of the mock ventricle tovarying ventricular preload and afterload over a wide range ofloading (Figure 7). The slope of the EDPVR for the heart failurestate (0.32 mm Hg/ml) is nearly twice as large as the normalstate (0.18 mm Hg/ml), which indicates a stiffer ventricle dur-ing filling (Figure 8). The slope of the ESPVR of the heart failurestate (0.28 mm Hg/ml) is less than half that of the normal state(0.62 mm Hg/ml), which demonstrates a marked reduction incontractile function of the mock ventricle (Figure 9).
The magnitude and phase characteristics of the systemicinput impedance of the mock vasculature for the normal21 and
heart failure22 (elevated input impedance) states are shown inFigure 10. The mechanical properties of the mock vasculatureestimated using the four element Windkessel model (Figure 4)for the normal and heart failure (elevated input impedance)states are listed in Table 3. Uncertainty analysis showed lessthan 10% error in the magnitude and phase values for up to 10harmonics, with less error in the lower order harmonics (� 5%error) compared with the higher order harmonics (7–10%error).
Discussion
Mock circulation systems provide an attractive platform fortesting cardiac devices. Although they cannot replace in vivomodels, they are well suited for developing experimental pro-tocols, testing device performance and feedback control algo-rithms, investigating velocity profiles, and training surgical staffwith operational procedures of cardiovascular devices in nor-mal and adverse circumstances. Some investigators connectthe cardiac device directly to a mock vasculature, therebyeliminating the need for a mock atrium and mock ventricle.Additionally, many approach tuning the mock circulation toproduce physiologically equivalent mean preload and after-load pressures and resistances while not considering other
Figure 4. The four element Windkessel model used to estimatetotal peripheral resistance (R), systemic arterial compliance (C),inertance (L), and characteristic impedance (Z) from vascular inputimpedance data (AoP � aortic pressure and AoF � aortic flow).
Figure 5. Adult mock circulation hemodynamic waveforms for leftventricle in (a) normal, (b) failure, and (c) partial cardiac recovery testconditions at heart rate � 100 beats per minute (bpm) (AoP � aorticpressure, LVP � left ventricular pressure, AoF � aortic flow, andLVV � left ventricular volume).
40 PANTALOS ET AL.

Tab
le2.
Ad
ult
Mo
ckC
ircu
lati
on
Hem
od
ynam
icP
aram
eter
Val
ues
for
No
rmal
,Fa
ilure
,an
dC
ard
iac
Rec
ove
ryT
est
Co
ndit
ions
atR
and
om
lyS
elec
ted
Hea
rtR
ates
of
80,
100,
and
120
bp
m
Ad
ult
Moc
kC
ircul
atio
nP
aram
eter
LVno
rmal
LVno
rmal
LVno
rmal
LVfa
ilure
LVfa
ilure
LVfa
ilure
LVre
cove
ryLV
reco
very
LVre
cove
ry
HR
�80
bp
mH
R�
100
bp
mH
R�
120
bp
mH
R�
80b
pm
HR
�10
0b
pm
HR
�12
0b
pm
HR
�80
bp
mH
R�
100
bp
mH
R�
120
bp
m
LVS
V(m
l)63
5044
3730
2754
4135
LVH
R(b
pm
)80
100
120
8010
012
080
100
120
LVC
O(L
/min
)5.
05.
05.
33.
03.
03.
24.
44.
14.
3LV
Pb
d(m
mH
g)�
9.3
�4.
7�
8.1
�0.
9�
1.3
�2.
1�
5.2
�2.
1�
3.6
LVP
ed(m
mH
g)2.
42.
40.
713
.715
.313
.54.
74.
24.
0LV
Pp
ksys
(mm
Hg)
139.
513
7.4
137.
193
.089
.685
.512
1.5
114.
911
4.4
�d
LVP
/dt
(mm
Hg/
s)21
4624
3527
0411
4913
5614
1417
2620
6622
00�
dLV
P/d
t(m
mH
g/s)
�45
87�
4552
�44
58�
3214
�31
75�
2870
�39
11�
3600
�37
92LV
EW
(mm
Hg-
ml)
7924
6173
5609
2582
2153
1876
5586
4279
3568
LVV
ed(m
l)15
215
513
419
018
819
017
417
217
1LV
Ves
(ml)
7999
8713
914
515
011
712
513
0LV
EF
(%)
4836
3527
2321
3328
24LA
Pm
ean
(mm
Hg)
10.5
11.5
11.7
16.3
15.0
14.2
11.5
11.9
13.2
AoP
sys
(mm
Hg)
125.
512
4.4
135.
384
.488
.877
.310
3.4
101.
910
4.4
AoP
dia
(mm
Hg)
68.0
70.6
73.8
43.1
46.9
47.7
55.8
59.7
60.5
AoP
mea
n(m
mH
g)95
.395
.195
.760
.662
.661
.379
.180
.379
.5A
oFm
ean
(L/m
in)
4.9
4.9
4.9
2.9
2.9
3.1
4.1
4.0
4.0
AoF
pk
(L/m
in)
20.1
20.1
21.4
11.0
12.7
12.9
16.1
16.9
16.4
LV,l
eftv
entr
icul
ar;S
V,s
trok
evo
lum
e;H
R,h
eart
rate
;CO
,car
dia
cou
tput
;LV
Pb
d,L
Vb
egin
ning
dia
stol
icp
ress
ure;
LVP
ed,L
Ven
dd
iast
olic
pre
ssur
e;LV
Pp
ksys
,LV
pea
ksy
stol
icp
ress
ure;
�d
LVP
/dt,
max
imum
pea
kp
ositi
veLV
slop
e;�
dLV
P/d
t,m
axim
ump
eak
nega
tive
LVsl
ope;
LVE
W,
left
vent
ricul
arex
tern
alw
ork;
LVV
ed,
LVen
dd
iast
olic
volu
me;
LVV
es,
LVen
dsy
stol
icvo
lum
e;LV
EF,
LVej
ectio
nfr
actio
n;LA
Pm
ean,
left
atria
lmea
np
ress
ure;
AoP
sys,
aort
icp
eak
syst
olic
pre
ssur
e;A
oPd
ia,a
ortic
dia
stol
icp
ress
ure;
AoP
mea
n,ao
rtic
mea
np
ress
ure;
AoF
mea
n,m
ean
aort
icflo
w;
AoF
pk,
pea
kao
rtic
flow
.
41MOCK CIRCULATION

properties such as the elastance and inertance of the mockvasculature. The mock circulation can be operated to mimicthe Frank–Starling response of the native ventricle for normal,failing heart, and partial cardiac recovery test conditions. Fur-thermore, it can be set up to test cardiac assist devices in avariety of different configurations, including the choice ofatrial or apical uptake cannulation and aortic root or descend-ing thoracic aorta return cannulation. This study demonstratedthe ability of the mock circulation to produce the Frank–Starling response with physiologic characteristic hemody-namic parameters and pressure–volume relationships for alltest conditions. The input impedance and mechanical proper-ties of the mock vasculature were comparable to the natural,normal vasculature, but only the resistance in the failing heartstate could be faithfully reproduced.
The cardiac and vascular hemodynamic waveforms of themock circulation are comparable to natural physiology in bothmagnitudes (Table 2) and morphologic features32–33 (Figure 5).These data demonstrate that the mock ventricle can simulatenormal, failing heart, and cardiac recovery test conditions.Specifically, filling pressures and ventricular volumes are ele-vated whereas cardiac output, stroke volume, and systolicpressures are depressed in the heart failure state comparedwith normal state, which are indicative of clinical findings. Themost notable departure in waveform morphologic features canbe seen in the aortic pressure waveform. There is ringing at thedicrotic notch during valve closure. The ringing is associatedwith the limitations of a rigid mounted mechanical valve andsubstantial inertance in the mock vasculature introduced bythe outflow conduit and flow probe used to measure aorticflow. This ringing is also observed in the vicinity of a prostheticmechanical valve that is attached to a natural vasculature.34
Despite this limitation, the characteristic hemodynamic pa-rameter values and waveform morphology are within the phys-iologic envelope and are adequate for testing cardiac devices.
The ventricular pressure–volume loops during baseline testconditions (Figure 6) are indicative of what has been reportedclinically.35 The ventricular SV and end systolic pressure are
depressed whereas filling pressure is elevated in the heartfailure state compared with normal heart state. Further, theexternal work of the mock ventricle in the failing heart state isnearly one-third that of the normal heart, which is also indic-ative of a dysfunctional heart.35 The EDPVR and ESPVR de-rived from the occlusion data (Figure 7) for each test conditionalso follow the expected physiologic response. The slope ofthe EDPVR for the failing heart state is approximately twicethat of the normal heart state (Figure 8), which is indicative ofa stiffer heart during filling. The slope of the ESPVR for thefailing heart state is less than half that of the normal heart state(Figure 9), which is indicative of a less contractile heart duringejection. The combination of a stiffer heart during filling and aless contractile heart during ejection are characteristic of thenatural, failing heart. Further, the pressure–volume loops, ED-PVR, and ESPVR for the cardiac recovery state demonstrate animproved cardiac state with a return toward the normal heartcondition. The pressure–volume relationships for each testcondition are comparable with what has been reported clini-cally in VAD patients.36–38
The input impedance and mechanical properties of themock vasculature are representative of the natural, normalvasculature (Figure 10). The magnitudes of the DC and 10harmonic terms are comparable. The phase angles for the firstthree harmonics show a good match between the mock andnatural vasculature. However, the zero phase crossover pointof the mock phase lags behind that of the native phase, and atthe higher order harmonics, phase values deviate by approxi-mately 30°. These differences are likely caused by alteredwave reflections or inertial effects inherent in the mock vas-culature because of the cross-sectional area and length oftubing, as well as areas of the mock vasculature componentsand the fluid volumes contained therein. The mechanicalproperties, particularly the vascular resistance and complianceindicate a good match between the natural and mock vascu-lature in the normal state (Table 3). For the heart failure con-dition, the mock vasculature can reproduce the DC compo-nent of the input impedance, indicative of the resistive load.The phase characteristics of the input impedance of the mockvasculature show similar differences (approximately 15–25°) ateach harmonic and a delay in the zero phase crossover point.The mechanical properties further support this finding becausethe resistance could be controlled but the compliance andcharacteristic impedance properties differed by an order ofmagnitude. Although the characteristic hemodynamic param-eter values (mean, systolic, and diastolic) and waveform mor-phology can qualitatively appear to provide a good matchbetween the natural and mock vasculature for the failing heart,differences in the input impedance and mechanical propertyestimates clearly demonstrate the limitations of the mock vas-culature and illustrate the importance of not relying solely onwaveform features, mean values, and peripheral resistance.This is a very significant point that can be easily overlooked. Ithas been shown that the systemic input impedance in heartfailure patients39–40 is stiffer (smaller compliance and largerresistance) compared with patients with normal ventricles.21 Astiffer vasculature can increase pulse wave propagation result-ing in early return of reflected wave energy increasing ventric-ular work load during ejection and reducing myocardial per-fusion during relaxation.41
Figure 6. Adult mock ventricle pressure–volume loops for simu-lated normal, failure, and partial cardiac recovery baseline testconditions at heart rate � 100 beats per minute (bpm).
42 PANTALOS ET AL.

Figure 7. Adult mock ventricle pressure–volume (PV) loops during a simulated vena cava (VC, dotted line) and aortic (Ao, solid line)occlusion for simulated (a) normal, (b) failure, and (c) partial cardiac recovery test conditions at heart rate � 100 bpm. The pressure–volumeloops follow patterns typically seen in natural ventricles.
43MOCK CIRCULATION

Clinical Significance
The ability to realistically simulate normal and various ab-normal conditions of cardiovascular function is a valuableasset for academic instruction and training of clinical person-nel. The mock circulation described in this report accords suchan opportunity with great versatility while avoiding or mini-mizing the need for using laboratory animals. Many principlesof cardiovascular function can be demonstrated without theinclusion of a neurohumoral response. Training on the use ofclinical hemodynamic instrumentation can be accomplishedwhile students and staff are exposed to a physical rather thanan electronic reproduction of cardiovascular function. Like-wise, instrumentation being considered for future applicationcan be evaluated with this system. With a mock circulatorysystem, students have a “safe” opportunity to explore the
consequences of changing parameters and can make a tangi-ble correspondence between an increase or decrease with thepressurization of the ventricular sac and pharmacologic agentsthat increase or decrease ventricular contractility. Likewise,the physical correspondence can be made between a changein the peripheral vascular resistance element and pharmaco-logic agents that increase or decrease vascular tone and pe-ripheral resistance. The hemodynamic consequences of hypo-volemia and the appropriate response can be readilysimulated. The simulation scenarios are numerous.
To date, impedance data have not been used as a clinicalassessment tool in the evaluation of cardiovascular patients.However, their relevance needs to be appreciated in the test-ing of cardiovascular devices to give an accurate evaluation ofdevice clinical performance and reliability. Using a mockcirculatory system for testing a cardiovascular device, such asa valve or an artificial ventricle, that does not have an inputimpedance that sufficiently matches the circumstances inwhich it will be applied can result in exposure to overloading
Figure 8. Adult mock ventricle end diastolic pressure–volumerelationship (EDPVR) for simulated normal, failure, and partial car-diac recovery test conditions at heart rate � 100 beats per minute(bpm).
Figure 9. Adult mock ventricle end systolic pressure–volumerelationship (ESPVR) for simulated normal, failure, and partial car-diac recovery test conditions at heart rate � 100 beats per minute(bpm).
Figure 10. Comparison of adult mock vasculature and naturalheart (native) vasculature input impedance (magnitude and phase)for (a) normal heart and (b) failing heart test conditions at heart rate� 80 beats per minute (bpm).
Table 3. Adult Mock Circulation Mechanical PropertyParameter Estimates for Normal and Failing Heart TestConditions at Heart Rates of 80 bpm Using 4-Element
Windkessel Model
Parameter
Normal Heart Heart Failure
Native Mock Native Mock
Resistance - R(dyne-s/cm5)
1218 1335 2023 1902
Compliance - C(ml/mmHg)
1.4 1.3 0.3 1.3
Inertance - L(mmHg-s2/ml)
0.02 0.01 0.05 0.02
Characteristicimpedance -Z (mmHg-s/ml)
65 75 1066 73
R, arterial resistance; C, arterial compliance; L, arterial induc-tance; Z, arterial characteristic impatience.
44 PANTALOS ET AL.

or underloading conditions that could yield misleading testresults. The response to these unrealistic results may be anunnecessary redesign of a device with corresponding compro-mises in device performance. Hence, the use of a mock cir-culation system with a valid input impedance is an essentialtool in the prediction of the clinical performance of a devicefrom laboratory testing.
Limitations
The performance of the mock circulation during normal,failing heart, and cardiac recovery test conditions is represen-tative of clinical observations from a purely hemodynamic/hydrodynamic viewpoint. Clearly, a mock circulation is notintended to replace in vivo models and is incapable of repli-cating all expected clinical responses. For instance, the mockcirculation cannot be used to study neurohumoral responses,tissue remodeling, activation of regulatory proteins, or changesin genetic phenotype. Furthermore, a number of mock circu-lation and numerical models have been proposed for investi-gating the performance of cardiac devices. The authors do notintend to suggest that the mock circulation system presented inthis article is superior to these other systems but rather todemonstrate that it is able to reproduce the Frank–Starlingresponse reported clinically and that it would be of interest fortesting cardiac devices and for approximating the input imped-ance of the natural vasculature.
A key current limitation of the mock circulation used in thisinvestigation is that it only represents the systemic circulationrestricting testing to left ventricular assist devices. A compara-ble pulmonary circulation has been developed25 and will beincorporated into future investigations to allow testing duringthe simulation of right ventricular and biventricular failure. Thecurrent mock circulation also lacks authenticity in certaindetails of the arterial waveform (ringing) and impedance phaseresponses (i.e., inductance), particularly in the failing heartvasculature. The instrumentation used to record hemodynamicvariables has inherent measurement errors associated witheach technique (i.e., pressure error � � 1 mm Hg, flow error� � 0.5 L/min), which the authors attempted to minimize byusing GLP compliant test equipment, calibration procedures,and documentation practices. The methods used to analyzethese data can also introduce error, particularly the calculationof the EDPVR, ESPVR, and lumped-parameter model for as-sessing vascular mechanical properties. Despite these limita-tions, the mock circulation presented here should be a valu-able research tool for assessing the performance of cardiacdevices, developing experimental protocols in a controlledenvironment in preparation for in vivo studies, and trainingpersonnel on the operation and maintenance of cardiacdevices.
Acknowledgment
This project was funded by a grant from the Jewish Hospital Re-search Foundation (Louisville, KY). The authors would like to thankCardioWest Technologies, Tucson, AZ, for providing the pneumaticheart controller essential for the conduct of this investigation.
References
1. Wieting DW: Design and evaluation of a system suitable foranalyzing flow behavior of prosthetic human heart valves (mas-ters thesis). University of Texas, Austin, 1966.
2. Cornhill JF: An aortic–left ventricular pulse duplicator used intesting prosthetic aortic heart valves. J Thorac Cardiovasc Surg73: 550–558, 1977.
3. Scotten LN, Dipl T, Walker DK, Brownlee RT: Construction andevaluation of a hydromechanical simulation facility for theassessment of mitral valve prostheses. Journal of Medical Engi-neering and Technology 3: 11–18, 1979.
4. Walker DK, Modi VJ, Brownlee RT: In vitro assessment of mitralvalve prosthesis. J Thorac Cardiovasc Surg 79: 680–688, 1980.
5. Schima H, Tsangaris S, Zilla P, Kadletz M, Wolner E: Mechanicalsimulation of shear stresses on the walls of peripheral arteries.J Biomech 23: 845–851, 1990.
6. Sipkema P, Latham RD, Westerhof N, Rubal BJ, Slife DM: Isolatedaorta setup for hemodynamic studies. Ann Biomed Eng 18:491–503, 1990.
7. Schima H, Baumgartner H, Spitaler F, Kuhn P, Wolner E: Amodular mock circulation for hydromechanical studies onvalves, stenosis, vascular grafts and cardiac assist devices. Int JArtif Organs 15: 417–421, 1992.
8. Garrison LA, Frangos JA, Geselowitz DB, Lamson TC, Tarbell JM:A new mock circulatory loop and its application to the study ofchemical additive and aortic pressure effects on hemolysis inthe Penn State electric ventricular assist device. Artif Organs 18:397–407, 1994.
9. Helal MA, Watts KC, Marble AE: Hydrodynamic simulation ofarterial networks which include compliant and rigid bypassgrafts. J Biomech 27: 277–287, 1994.
10. Vandenberghe S, Segers P, Meyns B, Verdonck P: Hydrodynamiccharacterization of ventricular assist devices. Int J Artif Organs24: 470–477, 2001.
11. Knierbein B, Reul H, Eilers R, Lange M, Kaufmann R, Rau G:Compact loops of the systemic and pulmonary circulation forblood pump testing. Int J Artif Organs 15: 40–48, 1992.
12. Ferrari G, Delazzari C, Mimmo R, Ambrosi D, Tosto G: Mockcirculatory system for in vitro reproduction of the left ventricle,the arterial tree and their interaction with a left-ventricular assistdevice. J Med Eng Technol 18: 87–95, 1994.
13. Vermette P, Thibault J, Laroche G: A continuous and pulsatile flowcirculation system for evaluation of cardiovascular devices.Artif Organs 22: 746–752, 1998.
14. Sharp MK, Dharmalingam RK: Development of a hydraulic modelof the human systemic circulation. ASAIO J 45: 535–540, 1999.
15. Schaub JD, Koenig SC, Schroeder MJ, Ewert DL, Drew GA, SwopeRD: Development of a flow feedback pulse duplicator systemwith rhesus monkey arterial input impedance characteristics.ASAIO J 45: 334–338, 1999.
16. Ferrari G, Nicoleti A, DeLazzari C, et al: A physical model of thehuman systemic arterial tree. Int J Artif Organs 23: 647–657,2000.
17. Baloa LA, Boston JR, Antaki JF: Elastance based control of a mockcirculatory system. Ann Biomed Eng 29: 244–251, 2001.
18. Ferrari G, Kozarski M, DeLazzari C, et al: A hybrid (numerical-physical) model of the left ventricle. Int J Artif Organs 24:456–462, 2001.
19. Ferrari G, DeLazzari CD, Kozarski M, et al: A hybrid mock circu-latory system: Testing a prototype under physiologic and patho-logical conditions. ASAIO J 48: 487–494, 2002.
20. Rosenberg G, Phillips WM, Landis DL, Pierce WS: Design andevaluation of the Pennsylvania State University mock circula-tory system. ASAIO J 4: 41–49, 1981.
21. Nichols WW, Conti CR, Walker WE, Milnor WR: Input imped-ance of the systemic circulation in man. Circ Res 40: 451–458,1977.
22. Koenig SC, Shafie M, Pearson A, et al: Intraoperative assessment ofacute hemodynamic changes after partial left ventriculectomy.J Card Surg 14: 152–156, 2000.
23. Pantalos GM, Hayes J, Khanwilkar P, Bearnson G, Olsen D: Leftventricular simulator for cardiovascular device testing. ASAIO J42: 46, 1996.
24. Pantalos GM, Chiang B, Bishop D, et al: Development of smallerartificial ventricles and valves made by vacuum forming. Int JArtif Organs 11: 373–380, 1988.
25. Gillars KJ: Design and validation of a four-region hydraulic model
45MOCK CIRCULATION

of the human cardiovascular system (masters thesis). Universityof Utah, Salt Lake City, 2003.
26. Woodruff SJ, Sharp MK, Pantalos GM: Improved compliancechamber design for the study of cardiac performance in micro-gravity. ASAIO J 43: 316–320, 1997.
27. Drew GA, Koenig SC: Biomedical patient monitoring, data acqui-sition, and playback with LabVIEW. Chapter 2, in Martin HT,Martin ML (eds), LabVIEW for Automative, Telecommunica-tions, Semiconductor, Biomedical, and Other Applications.Upper Saddle River, NJ: Prentice Hall PTR, pp. 92–98, 2000.
28. Schroeder MJ, Perrault B, Ewert DL, Koenig SC: HEART: an auto-mated beat-to-beat cardiovascular analysis package using Mat-lab. Comput Biol Med (in press).
29. Koenig SC, Schroeder MJ, Wheeler B, Jorgenson J, Ewert DL:Uncertainty analysis of measurement error in calculating vas-cular input impedance: How many harmonics can be resolved?2nd Joint EMBS–BMES Conference, Houston, TX, October 23–26, 2002.
30. Stergiopulos N, Westerhof BE, Westerhof N: Total arterial iner-tance as the fourth element of the Windkessel model. Am JPhysiol 276: H81–H88, 1999.
31. Essler S, Schroeder MJ, Phaniraj V, Koenig SC, Latham RD, EwertDL: Single beat estimation of arterial vascular parameters fortransient and steady beats with application to hemodynamicstate under variant gravitational conditions. Ann Biomed Eng27: 486–97, 1999.
32. Nichols WW, O’Rourke MF: McDonald’s Blood Flow in Arteries:
Theoretical, Experimental and Clinical Principles, Fourth edi-tion. Oxford: Oxford University Press, 1998.
33. Guyton AC: Textbook of Medical Physiology, 10th ed. Philadel-phia: WB Saunders, 2000.
34. Pantalos GM, Kim C, Robison P, Everett S, Olsen DB: Character-ization of natural and total artificial heart acceleration. ASAIOTrans 35: 235–238, 1989.
35. Sagawa K, Maughan WL, Suga H, Sunagawa K: Cardiac Contrac-tion and the Pressure–Volume Relationship. Oxford: OxfordUniversity Press, 1998.
36. Levin HR, Oz MC, Chen JM, Packer M, Rose EA, Burkhoff D:Reversal of chronic ventricular dilation in patients with end-stage cardiomyopathy by prolonged mechanical unloading.Circulation 91: 2717–2710, 1995.
37. Burkhoff D, Holmes JW, Madigan J, Barbone A, Oz MC: Leftventricular assist device-induced reverse ventricular remodel-ing. Prog Cardiovasc Dis 43: 19–26, 2000.
38. Madigan JD, Barbone A, Choudhri AF, et al: Time course ofreverse modeling of the left ventricle during support with a leftventricular assist device. J Thorac Cardiovasc Surg 121: 902–908, 2001.
39. Pepine CJ, Nichols WW, Conti CR: Aortic input impedance inheart failure. Circulation 58: 460–465, 1978.
40. Nichols WW, Pepine CJ, Conti CR: Vascular load defined by theaortic input impedance spectrum. Federation Proceedings 39:196–201, 1980.
41. Nichols WW, Pepine CJ: Ventricular/vascular interaction in healthand heart failure. Compr Ther 18: 12–19, 1992.
46 PANTALOS ET AL.











![WBJEE MOCK TEST PAPER POWERED BY … · wbjee mock test paper –powered by wbjee mock test paper [ pathfinder ] wbjee mock test – 2 [mathematics-2]](https://static.fdocuments.in/doc/165x107/5f5911bc7de6a572a9381525/wbjee-mock-test-paper-powered-by-wbjee-mock-test-paper-apowered-by-wbjee-mock.jpg)





