Chapter Four - Elsevier
18
Chapter Four c0020 The principles of combined movement assessment Chris McCarthy CHAPTER CONTENTS u0010 Subjective examination ............... 52 u0015 Physical examination ................ 54 u0020 Observation ................... 54 u0025 Functional demonstration ........... 54 u0030 Active movements ............... 56 u0035 Degree of symptom reproduction deemed acceptable .................... 57 u0040 Prime movement and prime combination . 57 u0045 Muscle assessment .............. 59 u0050 Passive movement and mini-treatments . 59 u0055 Assessing for the suitability of manipulative thrust techniques ................ 60 u0060 Cervical spine case study ............. 62 u0065 Lumbar spine case study ............. 65 p0070 The purpose of clinical examination is not simply to gather as much information as is possible in the time available. Often the inexperienced clinician can spend an entire examination gathering data with little evaluation of its clinical relevance. As manual therapists we provide our patients with incredibly sensitive examinations. The volume and sophistica- tion of our examination procedures is immense. However, we may occasionally fail to grasp the problem of specificity. We must find a balance between gathering enough information to prioritize the patient’s most significant dysfunction whilst not being distracted by the less relevant dysfunc- tions we discover. p0075 We are essentially searching for the patient’s ‘predominant dysfunction or fault’ in order to direct our intervention towards it. The process of ranking the importance of our findings requires that we test the hypothesis of ‘predominant dysfunction’ throughout our interaction with our patients. In short, during the examination of patients we are considering if our hypothesis will guide treatment more effectively than the next most likely hypothe- sis. In addition, during treatment we should be continually considering if our chosen intervention is in fact more effective than the next most likely intervention. This process of analytical assessment is not new and was advocated by Maitland (1986) and Grieve (1988, 1991) over 30 years ago. p0080 Simply gathering huge quantities of information that is neither discriminatory nor influential in man- agement represents a failure in our duty of care to our patients. The purpose of clinical examination is to evaluate valid information that will facilitate the prioritization of likely diagnoses and strategies of management. In other words, our duty to our patients is to ensure we are identifying their pre- dominant dysfunction/fault and to continually ensure that we are providing the most effective management strategy at the time. Ensuring we adhere to this principle will ensure we are facilitat- ing recovery as quickly as possible. It could be argued that the primary objective of manual therapy is to facilitate recovery as quickly as possible. On the whole, the conservative management of most musculoskeletal dysfunctions will facilitate recov- ery. Manual therapy’s role is in the acceleration of this process. Thus, ensuring our treatment choice is making more difference, more quickly than the next most likely choice of treatment is a crucial responsibility. 4 ã 2010, Elsevier Ltd. B978-0-443-06857-7.00004-6, 00004 McCarthy, 978-0-443-06857-7
Transcript of Chapter Four - Elsevier

Chapter Four
c0020 The principles of combinedmovement assessment
Chris McCarthy
CHAPTER CONTENTS
u0010 Subjective examination . . . . . . . . . . . . . . . 52
u0015 Physical examination . . . . . . . . . . . . . . . . 54
u0020 Observation . . . . . . . . . . . . . . . . . . . 54
u0025 Functional demonstration . . . . . . . . . . . 54
u0030 Active movements . . . . . . . . . . . . . . . 56
u0035 Degree of symptom reproduction deemedacceptable . . . . . . . . . . . . . . . . . . . . 57
u0040 Prime movement and prime combination . 57
u0045 Muscle assessment . . . . . . . . . . . . . . 59
u0050 Passive movement and mini-treatments . 59
u0055 Assessing for the suitability of manipulativethrust techniques . . . . . . . . . . . . . . . . 60
u0060 Cervical spine case study . . . . . . . . . . . . . 62
u0065 Lumbar spine case study . . . . . . . . . . . . . 65
p0070 The purpose of clinical examination is not simply togather as much information as is possible in thetime available. Often the inexperienced cliniciancan spend an entire examination gathering data withlittle evaluation of its clinical relevance. As manualtherapists we provide our patients with incrediblysensitive examinations. The volume and sophistica-tion of our examination procedures is immense.However, we may occasionally fail to grasp theproblem of specificity. We must find a balancebetween gathering enough information to prioritizethe patient’s most significant dysfunction whilstnot being distracted by the less relevant dysfunc-tions we discover.
p0075 We are essentially searching for the patient’s‘predominant dysfunction or fault’ in order to directour intervention towards it. The process of ranking
the importance of our findings requires that wetest the hypothesis of ‘predominant dysfunction’throughout our interaction with our patients. Inshort, during the examination of patients we areconsidering if our hypothesis will guide treatmentmore effectively than the next most likely hypothe-sis. In addition, during treatment we should becontinually considering if our chosen interventionis in fact more effective than the next most likelyintervention. This process of analytical assessmentis not new and was advocated by Maitland (1986)and Grieve (1988, 1991) over 30 years ago.
p0080Simply gathering huge quantities of informationthat is neither discriminatory nor influential in man-agement represents a failure in our duty of care toour patients. The purpose of clinical examinationis to evaluate valid information that will facilitatethe prioritization of likely diagnoses and strategiesof management. In other words, our duty to ourpatients is to ensure we are identifying their pre-dominant dysfunction/fault and to continuallyensure that we are providing the most effectivemanagement strategy at the time. Ensuring weadhere to this principle will ensure we are facilitat-ing recovery as quickly as possible. It could beargued that the primary objective of manual therapyis to facilitate recovery as quickly as possible. Onthe whole, the conservative management of mostmusculoskeletal dysfunctions will facilitate recov-ery. Manual therapy’s role is in the acceleration ofthis process. Thus, ensuring our treatment choiceis making more difference, more quickly than thenext most likely choice of treatment is a crucialresponsibility.
4
ã 2010, Elsevier Ltd.
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7
s0010Subjective examination
p0085 During the initial consultation the therapist will beginto form an impression of the patient based on verbaland non-verbal communication. Expert cliniciansform an impression regarding diagnosis, managementand expectations of the patient very quickly. Mixedmethods of clinical reasoning are utilized in this pro-cess as outlined in Chapter 3.
p0090 The diverse nature ofmusculoskeletal dysfunctionrarely allows the definitive identification of definitivepatterns of presentation. The clinician is frequentlyrequired to make reasoned judgements as to the pre-dominant dysfunction from several alternatives.Some of the typical judgements required are listedbelow. This is by no means an exhaustive list. Theprocess of establishing that one treatment approachis superior to another begins during the initial consul-tation with the patient. Early in the initial interviewwith a patient, the therapist should look for answersto the following questions.
s0030 Is this patient’s presentation suitable for amanual therapy approach?
u0070 • Is this patient presentation sounding like I shouldexplore further with an assessment ofbiomechanical dysfunction?
u0075 • Does this patient’s presentation suggest that amore psychosocial approach may elicit effectivetreatment strategies?
s0035 Which patterns of presentation does thispresentation match with?
u0080 • Does the presentation fit a pattern ofpresentation I have encountered before?
u0085 • If so, what is it that makes this patient’spresentation fit this pattern better than the nextmost likely pattern?
u0090 • What questions and tests do I need to use to testthis hypothesis?
s0040 Does the functional fault have a directionalquality?
u0095 • In what combination of positions are symptomsreproduced?
u0100 • In what combination of positions are symptomsreduced?
s0045 What is the likely source of the directionalfault?
u0105 • Does the presentation have predominantlyarthrogenic features?
u0110• Does the presentation have predominantlymyogenic features?
u0115• Does the presentation have predominantlyneurodynamic features?
s0050Is this predominantly a control orimpairment fault?
u0120• Does the presentation suggest a dysfunction incontrol of movement?
u0125• Does the presentation suggest a dysfunctionassociated with limitation (or impairment) ofmovement?
s0055Is it acceptable to reproduce symptoms – arethey ‘severe’?
u0130• Is the faulty position producing severe pain?
u0135• Is positioning in the faulty position likely to cause alatent or long-term exacerbation of symptoms?
u0140• Is there a position that will allow examinationand treatment whilst avoiding unacceptablesymptom reproduction?
u0145• Is it likely that caution needs to be taken due to apatho-anatomical reason that would make theuse of combined movement theory (CMT)unwise? See the contraindications to manualtherapy in the box below.
s0060What is the predominant pain mechanism?
u0150• Is the patient’s predominant pain mechanism:nociceptive, peripheral neurogenic, centralsensitivity, autonomic or affective?
b0010
p0215A proforma planning sheet can be found on the CD. SeeFigure 4.1.
p0370Prior to the conduct of a physical examinationusing the CMT approach the patient should beinformed of your plans and the risks and benefitsof the approach against other approaches.
p0375By examining the expectations of the patientthe suitability of utilizing a CMT approach can beestablished. If the patient’s expectations of treat-ment are radically different to the therapist’s, adiscussion of future management should ensue. Adetailed biomechanical assessment of spinal dys-function may be unwarranted if the patient isexpecting and consenting only to generic adviceand exercise.
S E C T I O N O N E Combined Movement Theory
52
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

Clinical pointb0015
b0015 Contraindications to spinal passive movementthat takes a joint to the end of passive range orthrust techniques
s0065 Bone
p0220 Any pathology that has led to significant bone weakening:
u0155 • Tumour, e.g. metastatic deposits
u0160 • Infection, e.g. tuberculosis
u0165 • Metabolic, e.g. osteomalacia
u0170 • Congenital, e.g. dysplasias
u0175 • Iatrogenic, e.g. long-term corticosteroid medication
u0180 • Inflammatory, e.g. severe rheumatoid arthritis
u0185 • Traumatic, e.g. fracture
s0070 Neurological
u0190 • Spinal cord compression
u0195 • Cauda equina compression
u0200 • Nerve root compression with increasing
neurological deficit
s0075 Vascular
u0205 • Aortic aneurysm
u0210 • Bleeding into joints, e.g. severe haemophilia
u0215 • Cervical artery dysfunction (Kerry et al, 2008a, 2008b)
s0080 Relative contraindications
p0300 Special consideration should be given prior to the use
of spinal manipulative thrust techniques in the following
circumstances:
u0220 • Adverse reactions to previous manual therapy
u0225 • Disc herniation or prolapse
u0230 • Inflammatory arthritides
u0235 • Pregnancy
u0240 • Spondylolysis
u0245 • Spondylolisthesis
u0250 • Osteoporosis
u0255 • Anticoagulant or long-term corticosteroid use
u0260 • Advanced degenerative joint disease and spondylosis
u0265 • Psychological dependence upon spinal manipulative
thrust techniques
u0270 • Ligamentous laxity
u0275 • Arterial calcification
u0280 • Hypertension (diastolic>95) in cervical manual therapy
(See Gibbons & Tehan, 2001a,b; Grieve, 1991.)
s0085 Is the patient suitable for a biomechanicalassessment of their movement fault?
p0380 Patient presentations suggestive of a predominantmechanical influence on symptoms are suitable fordetailed biomechanical assessment and treatment.
Presentations that do not feature mechanical/move-ment influences on symptomology suggest thatspecific positions and movements may not be the pre-dominant influences to be addressed during examina-tion and treatment. Thus, patients who have constantsymptoms, regardless of positioning, will be unlikelyto benefit from management with a positional bias.Patients with central sensitization or inflammatoryneurogenic pathology (‘irritable’ patients (Maitland,1985) have no mechanical predominance.
s0090How acceptable is it to reproduce symptoms?p0385Patients, seeking manual therapy, present with pain
and largely judge their improvement by an ameliora-tion of their pain. In the process of assessing theeffect of testing and treatment, changes in pain areassessed. However, in cases where pain is severe, itis unacceptable to reproduce pain and inappropriateto treat an underlying mechanical dysfunction whilstreproducing pain. Thus, prior to any physical testingthe therapist must be clear regarding the degree towhich pain is to be reproduced during their interac-tion with the patient. In certain presentations itmay be deemed acceptable to fully reproduce theminor discomfort the patient is seeking help for, inorder to fully relieve it. However, in situations wherepain is severe this is unacceptable. Using positionsthat can reduce the likelihood of reproducing severepain is one of the key advantages of CMT.
b0020Clinical relevance
p0390If it is not acceptable to reproduce symptoms, thecondition is severe. If it is acceptable it is not. Use a
nominal (yes/no) approach to this decision and your
clinical reasoning will be decisive and more reasonable.
s0095What is the functional demonstration ofthe positional fault?
p0395Patient presentations, suggestive of the suitability of aCMT approach, have symptoms predominantly influ-enced by specific positions or movements. Patientscan often demonstrate these movements or positionsand reproduce them in the course of replicating a func-tional activity. For example, patients with anteriorstretch patterns of the mid cervical spine often relatesymptom reproductionwith activities inducing ipsilat-eral lateral flexion and rotation, e.g. reversing the car.Themonitoring of change in the functional demonstra-tion, during examination and treatment is a crucialmonitor of treatment effectiveness. Again, theconcept of a functional demonstration is a long-
C H A P T E R 4The principles of combined movement assessment
53
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

established tenet of the Maitland concept (Maitland,1986) and at the heart of CMT.
s0100 What is the region of the spine that is likely tobe faulty?
p0400 The biomechanical interpretation of patient presen-tation can allow the therapist to judge the locationof regions of dysfunction. Careful questioning canelicit functional activities that influence specificregions of the spine. For example, the influence ofbreathing on thoracic movement can provide valu-able inference towards spinal or rib dysfunctions.
s0105 What is the predominant hypothesis for thesource and mechanism of symptom productionand the next most likely hypothesis that will betested against it?
p0405 It is crucial to form hypotheses regarding the under-lying source and mechanism of symptom productionas you recognize presentation patterns. As a patternof presentation begins to emerge the use of follow-upquestions will establish a good fit with this pattern.Having identified amatch with a recognizable pattern,the manual therapist should test the assumption thatthis hypothesis is predominant by comparing thematch with the nextmost likely pattern. For example,having established that a patient’s presentationmatched an ‘arthrogenic’ presentation, one wouldexpect the presentation to be less well matched witha ‘myogenic’ presentation. In order to facilitate thisprocess it can be useful to develop a library of ‘stock’questions and tests for common presentations.
p0410 The use of these strategies will facilitate thetherapist’s reasoning regarding the appropriatenessof using CMT, the most likely hypotheses foraetiology of symptoms, the extent and direction ofmovements to be included in the examination andmost importantly the starting positions in whichassessment and treatment will be undertaken.
p0415 Figure 4.1 shows a suggested planning sheet for usein clinical reasoning during the CMT examination.
s0110Physical examination
p0420 The objective examination will follow the subjectiveexamination and is conducted in light of the consid-erations and clinical reasoning process outlined inthis book. The object of the physical examinationis not to form a long list of impairments with littleevidence of their relative contribution tothe patient’s dysfunction. The physical examinationshould allow the hypotheses, generated following
the subjective examination, to be tested. Thus, theexamination should be structured to allow this pro-cess to occur. In order to assess the influence of thetesting procedures themselves on a patient’s dys-function the physical examination should be splitinto components.
p0425The order in which components of the examina-tion are conducted will be guided by the subjectiveexamination. A clinician may hypothesize that thepredominant mechanism of symptom production isrelated to a restriction in articular mobility ratherthan, e.g. a restriction in overlying muscle mobility.In this case, the examination would be structured toexamine the articular system, assess its influence onthe fault, and then assess the muscular influenceand reassess that system’s influence on the fault.In this way, in addition to gathering informationfrom each component of the examination the rela-tive influence of the components can be evaluated.
p0430Each component begins with an assessment ofmovement fault (using the patient’s functional dem-onstration), testing procedures and a subsequent reas-sessment of functional demonstration. See Figure 4.2.
s0115Observation
p0435Observation of static posture can give valuable insightinto the likely mechanical presentation of symptomswithmovement. A number of static features will helpin the interpretation of activemovement. A deep skincrease may suggest hypermobility at the level whilstflat sections with reduced muscle bulk may suggesthypomobility. Defined muscle borders may indicatehypertonicity whilst unilateral atrophy may indicatelocal neuropraxia or trophic change. See Figure 4.3.
s0120Functional demonstration
p0440The functional demonstration is the term given tothe combination of plane movements that thepatient has identified to take them into their mostaggravating position. This position identifies themovement fault, whilst the quality, range and speedof movement from neutral into this position andreturn, should be analyzed in depth. The combina-tion of physiological movements that constitutethe functional demonstration will provide invaluableinformation about the starting position that shouldbe adopted for passive movement assessment andtreatment. In addition, the three-dimensional com-ponents of this position will identify the movements
S E C T I O N O N E Combined Movement Theory
54
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

List your hypotheses for the nature of the condition. ...................................................................................................................................................................................................... ...................................................................................................................................................................................................... ......................................................................................................................................................................................................
Which two hypotheses will you test against each other in the initial physical examination? Primary ........................................................................................................................................................................................ Secondary ...................................................................................................................................................................................
Is the nature of the condition severe? Yes No
Is the nature of the condition irritable? Yes No
To what point are you allowing movement to occur? Before pain To pain To end
What is your functional demonstration/re-test marker? ......................................................................................................................................................................................................
What is the primary pain mechanism of this patient’s condition? Nociceptive Peripheral neurogenic Central Autonomic Affective
To what extent will you perform a neurological exam? None required Local peripheral Lower motor neuron, upper motor neuron, limbs Lower motor neuron, upper motor neuron, limbs and cranial
What is the weighting of the following components of the problem? % Arthrogenic
Myogenic Neurogenic Inflammagenic Psychogenic Sociogenic Pathogenic Viscerogenic Osteogenic
Likely first treatment:In: ...................................................................................................................................................................................................Will: ...................................................................................................................................................................................................
Comments/cautions: ..........................................................................................................................................................................................................................................................................................................................................................................................................................
OBJECTIVE EXAMINATION PLAN
0
50
100
Arthrogenic
Radar plot
MyogenicOsteogenic
NeurogenicViscerogenic
InflammagenicPathogenic
PsychogenicSociogenic
Figure 4.1 �f0010 Clinical reasoning form.
C H A P T E R 4The principles of combined movement assessment
55
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

that should be examined in isolation. Change inthe range of movement and pain experienced inthe functional demonstration position will mostaccurately reflect overall improvement in thepatient’s impairment.
s0125Active movements
p0445Active movements should be carefully controlled bythe therapist. It is important that the patient movesto a point in range that is appropriate for their severityand nature. Simply asking a patient to extend theirback will not give adequate guidance about howacceptable it is to reproduce their pain. A patient withvery severe pain may be eager to please the therapistand extend beyond the onset of pain causing anexacerbation, or alternatively, may be fearful of
PAIVMS
Mini-treatmentReassess functional
demonstration
PPIVMS
Mini-treatmentReassess functional
demonstration
Functional demonstration
‘Posterior stretch’
Second hypothesis
‘Myogenic’
Observation
‘Hypertonic musclesipsilaterally’
Active movement
Passive movement
Starting positionPalpation
Muscle stretch
Mini-treatmentReassess functional
demonstration
Muscle contraction
Mini-treatmentReassess functional
demonstration
First hypothesis
‘Arthrogenic’
Observation
‘Hypomobile mid cx’
Active movement
Prime movementPrime combination
Passive movement
In the correct starting positionPalpation
Figure 4.2 � f0015A flow chart showing
the suggested compartmentalization
of the physical examination.
The functional demonstration is at
the head of the differentiation. Two
common differentiations are
displayed: primary arthrogenic versus
primary myogenic.
Figure 4.3 �f0020 Active extension, right rotation, showing
hypomobility of L5, L4, with movement (and skin crease)
at L3. IN: standing; DID: active extension of lumbar spine.
Segmental restriction of L4/L5 demonstrated.
S E C T I O N O N E Combined Movement Theory
56
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

movement and not move to the point that reproducessymptoms. Variability on interpretation of incom-plete commands will lead to difficulties with the reli-ability of testing. Thus, clear commands regardinghow far to move in relation to reproduction of symp-toms should be included in the commands. A decisionabout how acceptable it is to reproduce symptomswill need to have been made prior to undertaking thissection of the examination.
s0130 Degree of symptom reproductiondeemed acceptable
p0450 Having agreed on this the therapist must use clearcommands to instruct the movement conducted:
u0285 • If the agreed degree of symptom reproduction isnil, then at the completion of a combination ofmovements, the therapist’s command shouldstate clearly ‘stop before the pain starts’.
u0290 • If the agreed degree of symptom reproduction isfull, then at the completion of a combination ofmovements, the therapist’s command should be‘move as far as you possibly can’.
u0295 • If the agreed degree of symptom reproduction ispartial then at the completion of a combinationof movements, the therapist’s command shouldbe ‘stop when the pain starts’.
p0470 Good control of symptom reproduction will enablethe combination of movements needed to fullyassess the patient’s movement dysfunction. Disre-gard of this important control will lead to situationswhere the patient’s symptoms are exacerbated orunder-evaluated.
b0025 Clinical point
p0475 If the patient has severe pain at rest the examination will
be aimed at finding the movement and position that
most reduces pain and it will typically involve finding
starting positions for assessment and treatment in thequadrant opposite to the dysfunctional quadrant.
s0135 Prime movement and primecombination
p0480 Whilst observing active movements, particular atten-tion should be paid to ensuring that the patient movesareas of the spine that are impaired. Very often apatient will have developed hypermobility above a
hypomobile section of the spine. The patient can findit difficult to move the hypomobile segments as theymove at areas presenting the least resistance to move-ment and move only at the hyper-mobile segments.This can lead to a situation where symptoms are notreproduced as the symptomatic levels are not beingtested, during the test movement. False negativescan occur unless this error in clinical reasoning is con-sidered. Consequently, it is important to guidepatients to move at regions you consider likely to besymptomatic during active movement testing. SeeFigures 4.4, 4.5 and 4.6.
p0485The active movement examination is structuredto examine the movements most relevant for thepatient’s impairment. The functional demonstrationwill have provided the examiner with evidence thatcertain movements are more important in reprodu-cing the dysfunction than others. The functionaldemonstration position will justify a detailed exam-ination of the three movements that constitute it.The next stage in examining the biomechanical fea-tures of the impairment is to examine each of thethree components of the position to establish which
Figure 4.4 � f0025Active movement of the lumbar spine. Here,
movement of the stiff L4/L5, L5/S1 segment is facilitated
by fixing the sacrum with one hand whilst guiding
movement to the low lumbar spine. IN: Standing, bed
edge support, lumbar extension; DID: active right lateral
flexion, range assessment. Note the wide stance required
to ensure balance.
C H A P T E R 4The principles of combined movement assessment
57
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

two movements are the most important, and withinthese two movements, which is of primary impor-tance or ‘prime movement’.
p0490 The primary movement has an importance withinCMT in both the classification of syndromes and inselection of starting positions for treatment. Themovement itself is defined as being the movementthat either reproduces the patient’s signs and/orsymptoms most completely (when it is appropriateto do so) or most completely relieves symptoms whenthe condition is too severe to reproduce symptoms.
p0495 Having established the prime movement in oneplane it should be explored by repeating the move-ment when combined with another movement, in
another plane, which will move one side of themotion segment in the same direction.
p0500In a simplifiedmodel of spinal biomechanics exten-sion, ipsilateral rotation and ipsilateral lateral flexionwill cause the superior joint facet to move down theinferior segment’s joint facet (see Fig. 4.7). Flexion,contralateral flexion and contralateral rotation willcause the superior facet to move up the inferior seg-ment’s joint facet. For example, right rotation is thepatient’s prime movement, reproducing right-sidedneck pain. Exploring this movement by examiningright rotation in extension and extension in right rota-tion will elicit which combination is the primary com-bination. The prime combination will closely resemblethe patient’s functional demonstration.
p0505The primary combination holds a crucial place inCMT as it is the starting position where passivemovement assessment is conducted. By positioningthe spine in the position of dysfunction the additionof passive movements will be more influential inreproducing symptoms and more likely to altermovement dysfunction than if conducted in a neutralposition. Passivemovement conducted in neutral willrarely be sufficient to reproduce symptoms ade-quately.When performed in a position related to dys-function, the application of passive movement ormuscle contraction will provide valuable informationon, not only the quality and control ofmovement, butalso the effect of the test on the dysfunction.
p0510Finding the primary combination is the processby which the clinician can be sure that passivemovement testing will be the most informativeand that treatment in this position will have thequickest effect on dysfunction. A two-dimensionalequivalent would be the need to assess and treat apatient with a 10� loss of elbow extension at this
Figure 4.6 �f0035 Active, guided low cervical flexion. IN: sitting,
cervical flexion; DID: active assisted left rotation of the low
cervical spine. The patient is given feedback on where to
move.
Right rotationNeutral ExtensionRight rotation
Sensitized nociceptors C6C5
Figure 4.7 � f0040The illustration shows the selective tension
of articular and peri-articular tissue with progressive
addition of three planes of movement. A progressive
increase in anterior stretch is observed with the addition
of extension to right rotation (right rotation being coupled
with right lateral flexion).Figure 4.5 �f0030 Active movement of the low thoracic spine.
Here, movement of the stiff T10/T11 segment is facilitated
by fixing the lumbar spine with one hand whilst guiding
movement to the low thoracic spine. IN: sitting, lumbar
neutral; DID: active left rotation, low thoracic range
assessment.
S E C T I O N O N E Combined Movement Theory
58
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

position, not at 90� of elbow flexion (the equivalentof assessing in neutral).
s0140Muscle assessment
p0515 The assessment of muscular influences on the spinaldysfunction should involve an assessment of muscu-lar activity (tone) in the primary combination startingposition. The degree and location of hypertonicitycan be readily palpated in local, deep paraspinal mus-cles and the overlaying, superficial, musculature (seeFigs 4.8 and 4.9). At this point an assessment for trig-ger points (Travell & Simmons, 1998) can be
conducted, followed by an assessment of extensibil-ity (Chaitow, 2006) of the superficial phasic musclesthat have a tendency to become hypertonic in thepresence of spinal pain. See Table 4.1.
p0520During this process, hypertonic muscles are pas-sively lengthened either locally, globally or both anda temporary reflexogenic reduction in muscular activ-ity can be induced. Consequently, these tests areeffectively mini-treatments of the muscular system.
p0525The effect of this mini-treatment on the patient’sfunctional demonstration can be immediately assessed.In this way the relative contribution of the myogenicsystem can be assessed against the arthrogenic systemby mini-treating first one system and then another.See Figures 4.10 and 4.11.
s0145Passive movement andmini-treatments
p0530Having established the optimal position to inducepassive movement at the motion segments movingdysfunctionally, an assessment is made to determinewhich passive movement will be the most effective
Figure 4.8 �f0045 Palpation of anterior paraspinal muscles,
fascia and neurovasular structures. IN: supine, neutral;
DID: palpation of anterior low cervical musculature.
Special care must be taken to ensure that the flat of the
thumb is used – to avoid painful pressure.
Figure 4.9 �f0050 Palpation of upper thoracic soft tissue tone.
IN: prone, neutral; DID: soft tissue tension palpation,
upper thoracic spine. Firm pressure will be needed to pick
and work through the superficial musculature. Bands of
resistance to movement will be palpated.
Table 4.1 t0010Listing the musculature that becomes over
or under-active in common spinal pain syndromes
(Chaitow, 2006)
Short/facilitated/overrecruited
Long/inhibited/underrecruited
Occipital extensors Upper cervical flexors (rectus
capitis anterior)
Sternocleidomastoid Deep cervical flexors (longus colli)
Scalenes Low cervical extensors
(iliocostalis)
Upper trapezius Lower/middle fibres of trapezius
Levator scapulae Subscapularis
Rhomboids Serratus anterior
Pectoralis minor
Pectoralis major
Latissimus dorsi
Iliopsoas Gluteal muscles
Tensor fascia latae Abdominal muscles
Quadratus lumborum
C H A P T E R 4The principles of combined movement assessment
59
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

at reducing the dysfunction. This will involve decid-ing between accessory and physiological passivemovement and between particular combinations ofboth. One method of deciding between two likelytreatment options is to compare the immediateeffectiveness of using the treatments. Even a shortperiod of treatment, if applied in the correct start-ing position, will have an immediate effect on move-ment dysfunction. The patient will be able todiscriminate between the treatment effects and tellyou which treatment to use!
p0535Mini-treatment requires a degree of skill to per-form. Whilst the treatment is of a short duration,in order to fit into the assessment process withoutbecoming too time consuming, it must be enoughof a ‘dose’ of treatment to evoke a change in muscleactivity and/or joint mobility. Thus, the examinerneeds the palpatory skill to be able to tell whenthese features have subtly changed. With practicethe skilled manual therapist can be as confident indiscriminating this change in mobility as they havein their ability to discriminate between a normal orhypomobile joint on initial assessment.
p0540If we really are striving to provide treatment thatis the most efficacious option we must prove thatthe specific treatment we are proposing is indeedmore effective at reducing the dysfunction thanthe next most likely option. Testing one treatmentagainst another is something we do whilst treatingpatients, however, the incorporation of this princi-ple during the assessment process is of particularimportance with the CMT approach.
s0150Assessing for the suitability ofmanipulative thrust techniques
p0545Local movement impairment, specific to one or twospinal segments, can present with hypomobility inthe contralateral side glide that accompanies ipsilat-eral lateral flexion and rotation. Acute musclespasm or long-standing movement impairment canlead to a perceptible change in the passive range ofcontralateral side glide during ipsilateral lateral flex-ion. When visualizing the quality of resistance topassive movement the movement diagram, devel-oped by Maitland (1986) is useful. When passivelyinducing lateral flexion at one spinal segment a per-ception of the profile of resistance to movement canbe drawn. Profiles of resistance that are short inrange represent a ‘crisp’ end feel, whilst a long rangeof resistance profile will feel ‘bouncy’. Finally amovement that has no range of resistance andcomes to a complete stop immediately resistanceis felt, will feel ‘solid’. See Figure 4.12. Segmentsthat do not have this ‘crisp’ profile do not generallycavitate in response to a high velocity thrust.
p0550Thus, unless the therapist assesses lateral flexionand its associated contralateral side glide the ratio-nale for choosing a manipulation technique over amobilization technique is less clear. The assessmentof accessory glides does not afford the informationto make this judgement. The assessment of
Figure 4.11 �f0060 Post-isometric relaxation technique for the
right, anterior paraspinal muscles. IN: supine, neutral
extension; DID: isometric contraction resisting extension and
right rotation. The patient performs an isometric contraction
in response to AP pressure. Contraction of the right anterior
musculature is produced. See video clip number 4
Figure 4.10 �f0055 Post-isometric relaxation technique for the
right, posterior paraspinals. IN: sitting, thoracic flexion;
DID: isometric contraction resisting left rotation of T1 on
T2. The patient is told to ‘Don’t let me win’ as the neck is
moved towards more flexion and rotation. The patient will
contract the extensors and right rotators. An isometric
contraction can be held for 6–10 seconds.
S E C T I O N O N E Combined Movement Theory
60
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7
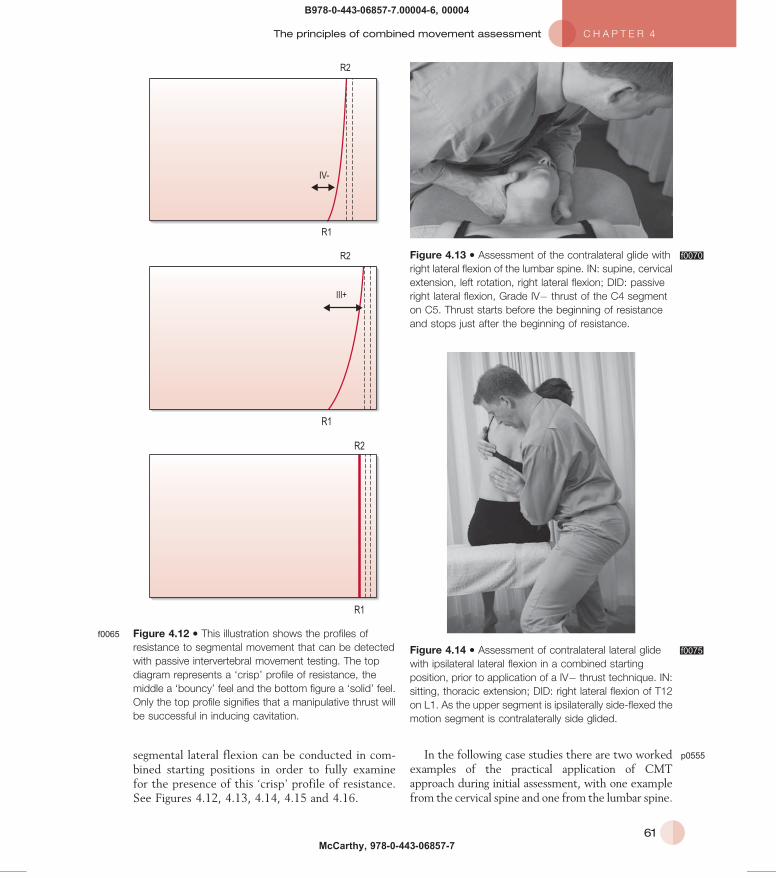
segmental lateral flexion can be conducted in com-bined starting positions in order to fully examinefor the presence of this ‘crisp’ profile of resistance.See Figures 4.12, 4.13, 4.14, 4.15 and 4.16.
p0555In the following case studies there are two workedexamples of the practical application of CMTapproach during initial assessment, with one examplefrom the cervical spine and one from the lumbar spine.
IV-
R1
R2
R1
R2
III+
R1
R2
Figure 4.12 �f0065 This illustration shows the profiles of
resistance to segmental movement that can be detected
with passive intervertebral movement testing. The top
diagram represents a ‘crisp’ profile of resistance, the
middle a ‘bouncy’ feel and the bottom figure a ‘solid’ feel.
Only the top profile signifies that a manipulative thrust will
be successful in inducing cavitation.
Figure 4.13 � f0070Assessment of the contralateral glide with
right lateral flexion of the lumbar spine. IN: supine, cervical
extension, left rotation, right lateral flexion; DID: passive
right lateral flexion, Grade IV� thrust of the C4 segment
on C5. Thrust starts before the beginning of resistance
and stops just after the beginning of resistance.
Figure 4.14 � f0075Assessment of contralateral lateral glide
with ipsilateral lateral flexion in a combined starting
position, prior to application of a IV� thrust technique. IN:
sitting, thoracic extension; DID: right lateral flexion of T12
on L1. As the upper segment is ipsilaterally side-flexed the
motion segment is contralaterally side glided.
C H A P T E R 4The principles of combined movement assessment
61
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

b0030b0030 CERVICAL SPINE CASE STUDY
s0155 INITIAL INTERVIEW
s0160 Symptomology
p0560 A 22-year-old female sought treatment for pain in the rightcervical spine and right shoulder. The pain was located in thelower cervical spine and referred into the right shoulderacross the right supra-scapula fossa (Fig. 4.17). The pain wasnot radicular in quality but severe (8/10). There was nosuggestion of an upper motor neuron lesion and no indicationof other red flags. There were no features suggestive ofsegmental cervical instability or shoulder derangement. Therewas no history of cervical locking, catching or weakness.There was no headache.
s0165 Relevant history
p0565 Symptoms developed over a 6-day period following a mild,rear shunt whiplash injury, a week previously.
s0170 Behaviour of symptoms
p0570 Pain was reproduced with low cervical flexion and left lateralflexion. Sitting with the neck in this position reproducedsymptoms within 2 minutes. The symptoms were easedimmediately, by positioning the lower cervical spine inextension and right lateral flexion. No latent pain was exhibited.
s0175 Diurnal pattern
p0575 There was no stiffness in the cervical spine in the morning.Shoulder pain developed in the evening. Sleep was notdisturbed.
s0180 Special questions
p0580 The patient’s general health was good. There was noweight loss, no dizziness, no dysphagia, no dysarthria,
no diplopia, no raised blood pressure, and no symptoms ofcervical artery dysfunction. Radiographs of the cervicalspine were normal. The patient was not currently takingany anticoagulant or steroid therapy and had received nobenefit from anti-inflammatory medication. There was nohistory of locking, clunking or giving way of the shoulder,with no history of trauma.
p0585See the completed planning sheet in Figure 4.18.
Figure 4.15 �f0080 Assessment of the contralateral glide
associated with ipsilateral flexion of the low lumbar spine.
IN: left side-lying, flexion; DID: right lateral flexion with left
side glide at the motion segment. As the lumbar spine is
laterally flexed, firm pressure is applied towards the bed.
Figure 4.16 � f0085Assessment of resistance profile of
contralateral glide in a combined position used to induce
cavitation. IN: flexion, left lateral flexion, right rotation; DID:
right rotation combined with contralateral glide
downwards. The combined starting position for a Grade
IV� rotation, thrust technique.
Figure 4.17 � f0090Cervical spine case study – pain chart.
S E C T I O N O N E Combined Movement Theory
62
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

List your hypotheses for the nature of the condition. 1. .......................... Posterior facet capsule sprain ......................................................................................................................... 2. .......................... Posterior paraspinal strain .............................................................................................................................. 3. .......................... Posterior annular disc sprain ...........................................................................................................................
Which two hypotheses will you test against each other in the initial physical examination? Primary ................. Articular predominance .................................................................................................................................. Secondary ............ Myogenic predominance .................................................................................................................................
Is the nature of the condition severe? Yes No
Is the nature of the condition irritable? Yes No
To what point are you allowing movement to occur? Before pain To pain To limit
What is the functional demonstration/primary re-test marker? .............................. Flexion contralateral, lateral flexion quadrant ...............................................................................................
What is the primary pain mechanism of this patient’s condition? Nociceptive Peripheral neurogenic Central Autonomic Affective
To what extent will you perform a neurological exam? None required Local peripheral Lower motor neuron, upper motor neuron, limbs Lower motor neuron, upper motor neuron, limbs and cranial
What is the weighting of the following components of the problem?
% Arthrogenic 50
Myogenic 40 Neurogenic 1 Inflammagenic 2 Psychogenic 1 Sociogenic 1 Pathogenic 1 Viscerogenic 1 Osteogenic 3
Likely first treatment:In: Extension, right lateral flexion quadrant .....................................................................................................................................Will: Anterior capsular stretch, large amplitude movement, in resistance (Grade III) ........................................................................
Comments/cautions: Pain relief approach, progressing to a stretch of the tissues driving the nociceptive pattern of presentation ....................................................................................................................................................................................................................................................
OBJECTIVE EXAMINATION PLAN
0
50
100
Arthrogenic
Radar plot
MyogenicOsteogenic
NeurogenicViscerogenic
InflammagenicPathogenic
PsychogenicSociogenic
Figure 4.18 �f0095 Objective examination plan for the cervical spine.
C H A P T E R 4The principles of combined movement assessment
63
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

s0185PHYSICAL EXAMINATION
s0190Observation
p0590There was no atrophy of the cervical musculature. Therewas an increase in muscle tone of the rightsternocleidomastoid, upper fibres of trapezius and levatorscapula and right scalenes.
s0195Active movement
p0595Pain was reproduced earliest in range with left lateralflexion. Restriction to flexion was apparent at the C5/C6level. Pain was reproduced further into range with flexionthan with left lateral flexion. Restriction to movementwas most obvious in the mid cervical region. SeeFigure 4.19.
Prime movement = left lateral flexionPrime combination = left lateral flexion followed by flexion. 3/4 full range
Right-sided cervical and shoulder painSevere
Figure 4.19 �f0100 Box diagram showing the prime
combination for the patient.
PAIVMS
Mini-treatmentEffect on functional
demonstration40%
PPIVMS
Mini-treatmentEffect on functional
demonstration10%
Functional demonstration
Flexion, left lat flex
Second hypothesis
Posterior musculaturestrain
Observation
Muscle atrophyHypertrophyHypotonicityHypertonicity
Active movement
Control and timing ofmuscles during movement
Passive movement
Starting positionPalpation
Local stretch
Mini-treatmentEffect on functional
demonstration0%
Muscle contraction
Mini-treatmentEffect on functional
demonstration10%
First hypothesis
Posterior facet capsulesprain
Observation
Postural positioningmalalignment
Active movement
Prime movementPrime combination
Passive movement
Starting positionPalpation
The technique that alters movement and muscle tone mostwith mini-treatment is the initial treatment choice
Figure 4.20 � f0105Flow chart of differential
examination for the cervical spine.
S E C T I O N O N E Combined Movement Theory
64
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

s0200 Passive physiological intervertebral movement(PPIVMS)
p0600 Due to the severity, the examination was undertaken in rightlateral flexion and extension (posterior structures off stretch)to establish the movement that most reduced pain anddysfunction. Right lateral flexion induced the greatestincrease in movement and reduction in muscle tone.
A short passive treatment, using this right lateral flexion of
C5 on C6 reduced the pain produced by the functional
demonstration by 10%.
s0205 Passive accessory intervertebral movement(PAIVMS)
p0610 Due to the severity, examination was undertaken in rightlateral flexion and extension (posterior structures off stretch)to establish the movement that most reduced pain anddysfunction. Anterior pressure (AP) on C5 induced the
greatest increase in movement and reduction in muscletone (greater than induced by AP movement of C4 or C6).
A short passive treatment, using this accessory movement
reduced the pain produced by the functional demonstration
by 40%.
s0210Muscular assessment
p0620In right lateral flexion and extension due to severity ofpain, palpation of musculature revealed hypertonicity ofdeep paraspinals (C4 to C6) and hypertonicity of theregion’s phasic muscles. No trigger points were detected.
Palpation and length assessment of the levator scapulae,
scalenes, upper fibres of trapezius and sternocleidomastoid
did not alter the functional demonstration.
p0630See Figure 4.20.
b0035b0035 LUMBAR SPINE CASE STUDY
s0215 INITIAL INTERVIEW
s0220 Symptomology
p0635 A 45-year-old male sought treatment for pain in the rightback and buttock (Fig. 4.21). The pain was not radicular inquality and not severe (4/10). There was no suggestion ofan upper motor neuron lesion and no indication of otherred flags. There were no features suggestive of segmentallumbar instability or disc derangement. There was nohistory of lumbar locking, catching or weakness and therewas no cauda equina syndrome.
s0225Relevant history
p0640Symptoms developed over a 6-month-period with nohistory of trauma.
s0230Behaviour of symptoms
p0645Pain was reproduced with low lumbar extension and rightlateral flexion (whilst arching his back to put on his coat).Standing reproduced symptoms within 20 minutes.Walking reproduced symptoms in 30 minutes. Thesymptoms were eased, immediately, by positioning theback in flexion, either by sitting or leaning over in standing.Pain was also eased by crossing the right leg over the left,in sitting. No latent pain was exhibited. Pain was alsoexperienced whilst turning over in bed.
s0235Diurnal pattern
p0650There was less than 30 minutes of stiffness in the back inthe morning. Buttock pain developed in the evening. Sleepwas not disturbed.
s0240Special questions
p0655His general health was good. There was no weight loss, nonight sweats or fever, no constant night pain (worse thanduring the day), no raised blood pressure, no symptomsof vascular stenosis or peripheral vascular disease. Nohistory of cancer. The patient was not currently taking anyanticoagulant or steroid therapy and had received nobenefit from anti-inflammatory medication.
p0660See the completed planning sheet in Figure 4.22.Figure 4.21 �f0110 Lumbar spine case study – pain chart.
C H A P T E R 4The principles of combined movement assessment
65
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

List your hypotheses for the nature of the condition. 1. .......................... Superior facet capsule source ......................................................................................................................... 2. .......................... Sacro-iliac joint source ................................................................................................................................... 3. .......................... Anterior paraspinal muscle source .................................................................................................................
Which two hypotheses will you test against each other in the initial physical examination? Primary ................. Lumbar articular drive (75%) ........................................................................................................................ Secondary ............ Sacro-iliac articular drive (25%) ...................................................................................................................
Is the nature of the condition severe? Yes No
Is the nature of the condition irritable? Yes No
To what point are you allowing movement to occur? Before pain To pain To limit
What is the functional demonstration/primary re-test marker? .............................. Extension, ipsilateral lateral flexion quadrant ...............................................................................................
What is the primary pain mechanism of this patient’s condition? Nociceptive Peripheral neurogenic Central Autonomic Affective
To what extent will you perform a neurological exam? None required Local peripheral Lower motor neuron, upper motor neuron, limbs Lower motor neuron, upper motor neuron, limbs and cranial
What is the weighting of the following components of the problem? % Arthrogenic 70
Myogenic 20 Neurogenic 1 Inflammagenic 4 Psychogenic 1 Sociogenic 1 Pathogenic 1 Viscerogenic 1 Osteogenic 1
Likely first treatment:In: Extension, right lateral flexion quadrant ....................................................................................................................................Will: Superior capsular stretch, large amplitude movement, in resistance (Grade III) ........................................................................
Comments/cautions: Pain relieving mobilization, combined with a stretch of the tissues driving the nociceptive pattern of presentation ................................................................................................................................................................................................................
0
50
100
Arthrogenic
Radar plot
MyogenicOsteogenic
NeurogenicViscerogenic
InflammagenicPathogenic
PsychogenicSociogenic
OBJECTIVE EXAMINATION PLAN
Figure 4.22 �f0115 Objective examination plan for the lumbar spine.
S E C T I O N O N E Combined Movement Theory
66
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

s0245 PHYSICAL EXAMINATION
s0250 Observation
p0665 There was no atrophy of the lumbar musculature. Therewas an increase in muscle tone of the right erectorespinae, quadratus lumborum and piriformis.
s0255 Active movement
p0670 Pain was reproduced earliest in range with rightlateral flexion. Restriction to extension was apparent atthe L4/L5 level. Pain was reproduced further into rangewith extension than with right lateral flexion. SeeFigure 4.23.
s0260 Passive physiological intervertebral movement(PPIVMS)
p0675 Right lateral flexion, in extension of L4 on L5, inducedthe greatest increase in movement and reduction inmuscle tone, when compared with movement at L3/L4and L5/S1.
A short passive treatment, using this right lateral flexion of
L4 on L5 reduced the pain produced by the functional
demonstration by 50%.
s0265 Passive accessory intervertebral movement(PAIVMS)
p0685 In right lateral flexion and extension, posterior pressure(unilateral posterior-anterior angled caudad) on L4 inducedthe greatest increase in movement and reduction in muscletone, when compared to the same accessory movementapplied to L3 or L5.
A short passive treatment, using this accessory movement
reduced the pain produced by the functional demonstration
by 20%.
s0270Passive movement of the sacroiliac joint (SIJ)
p0695In right lateral flexion and extension PA pressure on the rightapex of the sacrum (encouraging nutation) reproducedsymptoms and was the most restricted sacral glide, whencompared to the response of moving the other three cornersof the sacrum.
A short passive treatment, using this passive movement
reduced the pain produced by the functional demonstration
by 10%.
p0705See Figure 4.24.
PAIVMS
Mini-treatmentEffect on functional
demonstration20%
PPIVMS
Mini-treatmentEffect on functional
demonstration50%
Functional demonstration
Extension, right lat flex
Second hypothesis
Restricted nutation of theright SIJ
Observation
Postural positioningmalalignment
Active movement
SamePrime movement
Prime combination
Passive movement
SameStarting position
Palpation
SIJ passive movement
Mini-treatmentEffect on functional
demonstration10%
First hypothesis
Superior facet capsulesprain
Observation
Postural positioningmalalignment
Active movement
Prime movementPrime combination
Passive movement
Starting positionPalpation
The technique that most alters movement and painresponse with mini-treatment is the initial treatment choice
Figure 4.24 � f0125Flow chart of differential examination for the
lumbar spine.
Prime movement = right lateral flexionPrime combination = right lateral flexion followed by extension. 3/4 full range
Right-sidedlumbar and buttock painNot severe
Figure 4.23 �f0120 Box diagram showing the prime
combination for the patient.
C H A P T E R 4The principles of combined movement assessment
67
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7

References
Chaitow, L., 2006. Muscle energytechniques. Elsevier Health Sciences,Oxford.
Gibbons, P., Tehan, P., 2001a. Patientpositioning and spinal locking forlumbar spine rotation manipulation.Man. Ther. 6 (3), 130–138.
Gibbons, P., Tehan, P., 2001b. Spinalmanipulation: indications, risks andbenefits. Journal of Bodywork &Movement Therapies 5 (2), 110–119.
Grieve, G.P., 1988. Common vertebraljoint problems. ChurchillLivingstone, New York,pp. 525–526.
Grieve, G.P., 1991. Mobilization of thespine. A Primary handbook ofClinical Method. ChurchillLivingstone, Edinburgh.
Kerry, R., Taylor, A.J., Mitchell, J., et al.,2008a. Manual therapy and cervicalarterial dysfunction, directions for thefuture: a clinical perspective. TheJournal of Manual & ManipulativeTherapy 16 (1), 39–48.
Kerry, R., Taylor, A.J., Mitchell, J., et al.,2008b. Cervical arterial dysfunctionand manual therapy: a criticalliterature review to inform
professional practice. Man. Ther. 13(4), 278–288.
Maitland, G., 1986. Vertebralmanipulation. Elsevier HealthSciences, Sydney.
Travell, Simmons, 1998. TravellSimons’ myofascial pain anddysfunction: the trigger pointmanual, second ed. LippincottWilliams & Wilkins, San Francisco.
S E C T I O N O N E Combined Movement Theory
68
B978-0-443-06857-7.00004-6, 00004
McCarthy, 978-0-443-06857-7