Chapter 6 Disciplinary Actions, Sanctions, and Malpractice ...
23
Chapter 6 Disciplinary Actions, Sanctions, and Malpractice Compensation
Transcript of Chapter 6 Disciplinary Actions, Sanctions, and Malpractice ...

Chapter 6
Disciplinary Actions,Sanctions, and
Malpractice Compensation

CONTENTS
PageIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .“. ””121Disciplinary Actions by State Medical Boards . .............................122
Reliability of the Indicator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .........123Validity of the Indicator . . . . . . . . . . . . . . . . . . . . . . . . ....................123Feasibility of Using the Indicator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..126
Sanctions Recommended by Peer Review Organizations and Imposedby HAS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126
Reliability of the Indicator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. ...127Validity of the Indicator . . . . . . . . . . . . . . . . . . . . . . . ...........130Feasibility of Using the Indicator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...132
Malpractice Compensation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ........133Reliability of the Indicator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ....134Validity of the Indicator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. ....134Feasibility of Using the Indicator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...137
Conclusions and Policy Implications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 138Disciplinary Actions by State Medical Boards . ...........................138Sanctions Recommended by PROs and Imposed by HHS . .................139Malpractice Compensation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ........140Combinations of Indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..141
FiguresFigure Page
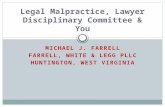
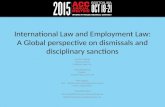
6-1. Overview of the PRO/HHS Sanction Process for Substantial Violations . 1286-2. Overview of the pRO/HHS Sanction Process for Gross and Flagrant Violations 128
TablesTable Page6-1. Physician Disciplinary Actions by Skateboards, 1986 . . . . . . . . . . . . . . . . . 1246-2. Interjudge Consistency in Complex Human Judgments . . . . . . . . . . . . . . . 135

Chapter 6
Disciplinary Actions, Sanctions,and Malpractice Compensation
INTRODUCTION
Federal and State laws and regulations and pri-vate sector medical entities have established manymethods to discipline and sanction errant mem-bers of the medical profession. This chapter evalu-ates as possible indicators of the quality of medi-cal care three such activities:
●
●
●
disciplinary actions taken by State medicalboards, ]
sanctions recommended by utilization andquality control peer review organizations(PROS) and imposed by the U.S. Departmentof Health and Human Services (HHS), andmalpractice compensation, particularly courtawards.
Disciplinary actions by State medical boards,PRO/HHS sanctions, and malpractice compen-sation, either separately or in conjunction witheach other and other indicators, may have the po-tential to identify physicians who do not followaccepted standards of care. Those physicians whoare disciplined, sanctioned, or successfully suedfor malpractice may actually provide substand-ard care. On the other hand, not all physicianswho provide substandard care are disciplined orsuccessfully sued. Studies of avoidable injuriesindicate that the universe of avoidable adverseoutcomes may be significantly greater than thenumber of disciplinary actions, sanctions, andmalpractice suits (152,595). These studies suggesta large number of poor-quality physicians are notidentified or penalized, thereby pointing to the in-effectiveness of existing systems to identify allthose individuals providing poor-quality care.
This chapter uses procedures somewhat differ-ent from those described in appendix C to evalu-ate the reliability and validity of disciplinary ac-
I In the following discussion, State licensing bodies and State dis-c]plinar}~ bodies will be called State medical boards, although theirofficial t i t les as we] 1 as their organizational loci var}~ among States,
tions, sanctions, and malpractice compensationas indicators of the quality of care. There are tworeasons for modifying the procedures describedin appendix C when considering these three indi-cators. First, the procedures described in appen-dix C apply to a systematic synthesis of the liter-ature, and studies that examine the causalrelationship between any of the three indicatorsdiscussed in this chapter and the quality of careare not available. In the absence of researchstudies, this chapter uses deductive reasoning fromthe indirect evidence of descriptive informationto provide some insight into the reliability andvalidity of disciplinary actions, sanctions, andmalpractice compensation as indicators of quality.
The second reason for modifying the proce-dures outlined in appendix C is that the three po-tential indicators discussed in this chapter are es-sentially legal processes that rely on judgment andhave little or no science base. 2 For purposes ofthis chapter, the term reliability refers to con-sistency of the decisions made by a legal body(e.g., disciplinary actions taken by State medicalboards). The term validity refers to the scope ofthe decisions made by a legal body and the ca-pacity of the decisions to actually measure qual-ity. Evidence on reliability and validity is derivedfrom examining the structure of the legal bodies,the grounds for taking actions, the proceduresused in taking actions, and the types of actionstaken. In the case of disciplinary actions by Statemedical boards and PRO/HHS sanctions, judi-cial review of the actions is also examined.
A possible confounding issue in OTA’S analy-sis is that the reliability and validity of discipli-nary actions, PRO/HHS sanctions, and malprac-
2 Rel iabilit y and validity, as described in app. C, are concepts usedin applied social science and are not traditionally associated w’]thlegal systems.
127

122
tice compensation as indicators of the quality ofmedical care depend to a large extent upon peerreview. 3 Differences in criteria used by peer phy-sicians, even experts, in making decisions aboutmedical diagnosis and treatment are well docu-mented (71,185). Such differences may havetroublesome implications for the reliability and
3State medical boards use the expert opinion of their physicianmembers to interpret and apply the vague language often found inlegislation governing license discipline. Furthermore, “expert” peerstestify when physicians are brought up for hearings. The entire sanc-tion process within PROs depends upon peer opinion, from the origi-nal identification of a possible violation to succeeding reviews ofthe violation. Peer review is also an important part of malpracticecases that are heard in court. “Expert” peers testify to the standardof care that can be applied to the case and whether the defendantmet the standard.
validity of expert peer opinion in disciplinary ac-tions taken by State medical boards, sanctions rec-ommended by PROS and imposed by HHS, andmalpractice compensation.
Analyses of the reliability and validity of dis-ciplinary actions, sanctions, and malpractice com-pensation as indicators of the quality of care arepresented below, Also presented are analyses ofthe feasibility of using each indicator. The finalsection of this chapter draws conclusions aboutthe current usefulness of the actions, used singlyand together, as quality indicators; suggests meth-ods for improving the reliability and validity ofthe three actions as quality indicators; and dis-cusses current and future means of disseminatinginformation about the three.
DISCIPLINARY ACTIONS BY STATE MEDICAL BOARDS
The legal authority for licensing physicians topractice medicine and for restricting or revokinglicenses rests with the States. In most States, thesame body that grants licenses to applicants thatit has determined are qualified to practice medi-cine also disciplines physicians who it has decidedare unfit to continue practice (32,260). All Statemedical boards have the authority to revoke orsuspend a physician’s license. Other disciplinaryactions include probation, limitations, fines, repri-mands, letters of censure, letters of concern, andcollecting costs of proceedings (206). The generalgrounds for disciplinary actions are unprofes-sional conduct or professional incompetence (32).The medical practice act of each State mandatesspecific grounds, such as incorrect drug prescrip-tion and substance abuse, for disciplining phy-sicians.
Medical licensure is intended to grant the priv-ilege of practicing medicine to individuals who areof good moral character and are competent toprovide safe care to the public (70 Corpus JurisSec. 19), but it does not ensure continuing com-petence—an important issue in light of changingmedical knowledge and techniques. The purposeof disciplinary actions by State medical boardsis to “protect the public against unfit practition-ers” (7o Corpus Juris Sec. 35). State medicalboards, which historically have been very con-
servative in censuring physicians (208), have in-creased their activity in recent years. Disciplinaryactions increased from 1,540 in 1984 to 2,108 in1985 (91) to 2,302 in 1986 (240). Nonetheless, thepercentage of practicing physicians disciplined in1986 (0.50 percent) 4 is significantly less than the5 to 15 percent of physicians that some authorshave hypothesized to be professionally incompe-tent to practice (169,208). Although the effective-ness of State medical boards in taking disciplinaryactions is an important quality concern, the morespecific intent of this chapter is to evaluatewhether the disciplinary actions taken by Statemedical boards are good indicators of the quali-ty of care.
Disciplinary actions taken by State medicalboards are worth examining as a measure of qual-ity, because they have face validity for averageconsumers. An average consumer would expectthat limiting or withdrawing a physician’s licenseto practice medicine indicates that the physicianis professionally incompetent and would be con-cerned about using the physician for health care.
‘There were 462,126 physicians providing patient care in 1986 (35),‘In most cases, revoking a physician’s Ii( enw prohlbit~ him or
her from practicing medicine. There have been well-publicized in-
stances in which physicians whose licenses wore revohed In one Stat(’continued to provide medical care in other States where thc,y heldlicenses. Public and private ctforts h~ve been working to (’lim inat(this problem.

123
Reliability of the Indicator
Nationwide consistency of disciplinary actionsby State medical boards is not to be expected, be-cause the granting and limitation or withdrawalof medical licenses are State responsibilities. Theproportion of physicians who have had theirlicenses revoked or modified varies greatly amongStates (see table 6-l). Differences in medical per-formance, legal impropriety, and inaccuracy ofreporting among the States can account for onlya small fraction of the variation in the propor-tion. A greater part of the variation is attributa-ble to differences in State laws and regulation,and, perhaps, the intensity with which State med-ical boards engage in disciplinary activities (499).
A State medical board’s discipline of similarcases may differ because of factors that are notrelated to the quality of care. Important witnessessometimes fail to appear, physicians’ lawyers varyin expertise, and aggravating and mitigating fac-tors, which are not defined in statute or case lawbut vary from case to case, must be weighed indisciplinary decisions (389). Consistency in deci-sions is particularly difficult to achieve in typesof cases where physicians disagree about whatconstitutes acceptable practice. In some States(e.g., Colorado and Connecticut), a threat t. con-sistency is that more than one body is involvedin disciplinary activities (206).
In general, the reliability of disciplinary actionsas an indicator of quality within a State dependson the individual State. An investigation of 24States by the Office of the Inspector General ofHHS found “inconsistencies in the type of discipli-nary actions taken in relation to the charges andeven in the meanings of the different types of ac-tions” (361), both among and within States.Whether disciplinary actions in other States areerratic, and if so, to what extent, is not known.
For the most part, the consistency of discipli-nary actions taken within a State depends on theprecision of the language specifying the groundsfor discipline. The more vague the language, thegreater the possibility for differing interpretationsand applicability. Consistency of such actions isalso related to the specific violation, since mostStates have precise grounds for some violationsand ambiguous grounds for others. Most State
medical practice acts list specific grounds for in-fractions dealing with drug prescription and use,fraud, and other violations (280,720). on theother hand, few of the States that specify in-competence in the practice of medicine or sub-standard practice as grounds for disciplinaryactions define incompetence precisely. Illinois’Professions and Occupations Code defines “pro-fessional incompetence as manifested by poorstandards of care” (111). In the face of such in-definiteness, consistency is difficult, and applica-tion of the rule requires a case-by-case interpre-tation of the applicable standard of practice.
A State medical board’s composition and oper-ating style also enter into the consistency of itsdecisions. Particularly if the grounds for discipli-nary actions are vague, a State medical boardcould be arbitrary and capricious in its adherenceto law and regulations and allow extraneous facts,such as the race, religion, or community stand-ing of physicians, to enter into their decisions. Inaddition, most boards are voluntary and worklong hours on difficult issues with little financialreward. Extensive caseloads are common (658),and the medical boards are usually limited in theirdisciplinary performance by staff and funds (361).As a result, the reliability of their decisions maybe compromised.
In addition to taking formal disciplinary actionsagainst physicians, State medical boards take in-formal disciplinary actions (91). The rationale andprocedures for informal actions differ among theStates. Boards take several times more informalthan formal actions (91). In some States, infor-mal disciplinary actions are taken because of alack of investigatory resources and the backlogof unheard cases that most boards currently face(658). In other States, informal actions are usedas a means of educating physicians. Even infor-mal actions are often serious (91). The propen-sity for inconsistency among such actions couldbe high, because informal actions are confiden-tial. Such actions could be used selectively toavoid disciplining some physicians and not others.
Validity of the Indicator
About one-half of the formal disciplinary ac-tions taken against physicians by State medical

124
Table 6-l.— Physician Disciplinary Actions by State Boards, 1986a
O t h e rL i c e n s e L i c e n s e regulatory
revocat ion Probation suspension action Total
Alabama . . . . . . . . . . . . . . . . . . . . . . .Alaska . . . . . . . . . . . . . . . . . . . . . . . . .Arizona . . . . . . . . . . . . . . . . . . . . . . . .Arizona b . . . . . . . . . . . . . . . . . . . . . . .Arkansas . . . . . . . . . . . . . . . . . . . . . .California . . . . . . . . . . . . . . . . . . . . . .California b . . . . . . . . . . . . . . . . . . . . .Colorado . . . . . . . . . . . . . . . . . . . . . .Connecticut . . . . . . . . . . . . . . . . . . . .District of Columbia. . . . . . . . . . . . .Delaware . . . . . . . . . . . . . . . . . . . . . .Florida . . . . . . . . . . . . . . . . . . . . . . .Florida b . . . . . . . . . . . . . . . . . . . . . . .Georgia . . . . . . . . . . . . . . . . . . . . . . . .Guam . . . . . . . . . . . . . . . . . . . . . . . . .Hawaii . . . . . . . . . . . . . . . . . . . . . . . .Idaho . . . . . . . . . . . . . . . . . . . . . . . . .Illinois . . . . . . . . . . . . . . . . . . . . . . . .Indiana . . . . . . . . . . . . . . . . . . . . . . . .lowa . . . . . . . . . . . . . . . . . . . . . . . . . .Kansas . . . . . . . . . . . . . . . . . . . . . . .Kentucky . . . . . . . . . . . . . . . . . . . . . .Louisiana . . . . . . . . . . . . . . . . . . . . . .Maine . . . . . . . . . . . . . . . . . . . . . . . . .Maryland . . . . . . . . . . . . . . . . . . . . . .Massachusetts . . . . . . . . . . . . . . . . .Michigan . . . . . . . . . . . . . . . . . . . . . .Michigan b . . . . . . . . . . . . . . . . . . . . .Minnesota . . . . . . . . . . . . . . . . . . . . .Mississippi . . . . . . . . . . . . . . . . . . . .Missouri . . . . . . . . . . . . . . . . . . . . . .Montana ......, . . . . . . . . . . . . . . . .Nebraska . . . . . . . . . . . . . . . . . . . . . .Nevada . . . . . . . . . . . . . . . . . . . . . . . .FJevadab . . . . . . . . . . . . . . . . . . . . . . .New Hampshire . . . . . . . . . . . . . . . .New Jersey . . . . . . . . . . . . . . . . . . . .New Mexico . . . . . . . . . . . . . . . . . . .New Mexico . . . . . . . . . . . . . . . . . . .New York .....,... . . . . . . . . . . . .North Carolina . . . . . . . . . . . . . . . . .North Dakota . . . . . . . . . . . . . . . . . . .Ohio . . . . . . . . . . . . . . . . . . . . . . . . . .Oklahoma . . . . . . . . . . . . . . . . . . . . . .Oklahoma . . . . . . . . . . . . . . . . . . . .Oregon . . . . . . . . . . . . . . . . . . . . . . . .Pennsylvania. . . . . . . . . . . . . . . . . . .Pennsylvania b . . . . . . . . . . . . . . . . . .Puerto Rico . . . . . . . . . . . . . . . . . . . .Rhode Island . . . . . . . . . . . . . . . . . . .South Carolina . . . . . . . . . . . . . . . . .South Dakota . . . . . . . . . . . . . . . . . .Tennessee . . . . . . . . . . . . . . . . . . . . .Tennessee b . . . . . . . . . . . . . . . . . . . .Texas . . . . . . . . . . . . . . . . . . . . . . .Utah . . . . . . . . . . . . . . . . . . . . . . . . . .Vermont . . . . . . . . . . . . . . . . . . . . . . .Virgin Islands ., . . . . . . . . . . . . . . . .Virginia State . . . . . . . . . . . . . . .Washington . . . . . . . . . . . . . . . . . . . .Washington b . . . . . . . . . . . . . . . . . . .West Virginia. . . . . . . . . . . . . . . . . . .West Virginia . . . . . . . . . . . . . . . . . .Wisconsin . . . . . . . . . . . . . . . . . . . .Wyoming . . . . . . . . . . . . . . . . . . . . . .
40601
3414572
224
16062
109
162
11041
253032
3211200
1030
6412
124
30291026160
28400
150080
230
41
:1
693
10220
234
42012
2518
7275251
“oo
223603101
1710
8313
12015
119
760050309
1200
18806020
01224
180
10200
303
15010
3830
:4805
1611
553010
:o
2200
2010
14307
11801501041106305010
7055161143
18840
1177
35021
4738
92215
55
15822
111648
01300
4500
3125
35116
32034
404
108
110
311760
5122
070
200
152
672417
1645
321713
2192
18108
010
5120
953529371811265016
7412486
25701
9440
19851
510937
4486119
07
269
210
7234
70
9033
0260
460
Total for bear. . . . . . . . . . . . . . . . . 458 528 335 981 2,302aExcept where designated, all boarcfs take disciplinzwy actions against both allopathic physicians (M.Ds) and osteopathic @wkians@D s)bTtlis board takes disciplinary actions against osteopathic physicians (OD.s) onlY
SOURCE B Galusha and DG Breadon, “Official 1966 Federation Summary of Reported Dlsciphnary ActIons.” Federatiorr Bulletin 75(2)41.46, 1988

125
boards are on the grounds of inappropriate writ-ing of prescriptions. Such infractions are the eas-iest to prove because of the exactness of prescrip-tion laws (658). Inappropriate prescribing and aphysician’s personal drug or alcohol abuse are thegrounds for three-fourths or more of the discipli-nary actions taken by State boards. Convictionfor felony and fraud is among the most commonof the remaining grounds for license discipline.A relatively small number of disciplinary actionsare based on incompetence—the ground for dis-cipline that would most clearly indicate poor qual-ity of care.
If incompetence is strictly interpreted as theonly violation that is a quality violation, discipli-nary actions by State medical boards would notbe a valid indicator of the quality of the medicalcare. A more liberal interpretation of incompe-tence to include inaccurate drug prescribing anddrug and alcohol abuse is reasonable. The statis-tics just cited on types of violations present anincomplete picture of the importance of incompe-tence in disciplinary procedures. In addition, fewmedical practice acts identify incompetence asgrounds for discipline, and the language of theacts that do is usually vague and difficult to in-terpret (694).6 In addition, obtaining “clear andconvincing evidence, ” of incompetence in mostStates is extremely difficult, time-consuming, andcostly (239). Boards often use overprescribing ofdrugs and drug and alcohol abuse, which theyhave found often coincide with incompetence, asgrounds for action instead of trying to prove in-competence (90,239,694,706,720). In particular,alcohol and drug abuse, characteristic of the im-paired physician, and physical and mental illnesscan result in substandard performance and avoid-able medical injury (636).
Several grounds for disciplinary actions are re-lated to law and ethics. Many of these may notaffect the technical aspects of quality but may in-fluence interpersonal relations. The grounds varygreatly in seriousness and include conviction ofa felony, conviction of a crime or felony related
6N0 ground for discipline adequately describes the lack of profes-sional ability or incompetence. The specific term varies among Statesand includes unprofessional conduct, gross incompetence, manifestincapacity, and malpractice and gross/repeated malpractice. All ofthese terms have no uniformly understood meaning.
to medical practice, fraud in obtaining a license,violations of narcotics laws, violations of childabuse reporting acts, betrayal of professionalsecrets or privileged communications, and mak-ing untruthful or exaggerated claims relating toprofessional excellence or abilities (34,260). Othergrounds for disciplinary action relate to chargesof essentially economic violations, such as fraudregarding fees, fee-splitting, false or deceptive ad-vertising, and overcharging or making false claimsfor reimbursement (34,260). Whether any, some,or all of these violations affect medical decision-making is not known, but to the extent that a vio-lation affects an individual’s trust in a physician’scare, the ability of a physician to provide com-petent interpersonal care is compromised. Peo-ple have different expectations of their physicians,and, depending on the type and seriousness of theviolation, many people would not be comforta-ble going to a physician who had violated the law.
If one accepts that all violations that lead toformal disciplinary actions are quality violations,then such actions appear to possess validity as ameasure of quality. The burden of proof for tak-ing formal disciplinary actions rests with the State,and such actions usually must be based on “clearand convincing evidence, ” a difficult standard ofproof. Due process safeguards are applied (70Corpus Juris Sec. 43), and procedural aspects aresufficiently rigorous that the decisionmaking proc-ess is unlikely to be affected by external influencesand the decisions are based on the evidence pre-sented (260). The time taken to complete a for-mal disciplinary action—about 3 years—is indica-tive of the carefulness of the process.
Other factors operate in favor of protectingphysicians’ licenses. Inadequate funding and staffoften limit States’ ability to prepare their cases aswell as the physicians’ paid legal counsels.7 Tes-timony from expert witnesses against the licen-see has often been difficult to obtain because ofa fear of civil liability for defamation (260,694 ).8
‘Andrew Watry, Executive Director of the Georgia State Boardof Medical Examiners, reports that the Board’s annual expenditures
for legal fees for 60 actions is $80,000 to $100,000. A physician mayspend as much as $50,000 to $100,000 in legal fees for one case (694).
8Professionals’ concern might decrease as a result of the recentpassage of the Health Care Quality Improvement Act of 1986 (PublicLaw 99-660). The act grants a limited immunity from damages un-
(confinued on next page)

726
Thus, it is more than likely that physicians whohave had formal disciplinary actions taken againstthem have violated State medical practice acts.
Nonetheless, the validity of formal disciplinaryactions can be questioned, since the decisions ofsome boards have been overridden by the courts.Every State gives physicians the right to some typeof judicial review of disciplinary actions takenagainst them to ensure that boards do not act inarbitrary, capricious ways or abuse discretion(260)(70 Corpus Juris Sec. 51). The courts haveruled against the boards in 30 percent of the casesbrought before them (168,342) 9 on issues of con-stitutional rights, statutory interpretation, suffi-ciency of evidence, appropriateness of disciplinaryaction (260), and technical errors (169). Consid-ering the number and range of reasons for over-riding boards decisions, including technical errors,one can consider 30 percent a “fairly good rec-ord ‘ (169).
Feasibility of Using the Indicator
Although information on formal disciplinaryactions taken by State medical boards is available,consumers have limited access to it. Formal dis-ciplinary actions are a matter of public record,
(continued from previous page)
der Federal and State laws to individuals providing information toa professional review body regarding the competence or professionalconduct of a physician unless they know the information is false.
‘In a 1983 article, Derbyshire notes that the percentage was con-sistent for court decisions from 1902 to 1966 and from 1969 to 1979(168). A similar percentage was found in an analysis of court deci-sions concerning actions taken against physicians who came beforethe Michigan Board of Medicine from 1977 to 1982 (342). More re-cent data are not available.
and consumers can obtain information about ac-tions taken against individual physicians by con-tacting State medical boards (190). Some boardseven periodically report disciplinary actions to thenews media (206), either directly or through news-letters, which almost a third of the boards nowpublish (206). Yet anecdotal information indicatesthat individuals and even representatives ofhealth-related organizations are unaware of theavailability of this information.
Another source of information on formal dis-ciplinary actions by State boards, the PhysicianDisciplinary Data Bank operated by the Federa-tion of State Medical Boards, is accessible onlyto organizations. The Federation’s data bank in-cludes information on formal disciplinary actionstaken against physicians by its member State med-ical boards and other government authorities. TheFederation of State Medical Boards sends monthlyreports to its member boards and some privateand public organizations on actions entered in thedata bank during the preceding month (205).When the American Medical Association receivesthe Federation’s monthly report, it informs all theState licensing boards under which a physicianis licensed that the physician has been disciplined.The Federation also screens individual physicians’disciplinary histories upon request; in 1986 it an-swered 39,000 inquiries from member boards andother organizations (636). Organizations such ashospitals and insurance companies can contractwith the Federation for information about discipli-nary actions (90). Easier access to cross-State in-formation will be available when the Federationcompletes a system for State medical boards todirectly access the data bank (636).
SANCTIONS RECOMMENDED BY PEER REVIEW ORGANIZATIONSAND IMPOSED BY HHS
In fulfilling its responsibility to assess and as- Health and Human Services sanctions providerssure the quality of care provided to Medicare ben- by imposing monetary penalties or exclusion fromeficiaries, HHS, upon recommendation of PROS, the Medicare program for specified periods ofimposes sanctions on providers who fail to pro- time.vide care that is medically necessary, appropri-
The sanction process is initiated when a PROate, and of adequate quality.10 The Secretary of physician finds that a quality problem exists andIOSee app, D for a comprehensive description of PROS. determines that a “substantial violation” or a

127
“gross and flagrant violation” may have oc-curred. 11 A “substantial violation” is a pattern ofcare over a substantial number of cases that is in-appropriate, unnecessary, does not meet recog-nized standards of care, or is not supported bythe documentation of care required by the PRO.A “gross and flagrant violation” is a violation thathas occurred in one or more instances and thatpresents an imminent danger to the health, safety,or well-being of a Medicare beneficiary, or un-necessarily places the beneficiary in a situation ofhigh-risk, for example of substantial and perma-nent harm (638).
If a PRO believes that a provider’s alleged vio-lation was a “substantial violation,” the PRO mustgive the provider two opportunities to discuss theallegations (see figure 6-l). Since the basic pur-pose of PROS is intended to be educational, thePRO first proposes corrective actions (e.g., requir-ing the physician to update skills by further edu-cation). If the quality problem is not corrected,the PRO recommends a sanction to the Office ofthe Inspector General of HHS. If the PRO believesthat the provider’s violation was a “gross and fla-grant violation, ” the provider receives no oppor-tunity to take corrective actions and only oneopportunity for discussion before the PRO rec-ommends a sanction (see figure 6-2).
In the case of “substantial violations” and “grossand flagrant violations, ” a provider is given 30days notice and an additional opportunity to sub-mit written comments before the PRO recom-mends sanctions to the Office of the InspectorGeneral. The final decision about whether to sanc-tion a physician is the responsibility of the Of-fice of the Inspector General under authoritydelegated by HHS. The Office of the InspectorGeneral decides if the medical evidence supportsthe decision of the PRO. If the decision of the In-spector General is to impose a sanction, a pro-vider may appeal the decision to an HHS admin-istrative law judge.
1’In addition to sanctions, PROS may also deny payment toproviders. The Consolidated Omnibus Budget Reconciliation Actof 1985 (Public Law 99-272) gave PROS authority to deny paymentfor quality of care violations, As of February 1988, the final regu-lations on these denial notices had not been released.
The intent of the discussion here is not to evalu-ate the effectiveness of the sanctioning process inidentifying all providers of poor-quality care, butto evaluate whether PRO-recommended sanctionsimposed by HHS are indicators of poor quality.As is true in the case of disciplinary actions takenby State medical boards, sanctions are expectedto measure the overall performance of a provider.The hypothesized relationship, that PRO-recom-mended sanctions imposed by the Office of theInspector General of HHS indicate providers ofpoor-quality care, has face validity. Since the Sec-retary of HHS is responsible for protecting thehealth and safety of Medicare beneficiaries, it islikely that beneficiaries and other consumerswould consider physicians whom HHS fined orexcluded from practicing in the Medicare andMedicaid programs
12 to be providers of poor-quality care.
Reliability of the Indicator
Sanctions result from actions taken by twodifferent organizations, a PRO and the Office ofthe Inspector General of HHS. Because of varia-tions in the process and criteria used to initiatesanctions among the 54 PRO programs, recom-mendations for sanctions by PROS on a nationalbasis as an indicator of quality are not reliable(622). Furthermore, the criteria of “professionallyrecognized standards of care” that PRO reviewersuse to assess the appropriateness and quality ofproviders’ care are based upon typical patternsof practice within the PRO’s geographic area ornational criteria where appropriate (638). To theextent that PROS use local and regional standardsof care in initiating sanctions, the criteria for
assessing care can vary among areas. Since differ-ent criteria are likely to be used, the possibilityof replicating sanction recommendations amongPROS is low.
To the extent that a given PRO reviews simi-lar cases in a similar manner, the PRO’s recom-mendations for sanctions to the Office of the In-spector General may have a considerable degreeof consistency as an indicator of quality. PRO rec-
IZpublic Law 100.93, the Medicare and Medicaid Patient and 1>ro-gram Protection Act of 1987, excludes physicians from Medicaidif they have been excluded from Medicare.

128
, . - - - - - - . - - - - - - - -8 Inithl sanction n0tk2e ;I
~ ; - - -- ” -
1 PROdecis&nI ~ Not a substantial violation
PRO decidea7
t a substantial violation has occurred and develops a
Provkkr doea ~ comply with cmecthm plan
, - - - - - - - : - - - - - - - -I second sanction notice :I
. - provider has 30 days to submit adddithal information ardor request a meeting- - - - - - - - - - - - - - - - - - “
I PRO decision + Not a substantial violation
, - - - - - - - : - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -~ Final sanction notice; PRO recommendation on decision to Offtce of h Inspector General of HHS ~.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - . . - - - - - - - - - - - - - - - - *
[ - Providar has 30 days to submit adddifkmal inkwmation to Office oftha lrwPOCW GeneralA -
I HI-IS Orfica of the Inspctor General decision }—s DO not sanctionI I
t, - - - - - - - - - - - - - - - .t sanction
I
I ,~ Provider accepts sanc t ion- - - - - - - - - - - - - - - -
fProvider appeals sanctkm to an administrative law judge of HHS
i
I FtHS Administrathm Law Judge decision * Dismiss sanction
*Sustain (or modify) sanction ~ Provider accepts sanction
+Provider appeals santion to the HHS Appeals Council
I 1
I Secretary of HHS Appeals Council decisionI
* Dismiss sanction
+Susta in (or modi fy ) sanct ion~ Provider accepts sanction
tProvider seeks judicial review of HHS Appeals Council’s decision to sustain sanction
i
I CQUrt decision ~ D i s m i s s s a n c t i o n
+Sustain sanction
a~ ~Uktmt~ “~~at~n Isa ~ttern of urn over a substarwaI ~Urn~r ‘f cases that )s mpproprlate, unnewasary, does not meet recognized pattemsot care, or is not supported bythe documentatm of care mqulred by the PRO
SOURCES: Adapted from U S Department of Heatth and Human Services, HeatttI Care Fmancmg Mmmistralfon, “Pear Rsrwew Orgamzation MUIUOL” HCFA Pub No 19, Trans-mmal No 15, Baltmore, MD, May 1987, and R P KUSSOW, Inspector General of the U S Oapwlmont of HealltI and HUman se-, testimony on the peer RevIawOrganlzatlon Proc9ss before the Subcommrttaeon Intergovernmental Relat~ns and Human Resources, mmmmee on Govern ment OperafmfM, House of Repreaenta-!h#s, U S tingresa, Washington, OC, Oct 20, 19137

129
, - - - - - - - - - - - - - - - -I
Initial sanction notice ~I . . Provider has 30 days to wbmit additional information andkx request a meating
~ 0 ” -- -
PROdectsbn = NOt a gross and flagrant Watkm
It, - - . - - - - - . - - - . - . - - - . . - - - . . - - - - - - - - . - - - . - q
: Final Sanc60n notice remrnmendation to Offic9 of the Inspectw General of HHS ;- - - - - - - - - - - - - . - - - . - . - - . - - . . . . - - - . - - . - - . 1
r
i. - Provider has 30 days to wbmil additional informati to _ of ha Irwpwtor Gerwral
- -A “ -
+, - - - - - - - - - - - - - - - -I I
1 ,~ P r o v i d e r a c c e p t s s a r w t i c m- - - - - - - - - - - - - - - -
iProvider appeals Sanctmn
o to an administrative law judge of H-B
i
I HHS Administrative I.Aw Judge decisionI
* Dismiss sanction
S u s t a i n ( o r m + i i ) w m c t i c m ~ Provider accepts sanction
Provider appeals samtion to the HHS Appeals Council
r I
I Secretary of HHS -Is Council decision ~ Dismiss sanction
tSustain (or modify) sanction~ Provider accapts sanction
+Provider seeks judicial review of HHS Appeals Council’s decision to sustain sanction
b
I t iUf ’ t decis ion } * Dismiss sanction
tSustain sanction
a~ - ~ flw,mt ~~~~ VKxaIlorl is ● Wolat)orl that - ~cu~ed In - of~benet%mry
more instances and presents an Immmant danger to the heatth, safety, or well-tang of a Medicare
SOURCES: Adapted from U S Oepartmentof Hoatth ● nd Human Serwces, liealth Care Financing Admimstrahon , ‘Peer Review Orgamzatlon Manual, - HCFA Pub No 19, Trans-mittal No 15, Baltimore, MD, May 1987, and R P Kusserow, Inspector General of the U S Department of Heatth and Human Servmss, testmony on the Peer RewewOrgamzdon Process Worethe SuIxornmrtteeon Intergovernmental Relahons and Human Resources, Commrttee on Government Operations, House of Representa-I-, U S Congress, Washington, OC, Ocf 20, 1987

130
ommendations for sanctions go through a num-ber of reviews before they are sent to the Officeof the Inspector General. The first round of phy-sician review offers chances for great incon-sistency. Similar cases could be reviewed by differ-ent physicians who for the most part use implicitcriteria in deciding to initiate a sanction. Further-more, some PROS have expressed concern thatinadequate funding makes them unable to recruit,train, and retain qualified physician reviewers(491).
Nonetheless, subsequent reviews can increasethe chances that a recommendation for a sanc-tion for a similar violation is replicable within aPRO. The number of additional reviews variesamong the PROS. In Iowa, for example, beforea sanction is recommended to the Office of theInspector General, the case is reviewed by a 15-member quality assurance committee; a 15-member comprehensive review committee; andthe board of directors of the PRO, composed of29 physicians, a business representative, a den-tist, a nursing home owner, an administrator ofa small hospital, and an administrator of a largehospital (405). Before a sanction recommendationis made to the Office of the Inspector General,the California PRO involves a regional medicaldirector, the associate medicaI director, the med-ical director, the monitoring committee, the chiefexecutive officer, and the board of directors (435).In all PROS, final review by the PRO’s board ofdirectors is required before a formal recommen-dation is made to the Office of the InspectorGeneral.
To the extent that a PRO’s board of directorsis stable in membership, that a consensus proc-ess is used in arriving at decisions, and that mem-bers are consistent in their rulings, reliability isincreased. If precise guidelines were used byboards of directors in arriving at recommenda-tions for sanctions, the replicability of their deci-sions could be increased. More exact guidelineswere provided in May 1987 as the result of anagreement among the American Association ofRetired Persons, the American Medical Associa-tion, the Office of the Inspector General, and theHealth Care Financing Administration (HCFA) to
specify and standardize the procedures PROS usein recommending sanctions (164).13
Since the imposition of sanctions is, for themost part, a function of the Office of the Inspec-tor General of HHS, the additional reviews theOffice conducts before a provider is sanctionedare crucial in establishing the reliability of sanc-tions. Federal regulations are specific about whatsteps the Office should take in arriving at a sanc-tion decision, but do not describe how the stepsshould be executed (42 CFR 1004.90 [1986]). Thesame small number of Office personnel, represent-ing the medical and legal professions, are involvedin considering whether a provider has violatedhis/her obligations and in determining an appro-priate sanction, and a single individual within theOffice of the Inspector General is responsible forthe final determination to sanction a provider(375).
Validity of the Indicator
It is not clear whether all sanctions are initi-ated on the basis of quality-related problems. 14Recommendations for sanctions are initiated byPROS when a provider’s services: 1) are not pro-vided economically and are not medically neces-sary, 2) are not of a quality that meets profession-ally recognized standards of health care, and 3)are not properly documented (638). Although pro-
IJThe recommended procedures include specifying model lettersthat PROS will send to physicians and hospitals during the sanc-tion process; ensuring that no physician member of a PRO makinga final sanction determination against a physician has a bias againstor is in competition with the subject physician; permitting an at-torney to accompany a physician to certain meetings required dur-ing the process; permitting the attorney to make opening and clos-ing remarks and to assist the physician in presenting the testimony
of expert witnesses who may appear on the physician’s behalf; mak-ing a verbatim record of such meetings with a copy made availableto the physician: and permitting the physician to submit additionalrelevant information to the PRO within 5 working days after themeeting (164).
IiThe Hea]th Care Financing Administration collects data on thenumber of sanctions initiated by PROS because of potential “sub-stantial violations” and “gross and flagrant violations, ” but doesnot have information on the grounds for the initiation of sanctions(228). The Office of the Inspector General does have the informa-tion but does not generally distribute it. The Office of the Inspec-tor General has provided the information to at least one consumeradvocacy group.

131
vision of unnecessary services could be classifiedas a quality issue, insufficient documentation ismost likely due to inadequate recordkeeping,which may or may not be associated with poor-quality care.
Of more importance is the fact that, if unnec-essary and inappropriate services and prematuredischarges are perceived as quality concerns,almost all of the sanctions imposed by the Officeof the Inspector General upon recommendationof PROS have been for quality violations. In fact,78 of the 79 sanctions the Office imposed by Sep-tember 1987, were on quality-based grounds. Onesanction was based exclusively on grounds of im-proper documentation (375).
Furthermore, the possibility of sanctioning phy-sicians who do not provide poor care is slight,an observation that suggests that PRO-recom-mended sanctions imposed by HHS are valid in-dicators of quality. An extensive weeding-outprocess takes places before PRO-recommendedsanctions are imposed by HHS, and only a fewsanctions have been imposed. From the 30 mil-lion hospital discharges involving Medicare ben-eficiaries from the beginning of October 1983 tothe end of December 1986, PROS identified 6,500discharges involving 2,500 providers as havingpotential quality-of-care or utilization problems(360). The great majority–over 97 percent–ofthe cases were resolved at the PRO level by PROSworking with providers during the steps of theprocess and were not referred to the Office of theInspector General. Most deficiencies were cor-rected by educational or corrective actions, andthrough December 1987, only 151 cases were re-ferred to the Office for review and final action.Not all of the 151 cases that were referred wereheld to be sustained in law or by medical evidence.Only 61 resulted in exclusion from the Medicareprogram (60 physicians and 1 hospital); 26 casesresulted in a monetary penalty; 8 cases are nowunder review; and 2 physicians have died (661).Many of the sanctions that the Office rejectedwere rejected because of procedural issues (e. g.,the PROS were late in submitting documentationor the documentation was not complete) (360).
Physicians who are sanctioned are often citedfor multiple violations. One physician, for exam-ple, was sanctioned on the basis of 22 cases of defi-cient care (713). Indeed, the 11 physicians whowere sanctioned by exclusion from Medicare inthe period February 8 to July 2, 1987, were re-sponsible for “gross and flagrant violations” in thecare of 48 patients. Physicians who are fined arealso likely to have committed one or two seriousviolations (501).
Another way to determine if physicians whoprovide standard care are being safeguarded fromsanctions is to examine if they are given appro-priate due process. The sanction process attemptsto balance the interest of HHS in protecting thehealth and safety of Medicare beneficiaries withthe due process rights of providers. As a peer re-view process, the system does not have the ex-tensive safeguards characteristic of the judicialprocess. Nonetheless, physicians have the oppor-tunity of submitting information, being heard be-fore two administrative bodies (the PRO and theOffice of the Inspector General) before a sanctionis imposed, and of appealing the imposition of asanction.
As noted earlier, regulations require that PROSallow physicians to submit information and meetonce with the PRO if they are alleged to havecommitted a gross and flagrant violation(s) andtwice if the violation is a substantial violation.After the PRO recommends a sanction, the Of-fice of the Inspector General conducts an inde-pendent review of the PRO report and any addi-tional information submitted by the physicianunder consideration. If the Office agrees with thePRO and also finds the physician unwilling or un-able to comply with statutory obligations, 15 it willsanction the physician, lb either by excludin g ‘hephysician from the Medicare program or by im-posing a monetary penalty. The Office’s decision
1 sThe “unwi]]ing and unab]e” condition has been questioned asbeing ambiguous and an impediment to protecting patients fromproviders of substandard care (360).
1bThe Office of the Inspector General of HHS has 120 days to ac-cept or reject the recommendation, or a sanction is imposed. Todate, the Office of the Inspector General has always acted on rec-ommendations within the allotted time (375).

132
can be appealed, in which case a hearing is heldbefore an administrative law judge of HHS. Thishearing is the first time in the process that a fullevidentiary hearing is held (360). This decisionmay then be reviewed upon request by the HHSAppeals Council. If dissatisfied with the result,physicians have the right to seek further reviewof their cases in the court system (see figures 6-1and 6-2).
A few cases have gone to district courts, andsome of them have been appealed. The appealscourts have upheld the adequacy of due processin the PRO sanction process (125,276,674). In itsruling, the 4th Circuit Court noted that the PRO-initiated sanctions process affords providersappropriate due process, since the Government’sneed to protect Medicare beneficiaries from poor-quality care is compelling. Disagreement with theadequacy of the process continues, however, inboth the medical and legislative communities.Some accommodation was made in the OmnibusBudget Reconciliation Act of 1987 (Public Law100-203), which allows physicians in certain un-derserved areas to continue to practice, althoughsanctioned, during the administrative review proc-ess.17
Feasibility of Using the Indicator
Although sufficient data exist for purposes offormulating PRO-recommended sanctions im-posed by HHS as an indicator of the quality ofcare, many consumers may find it difficult to gainaccess to the information. If the Office of the In-spector General imposes a sanction, a notice is
ITThe Omnibus Budget Reconciliation Act of 1987 (Public Law100-203) made some changes in the review process. The act pro-vides that in rural health areas with health manpower shortages andin counties with fewer than 70,000 people, physicians seeking tooverturn a decision that excludes them from Medicare for failureto furnish medical care of acceptable quality may continue to prac-tice during the administrative review process, unless an adminis-trative judge determines that continued practice would pose a seri-ous risk to Medicare beneficiaries.
published in a newspaper in the PRO area advis-ing the public of the Government’s action .18 TheMay 1987 agreement between the Office of theInspector General, the American Medical Asso-ciation, the American Association of Retired Per-sons, and HCFA, discussed earlier, included astipulation, subject to regulatory change, thatphysicians and other providers are to notify theirMedicare patients that they have been sanctionedin lieu of newspaper publication of this fact. Asof February 1988, the regulations were under de-velopment.
Anecdotal information indicates that the cur-rent publishing requirement has not been im-plemented in a way that provides easy access forconsumers to information about sanctioned phy-sicians. It is said, for example, that newspaperswith small circulations are often used, and noticesare placed in small type, often in the public no-tice section. There are potential problems with thenew method as well. It is not clear that havingphysicians privately inform their current or po-tential Medicare patients that they have been sanc-tioned will increase the effectiveness of provid-ing consumers with information on sanctions. Onthe one hand, Medicare beneficiaries would nothave to seek out the information. On the otherhand, sanctioned physicians will have conflictinginterests between defending their practices andtheir legal obligation to provide information.Thus, Medicare beneficiaries may not receive ascomplete an explanation about the grounds fora sanction from the sanctioned physician as froma newspaper notice. In addition, automatic notifi-cation concerning sanctioned physicians will notbe available to non-Medicare consumers (501).
18 Regulations require that the Office of the Inspector General
“notify the public by publishing in a newspaper of general circula-tion in the PRO area a notice that identifies the sanctioned practi-tioner or other person, the obligation that has been violated, thesanction imposed and if the sanction is exclusion, the effective dateand duration” (42 CFR Sh. V (10)-1986 cd.).

133
MALPRACTICE COMPENSATION
A malpractice suit indicates that a patient is dis-satisfied with care received from a provider. Thereis some evidence that patients who are satisfiedwith interpersonal aspects of care are less likelyto sue their physicians than patients who are dis-satisfied with these aspects. 19 The analysis in thischapter assumes that a malpractice suit suggeststhat the physician has some deficiency in inter-personal aspects of care. The question exploredhere is whether malpractice compensation is a rea-sonable indicator of poor technical performance.
Patients usually use the tort liability system toobtain monetary compensation for medical in-jury. The process of determining liability isinitiated when a patient or provider identifies amedical, possibly negligently induced, injury.Sometimes a “warning” file maybe opened by aninsurer on the basis of a report from an insuredprovider. The next step is likely to be a claim re-ceived directly from an injured claimant or clai-mant’s representative, which may accompany orsoon be followed by a lawsuit. The lawsuit mayor may not be resolved in favor of the patient.If the lawsuit is resolved in favor of the patient,the patient may receive medical compensation ei-ther through a jury verdict or through negotiatedsettlement with the physician’s insurance com-pany, usually prior to an actual courtroom pro-ceeding. Even after a jury verdict, the trial judgemay alter or overturn the verdict, and appealsmay be made. Many awards are reduced beforeactual payment is made (159).
Only some medical injuries, or adverse medi-cal outcomes, that occur are the result ofproviders’ failing to conform, through omission
“Obstetricians/ gynecologists and medical specialists who reportspending more time with their patients per office visit than similarphysicians, on average, incur fewer claims than physicians whospend less time (6).
or commission, to current standards of medicalcare (449,636). Other adverse medical outcomesare unavoidable results of insufficient medicalknowledge about the natural course of some con-ditions and unexpected effects of diagnostic andtherapeutic procedures (449,636).
Few studies have attempted to determine theoccurrence of medical injuries and fewer still theproportion that are possibly negligently induced.A pilot study in 1973 found that medical injuriesoccurred in nearly 8 percent of the cases reviewedand estimated that medical injuries due to medi-cal negligence occurred in 2.3 percent of cases re-viewed (494). A study of about 21,000 hospitalrecords of California hospitals performed in themid-1970s concluded that 1 out of every 20 ad-missions (5 percent) resulted in an injury causedby medical treatment (114). Seventeen percent ofthe injuries caused by medical treatment, or 1 outof every 126 hospital admissions (0.8 percent),were estimated to be caused by legally provablenegligence. A more recent analysis found thatalmost 1 percent of hospital admissions are asso-ciated with poor care that results in temporaryor permanent disability or death (159).
The discussion here will focus on the reliabil-ity and validity of court awards as an indicatorof the quality of care, in part because from a con-sumer’s perspective such awards would have facevalidity. In order for medical malpractice to beestablished in court, one must prove the existenceof a duty of the physician to the patient, the ex-istence of an applicable standard of care, negli-gence or the failure of the provider to meet thestandard of care, injury or damage to the patient,and the determination that the proximate causeof injury to the patient was the physician’s fail-ure to meet the standard of care (636). Most peo-ple would consider a physician who has beenfound liable of malpractice in a court action, par-

134
ticularly for a number of cases over a period oftime, to be a provider of poor-quality care.
The other major form of malpractice compen-sation is negotiated settlements, that is, paymentwithout a judicial determination. Malpractice set-tlements are often made for reasons unrelated toquality that are usually unknown to the generalpublic.
20 The lack of information does not meanthat any claim for which settlement was negoti-ated is not without meaning as an indicator ofquality. Indeed, it can be argued that cases withlarge settlements are settled out of court becausenegligence can be proven. It is likely that casesinvolving small settlements of $20,000 to $40,000may not go to trial for reasons of efficiency aswell as reasons of negligence. Furthermore, ne-gotiated settlements are the more important formof claims settlement, since 90 percent of medicalmalpractice claims are settled before trial, and ofthose settled with payment approximately 97 per-cent are closed as a result of a negotiated settle-ment (625). The reliability and validity of nego-tiated settlements as indicators of the quality ofcare cannot be evaluated, however, because thenegotiation process is confidential .21
Reliability of the Indicator
The many variations across the country in thetort system governing malpractice cases—includ-ing variations in laws, judges, and juries—makeit unlikely that court awards are reliable as an in-dicator of quality on a national level. There arefewer variations within States, because medicalmalpractice claims are resolved through State
ZoSett]ements are Usua]]y agreed to in cases whose resolution isclear (88). They are often made for reasons other than physiciannegligence, including court congestion, variation in the interest ofliability insurance carriers in settlements, probability of success ina particular court before specific judges, credibility of both plain-tiffs and defendants as witnesses (461), the cost of protracted litiga-tion compared to early settlement, the ability of the plaintiff’s coun-sel, the sympathy aroused by the plaintiff, aggravated fact situationsthat would inflate the award, the amount of the awards for a simi-lar injury in the jurisdiction, the personalities of the key witnesses,the desire to avoid publicity of a trial, and the existence of a statu-tory requirement to submit the claim to a pretrial panel (636). in-deed, some experts contend that settlements are not directly relatedto a finding of malpractice, i.e., negligently induced medical injury(636).
ZIThe section does not consider malpractice claims that have not
been resolved, because such claims represent an accusation of wrong-doing with no knowledge of the truth or falsity of the claim.
court systems and under State statutes. Evenwithin States, however, many judges and juriesare involved in malpractice cases, and not alljudges place the same interpretation upon the law.
Within a judge’s courtroom, a judge’s awardsmay be consistent. In addition, indirect evidencesuggests that jury awards might have some relia-bility as an indicator of the quality of care. Al-though the consistency of verdicts among jurieshas not been studied, the consistency in verdictsbetween judge and juries has been examined inboth criminal and civil cases. In 3,576 criminaltrials and about 4,000 civil trials, both judge andjury agreed on the verdict 78 percent of the time(338). These findings might have positive impli-cations for consistency among juries. In general,studies find that the rate of agreement among par-ticipants in complex human judgments, such asscientific peer review panels and decisions of prac-ticing physicians and judges, ranges from 55 to80 percent (see table 6-2). Nonetheless, the limitedboundary of one judge’s courtroom, within whichjury awards might have some consistency, worksagainst the usefulness of jury awards as an indi-cator of the quality of care.
Validity of the Indicator
Individual Awards for Malpractice
Court awards for malpractice as a measure ofthe quality of care would appear to have somevalidity as indicators of quality in that compen-sation is supposed to be awarded for negligenceonly. Other concerns, such as fraud and abuse,are not at issue. In addition, a judgment in favorof a patient, in theory, means that a physician’snegligence has been proven. Nonetheless, inweighing the evidence it appears that—except inextreme cases, such as amputating the wronglimb—individual jury awards are not indicatorsof a physician’s performance.
On the one hand, the difficulty and length oftime involved in filing and resolving malpracticeclaims, the formal process of the litigation, andthe small number of cases that are resolved in fa-vor of the patient/claimant appear to support thecontention that physicians who have been foundliable of malpractice are providing poor-qualitycare. Although these features have to do with

135
Table 6.2.—lnterjudge Consistency in Complex Human Judgments
Rate ofa g r e e m e n tbetween 2
D e c i s i o n m a k e r s S t i m u l u s Decis ion judges ( o / o )
National Science Foundation vs.National Academy of Sciences peerreviewers
7 Employment interviewers
4 Experienced psychiatrists
21-23 Prac t ic ing phys ic ians
3,576 Judge-jury pairs
12 Federal judges
8 Federal judges
150 Grant t)roDosals submitted to the T o f u n d o r n o t t o f u n d ( h a l f f u n d e d b v ‘-, ,National Science Foundation
10 Job applicants
153 Patients interviewed twice, onceby each of 2 psychiatrists
3 Patients-actors with presentings y m p t o m s
3,576 Jury trials
460 Presentence reports (atsentencing council)
439 Presentence reports (atsentencing council)
the National Science Foundation) -
Ranked in top 5 or in bottom 5
Psychosis, neurosis, characterdisorder
Diagnosis: correct or incorrect
Probability of agreement (both corrector both incorrect)a
Guilty or not guilty
Custody or no cus tody
Custody or no custody
f!J
70
70
66, 77, 70
55,65,57
78
80
79
alnflated because physicians could also be inaccurate in different ways.
SOURCE S.S Diamond, “Order In the Court: Consistency in Criminal Court Decisions,” The Master Lecture Series Vol. //: Psychology and the Law, C.J Schelrer andB.L Hammonds (eds ) (Washington, DC: American Psychological Association, 1983) Copyright 1983 by the American Psychological Association Ada~tedby permission of the publisher and the author.
adherence to procedural requirements rather thanwith the substance of claims, one could argue thatthey diminish the possibility that physicians whoare found liable will not in fact have been negli-gent. Of course, some of the physicians who arenot found liable of malpractice may in fact havebeen negligent.
The fact that very few injured people bring amalpractice claim (87) illustrates the difficulty ofthe process. A recent pilot study of the prevalenceof public perceptions of medically induced illnessin Maine concluded that of the 42 respondents thathad reported that they or a close relative had amedically induced injury, 2 discussed the incidentwith an attorney and only 1 initiated a suit (430).A more comprehensive analysis estimated thatclaims are filed for only a small percentage ofnegligently induced injuries. Extrapolating froma 1977 California Medical Association/Califor-nia Hospital Association study and 1974-76 datacollected by the National Association of InsuranceCommissioners, the researcher estimated thatabout 1 malpractice claim was filed for every 10potentially valid claims (159).
An attorney has to be convinced of the meritsof a case to take the case, because most attorneysin malpractice litigation cases are paid only if their
client wins (i. e., they work on a contingency feebasis). Since attorneys generally receive a percent-age of the award, most are concerned with po-tentially successful claims that are likely to resultin a substantial award. Although it is obvious thatthe number varies among lawyers, a dated sur-vey found that a claimant has less than one chancein eight of convincing an attorney to take a med-ical malpractice case (449).22
The extensive time required is another illustra-tion of the rigor of the claims resolution process.The median length of time from claim filing tocomplete disposition against all the providers in-volved is 19 months: the median time for paidclaims is 23 months. In general, the more severeand the more costly cases take a longer period toresolve (623),
Furthermore, during litigation, the substantiveand due process rights of participants are pro-tected. Formal rules of evidence control the ad-mission of unreliable or prejudicial testimony, andcompensation depends upon proving the providerat fault (449). Standards of care are generally infavor of the defendant (87). Providers are judgedby peer standards, and juries are instructed to as-
22 NeWer quantitative data are not available

136
sess and choose among the medical opinions pre-sented and not impose their own opinion of thecare. Finally, only a small percentage of claimsfiled are closed with a court award. A study of73,500 claims closed in 1984 found that 24,630(43.7 percent) were closed with payment; of the24,630, only 608 (2.5 percent) were closed witha court verdict either before or after appeal (622).
On the other hand, in reality, numerous otherfactors not related to the quality of medical careinfluence jury awards. Such factors include theeffectiveness of the attorneys (611); the ability ofthe jury and expert witnesses to assess medicalresponsibility (611,636); the effect of race, sex, andperceived economic status on the jury (486); theeffect of the passage of time from incident to ver-dict on the quality of the evidence (317); and theselective recall of witnesses (486); the effect of theextent of the injury and its obviousness (e. g.,when surgical instruments are left within a body)(159); and the effect of the number of defendants(the chance of a physician’s receiving an adversejudgment approximately doubles when a case in-volves multiple defendants) (159). It is not knownwhether some of these factors lead to increasedor decreased accuracy in the outcomes of medi-cal malpractice litigation.
In addition, individual jury awards are in-accurate indicators of specific physicians whoprovide substandard care, because multiple phy-sicians may be defendants in any one case. Phy-sicians who have had only peripheral involvementwith a supposed negligently induced injury maybe involved in the jury award. Heads of depart-ments, for example, are often held legally respon-sible for the actions of the residents in their de-partment, even though they were not present atthe time of an incident; the same may be true ofresidents who played only a small part in a com-plex procedure.
Another challenge to the validity of malprac-tice compensation as an indicator of the qualityof medical care is that malpractice litigation de-pends to a large extent on the lack of criteria re-garding poor-quality care. The disagreementsabout what constitutes real malpractice are long-standing and serious and need extensive researchbefore resolution.
Physician Profiles
A successful malpractice suit might indicate thata physician made an inadvertent error that hadserious consequences for the patient or it mightbe one instance of a dangerous practice patternof a physician that poses a risk in future patientencounters. There is a lack of empirical evidenceto indicate which applies. Some would argue thatfindings of negligence in a number of malprac-tice cases indicate that a physician is deliveringsubstandard care. Although this argument mayseem intuitively correct, evidence to disprove itis also lacking.
A report of an analysis of Maryland data from1960 to 1970 noted that a physician’s being suedmore than once could be attributed as much tochance as to poor practice, but the authors warnagainst generalizing the data to the entire coun-try (101). A hypothetical informal statistical anal-ysis confirmed the above finding (443). The anal-ysis assumed that all physicians were similar andall patients were similar and that all cases wereindependent of each other. Yet in practice, phy-sicians practice in different specialties and even,within a specialty, see different types of cases anddifferent numbers of patients. Physicians who arefrequently sued may be technically excellent butmay be treating difficult cases and using high-riskprocedures. In the absence of knowledge aboutpatient and practice characteristics, the relation-ship of a physician’s quality of care to multiplemalpractice suits cannot be determined.
It is clear, however, that liability experience isnot random with respect to specialty, and thatsome specialties have more malpractice claimsthan others. The specialists most often named inmalpractice actions are obstetricians/gynecolo-gists, general surgeons, and orthopedic surgeons;the percentage of claims paid is highest for pathol-ogists, urologists, otolaryngologists, and obstetri-cians/gynecologists (623). These specialties em-ploy invasive technologies with greater chancesof doing serious harm. The many suits against ob-stetricians may also reflect heightened expecta-tions on the part of consumers about what canbe done with procedures such as fetal monitor-ing or amniocentesis rather than anything to dowith the technical aspects of quality.

137
Studies also show that fairly few physicians ac-count for a large share of medical malpracticeclaims. One study reported that 1 percent of phy-sicians were responsible for 25 percent of paidclaims and 20 percent of physicians had three ormore paid claims in 10 years (301). Another studyfound that about 42 percent of physicians withclaims in one year had previous claims againstthem (623). Since such percentages reflect thedifferences in malpractice experience among spe-cialties, they do not necessarily mean that thesephysicians are providing substandard care,
Certain physicians in certain specialties havemore claims than expected by chance (301,529,675). In looking at large claims, researchers foundthat in some specialties, some physicians did nothave more claims than expected (675). In otherspecialties, including internal medicine and anes-thesiology, some physicians had disproportion-ately more claims than others; however, thedifference could be accounted for by differencesin practice level. This finding indicates that thepast experience of individual physicians in certainspecialties may be a valid measure of the individ-ual’s exposure to claims in the future and may beused to set malpractice premium rates. The lackof information about the characteristics and num-bers, however, of the patients and cases seen byphysicians compromises the ability to use medi-cal malpractice experience as a valid indicator ofsubstandard care provided by individual phy-sicians.
Currently, the frequency and severity23 ofclaims against individual practitioners are takeninto account in quality-of-care evaluations car-ried out by certain hospitals for the purposes ofpeer review and by certain State Iicensure andcredentialing organizations. The impetus for thisnew practice can be traced to lawsuits in Arizonaand California, where hospitals had been held re-sponsible to patients when lawsuit informationof attending physicians was not considered whenmedical staff committees determined whether togrant hospital privileges (197,504). The frequency
‘] Severity is related to frequency. Potentially high damages aremore likely to prompt a claim than are low ones, and anyonespecializing in high-damage cases, such as obstetricians /gynecolo-gists, is likely to generate higher frequency claims than others p e c i a l i s t s .
and severity of claims are also used by certain in-surance organizations to evaluate physicians whoare applying for malpractice insurance coverageor renewal and to identify physicians for risk man-agement and quality assurance review and reme-diation (30).
Feasibility of Using the Indicator
The remarkable limitations of available data onmalpractice litigation contravene the feasibility ofusing medical malpractice compensation as an in-dicator of the quality of care. The major sourceof data on settlements and jury awards is claimsclosed by insurers writing malpractice insurance,24
and data from this source are expensive to col-lect and limited in usefulness. One reason that theusefulness of the data is limited is that insurersdo not have a standard definition of claims andcount claims differently.
Systematically collected data on the number ofpaid malpractice physician claims are not read-ily available; also not readily available are dataon the frequency of malpractice claims that in-volve multiple providers and the identity of thedefendants in multiple-defendant malpracticesuits. Health insurance data that link proceduresperformed to individual physicians would be help-ful in addressing the issue of the relationship ofmultiple settlements to extent of practice. In mostinstances, such information is not available. Datathat identify physician performance that resultsin negligent actions and malpractice claims are notavailable. Without such information, it is not pos-sible to relate malpractice compensation to negli-gence. To obtain such information, costly medi-cal record reviews would be needed in additionto malpractice claims information.
Incomplete information on medical malpracticejudgments is compiled at present, but even thisinformation is not readily accessible to consumers.A malpractice judgment is a final court decision,and like any other court record, it is public. SomeState laws require reporting of malpractice judg-ments to medical licensing boards. If the State hasa Freedom of Information Act, the information
ZaThe last study of nationa] c]aims identified a universe of 102malpractice insurers in the United States in 1983 (623).

138
is available through a Freedom of Information re- metropolitan areas, such publications are expen-quest (578). Although an ongoing source of data sive, and it is unlikely that individual consumerson jury verdicts is the privately published Jury subscribe to them. Information on out-of-courtVerdict Reporter Newsletters, which cover many settlements is not publicly available.
CONCLUSIONS AND POLICY IMPLICATIONSThe causal relationship between license disci-
pline, sanctions imposed by HHS upon recom-mendations by PROS, and malpractice compen-sation on the one hand and quality of care on theother has not been the subject of scientificexamination. Since the interpretation of such rela-tionships relies on deductive reasoning fromdescriptive information, findings are not firmlyconclusive. Nonetheless, tentative conclusions canbe made and directions for policy and researchoffered.
Disciplinary Actions byState Medical Boards
Of the three potential indicators examined inthis chapter, formal disciplinary actions taken byState medical boards can currently be used withthe greatest degree of confidence in identifyingphysicians who provide substandard care. Al-though the reliability of disciplinary actions is notclear, the deliberateness of the disciplinary proc-ess and the safeguards of physicians’ rights to le-gal due process appear to ensure that the actionsindicate infractions of State medical practice acts.Some people do not consider all infractions ofState medical practice to be quality problems,however, because the scope of medical practiceacts is broad and infractions of the acts includeinaccurate drug prescribing, substance abuse, andcriminal actions as well as incompetence. Forthose consumers who believe that quality in pro-viding medical care is affected by a physician’scharacter and not confined to the physician’s tech-nical skills, formal disciplinary actions taken bya State medical board would be a fairly good in-dicator of poor-quality care. For those consumerswho limit their assessment of the quality of med-ical care to how physicians provide medical care,formal disciplinary actions generally would beaninexact indicator of poor-quality care. For all con-
sumers, formal disciplinary actions that are takenon grounds of incompetence are adequate, albeitnot perfect, indicators of substandard care.
If the reliability of formal disciplinary actionswere better established, individuals and organi-zations could use this indicator with greaterconfidence. In order to increase reliability, an es-sential step would be to open up to public exam-ination the processes that State medical boardsuse in disciplining physicians. Public scrutinywould also permit a better understanding of in-formal disciplinary actions and exactly when,why, and how they are taken and enforced. Theirrelationship to formal disciplinary actions and topoor care has not been examined. The validityof disciplinary actions as a quality indicator couldbe improved if all State medical practice acts in-cluded incompetence as a ground for disciplinaryaction, precisely defined the meaning of the term,and supplied guidelines for the actions applica-ble to the violation.
Although consumers can obtain informationabout formal disciplinary actions taken againstindividual physicians by contacting State medi-cal boards, most consumers do not know this. In-formation would reach more consumers if moreState boards would publicize their actions widely,and if State boards that currently supply infor-mation would increase their dissemination activ-ities. Without additional funding, most State med-ical boards would have difficulty assuming theadditional costs associated with providing infor-mation to the public. Most of the boards are un-der extreme financial constraints due to increas-ing investigatory and disciplinary activities (361).If dissemination of such information is a desira-ble government responsibility, additional Statefunding is needed. Federal funding is another pos-sibility, although many concerned individuals be-lieve that it would interfere with States’ preroga-tive to license physicians (190).

139
Another source of information on formal dis-ciplinary actions taken by State medical boardsis the Physician Disciplinary Data Bank operatedby the Federation of State Medical Boards. Re-porting of disciplinary actions by State medicalboards to the Federation is voluntary, but allStates participate in the Federation’s data bank.Through monthly reports and through direct ac-cess to the data bank, the information is dissemi-nated to State medical boards and other organi-zations; it is not disseminated to individuals. Somewould argue that the usefulness of individual ac-cess to the information in the Federation’s databank is questionable. Although organizations suchas third-party payers require updates on discipli-nary actions taken against many physicians, mostindividuals are interested in information concern-ing one or more physicians at one point in time,and that information can be obtained from Statemedical boards. The Federation charges for itsservices, and the charges might be high for mostpeople. In addition, the Federation does not ver-ify the accuracy of the information that the Statesreport. Organizations are expected to use the in-formation in the Federation’s data bank as a start-ing point for more intensive inquiry—a coursewhich many individuals might not be willing orable to pursue.
The national data bank mandated by the HealthCare Quality Improvement Act of 1986 (PublicLaw 99-660) is a potential source of informationon disciplinary actions .25 State medical boards areto report disciplinary actions to the data bank,but are not mandated to actively obtain informa-tion concerning other boards’ disciplinary actions.It appears the data bank will include the samelicense discipline information now available in theFederation’s Physician Disciplinary Data Bank,but will add new information on malpractice com-pensation and adverse actions taken by hospitalsregarding physicians’ privileges. National con-fidentiality requirements will not override Statelegislative requirements of confidentiality (706).
‘> The national data bank dld not receive funding for fiscal yearIOM3, a]though it is in the President’s budget for fiscal year 198Q.
Sanctions Recommended by PROSand Imposed by HHS
It is likely that sanctions imposed by the Of-fice of the Inspector General of HHS on the rec-ommendation of PROS are indicators of substand-ard quality of care. Available evidence about thesanctioning process suggests that recommenda-tions for sanctions are consistent within a PROarea and are imposed consistently by the Officeof the Inspector General. Such sanctions are validindicators of physicians and hospitals that pro-vide unnecessary services and substandard care.But evidence is very scanty and the sanctioningprocess is new and evolving. Although consumerscould use such sanctions as an indicator of poor-quality care at this time, the indicator needs con-tinuous evaluation.
The reliability and the validity of sanctions asan indicator of quality could be assessed withgreater accuracy if information about the proc-esses used by PROS and the Office of the Inspec-tor General were available. It is clear that thereis great variation in the approaches used by PROSin assessing quality, the number of groups withina PRO that review a case, and the number andtypes of intervention steps and amount of timebetween the identification of a quality problemand sanctioning (623,661). Yet little is knownabout how individual PROS make sanction rec-ommendations and how the Office of the Inspec-tor General executes the steps in arriving at a sanc-tion decision. It would appear that the use ofprecise guidelines by the boards of directors ofPROS in recommending sanctions to the Officeof the Inspector General and the standardizationof professional guidelines of care would allowconsumers to rely more heavily upon PRO/HHSsanctions as a quality indicator.
The potential usefulness of this indicator of thequality of care suggests that a policy requiringoversight of the effectiveness of actions to dissem-inate information on sanctions is warranted. Anew method has been agreed upon, and once reg-ulations are promulgated, providers will have tonotify their Medicare patients of sanctions. Sanc-tioned physicians may be hesitant about provid-ing complete information to their Medicare pa-tients, and their non-Medicare patients may notbe informed at all. Although private publications,

140
specifically the newsletter published by the Pub-lic Citizen Health Research Group, periodicallypublish the names of sanctioned physicians andanalyze the grounds for sanctions, these publica-tions do not reach all Federal beneficiaries.
A serious gap in availability of information isthe lack of a central source for obtaining infor-mation about physicians who have been sanc-tioned by HHS as a result of PRO recommenda-tions. As mandated by the Health Care QualityImprovement Act of 1986 (Public Law 99-660),the proposed national data bank is not intendedto include information on sanctions imposed byHHS that result from PRO recommendations. Inany event, the information in the data bank willnot be publicly available.
Malpractice Compensation
Medical malpractice compensation cannot cur-rently be used as an indicator of poor quality ofcare because of the many variables other than themerits of the case that affect the resolution of in-dividual malpractice court trials and of negotiatedsettlements. Although it is clear that more andhigher payments are made against some special-ties than other specialties, there is insufficient evi-dence to evaluate whether multiple awards againstan individual physician indicate poor quality.
Given present information, malpractice litiga-tion information could possibly be used as ascreen or trigger for further investigation into aphysician’s performance by patients, hospitals,liability insurers, and third-party payers. Thescreen would be weak, since so few people filemalpractice claims and resolution often occursyears after the triggering incident (548). Questionsof the type of malpractice information (claims,settlements, or jury awards) to be used for screen-ing purposes would need to be decided, as wellas how many claims, settlements, and jury awardsover what time period would initiate the triggeraction.
Before malpractice compensation can be con-sidered an indicator of quality, much more needsto be learned about standards of care. There aredisagreements about what constitutes real mal-practice, and establishing standards of care mighthelp remedy the problem. Information is needed
on the relationship between physician character-istics and medical malpractice claims, judgmentsand settlements and on physician malpractice pro-files and negligently induced adverse outcomes.To understand the relationship between multiplepayments and negligence, more needs to beknown about the relationship of patient and prac-tice characteristics (e.g., the number of proceduresperformed) to multiple claims and payments. TheHarvard Medical Practice Group is starting to ex-amine medical care and medical injuries in theState of New York. Similar national informationis needed on the incidence, severity, and patternof injuries of negligently induced adverse out-comes. The Harvard group also intends to deter-mine the relationship of adverse outcomes to sub-sequent tort or disciplinary actions, and therelationship between the probability of suits andthe distribution of adverse events and of substand-ard care.2b
Government agencies have not traditionallycollected data on malpractice. Recently, however,the Health Care Quality Improvement Act of 1986established a mechanism in Federal law for col-lection and limited dissemination of informationon malpractice payments as well as formal Statedisciplinary actions, adverse hospital privilege in-formation, and adverse membership actions takenby professional societies. The 1986 act providesthat any entity that makes payment under a pol-icy of insurance or self-insurance or in settlementor satisfaction of a judgment in a medical mal-practice action or claim must report that infor-mation to the Secretary of HHS or the Secretary’sdesignee. The penalty for failure to report mal-practice information is a substantial fine. The in-formation that is to be reported includes the phy-sician’s name, the amount of payment, and adescription of the acts and omissions or injuriesupon which the action or claim was based. Thisinformation would dramatically improve what isknown about malpractice litigation and may of-fer an opportunity for reexamining the validityof malpractice information as an indicator of thequality of care.
The Health Care Quality Improvement Actmay also considerably improve the dissemination
ZbThe Robert wood Johnson Foundation has funded 13 otherprojects to increase current understanding of what constitutes medicalmalpractice, what causes it, and how it can be prevented (522).

141
of information on malpractice litigation. Cur-rently, dissemination of information on malprac-tice compensation is limited to information oncourt awards, which like any other court recordis public. The information is published sporadi-cally in costly private newsletters that cover met-ropolitan areas. The 1986 act requires HHS tomake physician-identified information collectedin the national data bank available to health careentities and licensing boards. Hospitals are re-quired to obtain the information from HHS, andwill be presumed to have the information in anymedical malpractice action. Information in thedata bank will not be available to individuals.Given the problems of using malpractice compen-sation as an indicator of the quality of care, pub-licizing such information to consumers requiresfurther examination.
Combinations of Indicators
A centralized system that includes informationon formal disciplinary actions taken by State med-ical boards, sanctions imposed by HHS upon rec-ommendation of PROS, malpractice compensa-tion, and information on other disciplinaryactions taken by medical entities could }Lelp toidentify recurring problems in the care providedby physicians and perhaps improve the validityof each of the actions as an indicator of quality.Shared information could improve the level ofdecisionmaking by all concerned bodies. If differ-ent, independent bodies censure a physician, theprobability that the physician is providing sub-standard care increases.
A combination of indicators might be a morevalid indicator of substandard care than a singleindicator. The information could assist in im-proving future care by making it more difficultthan it is now for physicians who have been dem-onstrated to provide substandard care to continueto practice. However, extreme caution would beneeded in using this particular combination of in-dicators. As discussed above, the validity of med-ical malpractice claims and compensation as anindicator of the quality of care is not clear. Re-cent data from the New York State Departmentof Health indicate that there is a linkage betweenmultiple malpractice claims and disciplinary ac-tions taken by the State medical board (460). Phy-
sicians who have had 6 or more medical malprac-tice claims made against them are likely to bedisciplined by the New York State medical board:the State medical board took disciplinary actionagainst 17 percent of such physicians. Furtherwork is needed, since only 181 physicians werestudied. The validity of adverse actions taken byhospitals and professional societies also needs tobe examined.
The national data bank mandated by the HealthCare Quality Improvement Act of 1986 is uniquein that malpractice judgments on individuals canbe compared with the type of disciplinary actionstaken by State medical boards and the adverseactions taken by hospitals and professional soci-eties. Since PRO/HHS sanctions will not be in-cluded, the usefulness of the data bank will belimited. Information on such sanctions does notappear to be widely disseminated. The OmnibusBudget Reconciliation Act of 1986 (Public Law 99-509) requires that PROS share, when requested,information related to substandard care with Statemedical boards and others, but final regulationshad not been released by March 1988.
Interest in greater cooperation and sharing ofinformation is seen in the Medicare and Medic-aid Patient and Program Protection Act of 1987(Public Law 110-93). That law strengthens theprovisions in the earlier Health Care Quality Im-provement Act and requires States to make avail-able to the Secretary of HHS information concern-ing disciplinary actions taken by State medicalboards against a range of health care practitioners.The 1987 law also requires that the Secretary ofHHS disseminate information on these actions toState medical licensure boards and to other Stateand Federal officials.
As noted earlier, information in the data bankmandated by the Health Care Quality improve-ment Act will not be available to individuals, andthis situation might be reasonable. A prudentcourse of action in establishing the data bankwould be to begin with fairly detailed data butvery limited distribution, and then to test theseeming credibility and usefulness of the data asthey begin to accumulate for statistical power oractuarial credibility. The data bank will need tobe continuously analyzed and revised with con-tinuing experience.