Chapter 6 Care of the Patient with a Gallbladder, Liver, Biliary Tract,
91
1 Chapter 6 Care of the Patient with a Gallbladder, Liver, Biliary or Exocrine Pancreatic Disor
-
Upload
galvin-shepherd -
Category
Documents
-
view
127 -
download
2
description
Chapter 6 Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder. Liver, Biliary Tract, Pancreas, & Gallbladder Disorders. Cirrhosis Etiology/pathophysiology Chronic, degenerative disease of the liver - PowerPoint PPT Presentation
Transcript of Chapter 6 Care of the Patient with a Gallbladder, Liver, Biliary Tract,

1
Chapter 6
Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder
Chapter 6
Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder


Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis– Etiology/pathophysiology
• Chronic, degenerative disease of the liver
• Scar tissue restricts the flow of blood to the liver
• Types of cirrhosis– Laënnec’s cirrhosis
– Postnecrotic cirrhosis
– Primary biliary cirrhosis
– Secondary biliary cirrhosis

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Etiology/pathophysiology (continued)
• Alteration of liver function– Reduced ability to metabolize albumin
• Obstruction of portal vein– Increased pressure in veins that drain GI tract
• Complications– Portal hypertension
– Ascites
– Esophageal varices
– Hepatic encephalopathy

LIVER


Liver, Biliary Tract, Gallbladder, & Pancreas Disorders
• Cirrhosis (continued)– Clinical manifestations/assessment
• Early stages– Abdominal pain
– Liver is firm and easy to palpate
• Late stages– Dyspepsia
– Changes in bowel habits
– Nausea and vomiting
– Gradual weight loss

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Clinical manifestations/assessment (continued)
• Late stages (continued)– Ascites
– Enlarged spleen
– Spider angiomas
– Anemia
– Bleeding tendencies
– Epistaxis

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Clinical manifestations/assessment
(continued)• Late stages (continued)
– Purpura
– Hematuria
– Bleeding gums
– Jaundice
– Disorientation

Figure 46-2
Systemic clinical manifestations of liver cirrhosis.
(From Lewis, S.M., Heitkemper, M.M., Dirksen, S.R. [2004]. Medical-surgical nursing: assessment and management of clinical problems. [6th ed.]. St. Louis: Mosby.)

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Medical management/nursing interventions
• Eliminate the cause– Alcohol
– Hepatotoxins
– Environmental exposure to harmful chemicals
• Antiemetics– Benadryl and Dramamine
– Contraindicated: Vistaril, compazine, and Atarax

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Medical management/nursing interventions
(continued)• Diet
– Well-balanced
– High calorie
– Moderate protein
– Low fat
– Low sodium
– Supplemental vitamins and folic acid

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Medical management/nursing interventions
(continued)• Treatment of complications
– Ascites
• Bedrest
• Strict I&O
• Restrict fluids and sodium
• Diuretics: aldactone, Lasix, HCTZ
• Vitamins K, C, and folic acid supplements
• LeVeen peritoneal-jugular shunt
• Paracentesis

Figure 46-3
LeVeen continuous peritoneal jugular shunt.
(From Beare, P.G., Myers, J.L. [1998]. Adult health nursing. [3rd ed.]. St. Louis: Mosby.)

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Medical management/nursing interventions
(continued)• Treatment of complications (continued)
– Ruptured esophageal varices• Maintain airway; establish IV• Vasopressin drip to control bleeding• Sengstaken-Blakemore tube• Endoscopic sclerotherapy• Portacaval shunt• Blood transfusion

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cirrhosis (continued)– Medical management/nursing interventions
(continued)• Treatment of complications (continued)
– Hepatic encephalopathy• Decrease protein in diet• Avoid drugs which are detoxified by the liver• Lactulose• Neomycin

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Hepatitis– Etiology/pathophysiology
• Inflammation of the liver resulting from several types of viral agents or exposure to toxic substances
• Hepatitis A– Most common
– Oral-fecal transmission

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Hepatitis (continued)–Etiology/pathophysiology
• Hepatitis B– Transmission by contaminated serum; blood
transfusion, contaminated needles, dialysis, or direct contact with infected body fluids
• Hepatitis C– Transmitted through contaminated needles
and blood transfusions

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Hepatitis (continued)– Etiology/pathophysiology (continued)
• Hepatitis D– Co-infection with hepatitis B
• Hepatitis E– Fecal contamination of water– Rare in the U.S.; usually in developing
countries

HEPATITIS C

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Hepatitis (continued)– Clinical manifestations/assessment
• General malaise• Aching muscles• Photophobia• Headaches• Chills• Abdominal pain• Dyspepsia• Nausea

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Hepatitis (continued)– Clinical manifestations/assessment
• Diarrhea/constipation• Pruritus• Hepatomegaly• Enlarged lymph nodes• Weight loss• Jaundice• Dark amber urine• Clay-colored stools

Figure 46-5
Severe jaundice.

HEPATITIS

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Hepatitis (continued)– Medical management/nursing
interventions• Treat symptoms• Small, frequent meals
– Low fat, high carbohydrate
• IV fluids for dehydration• Vitamin C, vitamin B-complex, vitamin K• Avoid unnecessary medications, especially
sedatives

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Hepatitis (continued)– Medical management/nursing
interventions (continued)• Gamma globulin or immune serum globulin• Hepatitis B immune globulin (HBIG)
– Should be given to anyone exposed to hepatitis B
• Hepatitis B vaccine– Should be given to people identified as high risk
for developing hepatitis B

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Liver abscesses– Etiology/pathophysiology
• May be single or multiple
• Abscess forms in the liver due to an invading bacteria

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Liver abscesses (continued)– Clinical manifestations/assessment
• Fever• Chills• Abdominal pain and tenderness in the right upper
quadrant• Hepatomegaly• Jaundice• Anemia

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Liver abscesses (continued)– Medical management/nursing
interventions• IV antibiotics
• Percutaneous drainage of liver abscess
• Open surgical drainage

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
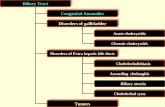
• Cholecystitis and cholelithiasis– Etiology/pathophysiology
• An obstruction, gallstone, or tumor prevents bile from leaving the gallbladder and the trapped bile acts as an irritant causing inflammation
• Risk factors– Female; American Indian or white; obesity;
pregnancy; diabetes; multiparous women; use of birth control

Figure 46-6
Common sites of gallstones.

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cholecystitis and cholelithiasis Clinical manifestations/assessment
• Indigestion after eating foods high in fat• Severe, colicky pain in the right upper
quadrant• Anorexia• Nausea and vomiting• Flatulence • Increased heart and respiratory rates• Diaphoresis

GALLSTONES

GALLSTONES

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cholecystitis and cholelithiasis (continued)– Clinical manifestations/assessment
(continued)• Low-grade fever
• Elevated WBC
• Mild jaundice
• Steatorrhea (fatty stool)
• Dark amber urine

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cholecystitis and cholelithiasis – Medical management/nursing
interventions• Mild attacks
– Bedrest
– NG tube to suction
– NPO
– IV fluids
– Antispasmodic/analgesic
– Antibiotics
– Avoid spicy foods when allowed PO intake

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Cholecystitis and cholelithiasis– Medical management/nursing
interventions (continued)• Lithotripsy
• Cholecystectomy– Laparoscopic– Open

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
PancreatitisEtiology/pathophysiology
Inflammation of the pancreasAcute or chronic
Predisposing factorsAlcohol
Trauma
Infectious disease
Certain drugs

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Pancreatitis (continued)– Clinical manifestations/assessment
• Abdominal pain• Anorexia; nausea and vomiting• Malaise• Low-grade fever• Jaundice• Weight loss• Steatorrhea• Tachycardia

Liver, Biliary Tract, Pancreas, & Gallbladder Disorders
• Pancreatitis (continued)– Medical management/nursing
interventions• NPO• IV fluids• NG tube• Antiemetics• Demerol 75-100 mg every 3-4 hours• Anticholinergics• Antacids or Tagamet (prevent ulcers)• Hyperalimentation

Figure 46-9
Whipple’s procedure, or radical pancreaticoduodenectomy.
(From Lewis, S.M., Heitkemper, M.M., Dirksen, S.R. [2004]. Medical-surgical nursing: assessment and management of clinical problems. [6th ed.]. St. Louis: Mosby.)

NURSING PROCESS
• NURSING DIAGNOSIS– Activity intolerance– Breathing pattern, ineffective– Fluid volume, deficient– Home maintenance, impaired– Injury, risk for– Knowledge, deficient

NURSING PROCESS
– Noncompliance– Nutrition, imbalanced, less than body
requirements– Pain, acute/chronic– Powerlessness– Skin integrity, impaired– Thought processes, disturbed

QUOTE
• "Don't procrastinate. Putting off an unpleasant task until tomorrow simply gives you more time for your imagination to make a mountain out a possible molehill. More time for anxiety to sap your self-confidence. Do it now, brother, do it now. " Author Unknown, from Ten Ways to Worry Less and Accomplish More

Chapter 24Agents Used to Treat Hyperacidity and
Gastroesophageal Reflux Disease

Secretory Functions of the Stomach Lining
• Parietal cells secrete hydrochloric (HCl) acid
• Chief cells secrete pepsinogen
• Mucoid cells secrete mucus

Stomach Hyperchlorhydria• Produced from:
– Eating high-fat meals– Increased alcohol intake– Emotional turmoil

Goal of Antacid Therapy
• Neutralize the acid
• Inhibit pepsin activity
• Increase resistance of the stomach lining
• Increase tone of the lower esophageal sphincter

AntacidsThree Forms
1. Aluminum
2. Magnesium
3. Calcium
• Mechanism of action– Neutralization of gastric acidity– Low doses promote gastric mucosal
defensive mechanisms

Systemic Antacids• Useful in short-term therapy
• Rapid onset
• Prolonged use causes an overload on the kidneys– Example: sodium bicarbonate

Nonsystemic Antacids
• Remain in gastrointestinal tract; useful in long-term therapy
• Most of the dose remains in the gastrointestinal tract
• Will not alter acid-base system– Examples: calcium carbohydrate (Tums,
Rolaids), aluminum carbonate (Basaljel), magaldrate (Riopan), etc.

Side Effects and Adverse Effects
• Magnesium: diarrhea
• Aluminum: constipation
• Calcium: constipation

Antacid Interactions• Binding of other drugs to the antacid
causes reduced availability of the other drugs to the client.
• Chemical inactivation
• Increases stomach and urine pH (alkaline), which decreases the absorption and excretion of certain drugs

Nursing Interventions
• Monitor for side effects– Nausea, vomiting, abdominal pain,
diarrhea– With calcium-containing products:
constipation, acid rebound
• Monitor for therapeutic response– Notify heath care provider if symptoms
are not relieved.

Histamine (H2) Receptor Antagonists
• Examples– Cimetadine (Tagamet)– Famotidine (Pepcid)– Nizatidine (Axid)– Ranitidine (Zantac)

Proton Pump Inhibitors• Omeprazole (Prilosec)
– Blocks the final step of acid production in the stomach
• Indicated for clients with:– Gastroesophageal reflux disease (GERD)– Gastric hypersecretory condition
• Interactions– Causes warfarin (an anticoagulant) action
to be increased

Helicobacter Pylori
• An organism associated with the development of peptic ulcer disease
• Treatment– Metronidazole (Flagyl), an antimicrobial
agent, along with bismuth subsalicylate (Pepto-Bismol) and tetracycline (antimicrobial) for 4 weeks to eradicate Helicobacter pylori

Metoclopramide (Reglan) • A drug that stimulates the motility of the
upper GI tract without stimulating the production of gastric, biliary, or pancreatic solutions
• Action– Increases peristalsis in the duodenum and
jejunum– Decreases gastroesophageal reflux
(continues)

Metoclopramide (Reglan)
• Adverse effects– Produces extrapyramidal (Parkinson-like
symptoms) effects– Central nervous system depression– Gastrointestinal upset
(continued)

Chapter 25
Emetics and Antiemetics

Emetics • Agents that induce vomiting
– Used in overdoses
• Example– Ipecac syrup
• Inappropriate use– Clients with bulimia

Antiemetics
Five categories of antiemetics
1. Anticholinergics
2. Antihistamines
3. Neuroleptic agents
4. Prokinetic agents
5. Serotonin blockers

Anticholinergics and Antihistamines
• Anticholinergics– Bind to and block acetylcholine
receptors• Prevent nausea stimuli from being
transmitted
• Antihistamines– Block H2 receptors
• Prevent cholinergic stimulation

Neuroleptic and Prokinetic Agents
• Neuroleptic agents– Bind to the dopamine receptors and
block action• Limit dopamine activity
• Prokinetic agents– Block dopamine– Stimulate acetylcholine to increase
gastric emptying

Serotonin Blockers• Block serotonin receptors in the
gastrointestinal tract
• Block serotonin receptors in the central nervous system (emetic center)– Used often when antineoplastic
agents are being given

Anticholinergics and Antihistamines
• Anticholinergics– Scopolamine (Trans Scop)
• Antihistamines– Promethazine (Phenergan)– Meclizine (Antivert)

Emetics and Antiemetics
• Neuroleptic agents– Chlorpromazine (Thorazine)
• Prokinetic agents– Metoclopramide (Reglan)
• Serotonin blockers– Ondansetron (Zofran)

Side Effects and Adverse Effects• General
– Dizziness– Drowsiness– Dry mouth– Headache

Nursing Process• Assessment
– Thorough history and physical
• Plan– Use proper route
• Implementation– Safely administer medication
• Evaluation– Are the nausea and vomiting gone?

Chapter 26
Laxatives and Antidiarrheals

Laxative Classifications• Stimulant
• Saline
• Bulk-forming
• Lubricant– Stool softeners– Suppositories
• Lactulose
• Enemas

Stimulant Laxatives• Action
– Chemical irritation• Increase motility of the GI tract
– Increase secretion of water into large and small intestine• Example: bisacodyl

Saline Laxatives• Increase osmotic pressure within
the intestinal tract– Cause more water to enter the
intestines
– Result in: • Bowel distention, increased
peristalsis, and evacuation
(continues)

Saline Laxatives• Contain salt
• Unpleasant taste
• Systemically absorbed
• Result in:– Poor client compliance– Risk for dehydration – Risk for congestive heart failure
(continued)

Bulk-Forming Laxatives• Safest form
– Absorbs water to increase bulk – Distends bowel to initiate reflex bowel
activity• Not systemically absorbed
– High fiber – Natural or semisynthetic
• Examples: psyllium hydrophilic muciloid (Metamucil), methylcellulose (Citrucel), and polycarbophil (Fibercon)
(continues)

Bulk-Forming Laxatives• Must be followed with a large amount
of fluid– If chewed or taken in dry powder form,
these agents can cause esophageal obstruction and/or fecal impaction.
(continued)

Lubricant Laxatives• Oils lubricate the fecal material
and intestinal walls, thereby promoting fecal passage:
– Prevent fat-soluble vitamins from being absorbed
• Popular lubricant– Mineral oil (liquid petroleum)
• Not digested or absorbed

Stool Softeners • Detergent-like drugs:
– Permit mixing of fats and fluids with the fecal mass
– Stool becomes softer and is passed much easier
– Takes several days to work
• Example: docusate salts (Colace and Surfak)

Suppositories • Usually in a wax base
• Administered rectally
• Absorbed systemically
• Available containing stimulant drugs– Glycerin
• Absorbs water from tissues, creating more mass
– Bisacodyl • Induces peristaltic contraction by direct
stimulation of sensory nerves


Lactulose Laxatives• Two monosaccharides that are not
digested or absorbed
• Digested in the colon by bacteria to form acids substances
– Acid substances cause water to be drawn into the colon

GoLYTELY • Polyethylene glycol (electrolyte
solution and salt)– Must consume 4 liters within 3
hours
– Causes a large volume of water to be retained in the colon
– Acts within one hour• Produces a diarrheal state

Enemas• Hyperosmotics
– Solution contain salts (e.g., Fleet enema) • Administered rectally and cause a
laxative effect by osmotically drawing fluid into the colon to initiate defecation


Long-Term Use• Long-term use of laxatives often
results in decreased bowel tone and may lead to dependency.
• Encourage– A healthy, high-fiber diet– Increased fluid intake

Adsorbents• Most commonly used
• Claylike materials administered in a tablet or liquid suspension form after each loose bowel movement
• Bind to the causative bacteria or toxin, and are eliminated through the stool
• Little scientific proof that they work– Examples: kaolin-pectin, attapulgite
(Kaopectate)

Antidiarrheals• Reduce GI motility• Opium is a narcotic.
– Decreases bowel motility and rectal spasms
– Depresses the CNS; monitor closely– Decreases transit time through the
bowel; more time for water and electrolytes to be absorbed
• Paregoric is an opium tincture.– May cause physical dependence (continues)

Antidiarrheals• Loperarmide HCl (Imodium)
– Made from chemicals related to meperidine, a narcotic
• Diphenoxylate HCl and atropine sulfate (Lomotil)– Narcotic and anticholinergic drug
• Reduces GI motility
(continued)

Anticholinergics• Decrease intestinal muscle tone
and peristalsis of GI tract
• Result: slows the movement of fecal matter through the GI tract
– Example: belladonna alkaloids (Donnatal)

Nursing Implications• Monitor for therapeutic effect